Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
A Comparative Analysis of Mobile versus Stationary Mammography Units: Performance and Outcomes in a Breast Cancer Screening Program
Authors Tari DU ![]() , De Lucia DR, Santonastaso R, Santarsiere M, Blasotti A
, De Lucia DR, Santonastaso R, Santarsiere M, Blasotti A
Received 31 January 2025
Accepted for publication 25 April 2025
Published 7 May 2025 Volume 2025:17 Pages 373—383
DOI https://doi.org/10.2147/BCTT.S516918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Daniele Ugo Tari,1 Davide Raffaele De Lucia,1 Rosalinda Santonastaso,2 Marika Santarsiere,1 Amedeo Blasotti3
1Department of Breast Imaging, District 12, Caserta Local Health Authority, Caserta (CE), 81100, Italy; 2Department of Economics, University of Campania “L. Vanvitelli”, Capua (CE), 81043, Italy; 3General Management, Caserta Local Health Authority, Caserta (CE), 81100, Italy
Correspondence: Daniele Ugo Tari, Department of Breast Imaging, District 12, Caserta Local Health Authority, Viale Paul Harris 79, Caserta (CE), 81100, Italy, Email [email protected]
Purpose: Breast cancer screening programs often encounter challenges related to high costs and limited accessibility, particularly in rural areas. Mobile mammography units (MMUs) have emerged as a potential solution to address these barriers. This study aimed to compare the outcomes of mammography screenings conducted in fixed units and MMUs, focusing on recall rates, follow-up adherence, and screen-detected breast cancer (BC) rates.
Patients and Methods: This retrospective study analyzed data from 790 women aged 50– 69 years who underwent mammography screening between January and February 2023. Participants were divided into two groups: group A (525 women, screened at fixed units) and group B (265 women, screened at MMUs). Key metrics included recall rates, biopsy rates, screen-detected BC rates, and refusal rates for follow-up evaluations. Statistical comparisons were made between the two groups to assess differences in outcomes.
Results: In group A (mean age 58.8 ± 5.7 years), the recall rate was 6.1%, with 32 recalls, 8 biopsies, and 7 confirmed BC cases, yielding a screen-detected BC rate of 1.33%. In group B (mean age 59.6 ± 5.8 years), the recall rate was higher at 10.6%, with 28 recalls, 5 biopsies, and 3 BC cases, resulting in a screen-detected BC rate of 1.13%. Notably, refusal rates for follow-up evaluations were significantly higher in group B (42.9%) compared to group A (9%).
Conclusion: While MMUs improve accessibility to underserved areas, they face challenges such as higher refusal rates for follow-up evaluations. The comparable screen-detected BC rates between MMUs and fixed units underscore the potential of combining both approaches in breast cancer screening programs. These findings highlight the importance of awareness campaigns to improve follow-up adherence and suggest that future research should focus on cost-effectiveness and sociocultural factors to optimize breast cancer prevention strategies.
Keywords: mobile unit, screening, digital breast tomosynthesis, telemedicine, mammography, breast density
Introduction
Breast cancer (BC) is a major global health issue and remains the leading cause of cancer-related deaths among women worldwide. In Italy, approximately 56,000 new cases are diagnosed annually, with an overall survival rate of 88%.1 Screening mammography has proven effective in reducing BC mortality by enabling early detection, though screening guidelines and practices vary by country, tailored to local resources and population needs. In Italy, BC screening was classified as an Essential Level of Assistance (L.E.A.) under the Prime Ministerial Decree (DPCM) of November 29, 2001,2 later updated by the DPCM of January 12, 2017.3 The European Society of Breast Imaging (EUSOBI) recommends biennial screening for women aged 50 to 69 with average risk. Once sufficient coverage for this group is achieved, extending the screening to women up to age 75 is suggested. Screening for women aged 40 to 49 is considered a lower priority and should be conducted annually if implemented, given the faster progression of breast cancer in this age group.4
Advances in early detection and improvements in surgical and medical treatments have contributed to increased survival rates. However, regional disparities persist within Italy. Indeed, women in Southern Italy face disadvantages, including lower survival rates (85%) compared to the North (88%), with higher adherence to screening (60%) observed in the northern regions.1 These disparities stem not from treatment quality but from delayed diagnosis, often due to limited awareness about the importance of early detection and inadequate or poorly implemented screening programs. The lack of sufficient human and technological resources, coupled with limited access to screening services due to distance or cost, further exacerbates this issue.5
To address these challenges, mobile mammography units (MMUs) have been introduced to bring screening services closer to underserved communities. They, typically consisting of vans or traveling clinics equipped with diagnostic tools and staffed by healthcare workers (HCWs), offer a flexible and accessible alternative to fixed clinics aiming to enhance community participation in screening programs, by reducing travel time and increasing convenience.6,7 Although initial setup costs for MMUs can be high, long-term savings are possible due to the absence of rental expenses.6,7 Furthermore, they have proven effective in reaching both working and nonworking women, particularly benefiting older women over the age of 60 who may face mobility challenges.8
Their importance has been underscored during the COVID-19 pandemic, which disrupted preventive healthcare services, including BC screening. As resources were diverted to COVID-19 management, BC screenings were delayed, and fewer new cases were diagnosed. This decline may also be attributed to patients avoiding hospitals due to fears of infection.9 As a result, the need for more accessible screening methods has become increasingly urgent, with MMUs emerging as a viable solution to enhance participation rates.10
This study aims to assess the impact of mobile mammography units within a breast cancer screening program in Southern Italy, considering both their outcomes and potential limitations.
Materials and Methods
Study Design
We retrospectively compared the breast cancer screening examinations of women aged between 50–69 years, who were invited to undergo a BC screening mammography using digital breast tomosynthesis (DBT) and 2D synthetic reconstructed views (2Ds) at the Department of Breast Imaging, District 12, Caserta Local Health Authority (Group A), during the period from January to February 2023. These were compared with the examinations of women living in area without access to screening facilities, who were invited to undergo BC screening DBT with 2Ds at MMU (Group B).
