Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
A Clinical Comprehensive Evaluation of Long-Acting GLP-1 Receptor Agonists in Type 2 Diabetes Management
Authors Chen Q, Chen T ![]() , Lin W
, Lin W ![]() , Chen X
, Chen X
Received 30 November 2025
Accepted for publication 28 January 2026
Published 10 February 2026 Volume 2026:19 585436
DOI https://doi.org/10.2147/DMSO.S585436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Halis Akturk
Qiying Chen,1,* Tianyu Chen,2,* Weicheng Lin,1,* Xi Chen1
1Department of Pharmacy, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian, 362000, People’s Republic of China; 2Department of Nursing, Quanzhou Medical College, Quanzhou, Fujian, 362011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weicheng Lin, Department of Pharmacy, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, Fujian, 362000, People’s Republic of China, Email [email protected]
Objective: To conduct a systematic, multi-dimensional clinical evaluation of five long-acting glucagon-like peptide-1 receptor agonists (GLP-1RAs) available in China, providing evidence-based guidance for clinical preference and institutional formulary selection.
Methods: This study was structured according to the “A Quick Guideline for Drug Evaluation and Selection in Chinese Medical Institutions. (Second Edition)” and the “Guidelines for the Workflow of Clinical Comprehensive Evaluation of Drugs” We constructed a quantitative evaluation system encompassing six core dimensions: efficacy, safety, economy, innovation, suitability, and accessibility. Indicator weights were determined via a Delphi expert consultation process. Dulaglutide, semaglutide, polyethylene glycol loxenatide, tirzepatide, and mazdutide were evaluated using a 100-point scoring system based on drug labels, systematic literature review, and real-world data.
Results: The comprehensive scores were as follows: semaglutide (76.6), dulaglutide (72.6), polyethylene glycol loxenatide (64.8), tirzepatide (62.9), and mazdutide (55.1). Semaglutide and dulaglutide, classified as Strong Recommendations, demonstrated superior efficacy (particularly in cardio-renal protection) and overall value. Tirzepatide and polyethylene glycol loxenatide were Conditionally Recommended; the former shows outstanding potential for glycaemic control and weight loss but is limited by cost, while the latter offers advantages in accessibility and economy but lacks high-level cardiovascular outcome evidence. Mazdutide is Not Recommended currently due to insufficient evidence, absence from the national reimbursement drug list, and high cost.
Conclusion: This evaluation identifies semaglutide and dulaglutide as the preferred long-acting GLP-1RAs in China’s current therapeutic landscape. The standardized, transparent six-dimensional framework provides a replicable methodology for the comprehensive assessment of chronic disease therapies, supporting rational drug selection and resource allocation.
Keywords: type 2 diabetes, GLP-1 receptor agonists, long-acting formulations, clinical comprehensive evaluation, multi-criteria decision analysis
Introduction
Type 2 diabetes mellitus (T2DM) constitutes a formidable and expanding public health threat in China, underpinned by the core pathophysiological duet of insulin resistance and progressive β-cell failure.1–3 Cardiovascular disease (CVD) looms as the most prevalent and grave complication of this metabolic disorder, sharply elevating mortality and imposing a heavy burden on healthcare systems. Contemporary management of T2DM thus demands a dual mission: achieving stringent glycaemic control while concurrently delivering robust cardiovascular risk reduction.4–7
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have ascended to the forefront of this therapeutic paradigm. Both the 2024 Chinese guidelines and the 2025 American Diabetes Association (ADA) Standards of Care throw considerable weight behind these agents, championing their proven capacity to improve glycaemic parameters, confer cardiovascular protection, and facilitate weight management.8,9 The guidance leaves little room for ambiguity: clinicians should favour GLP-1RAs with established cardiovascular benefit for individuals grappling with atherosclerotic cardiovascular disease (ASCVD) or perched high on the CV risk spectrum.
