Back to Journals » Journal of Asthma and Allergy » Volume 19
A Clinical Nomogram for Predicting Early Response to Biologics in Pediatric Allergic Asthma with Comorbid Allergic Rhinitis
Authors Wang L, Kang Z, Ma J, Wang C, Jiang W, Huang J, Liu S
Received 2 March 2026
Accepted for publication 8 June 2026
Published 30 June 2026 Volume 2026:19 604654
DOI https://doi.org/10.2147/JAA.S604654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Lixin Wang1,*, Zhaopeng Kang2,*, Jun Ma1, Chuanxi Wang1, Wanjin Jiang1, Jingjiang Huang1, Shaofeng Liu1
1Department of Otolaryngology Head and Neck Surgery, The First Affiliated Hospital of Wannan Medical University (Yijishan Hospital of Wannan Medical University), Wuhu, Anhui, People’s Republic of China; 2Health Management Center, The First Affiliated Hospital of Wannan Medical University (Yijishan Hospital of Wannan Medical University), Wuhu, Anhui, People’s Republic of China
*Lixin Wang and Zhaopeng Kang contributed equally to this work
Correspondence: Shaofeng Liu, Department of Otolaryngology Head and Neck Surgery, The First Affiliated Hospital of Wannan Medical University (Yijishan Hospital of Wannan Medical University), No. 2 Chushan West Road, Wuhu, Anhui, 241000, People’s Republic of China, Tel +86-15717282650, Email [email protected]; Jingjiang Huang, Department of Otolaryngology Head and Neck Surgery, The First Affiliated Hospital of Wannan Medical University (Yijishan Hospital of Wannan Medical University), No. 2 Chushan West Road, Wuhu, Anhui, 241000, People’s Republic of China, Email [email protected]
Background: The coexistence of allergic rhinitis (AR) and allergic asthma poses a significant burden on pediatric health. While biologics targeting type 2 inflammation have revolutionized treatment, individual responses vary significantly. There is a lack of practical tools to predict early therapeutic response before initiation. This study aimed to identify key baseline predictors and construct a nomogram to personalize the prediction of early response to biologics in children with AR and allergic asthma.
Methods: This retrospective cohort study included 246 children (recruited between January 2021 and August 2025) diagnosed with moderate-to-severe allergic AR and allergic asthma who received biologic therapy (Omalizumab or Dupilumab). Early response was assessed at 16 weeks based on a composite outcome involving the Asthma Control Test (ACT), visual analog scale (VAS) for nasal symptoms, and exacerbation history. Independent predictors were identified using LASSO regression and multivariate logistic regression analysis to build a nomogram. The model’s performance was evaluated using the concordance index (C-index), calibration curves, and decision curve analysis (DCA).
Results: Of the 246 patients, 164 (66.7%) were classified as early responders. Multivariate analysis identified baseline fractional exhaled nitric oxide (FeNO), blood eosinophil count (EOS), total IgE levels, comorbidity of atopic dermatitis (AD), and Body Mass Index (BMI) as independent predictors. The developed nomogram demonstrated good discrimination with a C-index of 0.88 (95% CI: 0.83– 0.93) in the training cohort and 0.85 (95% CI: 0.78– 0.92) in the validation cohort. Calibration curves showed excellent agreement between predicted and observed probabilities. DCA indicated significant clinical net benefit across a wide range of threshold probabilities.
Conclusion: We successfully developed a novel nomogram incorporating baseline type 2 inflammatory endotypes and AD comorbidity to predict early response to biologics in pediatric patients with allergic asthma and comorbid AR. This tool offers clinicians a practical method to screen potential “super-responders”, thereby optimizing therapeutic decision-making and resource allocation.
Keywords: allergic rhinitis, allergic asthma, biological therapy, nomogram, type 2 inflammation, pediatrics
Introduction
Allergic rhinitis (AR) and allergic asthma are among the most common chronic respiratory diseases in children, and their frequent coexistence is explained by the “one airway, one disease” concept. Epidemiological data indicate that up to 80% of children with allergic asthma suffer from concurrent AR, and children with both comorbid conditions face a significantly increased risk of emergency department visits and poorer disease control than those with isolated isolated allergic asthma.1,2 This comorbidity not only severely impairs the quality of life and lung development of pediatric patients but also imposes a substantial economic burden on families and healthcare systems.3,4
The shared pathophysiology of both conditions is predominantly driven by type 2 (T2) inflammation, characterized by the activation of T-helper 2 (Th2) cells and type 2 innate lymphoid cells (ILC2s), leading to the release of key cytokines such as interleukin (IL)-4, IL-5, and IL-13, and the production of immunoglobulin E (IgE).5 In recent years, biological agents targeting these specific pathways—such as Omalizumab (anti-IgE) and Dupilumab (anti-IL-4Rα)—have emerged as transformative therapies for children with moderate-to-severe allergic diseases who remain uncontrolled despite standard pharmacotherapy. Clinical evidence confirms that Omalizumab significantly reduces exacerbation rates and improves lung function in children with moderate-to-severe asthma.6 For Dupilumab, a Phase 3 trial in children demonstrated efficacy in reducing severe asthma exacerbations and improving lung function,7 with subsequent analyses showing significant improvements in asthma control and health-related quality of life for both patients and their caregivers.8 Meta-analyses further support the role of Dupilumab in enhancing pulmonary function and reducing inflammatory markers in patients with moderate-to-severe asthma.9 These targeted therapies represent a significant advance in managing severe pediatric allergic respiratory disease.10
