Back to Journals » Substance Abuse and Rehabilitation » Volume 13
A Community-Based Study of Level and Determinants of Substance Use: Findings from Children Experiencing Homelessness in Major Cities of Northern Ethiopia
Authors Asfaw Z ![]() , Mitiku M, Abebe HT
, Mitiku M, Abebe HT ![]() , Atsbeha MT
, Atsbeha MT
Received 15 July 2022
Accepted for publication 18 November 2022
Published 28 November 2022 Volume 2022:13 Pages 101—110
DOI https://doi.org/10.2147/SAR.S381768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Stephan Arndt
Zinabu Asfaw,1 Mengistu Mitiku,2,3 Haftom Temesgen Abebe,2,4 Mussie Tesfay Atsbeha5
1Department of Public Health, Adigrat University, Adigrat City, Tigrai, Ethiopia; 2School of Public Health, Mekelle University, Mekelle City, Tigrai, Ethiopia; 3Research and Community Engagement Coordination Office, Mekelle University, Mekelle City, Tigrai, Ethiopia; 4Laboratory Interdisciplinary Statistical Data Analysis, Mekelle University, Mekelle city, Tigrai, Ethiopia; 5School of Medicine, Mekelle University, Mekelle City, Tigrai, Ethiopia
Correspondence: Zinabu Asfaw, Department of Public Health, Adigrat University, P.O. Box: 50, Adigrat City, Ethiopia, Email [email protected]
Background: Homelessness among children is a significant problem in most nations of the world. Children who experienced homelessness are most often unable to get secured and adequate housing. Such problems expose them to a range of destructive practices such as substance use. This study, therefore, was designed to evaluate the level and determinants of substance use by children who experienced homelessness in major cities of Northern Ethiopia.
Methods: This cross-sectional study was undertaken from October 1, 2019 to February 30, 2020. We conducted street-based outreach searching to get a representative sample of the city’s children who experienced homelessness and a total of 422 were recruited. The collected data were analyzed using SPSS version 20. Regression analysis was done to identify factors associated with substance use and statistical significance was declared at p < 0.05 and 95% confidence interval.
Results: More than 80% of the children who experienced homelessness use alcohol, cigarette or chat. Marriage status of parents before the child experiences homelessness being divorce (AOR = 8.53, 95% CI: 1.87– 38.89), occupational status of mother being a daily laborer (AOR = 2.78, 95% CI: 0.83, 9.31), child relationship status with parents before child experiences homelessness (AOR = 0.08, 95% CI: 0.02– 0.30) and parents’ residential status before child experiences homelessness being rural (AOR = 5.63, 95% CI: 1.77– 17.89) are the independent variables that established statistically significant association with the outcome variable, substance use.
Conclusion and Recommendation: The majority of the children who experienced homelessness are exposed to substance use, particularly alcohol and cigarette. Efforts are needed by concerned bodies of the region to work on factors that predispose to homelessness and strategically safeguard the health and wellbeing of the children.
Keywords: homelessness, substance use, children, Northern Ethiopia
Introduction
Child is defined as “a human being below the age of 18 years unless under the law applicable to the child, majority is attained earlier”. This definition is approved by 192 of 194 member countries of the United Nations.1 Currently, the number of children who experienced homelessness and therefore live in unsafe places is increasing. A report by the World Health Organization indicated that as many as 100 million children live in streets of the world.2 In Europe, homelessness among the general population where the majorities are children is as low as 0.01% in Croatia and as high as 3.73% in Bosnia Herzegovina. Unlike the developed world, countries in Africa like Guinea have a huge ratio (68.5%) of people experiencing homelessness, with children representing a significant share.3
Child homelessness is a serious social problem facing the globe in general and the least developed nations in particular. For this reason, homelessness is exposing children to many problems such as severe substance use. Globally, around 90% of children who experienced homelessness consume substances such as cigarettes and alcohol4,5 though it is the setting or geographical location that could determine the type of substance to be used. As a result, the substances used by street children differ from one country to another. A systematic review of studies indicated that children from low- and middle-income countries who experienced homelessness use substances such as alcohol and cigarette unlike children from high-income countries which usually use substances in the form of injecting drugs.6
Studies from Africa showed different levels of substance use by children who experienced homelessness. A cross-sectional study of street children in Kenya revealed that current substance use is 83%.7 Likewise, a study from Democratic Republic of Congo reported that 82% and 63.5% of street children use marijuana and alcohol, respectively.8 An Egyptian study also indicated that 62% of children who experienced homelessness use alcohol and 3% use substance in the form of drug injection.9
In Ethiopia, there is high level of child homelessness which finally ends up with consumption of harmful substances. Reports showed that cigarette and alcohol use among street connected children is high.10,11 A recently conducted cross-sectional study in Bahir Dar, Ethiopia, indicated that level of substance use among youth who experienced homelessness is 55.8%.12
Substance use is usual way to freeze the day-to-day bad events that children who experienced homelessness face while leading their life on the streets and usually helps them reduce any worry they are confronted with.13 The worry that they face from napping and sleeping in unsecured shelter-like places is relieved by taking substances like alcohol and cigarette to sustain their energy and movement and quash starvation.14 Moreover, alcohol, cigarettes, and other substances may be consumed by these not fully formed and undeveloped individuals to keep them active for a prolonged period of time.14,15
Substance use affects the physical as well as filling the inner life of children who experienced homelessness children with false signals and meanings. Generally, substance use results in legal problems as there are certain substances which produce illegal wrongdoing, financial, social, medical and daily responsibilities related problems.16
Different factors are found to be associated with substance use among children who experienced homelessness. It is believed that poverty and unwise family norms in parenting are decisive factors for children to experience homelessness. Child connectedness with family brings about strong association which in turn helps the child develop safer behaviors.17–19 However, there are inconsistencies with regard to a couple of variables. For example, study findings revealed that substance use in combination with sex takes individuals to risky sexual practices. However, other investigations of the relation between risky sexual practice and substances utilization had shown different findings.20,21 Health problems such as depression and nervousness usually force children and young individuals to use alcohol and other substances and therefore consider them as treatments.22
Reports of the Ethiopian government indicated that as many as 150,000 children who experienced homelessness and around 50% are from Addis Ababa, the capital city of Ethiopia. But, other reports are confidently indicating that Ethiopia has more than half a million children living on streets and other unsecured buildings.23,24
Despite the presence of an alarming level of homelessness among children in Ethiopia, no formal and meaningful efforts were made to alleviate the problem.25 For this reason, the subject of homelessness is believed to be getting worse and factors associated remain still unclear. Hence, our study was planned to evaluate the level of substance use and its associated factors among children experiencing homelessness in major cities of Tigrai, northern part of Ethiopia.
