Back to Journals » Medical Devices: Evidence and Research » Volume 18
A Comparative Effectiveness Study of Two Narrow-Profile Staplers Used in Video-assisted Thoracoscopic Lobectomy
Authors Pan IW ![]() , Siddiqui ZA
, Siddiqui ZA ![]()
Received 8 August 2025
Accepted for publication 31 October 2025
Published 13 November 2025 Volume 2025:18 Pages 565—572
DOI https://doi.org/10.2147/MDER.S555680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
I-Wen Pan, Zasim Azhar Siddiqui
Medtronic PLC, Boston, MA, USA
Correspondence: I-Wen Pan, Medtronic PLC, 8200 Coral Sea St NE, Mounds View, MN, 55112, USA, Email [email protected]
Purpose: The objective of this study was to evaluate and compare the effectiveness of a narrow-profile, small-diameter reload to a powered vascular stapler when used during VATs lobectomy.
Patients and Methods: This was a retrospective, observational cohort study comparing outcomes after VATs lobectomy procedures in which either the Echelon Flex™ powered vascular stapler (PVS) or a Signia™ small-diameter reload (SDR) was used to transect pulmonary vasculature. Data from adult patients (≥ 18 years of age) who had lung cancer and underwent elective, primary VATs lobectomy in the 3 years between 2021 and 2023 were extracted from the PINC AI healthcare database. Two patient groups (PVS vs SDR) were propensity-score matched using a 1:1 nearest neighbor matching scheme with a caliper of 0.2 to adjust the baseline patient characteristic imbalance. Two sensitivity analyses were performed using multivariable regression models and propensity score inverse probability weighting.
Results: Of 558 (34.1% SDR and 65.9% PVS) eligible inpatient cases, 68.5% age ≥ 65, 58.2% were female, 59.0% were married, 79.8% White, 68.5% were Medicare, 73.5% had comorbidity ≥ 3. One hundred and ninety pairs were matched. The incidence rate of blood transfusion was significantly higher in the PVS group than in the SDR group (PVS vs SDR: 6.4% vs 0.5% for matched pairs, difference: 5.8%, 95% confidence interval (CI) 2.2%– 9.5%, p = 0.002). The incidence rate of bleeding was not significantly different between the groups and no conversions were observed. Intensive care unit visits and length of stay were higher in the PVS group. Sensitivity analyses results were consistent with these findings.
Conclusion: The narrow-profile SDR was an effective and beneficial tool for division and ligation during VATs lobectomy and is associated with fewer blood transfusions compared to PVS.
Plain Language Summary: PLS Title: Comparing the performance of two surgical staplers during minimally invasive lung surgery.
Surgical staplers are used for many kinds of surgeries. Some staplers are better for certain uses, depending on their design. In this article, we analyzed patient records from a US hospital-based, service-level, all-payer healthcare claims to help understand how two different surgical staplers performed in preventing bleeding during lobectomy (a type of lung surgery). One is called the “powered vascular stapler” (PVS) and the other is a “small-diameter reload” (SDR). We looked at lung cancer patients who underwent lobectomy in the years 2021 and 2023.
Both staplers were effective tools during surgery. However, patients who had a procedure using the SDR stapler were less likely to need a blood transfusion compared to those where the PVS stapler was used. This suggests that patients in the SDR group may have lost less blood during surgery. Therefore, the SDR stapler might be a more suitable tool for minimally invasive lobectomy.
Keywords: video-assisted thoracoscopic surgery, minimally invasive surgery, thoracic surgery, lobectomy, surgical stapler, small-diameter reload, blood transfusion
Introduction
It has been estimated that as many as 8000–9000 video-assisted thoracoscopic surgery (VATs) lobectomy procedures are performed in inpatient settings every year in the US.1,2 While the use of surgical staplers for tissue division and vessel ligation is common in thoracic surgery, the use of these staplers on the pulmonary vasculature is associated with the risk of severe and even fatal intraoperative bleeding along the staple line.3
The development of surgical staplers that simultaneously deliver multiple rows of staples while transecting has been beneficial for improving hemostasis in general surgery applications;4 however, many stapler reload-shaft assemblies, which include the jaw, the drive and firing mechanisms, and the reloadable staple reload can be bulky in size and shape, and lack maneuverability. This can present a challenge when structures are difficult to reach due to their size, surrounding space, and anatomical location. In particular, there is a growing need for reloads with smaller profiles that are optimal for procedures within the confines of the thoracic cavity.