However, significant heterogeneity exists in the therapeutic response to biologics. Not all patients achieve the desired clinical control; some are “super-responders”, operationally defined as patients who achieve complete symptom control (eg., Asthma Control Test [ACT] score ≥ 20, visual analog scale [VAS] score ≤ 2) and experience zero exacerbations during therapy, while others show partial or no response.11 Given the high cost of biological therapies, the potential for adverse effects, and the requirement for long-term parenteral administration, identifying which children are most likely to benefit before treatment initiation is a critical unmet clinical need.12 Current guidelines, such as the Global Initiative for Asthma (GINA) and Allergic Rhinitis and its Impact on Asthma (ARIA), emphasize the importance of “phenotype-guided therapy”—which refers to tailoring treatment strategies based on a patient’s unique, observable clinical and biological traits—but lack specific, quantitative tools for individual probability prediction.13,14
Existing prediction models in this field have limitations. Most focus solely on allergic asthma or severe adult populations, neglecting pediatric-specific characteristics and the significant impact of multimorbidity.15 Traditional predictive models have achieved moderate success (C-indices ranging from 0.70 to 0.78) using isolated parameters like baseline blood eosinophil count (EOS) or fractional exhaled nitric oxide (FeNO), though recent large-scale analyses demonstrate that combining these biomarkers significantly enhances prognostic accuracy.16 The role of extra-respiratory comorbidities, particularly atopic dermatitis (AD), which shares the underlying systemic T2 inflammatory burden, is often underappreciated in respiratory outcome prediction models.17 Evidence suggests that the “atopic march” phenotype, involving skin and airway sensitization, may represent a distinct endotype with higher susceptibility to specific biologic interventions.18
Therefore, this study aims to bridge this gap by conducting a retrospective analysis of pediatric patients with allergic AR and comorbid allergic asthma treated with biologics over the past five years. We hypothesize that a combination of readily available baseline clinical characteristics—specifically T2 inflammatory biomarkers (FeNO, IgE, EOS) and comorbidity profiles (AD status, BMI)—can accurately predict early therapeutic response. By integrating these factors, we sought to develop and validate a visual, easy-to-use nomogram. This tool intends to assist clinicians in precise decision-making, ensuring that the right patient receives the right treatment at the right time, thereby advancing the practice of precision medicine in pediatric allergy.
Materials and Methods
Study Design and Population
This retrospective cohort study was conducted at the Department of Allergy and Respiratory Medicine of our hospital. We screened electronic medical records of pediatric patients diagnosed with allergic rhinitis (AR) and comorbid bronchial allergic asthma who received biological therapy between January 2021 and August 2025. The study protocol was approved by the Institutional Ethics Committee of The First Affiliated Hospital of Wannan Medical University (Yijishan Hospital of Wannan Medical University) (No. 2025053) and was conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study, and patient data were anonymized.
The inclusion criteria were as follows: (1) Age between 6 and 18 years; (2) Physician-diagnosed moderate-to-severe persistent AR and bronchial allergic asthma according to the Global Initiative for Asthma (GINA) and Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines,19,20 with the asthma phenotype restricted strictly to allergic asthma; (3) Documented history of at least one specific allergen sensitization (eg., house dust mites, pollens, molds, or animal dander) confirmed by serum specific IgE (sIgE ≥ 0.35 kUA/L) or skin prick test (mean wheal diameter ≥ 3 mm compared with negative control)-often supplemented by molecular component-resolved diagnostics to rule out cross-reactivity, interpreted in accordance with the updated European Academy of Allergy and Clinical Immunology (EAACI) standards;21 (4) Initiation of biological therapy (Omalizumab or Dupilumab) due to uncontrolled symptoms despite optimal pharmacological treatment (eg., persistent symptoms despite treatment with GINA Steps 4–5 controllers and daily intranasal corticosteroids combined with antihistamines); and (5) Availability of complete baseline data and follow-up records for at least 16 weeks post-initiation. Patients were excluded if they had: (1) Concomitant active parasitic infection; (2) Other significant chronic respiratory diseases (eg., cystic fibrosis, bronchiectasis); (3) Systemic autoimmune diseases; or (4) Irregular administration of the biologic agent.
Data Collection and Predictor Variables
Baseline demographic and clinical characteristics were extracted from medical records prior to the first injection. Demographic variables included age, gender, delivery mode (vaginal vs. cesarean), and family history of allergic diseases. Anthropometric measurements, specifically Body Mass Index (BMI), were recorded and converted to z‑scores based on age‑ and sex‑specific WHO Child Growth Standards.22,23
We focused on Type 2 (T2) inflammatory endotype markers and comorbidity profiles as potential predictors. Laboratory indicators included: peripheral blood eosinophil count (EOS) and percentage, serum total Immunoglobulin E (tIgE), and fractional exhaled nitric oxide (FeNO). All laboratory tests were performed within one week prior to the initial treatment. Comorbidity data specifically focused on the presence and severity of Atopic Dermatitis (AD), chronic rhinosinusitis (with or without nasal polyps), and food allergies.
Disease severity at baseline was assessed using the Visual Analog Scale (VAS) for nasal symptoms (0–10 cm),24,25 the Total Nasal Symptom Score (TNSS) – a sum of four individual symptom scores (sneezing, rhinorrhea, nasal congestion, nasal itching) each rated on a 0‑3 scale,26 and the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ).27
Outcome Definition
The primary outcome was “Early Therapeutic Response”, assessed at 16 weeks (approx. 3 months follow-up window) after treatment initiation. Based on established criteria and real-world evidence,28 patients were classified as “Responders” if they met the following composite criteria: (1) A reduction in TNSS of ≥30% from baseline OR a decrease in VAS score of ≥2 points; AND (2) No asthma exacerbations requiring systemic corticosteroids or hospitalization during the treatment period. Patients failing to meet these criteria were classified as “Non-responders.”