Methods
Study Setting and Study Design
This study was undertaken in the major cities of Tigrai region, northern part of Ethiopia from October 1, 2019 to February 30, 2020. The major cities of the region, in addition to Mekelle city, are: Adigrat, Aksum, Shire, Humera, Adwa, Alamata, Wukro, Maichew, and Abyi Adi. There are an estimated 1446 children in the major cities.26
Source and Study Population
All children who experienced homelessness in northern Ethiopia were taken as source population. Those aged 12–18 years and found in the selected major cities of Tigrai, northern Ethiopia, during the planned study duration were the study population. Major cities were selected randomly and population proportional to size was used to allocate the study subjects to the respective cities. Finally, we conducted street-based outreach searching for five months in Mekelle, Shire, Adigrat and Wukro cities to get a representative sample of the city’s children until the required sample size (ie, 422) was reached. Children who experience homelessness do concentrate themselves in some areas of cities. Most of the time, the children spent their time in sections of the cities where there are big hotels, restaurants and bars. Therefore, the research team targeted such sections of the cities included in our study.
Eligibility Criteria
All children who experienced homelessness and aged 12–18 years and who stayed in the street for a week and above were part of the study; and those who experienced illness like conditions and consequently were in a difficult position to respond to questions forwarded by data collectors were denied from participation in the study.
Data Collection Process
The children who experienced homelessness were interviewed using interviewer administrated structured questionnaire/tool which was adopted from other literatures.10,11,15 The tool comprised socio-demographic variables, family details, relationship with family and substance use of children who experienced homelessness. It was designed in English and then translated to Tigrigna language. Moreover, short training was arranged and delivered for the recruited enumerators and supervisors on the overall aim of the study and the way the data collection process has to proceed. Prior to data collection, pre-testing on 5% of the sample size of the research questionnaire was carried out at one of the cities of Tigrai, which would later be excluded from the study and correction was made accordingly.
Variables of the Study
Substance use was the outcome variable of interest [coded: yes/no] and socio-demographic characteristics such as age, sex and income; family details such as whereabouts of parents, educational status and occupation of parents, current marriage condition of parents and children’s current relationship with parents were the independent variables.
Operational Definitions
Substance use: Refers to the use of at least one of the substances (alcohol, chat, and cigarette) in the last 12 months by children who experienced homelessness.
Children: Refers to individuals aged 12–18 years.
Homeless: Refers to a minor child without permanent housing who lives for at least one week on the streets or in abandoned building or place.
Data Quality Handling
To make sure that the data collected in the field were of good quality, the questionnaire was pre-tested two weeks before the actual study commences. Moreover, randomly selected filled questionnaires were tested for absolute completeness by the members of the research team and amendments were made accordingly. Hard copy of filled questionnaires was kept in safe place to prevent damage and access by unauthorized individuals. Data were coded and moved into Epi Info version 3.5.1. The soft copy of the data was stored on computer, flash disks and CD for backup purpose.
Data Analysis Procedures
Data were exported to SPSS version 20 for analysis. Description of the study subjects was presented as frequencies, percentages and mean. The outcome variable of interest was regressed against the independent variables using logistic regression analysis and statistical significance was set at p-value <0.05. Model assumptions were checked.
Ethics Statements
The research team secured ethical clearance from the review board of Adigrat University in Northern Ethiopia. Moreover, official communication was made with the security office of selected major cities as data collection was conducted during the night time in addition to the day time period. Appropriate information was given to the minor child based on the child’s level of comprehension and assent (the minor child’s affirmative agreement to participate in the study) was obtained from each child. For those who were accompanied by their parents, written consent was taken from their father or mother after explaining their right not to answer any of the questions if they were not comfortable. Whether the child is accompanied by their parents or not (This amendment is made in Table 1) was roughly determined by asking the child and his/her parents. Face morphology of parents and child was also checked by simple observation. Coding system was used to keep confidentiality of information collected from each child.