Previously, a narrow-profile, powered vascular stapler (PVS) has been shown to be similarly effective to standard-of-care (SOC) staplers during VATs lobectomy,5 with improvements in incidence of bleeding and blood transfusion.6 Another narrow-profile, small-diameter reload (SDR) with an alternative design was subsequently commercialized, and a recent prospective, non-comparative registry study demonstrated that the novel SDR provided effective hemostasis when fired on pulmonary vasculature during indicated thoracic procedures without introducing new risks or harms to patients.7 However, to our knowledge, an analysis of the comparative effectiveness of the two staplers has not been reported. The aim of this study was to evaluate and compare the effectiveness of SDR and PVS used during VATS lobectomy, with bleeding and blood transfusion as primary outcomes, and conversion rate, intensive care unit (ICU) admission, and length of stay as secondary outcomes.
Methods
Study Design and Ethics
This was a retrospective, observational cohort study comparing outcomes after VATs lobectomy procedures during which one of the two brands of narrow-profile staplers was used to transect pulmonary vasculature. All patient data were from a third-party licensed database and de-identified in accordance with the Health Insurance Portability and Accountability Act. Therefore, the study was determined exempt from full board review and informed consent requirements by Sterling IRB.
Study Devices
The specific devices compared in this analysis were the Echelon Flex™ powered vascular stapler, product code PVS35A (Johnson & Johnson, New Brunswick, NJ) and the Signia ™ small-diameter reloads, with either manual or powered handles, product codes SIGSDS30CTV, SIGSDS30CTVT, and SIGSDL45CTVT (Medtronic, Minneapolis, MN).
Data Source and Cohort Construction
Patient data was extracted from the PINC AI healthcare dataset (Premier, Inc., Charlotte, NC). PINC AI contains charge master and hospital charge files from more than 1160 contributing healthcare systems, from patients covered by both Medicare and commercial payers. The database allows identification of specific procedure types and device use by searching procedure codes and text strings.
The patient population for this analysis consisted of adult patients (≥18 years of age) who underwent elective, primary VATs lobectomy in the 3-year period between January 1, 2021, and December 31, 2023. Patients were identified based on the presence of an inpatient claim with relevant primary procedure codes (ICD 10 PCS; Supplementary Material A). Patient records enrolled in the study were assigned to one of the two cohorts based on whether the SDR or PVS study device was used in the VATs procedure. Use of the devices was identified by performing a text-based search through the charge master and hospital charge files, using the brand names and product numbers.
Patients were excluded from the analysis if both of the name-brand devices were used during the same procedure, if the surgical procedure was not elective, or if records were missing the key analysis variables. Lastly, to reduce the heterogeneity, we removed cases with no lung cancer diagnosis.
Variables and Outcomes
Baseline variables extracted from records included patient age, marital status, gender, race and ethnicity, payer category, and Charlson Comorbidity Index (CCI) score.
The primary study outcomes were bleeding and blood transfusion, based on the presence of ICD 10 diagnosis and procedure codes and current procedural terminology (CPT) codes (Supplementary Material B) in inpatient claim files.8 The secondary outcome was conversion rate (Supplementary Material C), defined as patient records with secondary diagnosis codes of Z53.31, Z53.32, Z53.39,9 ICU visit, and length of stays.
Analytical Methods
Descriptive analyses were used to report the number of cases and the proportion of subcategory for categorical baseline demographics, clinical and provider characteristics, and the unadjusted outcomes. Bivariate analysis using chi-square or Fisher’s exact test examined the baseline balance in covariates between the SDR and PVS cohorts.