The fixed unit was equipped with a Hologic Selenia Dimensions Mammograph (Hologic, Bedford, MA, USA) while the mobile unit was equipped with an IMS Giotto Class Mammography (IMS Giotto, Sasso Marconi, BO, ITA). In both cases, images were acquired in double projections, medio-lateral-oblique (MLO) and cranio-caudal (CC), for each breast. Before the exam, a nurse or a radiographer interviewed the patients with the aim of compiling the medical record with the anamnestic data essential for assessing the risk of breast cancer.
All the data were recorded in the Sani.ARP web portal, the Caserta LHA reporting database. Images acquired at the stationary unit were stored directly in the Picture Archiving and Communication System (PACS) at the breast center. Images taken at the mobile unit were stored on a portable secure storage drive and taken to the breast center, where they were transferred to the PACS.
The same group of radiologists conducted both the screen-reading and recall assessments for all women participating in the study. Two radiologists independently double read all screening examinations, according to ACR BI-RADS lexicon 5th Edition for findings and density evaluation (BD).11 BD has been evaluated with Quantra software version 2.2.3.12 BI-RADS assessment categories A and B were considered non-dense, and categories C and D were considered dense.
We excluded examinations that did not include exactly the four standard mammographic images and examinations of women with breast implants due to BC surgery or breast augmentation (stationary n:8; mobile n:2) (Figure 1).
 |
Figure 1 Study design. Group A: women performed digital breast tomosynthesis (DBT) on stationary unit. Group B: women performed DBT on mobile mammography units (MMUs). PACS: Picture Archiving and Communication System. Breast density has been evaluated with Quantra software version 2.2.3 according to BIRADS 5th Edition. |
Early performance measures included the rate of recall, the screen-detected breast cancer, and the positive predictive value of recalls and needle biopsies, as well as histopathologic tumor characteristics. These included tumor diameter (<10 mm, 10–20mm and >20 mm), histologic grade (1, 2 and 3), lymph node involvement (positive/negative), and estrogen receptor (%), progesterone receptor (%), human epidermal growth factor receptor 2 status (positive/negative) and Ki-67 proliferation index.
We employed the International Academy of Cytology (IAC) Yokohama System for Reporting Breast Fine-Needle Aspiration Biopsy Cytopathology (1st Edition, 2020) to classify FNAC findings. The system categorizes results as follows: C1 - insufficient/inadequate; C2 - benign; C3 - atypical; C4 - suspicious for malignancy; and C5 – malignant.13 We employed the Guidelines for non-operative diagnostic procedures and reporting in breast cancer screening to classify CNB and VABB findings. This system categorizes results as follows: B1 – normal breast tissue; B2 – benign (not cancer); B3 – abnormal or uncertain but probably benign; B4 – suspicious and possibly cancer; B5 – cancer.14
Statistical Analysis
A sample size estimation has been performed to evaluate if the number of patients enrolled in each group was sufficient to ensure reliable results. We used an assumed effect size of 0.3 (representing a small to medium effect), a significance level (α) of 0.05, and a statistical power of 80%. This analysis determined that a minimum of 175 observations per group was required to reliably detect meaningful differences.
Descriptive statistics were used to compare distributions of age, breast density and early performance measures, including histopathologic tumor characteristics, stratified by stationary and mobile screening unit. We presented means and standard deviation. We applied the Shapiro–Wilk test to evaluate the normality of age distributions for participants in the stationary and mobile mammography units.
A Kolmogorov–Smirnov test was subsequently used to compare differences in the age distribution between group A and B.
To compare the distribution of density between the two groups and to examine the relationship between age and density both overall and within each group, a Chi-square test, a Kruskal–Wallis test, and Spearman correlation were applied, respectively.
A Fisher’s exact test and a Z-test were employed to compare the biopsy rate, detection rate (DR) and positive predictive value rates (PPV), respectively.
The recall rate was defined as the proportion of women recalled due to abnormal mammographic findings. The biopsy rate referred to the proportion of needle biopsies performed during recall assessments. The rate of screen-detected breast cancer was measured as the number of breast cancer cases diagnosed following a recall, relative to the total screening examinations. PPV of recalls was the percentage of screen-detected breast cancer cases among all recalls, while the PPV of needle biopsies represented the percentage of screen-detected breast cancer cases identified through biopsies performed during recall assessments. The statistical analysis was conducted using STATA version 13 (Stata Corp, TX), and the results were visualized through boxplots, kernel density estimates (KDE), and frequency histograms to illustrate age distributions, density patterns, and frequency trends. A p-value of <0.05 was considered statistically significant.
Results
A total of 790 BC screening examinations were retrospectively evaluated. Of these, 525 were women aged between 50–69 years old (58.8 ± 5.7) who underwent BC screening with digital breast tomosynthesis (DBT) at the Department of Diagnostic Senology District 12, Caserta Local Health Authority (LHA), from January to February 2023 (Group A); 265 were women in the same age range (59.7 ± 5.4) who underwent BC screening with DBT at the MMU of Caserta LHA (Group B) in the same period. We excluded 8 women from Group A and 2 women from Group B.
The current sample sizes, comprising 527 observations for group A and 265 observations for group B, exceed the threshold of the required observations, confirming that the study is sufficiently powered to identify statistically significant effects. While the fixed group’s larger sample size provides additional statistical robustness, the imbalance in group sizes does not compromise the validity of the analysis, as both groups exceed the minimum requirement for adequate power.
Characteristics of both groups are reported in Table 1.