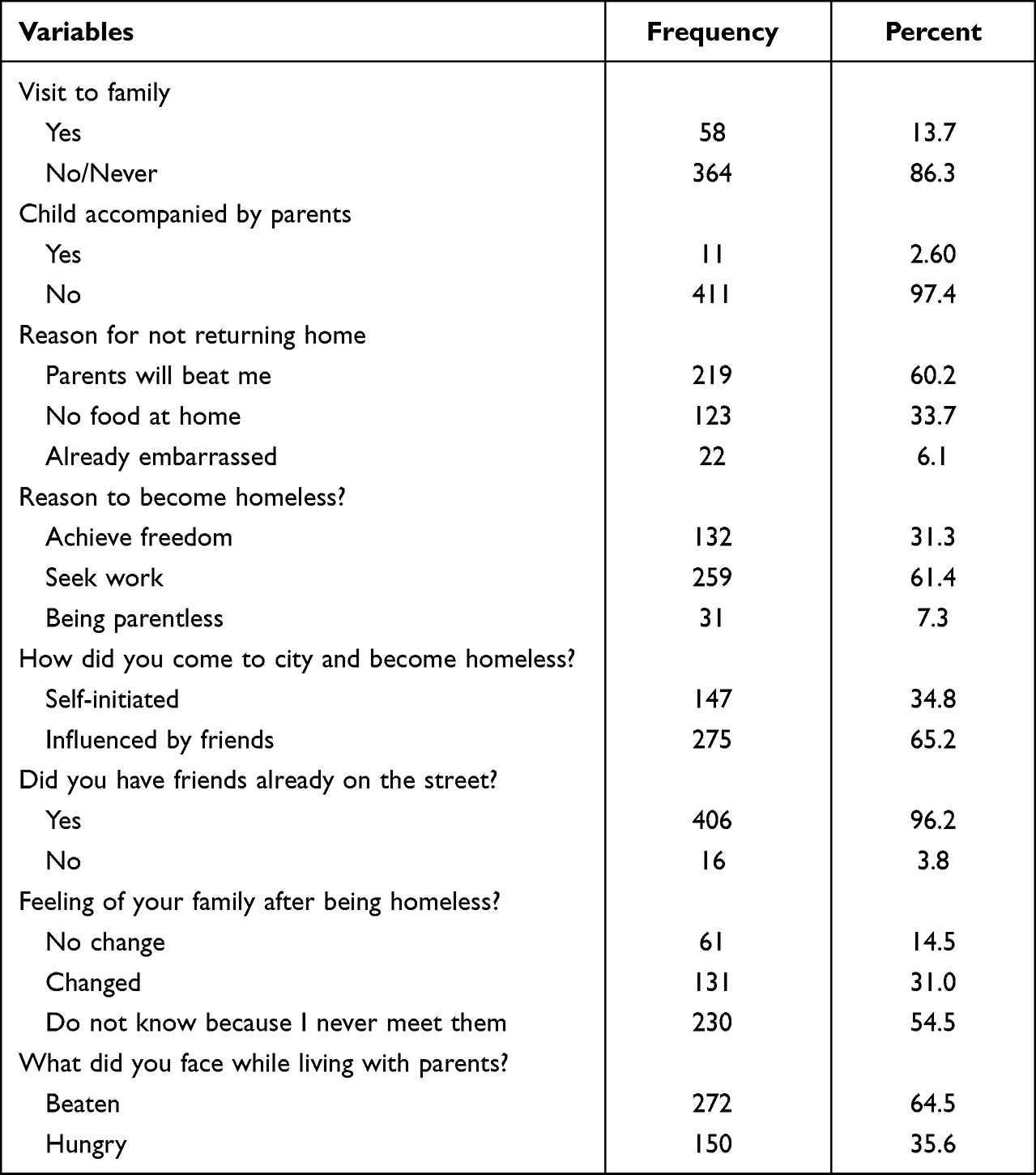 |
Table 1 Present Relationship of Homeless Children with Their Family in Tigrai, 2020 [n = 422] |
Result
Socio-Demographic Characteristics of Children
Of the 422 children experiencing homelessness enrolled in our study, only four (0.95%) were ineligible due to illness. Most of them (87%) were males and two-thirds (66%) were aged 15–18 years. Only 11 (2.61%) were accompanied by their parents. Most of them (90.5%) were from the Tigrai ethnic group, 343 (81.3%) were Orthodox Christians and around two-thirds (65.2%) were able to read and write. Monthly income for 407 (96.4%) of the children who experienced homelessness ranged from 500 to 1000 Ethiopian birr (Table 2).