Propensity Score Matching
To mitigate the influence of potentially confounding baseline variables on the estimated impact of the interventions, propensity score matching was performed between the SDR and PVS cohorts using a 1:1 nearest neighbor matching scheme with a caliper of 0.2.8,10 Based on existing literature, the baseline covariates for propensity score matching were age (<65 and ≥65), gender (male or female), marital status (married or other), race and ethnicity (non-Hispanic white or other), payer type (Medicare or other), and CCI score (0–2 or ≤3). The standard differences between subgroups of covariates before and after propensity score matching were reported. After matching, the post-PSM outcomes estimation was used with bias correction regression adjustment.11
To evaluate uncertainty and assess the robustness of the results, two sensitivity analyses were performed: first, multivariable logistic regression and generalized linear models for categorical and continuous outcomes, respectively; and second, propensity score inverse probability weighting (IPW) method. The Hosmer–Lemeshow goodness-of-fit test was used to assess the post-logistic regression model’s fit and calibration.
All analyses were conducted using SAS 9.4 (SAS Institute Inc, Cary, NC) and Stata 18.0 (College station, TX) using 2-sided statistical tests.
Results
Between January 1, 2021, and December 31, 2023, a total of 14,428 patients within the PINC AI dataset were discharged after VATs surgery (Figure 1). Of those, 558 met all eligibility criteria (34.1% SDR and 65.9% PVS; Table 1) and were included in the analysis. The majority of patients were 65 or older (68.5%), female (58.2%), married (59.0%), non-Hispanic White (79.8%), with Medicare (68.5%), and had CCI score of 3 or greater (73.5%). There was heterogeneity of race and ethnicity and payers in two groups (p < 0.05; Table 1).
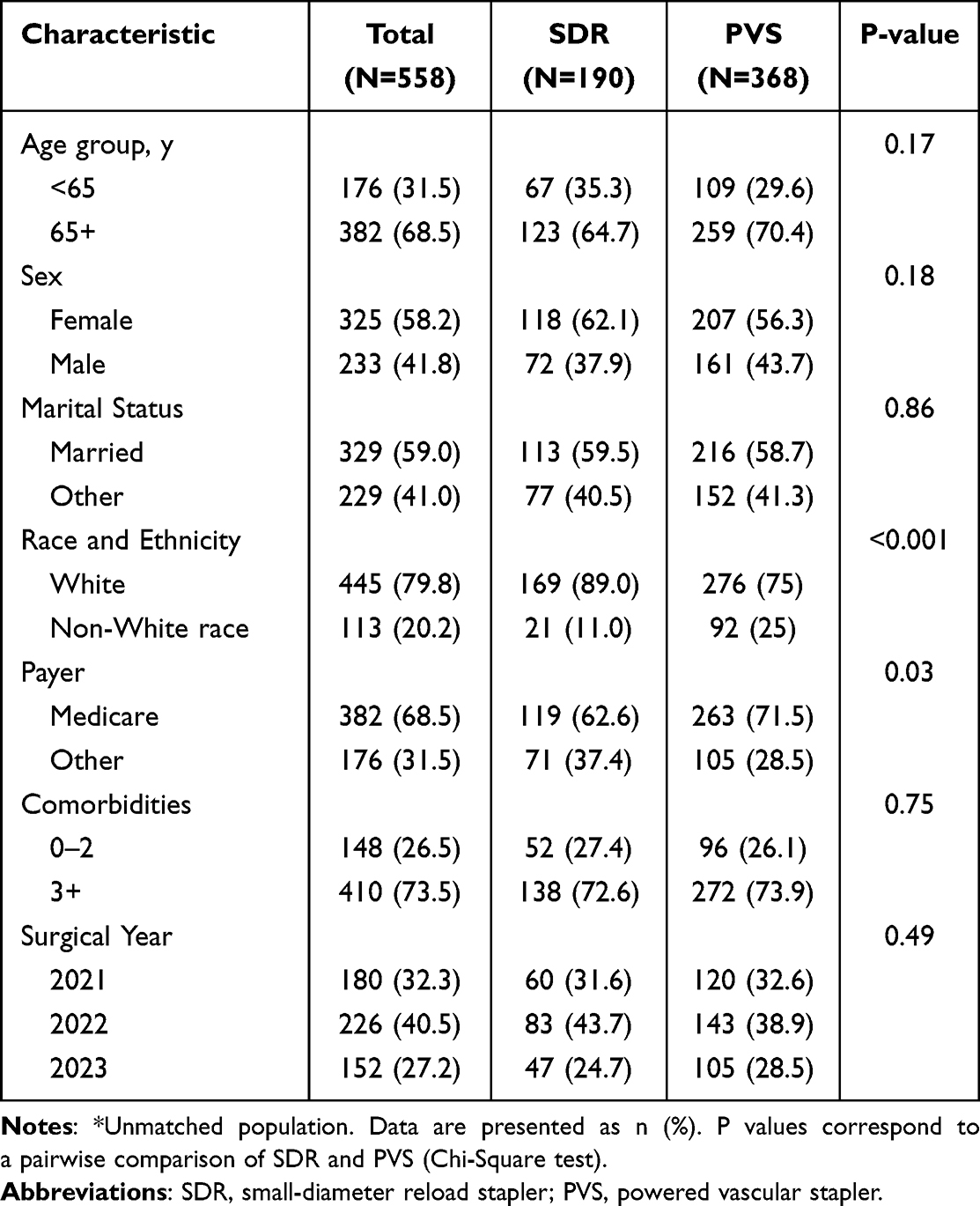 |
Table 1 Baseline Demographics, Clinical Characteristics, and Provider Characteristics* |
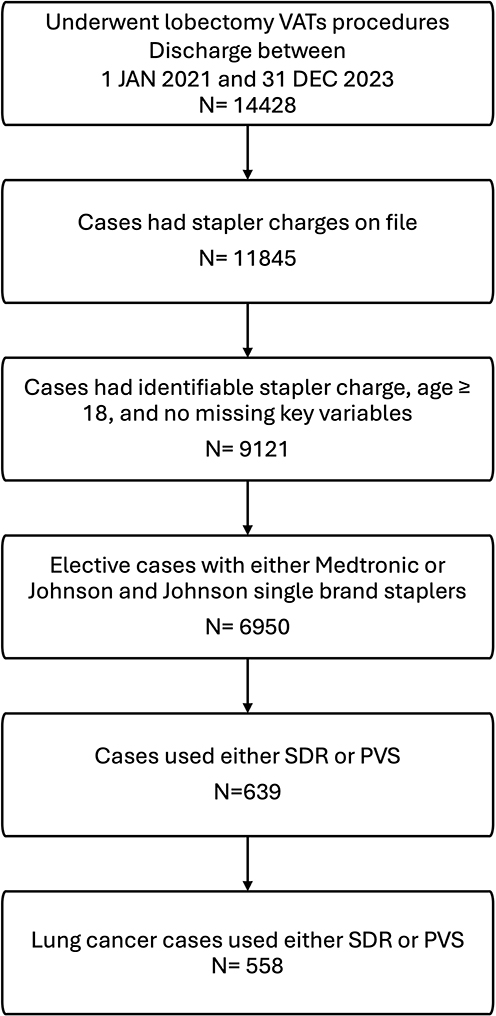 |
Figure 1 Subject disposition. |
Following propensity scores matching, there were 190 matched pairs available for analysis (Table 2). Overall, the standard difference in patient characteristics for the 190 matched pairs was <0.05 (Figure 2).