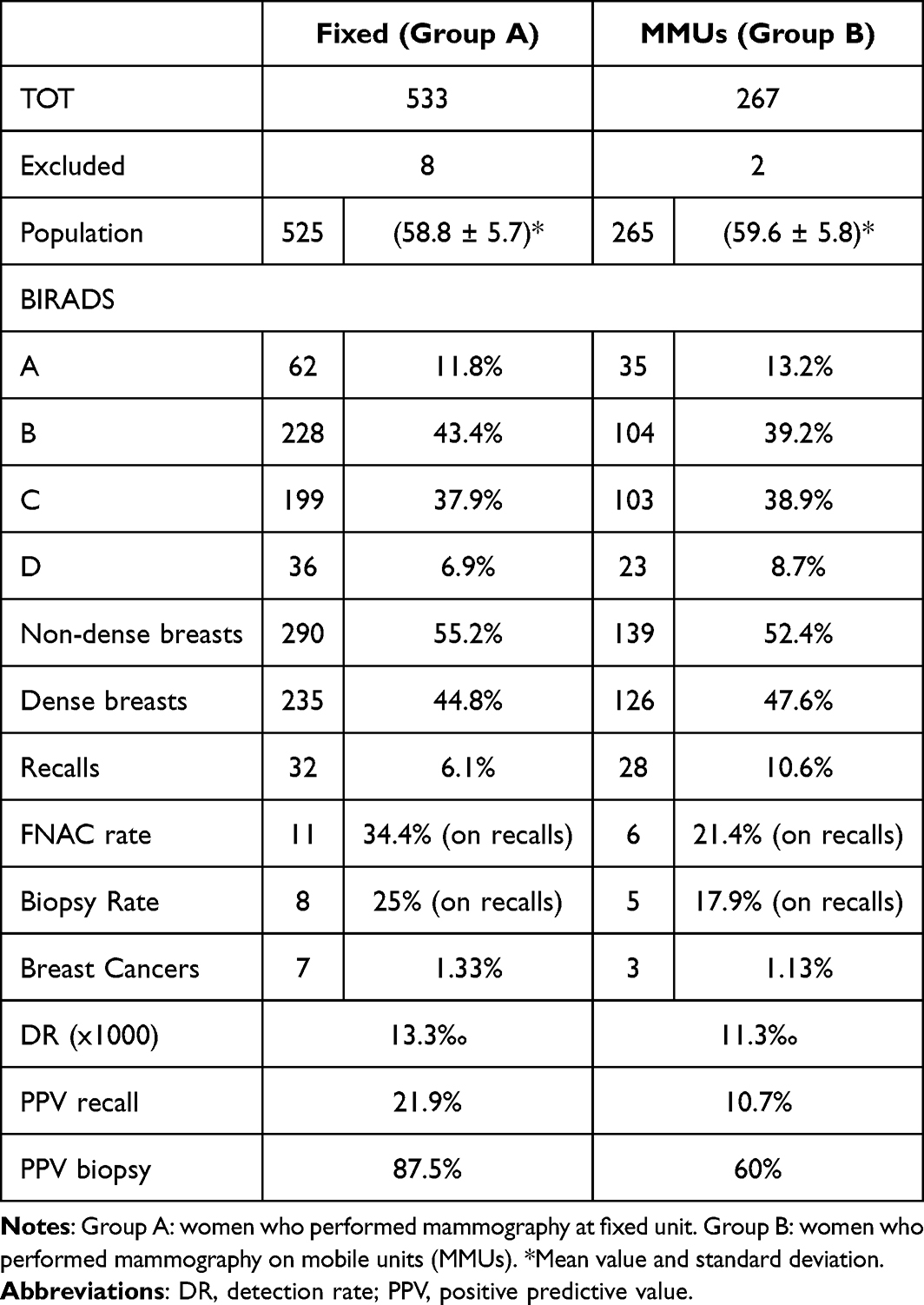 |
Table 1 Population and Results |
In group A, 454 women already underwent screening mammography in the last two years (86.5%) and 32 women were recalled for further evaluations (BI-RADS category > 3). Of these, 5 underwent magnetic resonance imaging (MRI) and 13 underwent ultrasounds (US) resulting in negative or benign findings; 11 performed fine-needle aspiration cytology (FNAC) with 8 subsequent core-needle biopsies (CNB). We finally diagnosed 6 cases of breast cancer and 1 atypical ductal hyperplasia (ADH) who showed foci of ductal carcinoma in situ (DCIS) at surgery. The recall rate was 6.1% with a biopsy rate of 34.4% (25% CNB) and a rate of screen-detected BC of 1.33%. The PPV of recalls was 21.9% while the PPV of needle biopsies was 87.5% for CNB. With regards to the breast density, radiologists classified 62 women as category A, 228 as B, 199 as C and 36 as D. Consequently, we founded 290 women categorized with non-dense breasts and 235 with dense breasts. The highest number of recalls was founded in the dense breast group (22 women; 68.8% of recalls). Nevertheless, among recalls, 3 women (59.3 ± 8.5 years; median: 56) with suspicious findings refused to perform second level examinations (9%) (Table 2).