Statistical Analysis
Statistical analyses were performed using R software (version 4.5.1; The R Foundation). Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR) depending on normality, and categorical variables were presented as frequencies (%). Differences between Responders and Non-responders were analyzed using the Student’s t-test, Mann–Whitney U-test, or Chi-square test as appropriate.
To identify robust predictors and avoid overfitting, we employed the Least Absolute Shrinkage and Selection Operator (LASSO) regression analysis. Variables with non-zero coefficients in the LASSO model were subsequently entered into a multivariate logistic regression analysis to determine independent predictors. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated.
A nomogram was constructed based on the multivariate logistic regression model. The model’s predictive performance was evaluated in terms of discrimination (Concordance Index, C-index) and calibration (calibration plots with 1000 bootstrap resamples). Decision Curve Analysis (DCA) was conducted to assess the clinical utility of the nomogram by quantifying the net benefit at different threshold probabilities. A two-sided P-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population
A total of 246 pediatric patients met the inclusion criteria and were included in the final analysis. The cohort was randomly divided into a training set (n = 172) and a validation set (n = 74) at a ratio of 7:3. In the total population, the mean age was 10.4 ± 3.2 years, and 142 (57.7%) were male. The overall early response rate at 16 weeks was 66.7% (164/246). The baseline characteristics were well-balanced between the training and validation sets (P > 0.05 for all variables). Detailed demographic and clinical data are summarized in Table 1. A flowchart summarizing the entire study process, including patient recruitment and model development, is provided in Supplementary Figure S1.
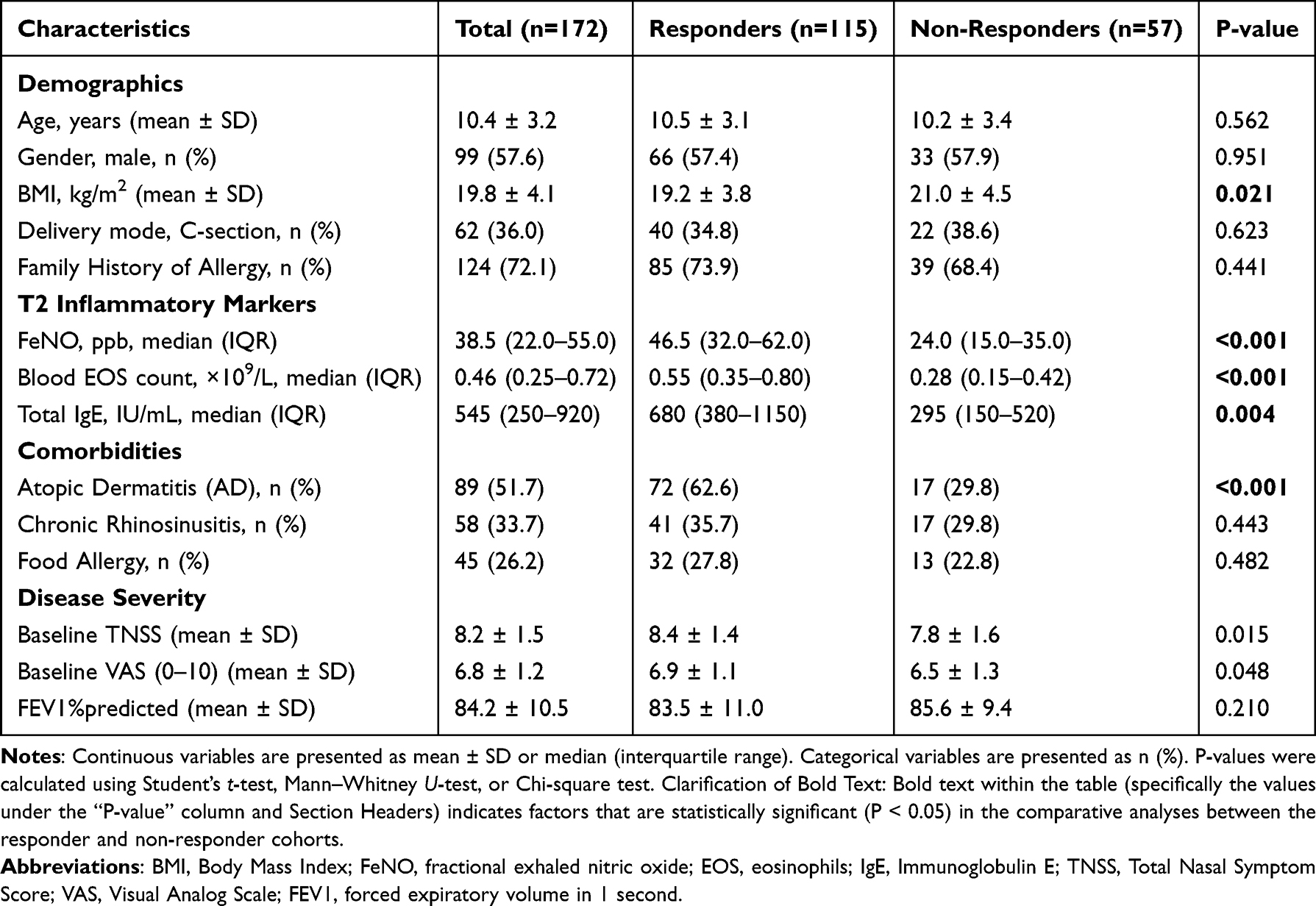 |
Table 1 Baseline Demographic and Clinical Characteristics of the Study Population in the Training Cohort (n=172) |
Univariate Analysis of Factors Associated with Therapeutic Response
In the training cohort, we compared the baseline characteristics between the Responder (n = 115) and Non-responder (n = 57) groups. Univariate analysis revealed that Responders exhibited significantly higher baseline levels of T2 inflammatory biomarkers compared to Non-responders. Specifically, the median FeNO was higher in Responders (46.5 vs. 24.0 ppb, P < 0.001), as was the blood EOS count (0.55 vs. 0.28 ×109/L, P < 0.001) and total IgE (680 vs. 295 IU/mL, P = 0.004).