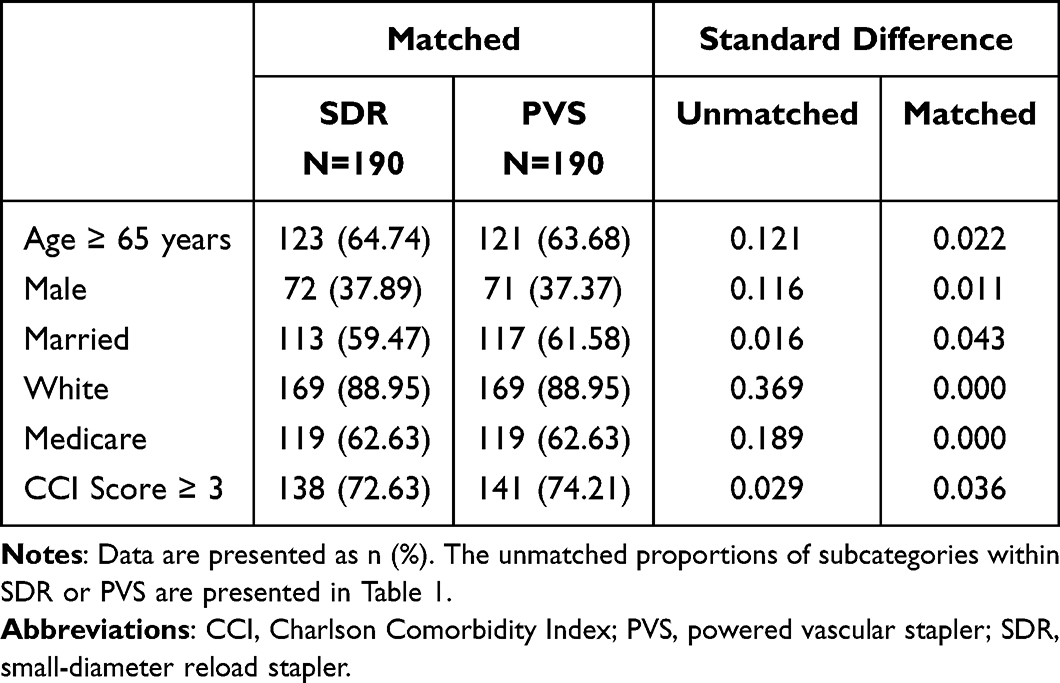 |
Table 2 Standard Difference in Unmatched and Matched Cohort |
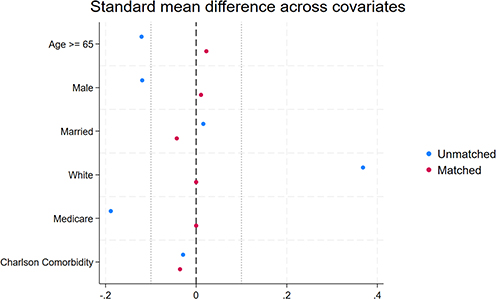 |
Figure 2 Standard differences for study cohort before and after propensity matching. The overall standard difference was < 0.05. |
Prior to propensity matching, the unadjusted incidence of blood transfusion was significantly higher in the PVS cohort than in the SDR cohort (5.4% vs 0.6%; p = 0.002; Table 3). The incidence of bleeding was not significant between the two groups, and no conversions were observed in either group. Additionally, the incidence of ICU visits (p = 0.001) and the mean length of stay (p = 0.027) were significantly higher in the PVS group compared to SDR group (Table 3).
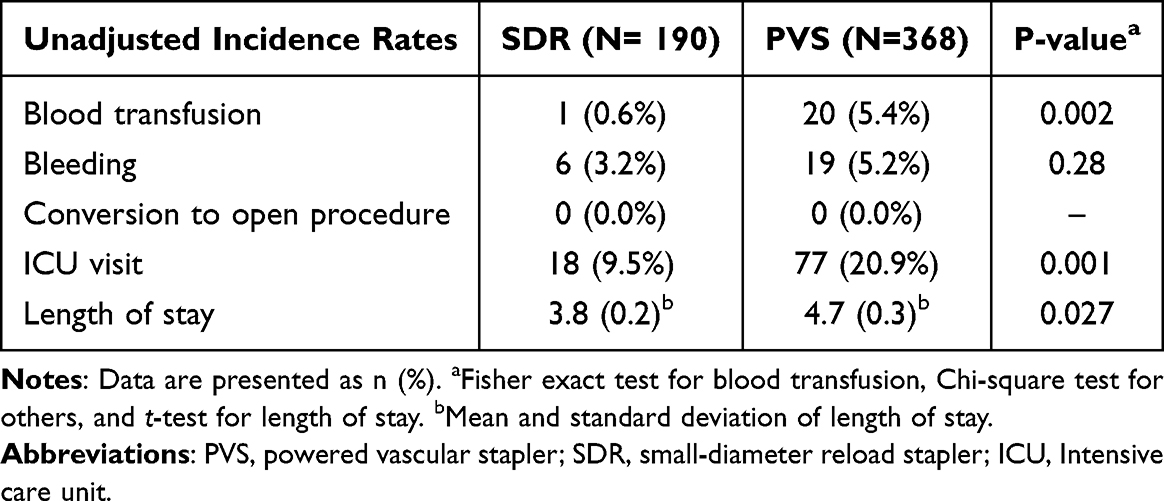 |
Table 3 Outcomes by Type of Staplers Before Propensity Score Matching |
Consistent with the unadjusted outcomes, an analysis of the matched pairs showed that the rate of blood transfusion in the PVS group was 12.8 times greater than in the SDR group (incidence rate: 6.4% vs 0.5%, respectively; p = 0.002; Table 4). The incidence rate of ICU visit (25.3% vs 9.5%, p<0.001) and mean length of stay (5.0 vs 3.8 days, p = 0.025) were higher in the PVS group compared to the SDR group. Lastly, the incidence rates of bleeding remained insignificant between the two groups in the matched analysis (p = 0.14).