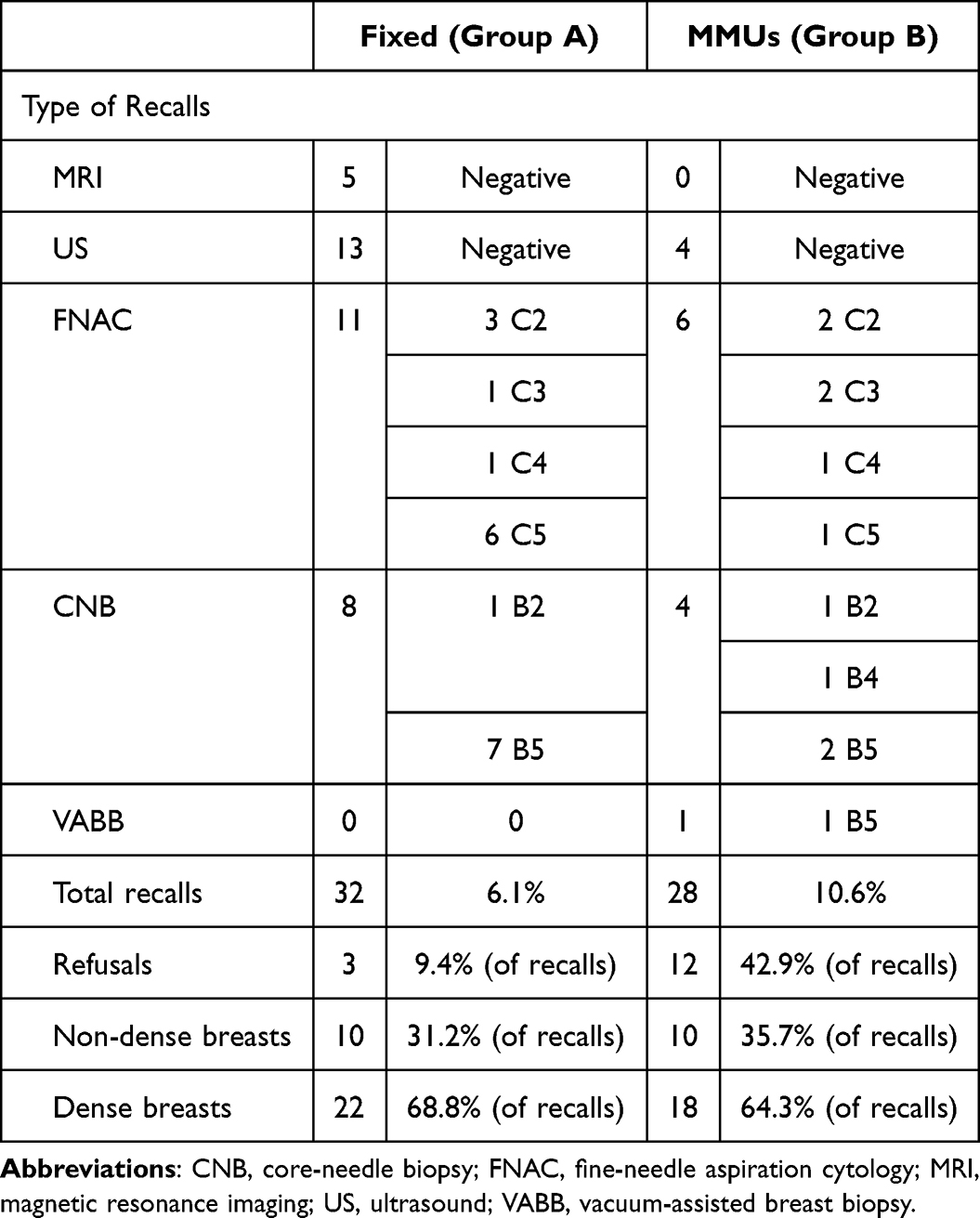 |
Table 2 Recalls and Refusals. Type of Recalls and Findings |
In group B, 132 women already underwent screening mammography in the last two years (49.8%) and 28 women were recalled for further evaluations (BI-RADS category > 3). Of these, 9 underwent ultrasounds (US) resulting negative or with benign findings; 6 performed FNAC with 4 subsequent CNB and 1 performed directly a tomosynthesis-guided vacuum-assisted breast biopsy (VABB). By the end of these examinations, we diagnosed 3 BC and 1 ADH. The recall rate was 10.6% with a biopsy rate of 17.9% (21.4% of CNB/VABB) and a rate of screen-detected BC of 1.13%. The PPV of recalls was 10.7% while the PPV of needle biopsies was of 60% for CNB/VABB. With regards to the breast density, radiologists, classified 35 women as category A, 104 as B, 103 as C and 23 as D. Consequently, we founded 139 women with non-dense breasts and 126 with dense breasts. The highest number of recalls was founded in the dense breast group (18 women; 64.3% of recalls). Nevertheless, among recalls, 12 women (59.79 ± 6.6 years; median: 60) refused to perform second level examinations (42.9%) (Table 2). Of these, 7 had doubtful findings classified as BI-RADS 3 and 5 had suspicious findings classified as BI-RADS 4 according to BI-RADS 5th Edition lexicon.11
Types of recalls are reported in Table 2. Histopathological characteristics of BC are reported in Table 3.