Notably, regarding comorbidities, patients with a history of concurrent Atopic Dermatitis (AD) showed a significantly higher response rate (62.6% in Responders vs. 29.8% in Non-responders, P < 0.001). Conversely, patients with a higher BMI were less likely to respond to biological therapy (P = 0.021). No significant differences were found regarding gender, delivery mode, or family history. The detailed univariate analysis results are presented in Table 1.
Predictor Selection and Model Construction
To handle the multicollinearity among clinical variables and select the most impactful features, LASSO regression analysis was performed. As shown in Figure 1A and B, the partial likelihood deviance was minimized, and five potential predictors with non-zero coefficients were identified: FeNO, EOS count, Total IgE, Comorbid AD, and BMI.
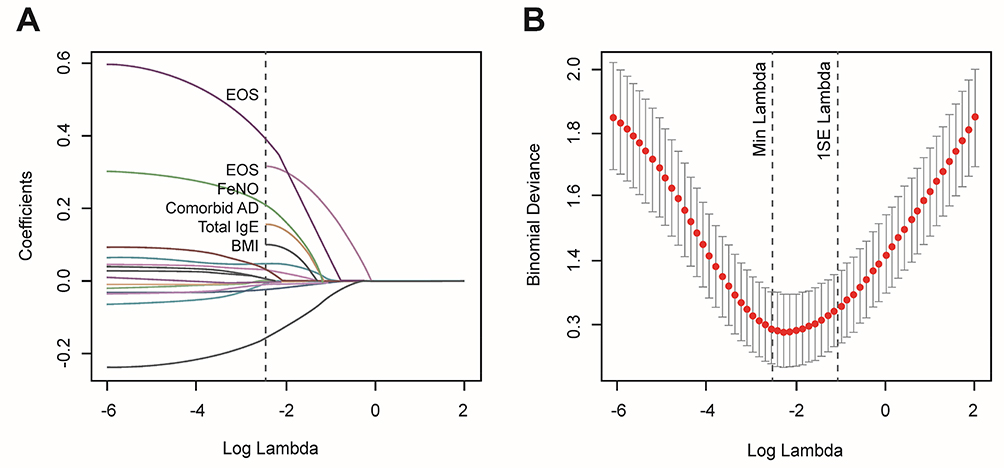 |
Figure 1 Predictor selection using the Least Absolute Shrinkage and Selection Operator (LASSO) binary logistic regression model. (A) LASSO coefficient profiles of the 12 candidate clinical features. A coefficient profile plot was produced against the log (lambda) sequence. (B) Tuning parameter (lambda) selection in the LASSO model used 10-fold cross-validation via minimum criteria. The dotted vertical lines were drawn at the optimal values using the minimum criteria and the 1 standard error of the minimum criteria. |
These five variables were then incorporated into a multivariate logistic regression analysis. The results demonstrated that baseline FeNO (OR 1.06, 95% CI 1.03–1.09, P < 0.001), EOS count (OR 2.84, 95% CI 1.42–5.68, P = 0.003), Total IgE (OR 1.01, 95% CI 1.00–1.02, P = 0.045), and the presence of Comorbid AD (OR 2.56, 95% CI 1.28–5.12, P = 0.008) were independent positive predictors of early therapeutic response. Interestingly, BMI was identified as a negative independent predictor (OR 0.86, 95% CI 0.75–0.98, P = 0.024), suggesting that obesity may attenuate the efficacy of T2-targeted biologics. The detailed regression results are shown in Table 2.
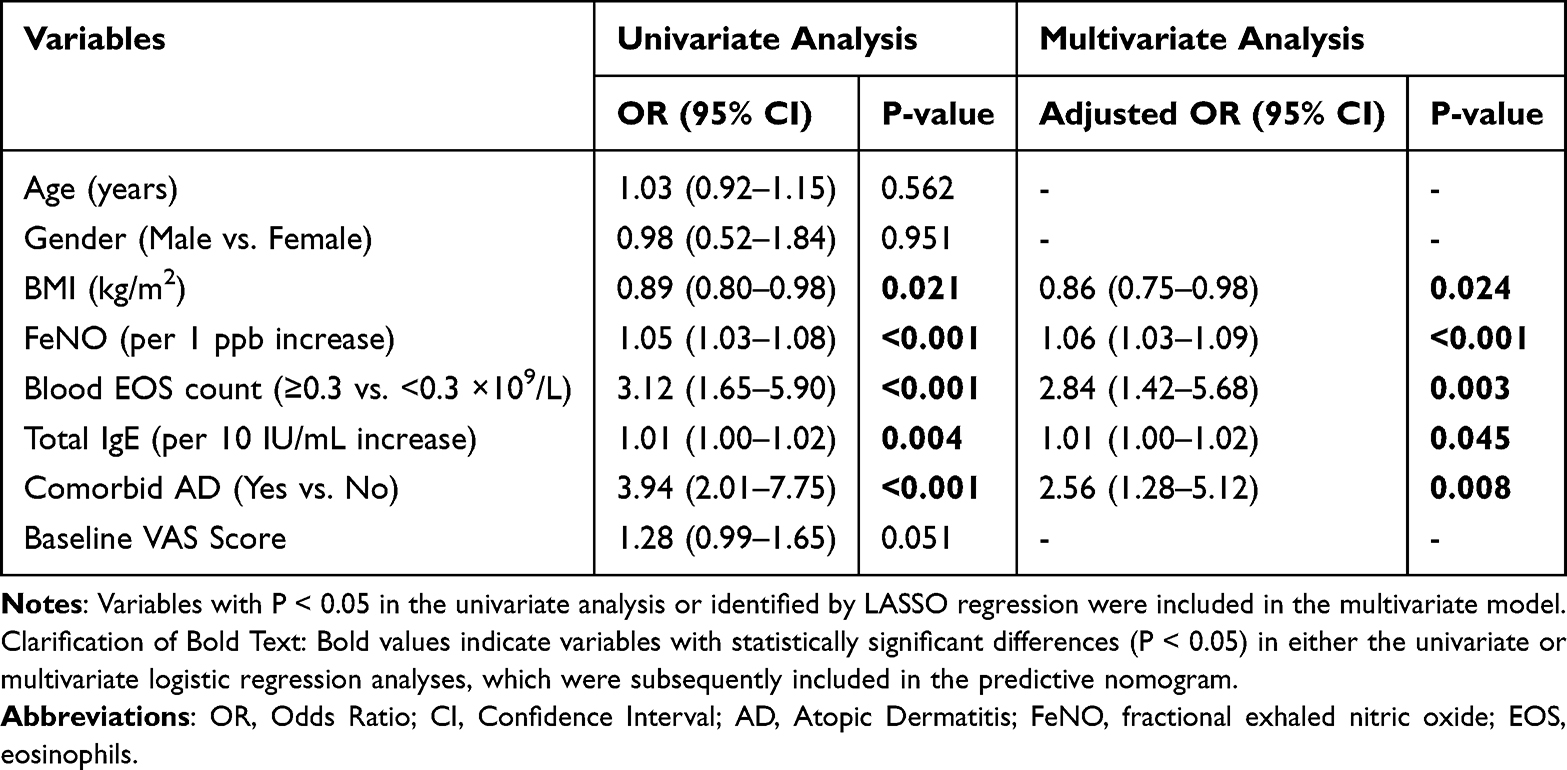 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Predictors for Early Therapeutic Response in the Training Cohort |
Development and Validation of the Nomogram