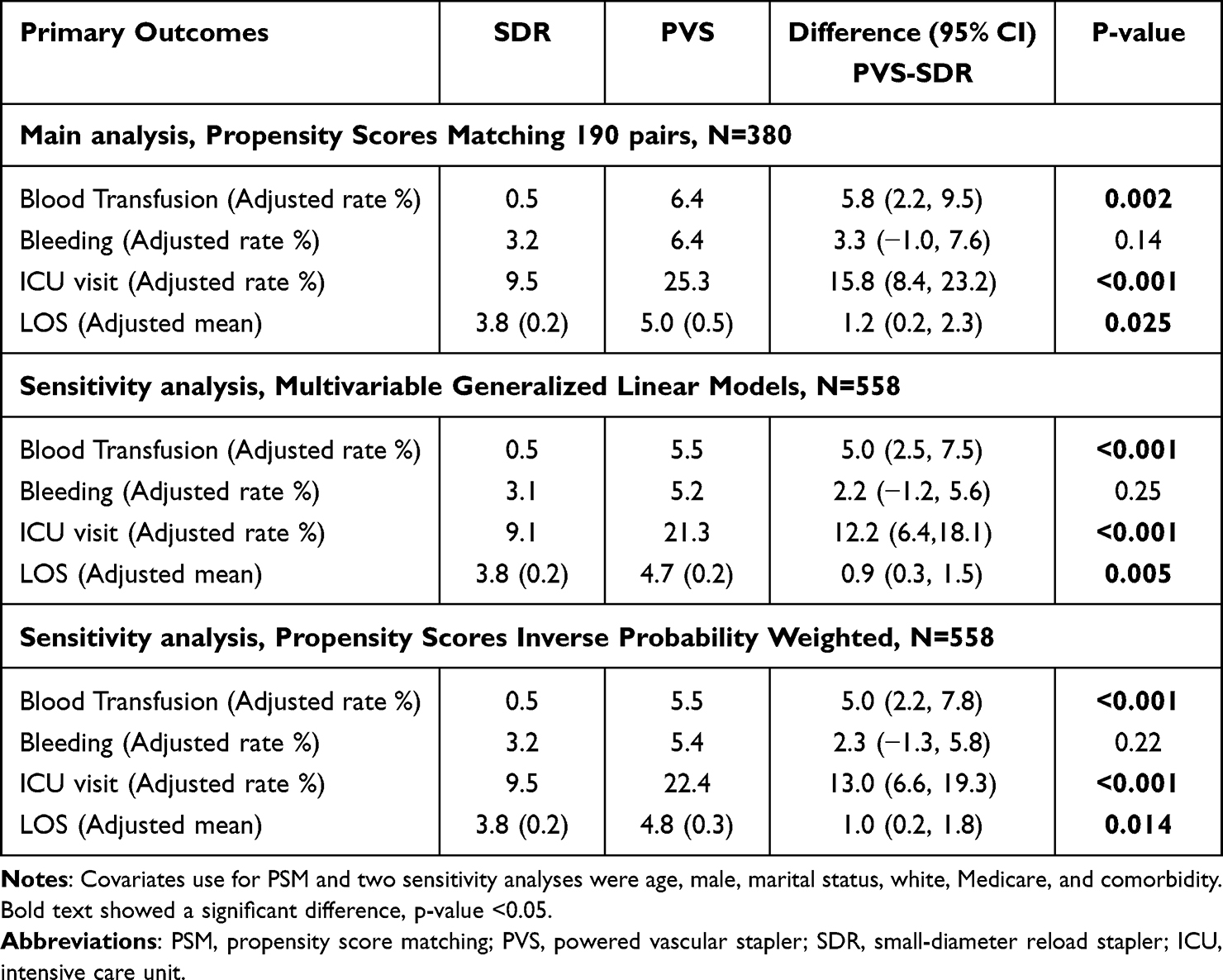 |
Table 4 Clinical Outcomes After Propensity Score Matching and Two Sensitivity Analyses |
Sensitivity analyses using multivariable regression and IPW showed results consistent with the primary PSM analysis (Table 4). The incidence of blood transfusion remained significantly higher in the PVS cohort compared with the SDR cohort (PVS 5.5% vs SDR 0.5%, p < 0.001) in both the logistic regression and IPW models. Similarly, the rates of ICU visits were higher in the PVS cohort (regression: 21.3% vs 9.1%, p < 0.001; IPW: 22.4% vs 9.5%, p < 0.001), as was the mean length of stay (regression: 4.7 vs 3.8 days, p = 0.005; IPW: 4.8 vs 3.8 days, p = 0.014). There was no significant difference in the incidence of bleeding between the two groups.