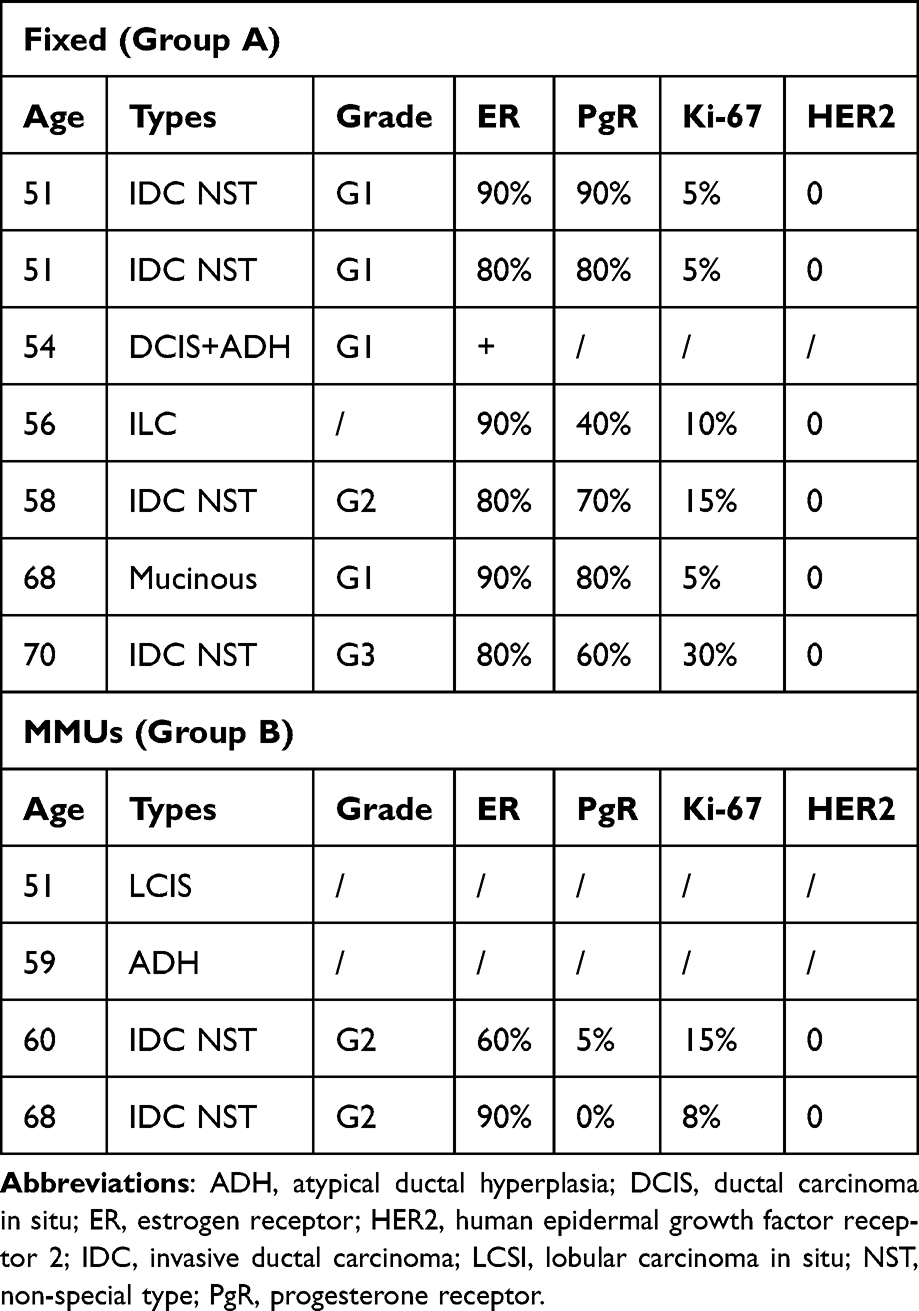 |
Table 3 Final Findings. Characteristics of Findings in Both Groups After Surgery with Prognostic Factors |
Group B exhibits the highest recall rate, while both groups demonstrate comparable percentages of breast cancer diagnoses and detection rates. The highest number of recalls has been performed for women with dense breasts in both groups. Group B has the highest rate of refusal.
The results of the Shapiro–Wilk test for each group (A: 0.9533, p-value < 0.05; B: 0.959, p-value < 0.05) indicate that the age distributions in both the stationary and mobile units deviate significantly from normality. This suggested the use of non-parametric tests for further evaluation. The Kolmogorov–Smirnov test (KS Statis-tic: 0.111; p-value: 0.024) indicated a statistically significant difference in the age distribution between group A and B. These findings suggested that while both groups shared close age characteristics, the MMUs group had a higher central age, and the age distribution patterns differed significantly. We illustrated these results in Figures 2, 3A and B. The boxplot (Figure 2) shows the age distribution for each group. Each box represents the interquartile range, with the central line indicating the median. This plot allows a comparison of the spread and central position of ages in each group, highlighting the differences in variability and outliers.
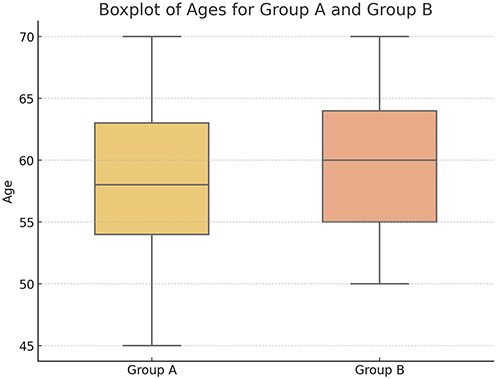 |
Figure 2 Boxplot of ages. Group A: stationary unit. Group B: mobile mammography units. Median: 58 (group A), 60 (group B); First quartile: 53 (A), 54 (B); Third quartile: 63 (A), 64 (B). |
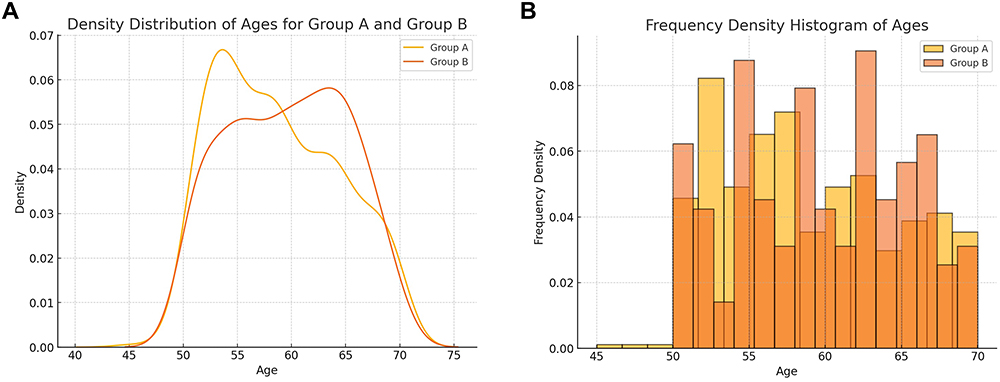 |
Figure 3 (A) KDE (Kernel Density Estimation): density distribution of ages for each group. (B) Frequency density histogram of ages for each group. The y-axis represents frequency density, ensuring that the total area under each histogram equals 1. The density values indicate the relative proportion of individuals per unit of age. |
The Kernel Density Estimation (KDE) plot (Figure 3A) and the frequency density histogram (Figure 3B) illustrate the age distributions for the two groups. In the KDE plot, differences in the shapes of the distributions are evident. Group A exhibits a slightly broader distribution with a higher peak density, indicating a greater concentration of ages around its most frequent range, whereas group B has a lower peak density, suggesting a more evenly distributed range of ages, albeit with a pronounced peak in certain age intervals.