Based on the independent predictors identified above, we constructed a diagnostic nomogram to predict the probability of early response (Figure 2). In this nomogram, each predictor is assigned a score on a point scale. By summing the scores for each variable, the total score can be located on the total point scale to determine the estimated probability of response.
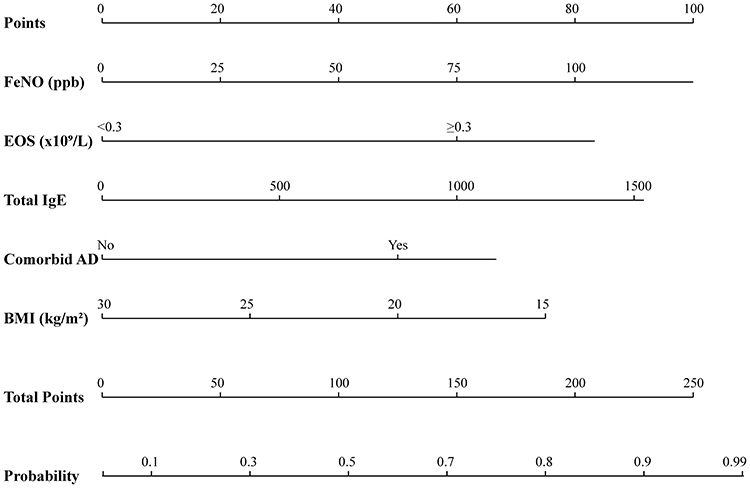 |
Figure 2 Developed nomogram for predicting the probability of early therapeutic response to biologics in pediatric AR and asthma. To use the nomogram, locate the patient’s value on each variable axis (FeNO, EOS, Total IgE, Comorbid AD, BMI). Draw a vertical line upward to the “Points” axis to determine the score for each variable. Sum these scores to obtain the “Total Points.” Finally, draw a vertical line downward from the Total Points axis to the “Probability of Response” axis to obtain the individual predicted probability. |
The performance of the nomogram was evaluated using the C-index and ROC curves. In the training set, the model achieved a C-index of 0.88 (95% CI: 0.83–0.93), indicating excellent discrimination. This high performance was maintained in the validation set with a C-index of 0.85 (95% CI: 0.78–0.92), as illustrated in the ROC curves (Figure 3).
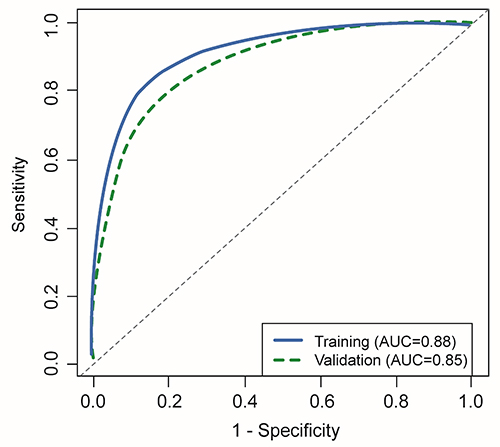 |
Figure 3 Receiver Operating Characteristic (ROC) curves of the nomogram. Receiver Operating Characteristic (ROC) curves of the nomogram. The blue solid line represents the diagnostic performance in the training cohort (AUC = 0.88), and the green dashed line represents the performance in the validation cohort (AUC = 0.85). The high Area Under the Curve (AUC) values in both cohorts indicate the excellent discrimination capability of the model. |
The calibration curves for the probability of response demonstrated good agreement between the nomogram prediction and the actual observation in both the training and validation cohorts (Figure 4). Furthermore, Decision Curve Analysis (DCA) showed that using this nomogram to predict response provided a greater net benefit than either the “treat all” or “treat none” strategies across a wide range of threshold probabilities (approximately 15% to 85%), confirming its clinical utility (Figure 5).