Discussion
In this comparative effectiveness study of real-world patient claims, we have shown that there is a large, clinically and statistically significant reduction in the risk of blood transfusion during VATs lobectomy procedures when SDR is used for division and ligation instead of PVS although there was no significant difference in bleeding rates. Two additional outcomes, ICU visits and length of stay, also demonstrated a significantly lower incidence and shorter mean duration in the SDR group. The cohort sizes were small; consequently, the study may not have been able to detect real differences between the device alternatives in some outcomes. Specifically, the incidence of conversion to open surgery was rare and not observed in the present study.
The effectiveness of both PVS and SDR for pulmonary procedures has been reported previously.5,7 A 2020 study published by Molins et al evaluated the effectiveness of the PVS compared to SOC staplers in VATs lobectomy.5 In this randomized, controlled, multicenter study in 201 patients, the rate of intraoperative hemostatic interventions were not statistically different between the two cohorts (5.3% for SOC versus 8.3% for PVS, respectively; p = 0.137). About 2.9% blood transfusion requirement for any reason was reported. There were no adverse events related to the use of the study devices. Another study by Chen et al, which compared outcomes from 50 patients who participated in a single-arm, multicenter clinical trial of PVS against 225 matched SOC controls, found that the incidence of bleeding in the SOC stapler group was 17.3% versus 4.0% in the PVS group (p = 0.0167).6 Reoperation rates and hospital LOS were also reduced in the PVS group.
More recently, Khandhar et al reported a multi-center, retrospective study of outcomes after use of SDRs for ligation and division of the pulmonary vasculature, in 120 thoracic procedures comprising a total of 302 SDR firings.7 Clinically necessary hemostatic intervention was required in 3/302 firings (0.99%). None of the 4 conversions to open surgery were due to SDR staple lines. The 99% hemostatic rate was independent of surgical access and stapler handle preference.
Lung parenchyma and hilum are highly vascularized tissues that are especially delicate and at high risk of bleeding and air leak during resection. Even hemostatic interventions that work well in other surgical procedures—such as surgical stapling—can, themselves, cause tensional stress, tearing, and bleeding in the lungs. Coupled with the restricted access encountered during VATs procedures, pulmonary tissue presents specific needs that are not well met by general-use surgical staplers. The two staplers alternatives evaluated in the present study were specifically designed for improved access within the narrow confines of a VATs procedure, and also with specific consideration of pulmonary tissue, and therefore this direct comparison of effectiveness for reducing the risk of relevant complications is a useful and pertinent contribution to the surgical literature.
Study Limitations
This was a retrospective database study and therefore is subject to several limitations. For one, it used searches based on coding, text strings, and product numbers, which may result in missed cases depending on the quality of data entry—and especially the consistent use of product names—by participating healthcare providers. Selection of characteristics for propensity score matching was based on existing literature, which may have its own limitations. Additionally, details of stapling firing information were not available from the database. We reported the differences in the incidence rates of blood transfusion in SDR and PVS groups based on a few controlled patient characteristics. Therefore, we could not confirm the causality of blood transfusion, but only described the association between stapling use and the outcomes. Future prospective clinical studies will be needed to confirm this study’s findings and to overcome the inherent limitations of observational database research. Finally, the authors’ conflicts of interest, which may introduce a potential source of bias, have been disclosed in the manuscript.