In the frequency density histogram, the distributions are normalized to allow for direct comparison irrespective of sample size. It further emphasizes that group A spans a broader range of ages, while group B displays a tighter concentration around specific age ranges. These findings suggest potential demographic differences between the two groups.
The comparison of density evaluation for each group was performed as follows. The Chi-square test compared the distribution of density between the two groups. With a p-value of 0.606, we concluded that there was no statistically significant difference. The Kruskal–Wallis test obtained a very low p-value (1.97×10−5) for group A and a p-value of 0.126 for group B. This suggested that the ages varied significantly with the breast density in the fixed unit group while there was no significant difference in age distribution across density categories within the MMUs group. Finally, the Spearman’s Rank Correlation showed a low p-value for both groups (1.05×10−5 for group A, 0.021 for group B). This suggests an inverse association between age and breast density in both groups, with the association being weaker in the mobile units group compared to the fixed unit group. To complete this analysis, we provide a boxplot for ages across density categories within each group (Figure 4). These visualizations confirm the findings, showing a more distinct age-dependent variation in density levels within the fixed unit group than in the MMUs group.
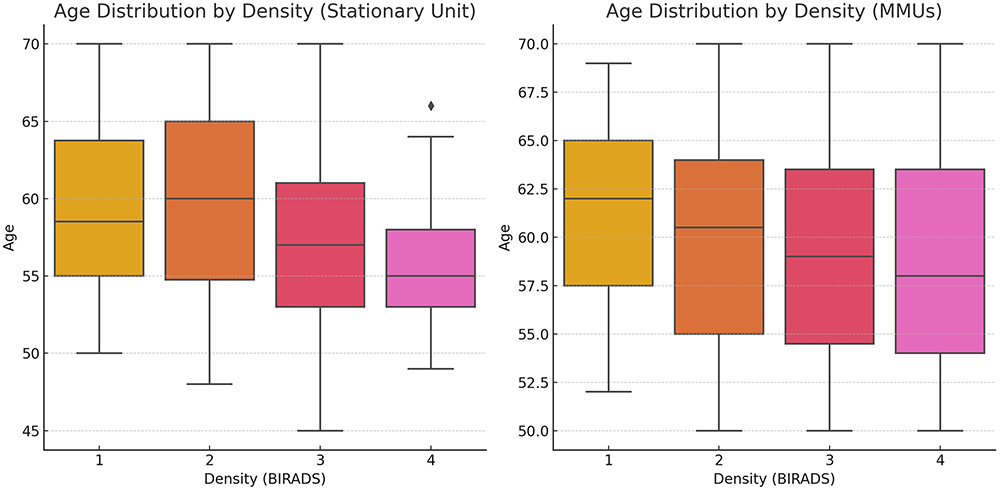 |
Figure 4 Boxplot showing the age distribution by density. The fixed unit group is displayed on the left, and the mobile mammography units (MMUs) group on the right. Age is expressed in years, and density is categorized according to BIRADS (5th Edition). |
The results of the statistical evaluation for biopsy rates (p: 0.77), DR (p: 0.81), PPV Recall (p: 0.25) and PPV Biopsy (p: 0.25) showed no-statistical significance. Consequently, these results suggest that, from a statistical point of view, the two screening modalities may be similar in performance. Indeed, there is not enough statistical evidence to assert that the breast cancer detection rate is different between the fixed and mobile units. Although the absolute numbers are slightly different (13.3‰ for the fixed units and 11.3‰ for the MMUs), this difference could be due to chance rather than a true difference in the performance of the two screening modalities. Even though the PPV of recalls is higher in the fixed unit group (21.9% vs 10.7%), the statistical test indicates that this difference is not significant enough to conclude that one group has a significantly better PPV. Similarly, there is not sufficient statistical evidence to assert that the PPV of biopsies is significantly different between the two groups (87.5% for the fixed unit group vs 60.0% for the mobile group). In other words, while there are some numerical differences in the results between the two groups, the statistical tests indicate that these differences could be due to chance and are not strong enough to be considered real or clinically relevant differences. Therefore, it cannot be confidently stated that one of the two methods (fixed or mobile units) is significantly better than the other in terms of DR or PPV.
Discussion
The implementation of screening and early detection programs is a fundamental aspect of cancer prevention. However, despite clear evidence that early detection saves lives, significant global disparities in access to these services remain.15 Common barriers to cancer screening include limited availability of healthcare providers, inadequate community access to screening facilities, and low demand for screening within communities.16 In certain rural areas of Southern Italy, access to screening clinics is often hindered by high costs, long travel distances, inconvenient operating hours, and limited awareness of available services. Additionally, many women lack knowledge about the importance of early diagnosis, do not perceive themselves as being at risk, or avoid screenings due to fear of the results. In our experience, MMUs showed a high potential to improve BC screening, even though they reiterated certain limitations of both logistical and social nature.