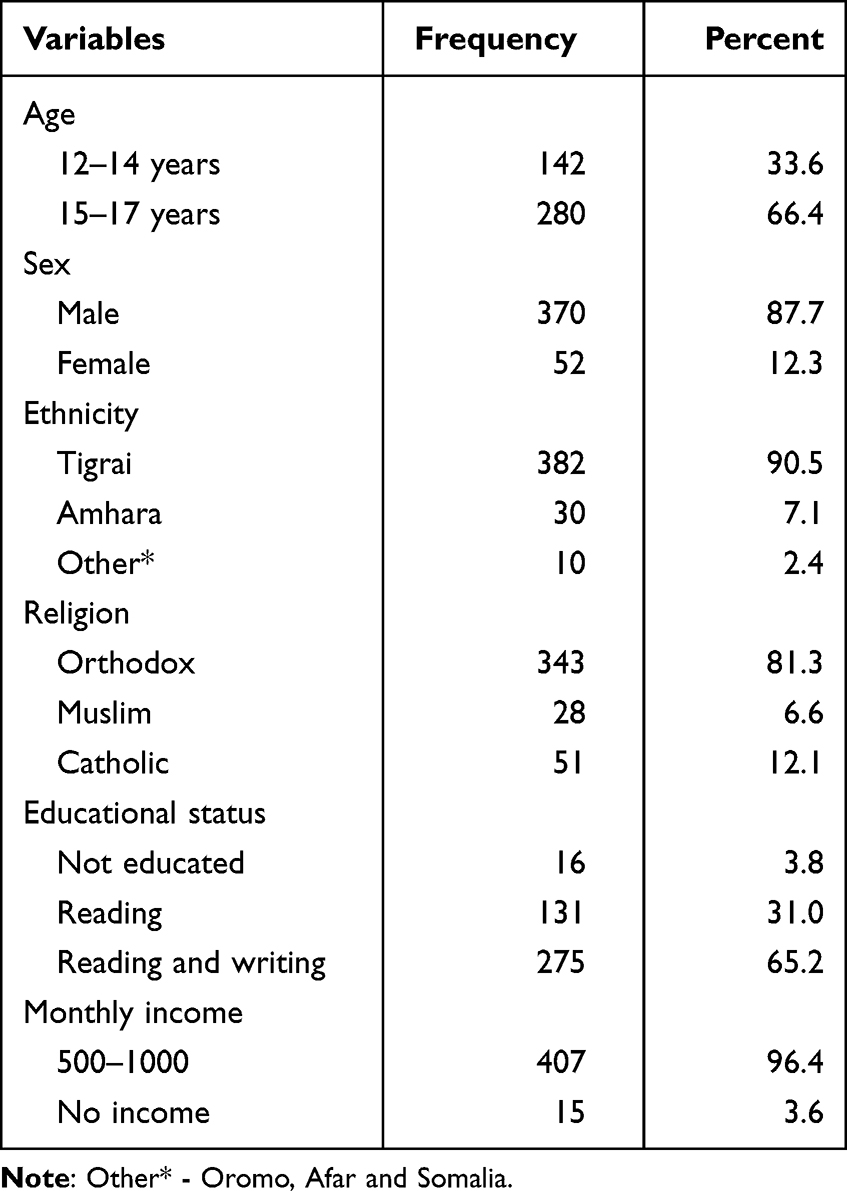 |
Table 2 Socio-Demographic Characteristics of Homeless Children in Major Cities of Tigrai, 2020 [n = 422] |
Family Details of Children
Majority (82%) of the children’s father is alive of which 197 (46.7%) are farmers. More than two-thirds (70.6%) of children’s fathers were not educated. Around 341 (80.8%) had alive mothers of which 211 (50.0%) were farmers and 231 (54.7%) mothers were not educated. Two hundred twenty-four (53.1%) of the children’s parents are divorced. Around half (49.8%) were living with their parents before they experience homelessness. Most of them left their family because they got beaten (41.2%) and they were influenced by their peers (40.0%). Almost all (98.3%) came to the city where they currently live in to get job opportunities (Table 3).
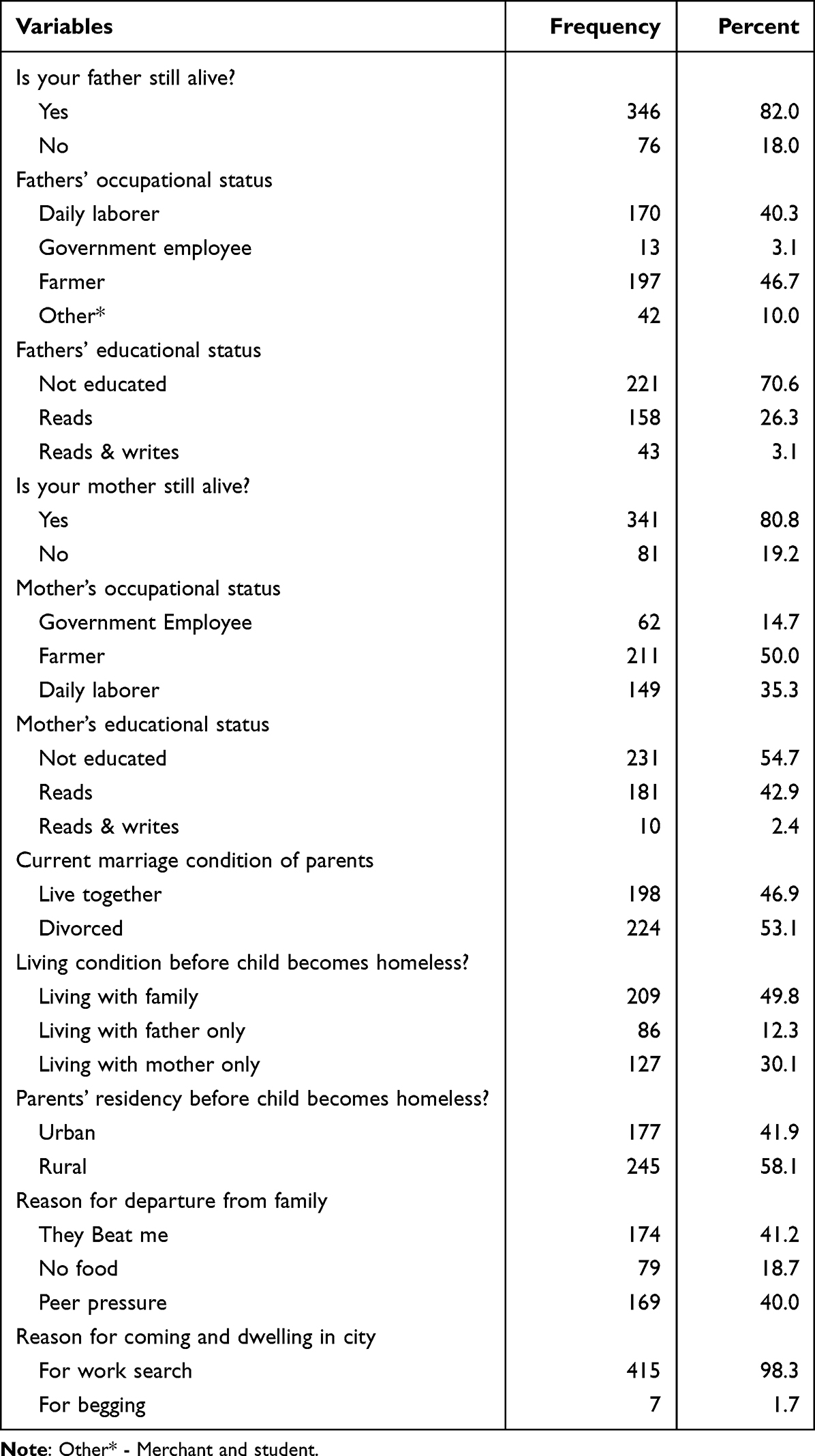 |
Table 3 Family Details of Homeless Children in Major Cities of Tigrai, 2020 [n = 422] |
Present Relationship of Children with Their Parents
Almost half of the children who experienced homelessness 364 (86.3%) have never met their parents of these 219 (60.2%) do not want to return home because they feel that their parents will beat them again. About two-thirds (65.2%) joined the street life because of their friends influence. Two hundred thirty (54.5%) of them do not know the feeling of their parents after they experienced homelessness and around two-thirds (64.5%) reported that they got beaten by their parents while they were living together (Table 1).