Conclusions
The study found that the narrow-profile SDR was an effective and beneficial tool for division and ligation during VATs lobectomy and is associated with fewer blood transfusions compared to PVS. Future clinical studies are needed to substantiate these findings and to account for variables not captured in this study, including surgeon-related factors, institutional practices, and clinical or laboratory values associated with the study outcomes.
Abbreviations
ICU, intensive care unit; PVS, powered vascular stapler; SDR, small-diameter reload; SOC, standard of care; VATS, video-assisted thoracoscopic surgery.
Ethical Conduct of Research Disclosure
This retrospective study was conducted in compliance with the Declaration of Helsinki. All patient data were from a fully de-identified database, and the study was determined exempt from full board review and informed consent requirements by Sterling IRB.
Acknowledgments
The author thanks Neetha Desai (Medronic PLC) for providing clinical and technical information regarding two studied products, and Jeanne McAdara PhD for professional medical writing support, which was funded by Medtronic PLC.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
IWP and ZAS are employees of Medtronic PLC. The authors report no other conflicts of interest in this work.
References
1. Alwatari Y, Khoraki J, Wolfe LG, et al. Trends of utilization and perioperative outcomes of robotic and video-assisted thoracoscopic surgery in patients with lung cancer undergoing minimally invasive resection in the United States. JTCVS Open. 2022;12:385–398. doi:10.1016/j.xjon.2022.07.014
2. McKenna RJ, Houck W, Fuller CB. Video-assisted thoracic surgery lobectomy: experience with 1,100 cases. Ann Thorac Surg. 2006;81(2):421–425; discussion 425–426. doi:10.1016/j.athoracsur.2005.07.078
3. Shimizu N, Tanaka Y, Okamoto T, Doi T, Hokka D, Maniwa Y. How to prevent adverse events of vascular stapling in thoracic surgery: recommendations based on a clinical and experimental study. J Thorac Dis. 2018;10(12):6466–6471. doi:10.21037/jtd.2018.11.14
4. Akopov A, Artioukh DY, Molnar TF. Surgical staplers: the history of conception and adoption. Ann Thorac Surg. 2021;112(5):1716–1721. doi:10.1016/j.athoracsur.2021.03.107
5. Molins L, Lanuti M, Force S, et al. Evaluation of a powered vascular stapler in video-assisted thoracic surgery lobectomy. J Surg Res. 2020;253:26–33. doi:10.1016/j.jss.2020.03.023
6. Chen B, Fan C, Tao L, Cui B. Clinical and economic benefits of patients undergoing lobectomy with the use of powered vascular staplers-based on China’s real-world data. J Med Econ. 2024;27(1):1499–1505. doi:10.1080/13696998.2024.2425250
7. Khandhar SJ, Desai NP, Anselme S, Shersher DD, Seder CW, Sanchez PG. A real-world study evaluating the safety and utility of a two-row stapler reload on pulmonary vasculature. J Thorac Dis. 2024;16(6):3753–3763. doi:10.21037/jtd-24-179
8. Miller DL, Roy S, Kassis ES, Yadalam S, Ramisetti S, Johnston SS. Impact of powered and tissue-specific endoscopic stapling technology on clinical and economic outcomes of video-assisted thoracic surgery lobectomy procedures: a retrospective, observational study. Adv Ther. 2018;35(5):707–723. doi:10.1007/s12325-018-0679-z
9. Zervos M, Song A, Li Y, Lee SH, Oh DS. Clinical and economic outcomes of using robotic versus hand-held staplers during robotic lobectomy. Innovations. 2021;16(5):470–476. doi:10.1177/15569845211040814
10. Shigeeda W, Deguchi H, Tomoyasu M, et al. Utility of the powered stapler for radical pulmonary resection: a propensity score-matched analysis. Surg Today. 2021;51(4):582–588. doi:10.1007/s00595-020-02154-9
11. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.