From a statistical perspective, the fixed and mobile units performed similarly, with nearly identical detection rates (DR). Additionally, there was no significant difference in the distribution of density categories between the two groups, even if the association between age and density was more pronounced in the stationary unit group. This latter factor is particularly important, as breast density (BD) is widely recognized as an independent risk factor for breast cancer and its assessment is crucial.14 Indeed, the study confirmed that age and BD are inversely correlated, with younger women having denser breasts and older women having more non-dense breasts.
Moreover, our findings suggested that while both groups shared close age characteristics, group B has a higher central age (Figure 2), and the age distribution patterns differed significantly (Figure 4). Comparing the age distribution by density, our study showed a more distinct age-dependent variation in density levels within group A than in group B (Figure 4). This aspect could justify the higher recall rate and lower positive predictive value (PPV) for biopsies in the MMUs group. In contrast to these findings, Holen et al17 reported a lower recall rate for MMUs. However, in their study, the proportion of highly dense breasts was greater in the stationary units than in the mobile ones, which could explain the different findings. Another factor to consider is that we used two different mammography machines for the mobile unit and the fixed unit, which may have affected the readers’ confidence and, consequently, the recall rate. Finally, the absence of prior examinations and the lack of direct radiologist supervision during the exams may have contributed to an increase in unnecessary recalls.18 Since teleradiology has been shown to be effective for screening reports without compromising image quality,19 a centralized reporting system, with all mammograms processed via double-blind review, has demonstrated efficiency in improving reporting. This system reduced the turnaround time to less than 10 days and lowered recall rates from over 70%.20
MMUs decreased the distance and travel time needed to perform the examinations. They have also been able to generate significant participation among women, and they were effective in detecting abnormalities on screening examinations.7 Guillaume et al demonstrated that the participation rate for women living more than 20 km from a radiologist’s office was much higher when mobile units were available.21 This aspect is particularly relevant in our territory where the screening facilities are not easily reachable from some rural areas for geographical reasons.
MMUs have been also associated with poor follow-up rates.6 This aspect was confirmed by our study, which showed a higher percentage of refusal among mobile than fixed units, at 42.9% versus 9.4%, respectively. This result may be related also to the disparity between the number of women who underwent screening mammography in the last two years (49.8% in group B versus 86.5% in group A). Conversely, the markedly lower rate of prior participation among women accessing mobile units underscores their critical role in engaging under-screened populations who might otherwise remain unreached by conventional programs. Vang et al18 showed that also MMUs can face barriers to screening, such as concerns about cost, mammogram-related pain, and fear of receiving bad news – challenges that are especially common among women in rural areas. However, in our territory, women’s perception of screening may be limited in both rural and urban settings, due to a general lack of knowledge about the importance of early diagnosis, which ultimately affects overall participation rates.
In our study, the two groups have similar but significantly different age distribution and mean ages with mobile units’ group having a slightly higher average age. Analyzing the characteristics of women who refused to undergo further investigations, and acknowledging the limited number of observations, women in the MMUs group were older than those in the fixed unit group (median age 60 vs 56). This aspect may have impacted the mobility of older women, who may have faced difficult in accessing the screening facilities for second-level examinations.
Consequently, to overcome these limitations, additional strategies should be considered.
Patient navigation refers to a support system designed to help patients overcome barriers to accessing healthcare services that can include social, economic, cultural, and logistical challenges: lack of information, language difficulties, transportation issues, and fear or anxiety about diagnosis. A patient navigator assists individuals in navigating the healthcare system, ensuring they receive the necessary screenings, follow-up care, and treatments. This approach has proven especially effective for underserved populations, such as women in rural areas or minority groups, by improving adherence to screening programs and reducing health disparities.20,21
Many mobile users underestimated their risk, which affected their likelihood to participate in screening and follow-up. Providing culturally appropriate education could help improve these outcomes. McElfish et al22 demonstrated that both mobile units and community events without MMUs are effective in increasing screening participation. However, women recruited through mobile units tended to have lower educational levels; approximately 58.8% of them had a high school education or less, compared to 24.8% from community events. We believe that combining these two recruitment methods could be a key step toward better addressing the issue. Recruitment through community events – such as sports events, church gatherings, health fairs, and workplace wellness programs – organized in collaboration with community members can also be beneficial in rural areas. Staff and volunteers could approach women as they pass by the booth and invite them to undergo a screening exam directly on the mobile units.
Our study has some limitations. Although the sample size estimation indicated that the sample sizes were sufficient to ensure reliable results, the single-center nature of the study may limit the generalizability of the findings. Additionally, different mammography units were used for the MMUs and the fixed clinic. Although both were high-quality machines capable of performing digital breast tomosynthesis (DBT), the quality of the images may have influenced the interpretation by different readers, potentially impacting the recall rate. Finally, limited access to individual socio-economic data may have affected the outcomes.
Our study demonstrated a higher detection rate compared to previous research, highlighting the success of this screening approach and providing a strong foundation for further investigation. Additionally, the comparable performance of MMUs and fixed units underscores their effectiveness and adaptability, making both viable options for breast cancer screening, depending on accessibility and community needs.
Future research should stratify results by factors such as cost-effectiveness, socio-economic background, education levels, reasons for non-adherence to screening programs, and refusal of second-line examinations. This would support the development of more targeted and effective prevention strategies, ultimately improving breast cancer screening outcomes.
Conclusion
Mobile Mammography Units provide versatile solutions for delivering essential screening services in both urban and rural areas. To enhance their effectiveness, well-equipped vans combined with targeted awareness campaigns prior to deployment could significantly improve participation rates. In instances where a radiologist is unavailable during screenings on mobile units, a centralized reporting system should be implemented to minimize unnecessary recalls. For rural areas located more than 20 km from fixed clinics, onsite second-level ultrasound examinations are recommended. This approach ensures that only women requiring biopsies or advanced evaluations are referred to specialized breast imaging departments.