Level of Substance Use
At least three-fourths (80.2%) have ever used substance, of those around 34 (10%) used all substances (alcohol, chat and cigarette) and almost all (96.9%) started substance use after they experienced homelessness. Two hundred sixty four (77.4%) started to use substance to alleviate the stress they face in their street life. Majority (82.2%) do have the awareness that substance use causes health problems (Table 4).
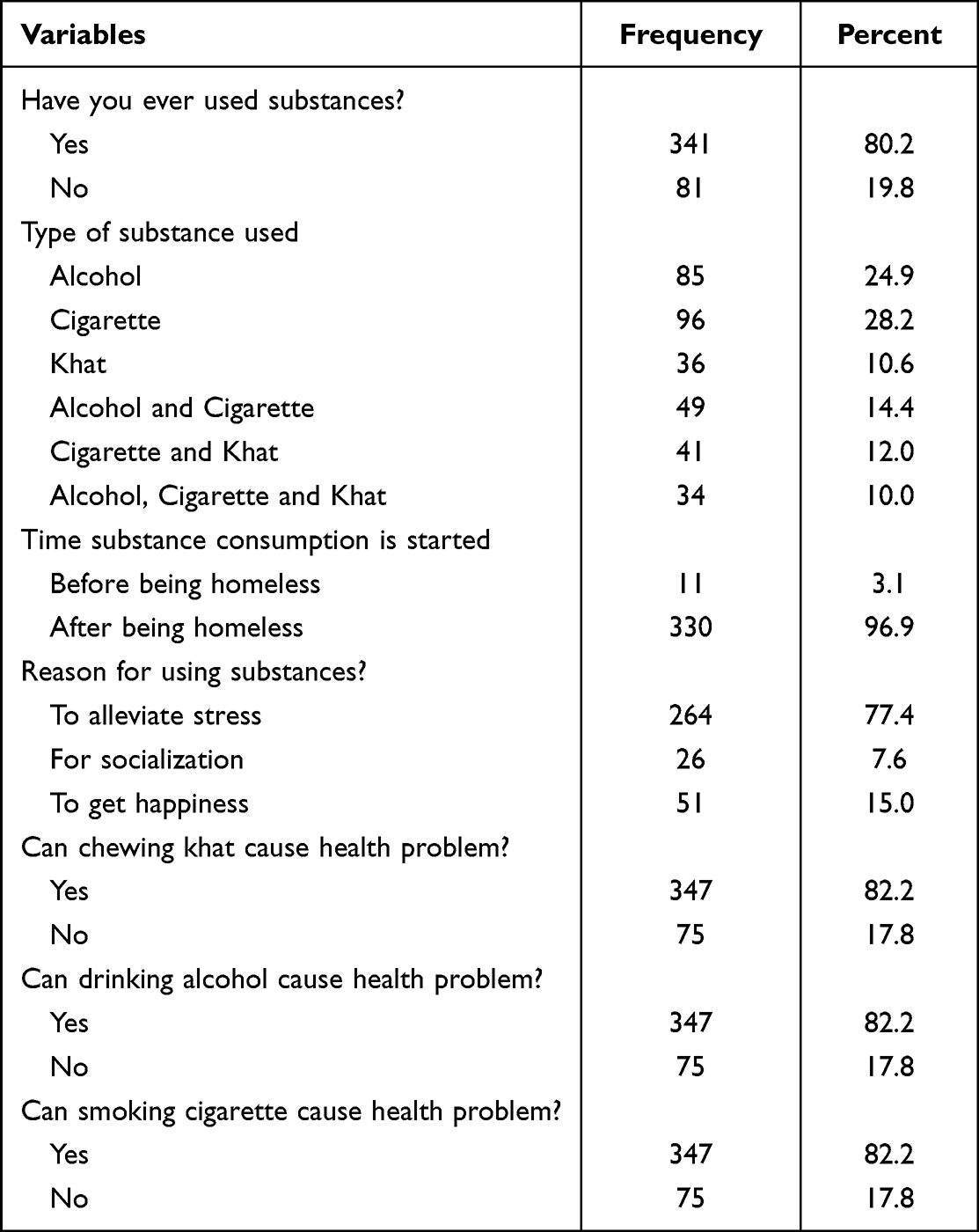 |
Table 4 Substance Use, Reasons for Using and Street Life Duration of Homeless Children in Major Cities of Tigrai, 2020 [n = 422] |
Determinants of Substance Use Among Children Who Experienced Homelessness in Major Cities of Northern Ethiopia
The bivariate analysis highlighted that, age of the child, current marriage status of parents, educational status of mother, occupational status of mother, mother’s aliveness, child relationship status with parents before experiencing homeless, parents’ residence before their child experienced homelessness were correlated with substance use. In the multivariable analysis, educational status of mother, marital status of parents, occupational status of mother, child relationship status with parents before experiencing homeless, parents’ residence before their child experienced homelessness were variables that demonstrated statistically significant association with substance use (Table 5).