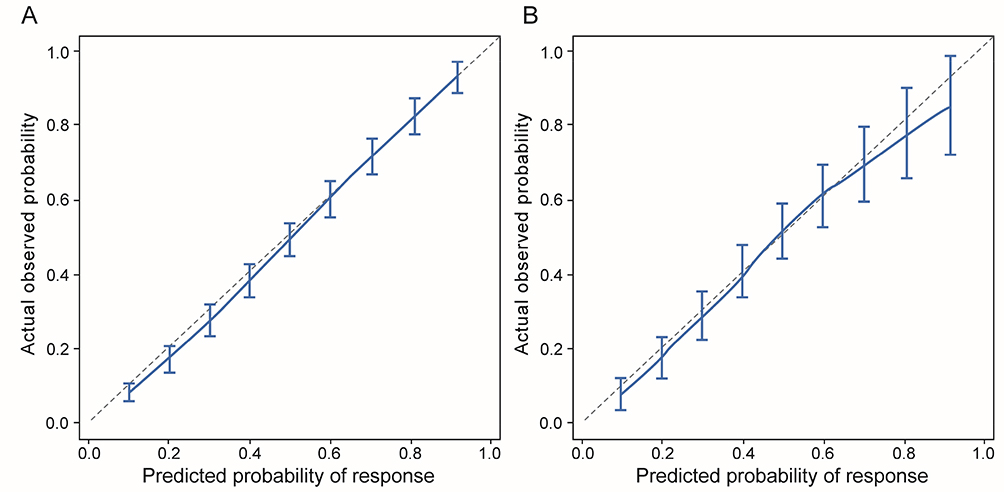 |
Figure 4 Calibration curves of the nomogram. (A) Calibration curve for the training cohort. (B) Calibration curve for the validation cohort. The x-axis represents the predicted probability of response, and the y-axis represents the actual observed probability. The diagonal dotted line represents a perfect prediction by an ideal model. The solid blue line represents the performance of the nomogram, and the vertical bars indicate the 95% confidence intervals. |
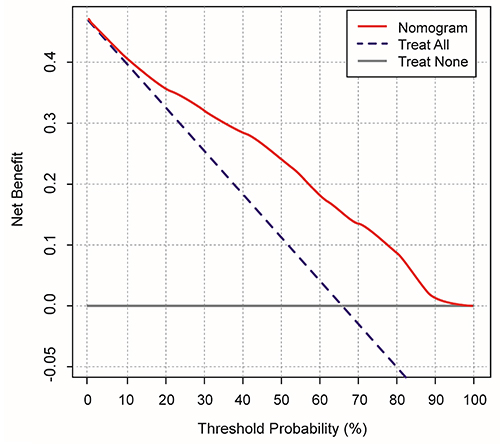 |
Figure 5 Decision Curve Analysis (DCA) for the nomogram. The y-axis measures the net benefit. The red line represents the nomogram. The blue line represents the assumption that all patients respond to treatment. The gray line represents the assumption that no patients respond. The decision curve demonstrates that utilizing the developed nomogram to guide therapeutic decisions yields a higher clinical net benefit than either of the extreme clinical approaches (assuming all patients will respond and treating everyone, or assuming no patients will respond and treating none) across a broad threshold probability range of 15% to 85%. |
Discussion
In this retrospective cohort study, we successfully developed and validated a novel nomogram to predict early therapeutic response to biologics in pediatric patients with allergic rhinitis (AR) and comorbid allergic asthma. By integrating baseline type 2 (T2) inflammatory endotypes (FeNO, EOS, Total IgE) with comorbidity characteristics (Atopic Dermatitis status and BMI), our model demonstrated robust discrimination (C-index 0.88) and calibration. To our knowledge, this is one of the first pragmatic tools to incorporate extra-respiratory comorbidities into the prediction of respiratory biologic response in children, addressing a critical gap in precision medicine.
Our findings confirm that high baseline levels of FeNO, blood eosinophils, and total IgE are strong positive predictors of therapeutic efficacy for targeted biologics. This aligns with the biological mechanisms of agents like Omalizumab and Dupilumab, which specifically target the IgE-mediated and IL‑4/IL‑13 pathways central to type 2 (T2) inflammation.29,30 Elevated baseline biomarkers often indicate a distinct T2‑high endotype that is particularly responsive to these therapies. Conversely, patients with low T2 inflammatory markers may have disease driven by neurogenic or mixed‑granulocytic pathways, rendering them less responsive to T2‑targeted biologics.31 This evidence reinforces the recent recommendations from the Global Initiative for Asthma (GINA) and the Allergic Rhinitis and its Impact on Asthma (ARIA) initiative to phenotype patients before initiating expensive biological therapies.20,32
A unique and clinically significant finding of our study is that comorbid Atopic Dermatitis (AD) acts as an independent positive predictor for respiratory outcomes. We observed that children with the “Atopic March” phenotype (allergic asthma + AR + AD) had a significantly higher response rate (OR 2.56). This likely reflects a high systemic inflammatory burden driven by shared cytokines, particularly IL-4 and IL-13, which are pleiotropic mediators in both skin and airway inflammation, with their blockade being implicated in suppressing the atopic march.33 When systemic biological therapy suppresses this central pathway, patients experience a “dual-organ” benefit, leading to a more profound improvement in overall quality of life and symptom scores compared to those with isolated respiratory disease, as evidenced by significant enhancements in both asthma control and quality of life in patients treated for severe AD.34 This suggests that clinicians should view comorbid AD not merely as a burden, but as a marker of high biologic suitability.