Ethics and Consent Statements
The Study was conducted according to the guidelines of the Declaration of Helsinki. According to Italian regulations (Ministerial Decree of December 17, 2004) and the guidelines issued by the Italian Medicines Agency (AIFA), the Institutional Review Board’s approval is not required, considering the retrospective nature of the study. Informed consent has been obtained from the patient(s) to participate in this research.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. AIRTUM Working Group; AIOM Working Group; PASSI Working Group; SIAPEC-IAP Working Group. I Numeri del Cancro in Italia.
2. Presidente del Consiglio dei ministri. Decreto “Definizione dei livelli essenziali di assistenza” 29 novembre 2001. GU Serie Generale n.33 del 08-02-2002 - Suppl. Ordinario n. 26.
3. Presidente del Consiglio dei ministri. Decreto “Definizione e aggiornamento dei livelli essenziali di assistenza, di cui all’articolo 1, comma 7, del decreto legislativo 30 dicembre 1992, n. 502. (17A02015)”, 12 gennaio 2017. GU Serie Generale n. 65 del 18-03-2017 - Suppl. Ordinario n. 15.
4. Tari DU. Chapter 17 - Guidelines for breast imaging in the COVID-19 pandemic. In: Rajendram R, Preedy VR, Patel VB, Martin CR, editors. Management, Body Systems, and Case Studies in COVID-19. London, UK: Academic Press; 2024:187–199. doi:10.1016/B978-0-443-18703-2.00015-3
5. Tari DU, Santarsiere A, Palermo F, Morelli CD, Pinto F. The management of a breast unit during the COVID-19 emergency: a local experience. Future Oncol. 2021;17:4757–4767. doi:10.2217/fon-2021-0243
6. Trivedi U, Omofoye TS, Marquez C, Sullivan CR, Benson DM, Whitman GJ. Mobile mammography services and underserved women. Diagnostics. 2022;12:902. doi:10.3390/diagnostics12040902
7. Gold RH, Bassett LW, Widoff BE. Highlights from the history of mammography. Radiographics. 1990;10:1111–1131. doi:10.1148/radiographics.10.6.2120679
8. Vellozzi CJ, Romans M, Rothenberg RB. Delivering breast and cervical cancer screening services to underserved women: Part I. Literature review and telephone survey. Womens Health Issues. 1996;6:65–73. doi:10.1016/1049-3867(96)80028-5
9. Tari DU, Santonastaso R, Pinto F. Consequences of the impact of COVID-19 pandemic on breast cancer at a single Italian institution. Explor Target Antitumor Ther. 2022;3:414–422. doi:10.37349/etat.2022.00091
10. Cancino RS, Su Z, Mesa R, Tomlinson GE, Wang J. The impact of COVID-19 on cancer screening: challenges and opportunities. JMIR Cancer. 2020;6:e21697. doi:10.2196/21697
11. Sickles EA, D’Orsi CJ, Bassett LW, et al. ACR BI-RADS mammography. In: D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA, editors. ACR BI-RADS Atlas, Breast Imaging Reporting and Data System.
12. Tari DU, Santonastaso R, De Lucia DR, Santarsiere M, Pinto F. Breast density evaluation according to BI-RADS 5th Edition on digital breast tomosynthesis: AI automated assessment versus human visual assessment. J Pers Med. 2023;13(4):609. doi:10.3390/jpm13040609
13. Field AS, Raymond WA, Rickard M, et al. The international academy of cytology Yokohama system for reporting breast fine-needle aspiration biopsy cytopathology. Acta Cytol. 2019;63:257–273. doi:10.1159/000499509
14. Lee AHS, Carder P, Deb R, et al. Guidelines for Non-Operative Diagnostic Procedures and Reporting in Breast Cancer Screening. London, UK: The Royal College of Pathologists Publications G-150; 2021.
15. Greenwald ZR, El-Zein M, Bouten S, Ensha H, Vazquez FL, Franco EL. Mobile screening units for the early detection of cancer: a systematic review. Cancer Epidemiol Biomark Prev. 2017;26:1679–1694. doi:10.1158/1055-9965.EPI-17-0451
16. Brooks SE, Hembree TM, Shelton BJ, Beache SC, Aschbacher G, Schervish PH. Mobile mammography in underserved populations: analysis of outcomes of 3,923 women. J Community Health. 2013;38:900–906. doi:10.1007/s10900-013-9690-9
17. Holen Å, Sebuødegård S, Waade GG, et al. Screening at stationary versus mobile units in BreastScreen Norway. J Med Screen. 2020;27(1):31–39. doi:10.1177/0969141319875158
18. Vang S, Margolies LR, Jandorf L. Mobile mammography participation among medically underserved women: a systematic review. Prev Chronic Dis. 2018;15:E140. doi:10.5888/pcd15.180291
19. Fruehwald-Pallamar J, Jantsch M, Pinker K, et al. Teleradiology with uncompressed digital mammograms: clinical assessment. Eur J Radiol. 2013;82(3):412–416. doi:10.1016/j.ejrad.2012.03.004
20. Gultekin M, Ozturk C, Karaca S, et al. Centralization of mammography reporting with mobile trucks: turkish experience. Prev Med Rep. 2018;10:317–322. Erratum in: Prev Med Rep. 2020; 20:101282. doi:10.1016/j.pmedr.2020.101282. doi:10.1016/j.pmedr.2018.04.008
21. Guillaume E, Launay L, Dejardin O, et al. Could mobile mammography reduce social and geographic inequalities in breast cancer screening participation? Prev Med. 2017;100:84–88. doi:10.1016/j.ypmed.2017.04.006
22. McElfish PA, Su LJ, Lee JY, Runnells G, Henry-Tillman R, Kadlubar SA. Mobile mammography screening as an opportunity to increase access of rural women to breast cancer research studies. Breast Cancer. 2019;13:1178223419876296. doi:10.1177/1178223419876296
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.