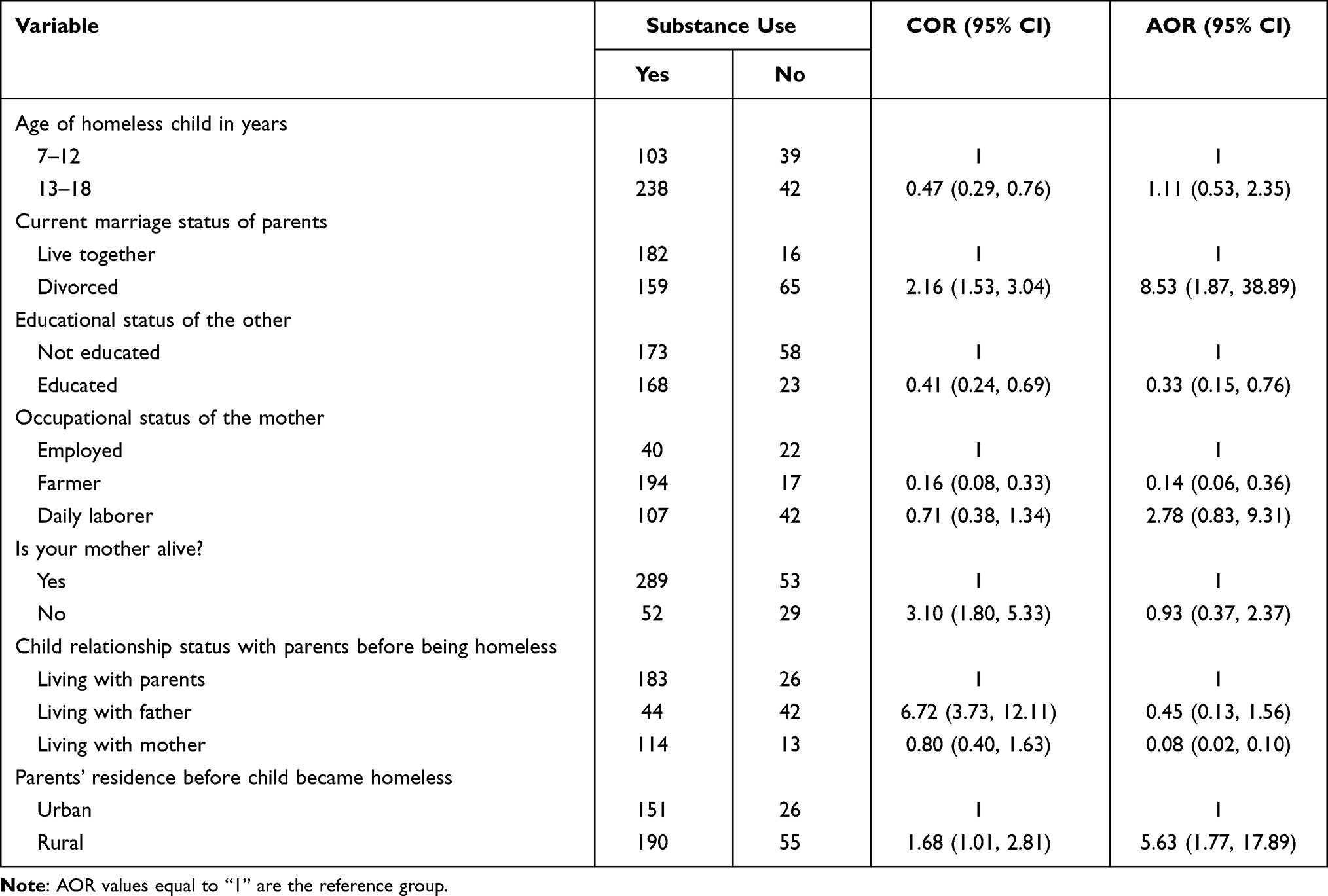 |
Table 5 Predictors of Substance Use Among Homeless Children in Major Cities of Tigrai, 2020 [n = 422] |
Children whose parents were divorced had 8.5 times (AOR = 8.53, 95% CI: 1.87–38.89) more chance of using substance as compared to those whose parents were living together. Those children whose mothers were educated had 67% less chance (AOR = 0.33, 95% CI: 0.15–0.76) of using substance than their counterparts. Children whose mothers were daily laborers had higher odds (AOR = 2.78, 95% CI: 0.83–9.31) of using substance when compared to those whose mothers were government employees. Children who were living with their father before they experienced homelessness had 37% more chance of using substance when compared to those living with their mothers only (AOR = 0.45, 95% CI: 0.13, 1.56 vs AOR = 0.08, 95% CI: 0.02–0.10). Children who were living in rural area had 5.63 times (AOR = 5.63, 95% CI: 1.77–17.89) more odds of using substance than those living in urban area (Table 5).