Conversely, our model identified higher BMI as a negative predictor of response. This is consistent with emerging evidence in adults suggesting that “obese asthma” represents a distinct phenotype often characterized by non-T2 inflammation, oxidative stress, and mechanical factors, which are less responsive to current biologics.35,36 In pediatric populations, obesity promotes a systemic pro-inflammatory state mediated by leptin and IL-6 rather than Th2 cytokines.37 Our nomogram quantifies this negative impact, cautioning clinicians to manage expectations and consider weight management as an adjunct strategy in obese children receiving biologics.
The clinical utility of our nomogram is highlighted by the Decision Curve Analysis (DCA). The analysis showed that using the nomogram provides a higher net benefit than treating all patients or treating none across a wide range of probability thresholds. Practically, this means that for a child with “borderline” indications, the nomogram can help the physician and family visualize the probability of success. If the calculated probability is low (eg., <30%), alternative strategies such as allergen immunotherapy (AIT) or investigating alternative diagnoses might be prioritized over immediate biological therapy.
Our study has several limitations. First, as a retrospective single-center study, selection bias is inevitable Second, although we included the two most common biologics, we did not stratify the model by specific drug type due to sample size limitations; however, both drugs target the T2 axis, justifying the pooled analysis. Third, the follow-up period of 16 weeks focuses on early response; long-term remission rates warrant further investigation. Future multi-center prospective studies are needed to externally validate this tool.
Conclusion
In conclusion, we constructed a practical nomogram based on baseline FeNO, EOS, IgE, AD comorbidity, and BMI to predict early response to biologics in children with allergic AR and allergic asthma. This tool offers excellent predictive performance and clinical utility, aiding clinicians in identifying “super-responders” and optimizing resource allocation. The inclusion of AD status and BMI highlights the importance of a holistic, multimorbidity-focused approach in pediatric allergy management.
Abbreviation
ACT, Asthma Control Test; AD, Atopic Dermatitis; AR, Allergic Rhinitis; ARIA, Allergic Rhinitis and its Impact on Asthma; AUC, Area Under the Curve; BMI, Body Mass Index; C-index, Concordance Index; DCA, Decision Curve Analysis; EOS, Eosinophil count; FeNO, Fractional exhaled nitric oxide; GINA, Global Initiative for Asthma; IgE, Immunoglobulin E; IL, Interleukin; LASSO, Least Absolute Shrinkage and Selection Operator; ROC, Receiver Operating Characteristic; RQLQ, Rhinoconjunctivitis Quality of Life Questionnaire; TNSS, Total Nasal Symptom Score; VAS, Visual Analog Scale.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author, Shaofeng Liu, on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Institutional Ethics Committee of The First Affiliated Hospital of Wannan Medical University (Yijishan Hospital of Wannan Medical University) (No. 2025053) and was conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective nature of the study, and patient data were anonymized.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Lixin Wang and Zhaopeng Kang are co-first authors for this study. The authors declare that they have no competing interests for this work.
References
1. Tenero L, Vaia R, Ferrante G, et al. Diagnosis and management of allergic rhinitis in asthmatic children. J Asthma Allergy. 2023;16:45–11. doi:10.2147/JAA.S281439
2. Bousquet J, Schünemann HJ, Togias A, et al. Next-generation Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol. 2020;145(1):70–80.e73. doi:10.1016/j.jaci.2019.06.049
3. De Prins L, Raap U, Mueller T, et al. White paper on European patient needs and suggestions on chronic type 2 inflammation of airways and skin by EUFOREA. Front Allergy. 2022;3:889221. doi:10.3389/falgy.2022.889221
4. Pugin B, Deneyer L, Bachert C, et al. Patient advisory board for chronic rhinosinusitis - A EUFOREA initiative. Rhinology. 2019;57(5):331–335. doi:10.4193/Rhin19.012
5. Nur Husna SM, Md Shukri N, Mohd Ashari NS, Wong KK. IL-4/IL-13 axis as therapeutic targets in allergic rhinitis and asthma. PeerJ. 2022;10:e13444. doi:10.7717/peerj.13444
6. Fu Z, Xu Y, Cai C. Efficacy and safety of omalizumab in children with moderate-to-severe asthma: a meta-analysis. J Asthma. 2021;58(10):1350–1358. doi:10.1080/02770903.2020.1789875
7. Bacharier LB, Maspero JF, Katelaris CH, et al. Dupilumab in children with uncontrolled moderate-to-severe asthma. New Engl J Med. 2021;385(24):2230–2240. doi:10.1056/NEJMoa2106567
8. Fiocchi AG, Phipatanakul W, Zeiger RS, et al. Dupilumab leads to better-controlled asthma and quality of life in children: the VOYAGE study. Europ resp J. 2023;62(5):2300558. doi:10.1183/13993003.00558-2023
9. Zaazouee MS, Alwarraqi AG, Mohammed YA, et al. Dupilumab efficacy and safety in patients with moderate to severe asthma: a systematic review and meta-analysis. Front Pharmacol. 2022;13:992731. doi:10.3389/fphar.2022.992731
10. Ferrante G, Tenero L, Piazza M, Piacentini G. Severe pediatric asthma therapy: dupilumab. Front Pediatrics. 2022;10:963610. doi:10.3389/fped.2022.963610