Discussion
This cross-sectional study was designed to evaluate the level of substance use in children who experienced homelessness in major cities of Tigrai, Northern Ethiopia. Accordingly, 80.2% of children use substances. This result is in line with the results of studies conducted in India, Guwahati City27 and Mumbai28 where substance use magnitudes are 80.9%, 80.98%, respectively. However, the magnitude of substance use in our study is higher than the magnitude reported from Jimma town, Ethiopia where the magnitude was 30.8%.29 The discrepancy might be due to the coverage of the study area in that the study in Jimma zone could have considered a relatively small town and it seems that the people there are not impacted by globalization and therefore minimizes substance use. At this time, leading street life exposes children to an increased level of stress, sadness and pressure which in turn results in a condition that forces children to use substance.10,15,21,22,30 Moreover, the relatively small sample size that Jimma study used could be another reason. On the other hand, level of substance use among children who experienced homelessness (current study) is higher than the level in housed Ethiopian children as it was revealed in studies conducted in Dire Dawa (19.6%) and Wereta (47.9%) cities.31,32 This could imply that housed children may have the chance to be involved in clubs of their schools and other organization. In addition, the degree of valuing one’s health is by far greater among housed children than children who experienced homelessness.
A study conducted in three national samples in the United States of America33 revealed that substance use was higher among children who experienced homelessness than that who did not. It is estimated that more than 75% children used three substances simultaneously unlike our study where the magnitude is 10%. This may imply that children in the United States of America are highly liable to effects of modern day life styles. About 81.4% and 80.9% children used tobacco and alcohol, respectively, which are higher figures than our study’s finding. Moreover, children in the United States of America are exposed to films and videos that might trigger children to use substance, a practice considered to be a sign of globalization. Moreover, the availability of low cost psychoactive active substances like alcohol and drugs in developed countries34 enables street children to have an easy access to the substances and raises their spirit to use. The presence of strong religious belief among adolescents in most low- and middle-income countries also serves as an individual protective factor and contributes a lot in the reduction of level of substance use in those countries.
An Iranian study showed that alcohol use among children who experienced homelessness was 31.2%.35 This is somewhat lower than our study’s finding which lies at 24.9%. Such deviations could be due to the existence of easy access to and affordable price of alcohol in Iran.
Results of multivariable analysis showed that children whose parents were divorced had higher chance of using substance as compared to those whose parents were living together, a finding consistent with similar studies done previously.29,36 This implies that, in case of divorced family, children would be managed with one of the parents which could cause decrease in economy and family-ship treatment which in turn might enforce children to get stressed and therefore use substance.
In the current study, children whose mothers were able to read had 67% less chance of using substance as compared to those whose mothers were not educated. It is obvious that educated mothers might educate their children about what substance is and how it affects the brain of humankind. Furthermore, children whose mothers were farmers had lower odds of using substance as compared to children whose mothers were daily laborer. The reason could be children whose parents were farmers could be less exposed to substance as there is limited access to in rural area whereas daily laborers are mostly found in urban areas where their children have easy access to substance use.
Moreover, children who were living in rural area had by far higher odds of using substance than those living in urban area. A study conducted in Delhi, India, supported the current study findings in that it declared family-related variables are possible determinants of substance use.36
Children were well aware that substance use was unhealthy, yet many were still using it. It could be said that knowing the harmful effect of substance use alone might not be enough. Inability to decide, set one’s own goal and lack of recreational amenities in cities where children who experience homelessness could have a visit to and refresh their mind is another factor.37
Conclusion and Recommendation
More than 80% of the children use substance, particularly alcohol and cigarette. Current marriage condition of parents, educational status of mother, occupational status of mother, child relationship status with parents before experiencing homelessness, parents’ residential status before experiencing homelessness were variables that demonstrated statistically significant association with substance use. Thus, governmental and non-governmental organizations should collaborate to reduce the magnitude of substance use. Moreover, the region’s health bureau should strive by applying innovative strategies to safeguard the health and wellbeing of children living in the street.
Data Sharing Statement
Dataset of this study is available from the corresponding author provided a reasonable and official request is forwarded.
Funding
Adigrat University funded this research project.
Disclosure
The authors report no conflict of interest in this work.
References
1. The United Nations convention on Child right; 2016. unicef.org. Convention on the Rights of the Child For every child, every right. Available from: https://www.unicef.org/child-rights-convention. Accessed November 24, 2022.
2. Room R. Alcohol in Developing Societies: A Public Health Approach. Geneva: Finnish foundation for alcohol studies in collaboration with World Health Organization; 2002.
3. World Health Organization (WHO). ATLAS on Substance Use, Resources for the Prevention and Treatment of Substance Use Disorders. Geneva, Switzerland: World Health Organization (WHO); 2010.
4. World Health Organization (WHO). Fact sheet; 2016.
5. Odejide AO. Status of drug use/abuse in Africa: a review. Int J Ment Health Addict. 2006;4(2):87–102. doi:10.1007/s11469-006-9015-y
6. Embleton L, Mwangi A, Vreeman R, Ayuku D, Braitstein P. The epidemiology of substance use among street children in resource-constrained settings: a systematic review and meta-analysis. Addiction. 2013;108(10):1722–1733. doi:10.1111/add.12252
7. Embleton L, Ayuku D, Atwoli L, Vreeman R, Braitstein P. Knowledge, attitudes, and substance use practices among street children in western Kenya. Subst Use Misuse. 2012;47(11):1234–1247. doi:10.3109/10826084.2012.700678
8. Kayembe PK, Mapatano MA, Fatuma AB, et al. Knowledge of HIV, sexual behaviour and correlates of risky sex among street children in Kinshasa, Democratic Republic of Congo. East Afr J Public Health. 2008;5(3):186–192.
9. Nada KH, Suliman EDA. Violence, abuse, alcohol and drug use, and sexual behaviors in street children of greater Cairo and Alexandria, Egypt. AIDS. 2010;24:S39–S44. doi:10.1097/01.aids.0000386732.02425.d1
10. United Nations Children’s Fund (UNICEF). Study on Street Children in Four Selected Towns in Ethiopia. Dublin Institute of Technology; 2014.
11. UNICEF. A base line survey of children living on the streets of Addis Ababa; 2012.
12. Shegaw M, Fekadu W, Beka M, et al. Problematic substance use and its associated factors among street youth in Bahir Dar city, Ethiopia. Front Psychiatry. 2022;13:930059. doi:10.3389/fpsyt.2022.930059
13. Thompson SJ. Risk/protective factors associated with substance use among runaway/homeless youth utilizing emergency shelter services nationwide. Subst Abuse. 2004;25(3):13–26. doi:10.1300/J465v25n03_02
14. Ayerst SL. Depression and stress in street youth. Adolescence. 1999;34(135):567–575.
15. Fest J. Understanding street culture: a prevention perspective. School Nurse News. 2003;20(2):16–18.
16. National Institute on Drug Abuse. Advancing addiction science. Health consequences of drug misuse, updated fact sheet; 2017.
17. Adebiyi AO, Owoaje O, Asuzu MC. Relationships as determinants of substance use amongst street children in a local government area in south-western Nigeria. SA Fam Pract. 2008;50(5):47. doi:10.1080/20786204.2008.10873761
18. Ginzler JA, Cochran BN, Domenech-Rodriguez M, Cauce AM, Whitbeck LB. Sequential progression of substance use among homeless youth: an empirical investigation of the gateway theory. Subst Use Misuse. 2003;38(3–6):725–758. doi:10.1081/JA-120017391
19. Resnick MD, Harris L, Blum R. The impact of caring and connectedness on adolescent health and well-being. J Paediatr Child Health. 1993;29:53–59. doi:10.1111/j.1440-1754.1993.tb02257.x
20. Ostrow DG. Substance abuse and HIV infection. Psychiatr Clin North Am. 1994;17:69–89. doi:10.1016/S0193-953X(18)30131-X
21. Leigh BC, Stall R. Substance use and risky sexual behavior for exposure to HIV: issues in methodology, interpretation, and prevention. Am Psychol. 1993;48:1035–1045. doi:10.1037/0003-066X.48.10.1035
22. Room R, Zucker R. Adolescent drinking as collective behavior and performance. The development of alcohol problems: national Institute on Alcohol Abuse and Alcoholism. NIAAA Res Monogr. 1994;26:205–208.
23. News I. Focus on street children rehabilitation project. Available from: http://www.irinnews.org/report/48799/ethiopia-focus-street-childrenrehabilitation-project.
24. UNICEF. Investing in boys and girls in Ethiopia. Past, present and future; 2012: 29–30.
25. Federal Ministry of health. Ministry of women and children affairs report; 2019.
26. Bureau of women and children affairs report, Tigrai region, Ethiopia; 2020. unicef.org. Situation Analysis of Children and Women: Tigray Region. Available from: https://www.unicef.org/ethiopia/media/2351/file/Tigray%20region%20.pdf. Accessed November 24, 2022.
27. Islam F, Kar S, Debroy A, Sarma R. Substance abuse amongst the street‑children in Guwahati City, Assam. Ann Med Health Sci Res. 2014;4(3):S233–8. doi:10.4103/2141-9248.141965
28. Abhay MG, Quazi SZ, Lalit W, Sunita S, Sanjay Z, Sudhakar RJ. Substance abuse among street children in Mumbai. Vulnerable Child Youth Stud. 2008;3(1):42–51. doi:10.1080/17450120701843166
29. Ayenew M, Kabeta T, Woldemichael K. Prevalence and factors associated with substance use among street children in Jimma town, Oromiya national regional state, Ethiopia: a community based cross-sectional study. Subst Abuse Treat Prevent Policy BMC. 2020;15:61. doi:10.1186/s13011-020-00304-3
30. Pagare D, Meena GS, Singh MM, Sahu R. Risk factors of substance use among street children from Delhi, Indian pediatrics. Indian Pediatrics. 2004;41(3):221–225.
31. Negussie B. Substance use among high school students in Dire Dawa, Ethiopia. Harar Bull Health Sci. 2012;4:38–42.
32. Anteneh MB, Telake AB, Solomon MW. High prevalence of substance use and associated factors among high school adolescents in Woreta Town, Northwest Ethiopia: multi-domain factor analysis. BMC Public Health. 2014;14:1186. doi:10.1186/1471-2458-14-1186
33. Jodv M, Greetne MS, Ennett ST. Substance use among runaway and homeless youth in three national samples. Am J Public Health. 1997;87(2):229–235. doi:10.2105/AJPH.87.2.229
34. World Health Organization. Working with Street Children. WHO/MSD/MDP/00.14. World Health Organization; 1995.
35. Mehrdad K, Ali M, Willi M, et al. Prevalence and correlates of substance use among homeless youth in Kerman, a city in southeast Iran. Child Youth Serv Rev. 2020;116:105070.
36. Bhattacharjee S, Kumar R, Agrawal A, O’Grady KE, Jones HE. Risk factors for substance use among street children entering treatment in India. Indian J Psychol Med. 2016;38:419–423. doi:10.4103/0253-7176.191375
37. Slap GB, Lot L, Huang B, Daniyam CA, Zink TM, Succop PA. Sexual behavior of adolescents in Nigeria: cross sectional survey of secondary school students. BMJ. 2003;326:15. doi:10.1136/bmj.326.7379.15
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.