11. Upham JW, Le Lievre C, Jackson DJ, Masoli M, Wechsler ME, Price DB. Defining a severe asthma super-responder: findings from a delphi process. J Allergy and Clin Immunol Prac. 2021;9(11):3997–4004. doi:10.1016/j.jaip.2021.06.041
12. Rattu A, Dixey P, Charles D, et al. Predictors of response to biologics for severe asthma: a systematic review and meta-analysis. Allergy. 2026;81(1):24–55. doi:10.1111/all.70031
13. Levy ML, Bacharier LB, Bateman E, et al. Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med. 2023;33(1):7. doi:10.1038/s41533-023-00330-1
14. Aigbirior J, Almaghrabi A, Lafi M, Mansur AH. The role of radiological imaging in the management of severe and difficult-to-treat asthma. Breathe. 2024;20(2):240033. doi:10.1183/20734735.0033-2024
15. Perikleous EP, Steiropoulos P, Nena E, Paraskakis E. Biologic therapies in pediatric asthma. J Personalized Med. 2022;12(6):999. doi:10.3390/jpm12060999
16. Couillard S, Laugerud A, Jabeen M, et al. Derivation of a prototype asthma attack risk scale centred on blood eosinophils and exhaled nitric oxide. Thorax. 2022;77(2):199–202. doi:10.1136/thoraxjnl-2021-217325
17. Guglielmo A, Deotto ML, Naldi L, et al. Biologics and small molecules treatment for moderate-to-severe atopic dermatitis patients with comorbid conditions and special populations: an Italian perspective. Dermatology Reports. 2024;16(2):9839. doi:10.4081/dr.2023.9839
18. Spergel JM, Du Toit G, Davis CM. Might biologics serve to interrupt the atopic march? J Allergy Clin Immunol. 2023;151(3):590–594. doi:10.1016/j.jaci.2023.01.001
19. Brozek JL, Bousquet J, Baena-Cagnani CE, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126(3):466–476. doi:10.1016/j.jaci.2010.06.047
20. Venkatesan P. 2023 GINA report for asthma. Lancet Respir Med. 2023;11(7):589. doi:10.1016/S2213-2600(23)00230-8
21. Dramburg S, Hilger C, Santos AF, et al. EAACI molecular allergology user’s guide 2.0. Pediatric Allergy Immunol. 2023;34 Suppl 28(Suppl 28):e13854. doi:10.1111/pai.13854
22. WHO Multicentre Growth Reference Study Group, de Onis M. Assessment of differences in linear growth among populations in the WHO multicentre growth reference study. Acta Paediatr Suppl. 2006;450:56–65. doi:10.1111/j.1651-2227.2006.tb02376.x
23. de Onis M. Development of a WHO growth reference for school-aged children and adolescents. Bulletin World Health Organiza. 2007;85(9):660–667. doi:10.2471/BLT.07.043497
24. Del Cuvillo A, Santos V, Montoro J, et al. Allergic rhinitis severity can be assessed using a visual analogue scale in mild, moderate and severe. Rhinology Journal. 2017;55(1):34–38. doi:10.4193/Rhin16.025
25. Bousquet PJ, Combescure C, Neukirch F, et al. Original article: visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy. 2007;62(4):367–372. doi:10.1111/j.1398-9995.2006.01276.x
26. Meltzer EO, Hampel FC, Ratner PH, et al. Safety and efficacy of olopatadine hydrochloride nasal spray for the treatment of seasonal allergic rhinitis. Ann Allergy Asthma Immunol. 2005;95(6):600–606. doi:10.1016/S1081-1206(10)61025-3
27. Juniper EF, Thompson AK, Ferrie PJ, Roberts JN. Validation of the standardized version of the rhinoconjunctivitis quality of life Questionnaire☆☆☆★. J Allergy Clin Immunol. 1999;104(2):364–369. doi:10.1016/S0091-6749(99)70380-5
28. Snelder SM, Weersink EJM, Braunstahl GJ. 4-month omalizumab efficacy outcomes for severe allergic asthma: the Dutch national omalizumab in asthma registry. Allergy Asthma Clin Immunol. 2017;13(1):34. doi:10.1186/s13223-017-0206-9
29. Hanania NA, Wenzel S, Rosén K, et al. Exploring the effects of omalizumab in allergic asthma: an analysis of biomarkers in the EXTRA study. Am J Respir Crit Care Med. 2013;187(8):804–811. doi:10.1164/rccm.201208-1414OC
30. Runnstrom M, Pitner H, Xu J, Lee FE, Kuruvilla M. Utilizing predictive inflammatory markers for guiding the use of biologicals in severe asthma. J Inflamm Res. 2022;15:241–249. doi:10.2147/JIR.S269297
31. Maison N, Omony J, Illi S, et al. T2-high asthma phenotypes across lifespan. Europ resp J. 2022;60(3):2102288. doi:10.1183/13993003.02288-2021
32. Delgado J, Dávila IJ, Domínguez-Ortega J. Clinical recommendations for the management of biological treatments in severe asthma patients: a consensus statement. J Invest Allergol Clin Immunol. 2021;31(1):36–43. doi:10.18176/jiaci.0638
33. Nakagome K, Nagata M. The possible roles of IL-4/IL-13 in the development of eosinophil-predominant severe asthma. Biomolecules. 2024;14(5):546. doi:10.3390/biom14050546
34. Dubini M, Benzecry V, Rivolta F, et al. Asthma improvement in patients treated with dupilumab for severe atopic dermatitis. Front Allergy. 2023;4:1223657. doi:10.3389/falgy.2023.1223657
35. Farzan S, Coyle T, Coscia G, Rebaza A, Santiago M. Clinical characteristics and management strategies for adult obese asthma patients. J Asthma Allergy. 2022;15:673–689. doi:10.2147/JAA.S285738
36. Alhamdan F, Marsh LM, Pedersen F, et al. Differential regulation of interferon signaling pathways in CD4(+) T cells of the low type-2 obesity-associated asthma phenotype. Int J Mol Sci. 2021;22(18):10144. doi:10.3390/ijms221810144
37. Bantulà M, Roca-Ferrer J, Arismendi E, Picado C. Asthma and obesity: two diseases on the rise and bridged by inflammation. J Clin Med. 2021;10(2):169. doi:10.3390/jcm10020169
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.