This work confronts an unmistakable shift in practice: long-acting weekly GLP-1RA formulations are steadily cementing their role as foundational elements of T2DM care.10,11 They stand in stark contrast to their short-acting counterparts, which zero in on postprandial glucose excursions. The weekly agents, instead, enforce a continuous and stable command over both fasting and postprandial glucose levels. Their user-friendly, once-weekly schedule fosters superior long-term treatment persistence—a paramount virtue in managing a lifelong condition.12–14 Mirroring this clinical advantage, the 2025 ADA guidelines, leaning on a formidable body of evidence, assign a preferential status to long-acting GLP-1RAs such as semaglutide and high-dose dulaglutide.15 Their standout efficacy and compelling track record in cardio-renal outcome trials herald a new chapter in T2DM management—a decisive pivot from a myopic “glucose-centric” view to a holistic strategy that champions long-term organ preservation.16,17 A systematic, multi-angled appraisal of these leading weekly agents is therefore not only warranted but urgently needed to navigate this evolving terrain.18
Within this context, we turn our spotlight onto the five dominant once-weekly GLP-1RA formulations accessible in the Chinese market: dulaglutide, semaglutide, polyethylene glycol loxenatide, tirzepatide, and mazdutide. While united by their engagement with the GLP-1 receptor, each agent carves out a unique profile defined by its molecular architecture, pharmacokinetic behaviour, potency, safety footprint, and economic implications.19–22 Dulaglutide rests on a wealth of real-world experience garnered as a pioneer; semaglutide is distinguished by unassailable cardio-renal outcome data; tirzepatide, a dual GIP/GLP-1 receptor agonist, posts remarkable figures in glucose reduction and weight loss; meanwhile, the home-grown contenders—polyethylene glycol loxenatide and mazdutide (a GCG/GLP-1 dual agonist)—embody novel therapeutic pathways.23,24
A conspicuous evidence void persists: the scarcity of a systematic, head-to-head juxtaposition of these five agents across multiple domains. This gap directly undercuts informed clinical choices and rational drug selection in healthcare institutions. Comprehensive clinical drug evaluation emerges as the pivotal methodology to bridge this divide, weaving together evidence from six core pillars: safety, effectiveness, economy, innovation, suitability, and accessibility.25 While China has sketched preliminary evaluation frameworks for cardiovascular agents, anticancer drugs, and paediatric medicines, a standardized template for T2DM therapeutics remains conspicuously absent.
Therefore, a systematic and quantitative head-to-head comparison of these five dominant once-weekly GLP-1RA formulations across multiple domains is warranted. Although abundant evidence from meta-analyses and cardiovascular outcome trials exists for GLP-1 receptor agonists, it often focuses on single therapeutic endpoints or comparisons across broad drug classes. This makes it difficult to directly support holistic trade-offs and optimal selection decisions regarding the clinical and health economic value of these five specific weekly formulations available in China. This study aims to construct and apply a standardized six-dimensional evaluation framework to fill this specific evidence gap and provide integrated evidence for clinical practice and health policy decisions. We pursue two overarching goals: first, to plug the comparative evidence gap and furnish clear directives for clinical practice and reimbursement policy; second, to forge a transferable “T2DM Therapeutic Drug Evaluation Toolkit” that can serve as a methodological blueprint for the systematic assessment of chronic disease pharmacotherapies.
Materials and Methods
Evaluation Framework Development
Our methodology builds upon the structured, quantitative framework established by the “A Quick Guideline for Drug Evaluation and Selection in Chinese Medical Institutions (Second Edition)”.26 To enhance comprehensiveness, we integrated core principles from the “Guidelines for the Workflow of Clinical Comprehensive Evaluation of Drugs”25 and incorporated relevant clinical guidelines and literature evidence. This process established our preliminary evaluation framework centered on six primary dimensions: efficacy, safety, economy, innovation, suitability, and accessibility, which subsequently informed the Delphi process for indicator specification and weighting. This six-dimensional framework is designed to account for the pharmacological and clinical heterogeneity among the evaluated agents (including single and dual receptor agonists). By encompassing a broad range of indicators—from glycemic control and weight loss to cardio-renal outcomes and innovative mechanisms—the system ensures a fair and comparable assessment of comprehensive value within a unified structure.
Indicator Weight Determination
A multidisciplinary Delphi panel was convened, consisting of 10 experts with senior professional titles and more than 10 years of relevant experience in diabetes management or related fields. The panel included clinical experts (3 clinical pharmacists, 3 endocrinologists, and 2 cardiologists) from tertiary hospitals, as well as 2 experts in drug policy and health technology assessment from academic institutions. Consensus on the evaluation indicators and their respective weights was achieved through multiple rounds of the Delphi process, which continued until the coefficient of variation for all items was below 0.15, thereby finalizing the evaluation system.27
Evaluation Implementation
Two independently trained researchers conducted blinded assessments using the finalized evaluation system, assigning scores across all dimensions. Discrepancies exceeding 2 points triggered joint data review and consensus formation, with final scores representing the average of both assessments.
Data Sources and Criteria
We structured our evidence collection around a “label-first, literature-supported” framework. For core drug profiles—including approved indications, mechanisms of action, and pharmacokinetic properties—we drew directly from the latest official product labels (updated as of September 2025). To build a more complete picture of real-world effectiveness and safety, we supplemented this foundation with data from systematic searches across major Chinese and English databases, including CNKI, PubMed, Embase, and the Cochrane Library. We graded adverse events according to CTCAE v5.0 criteria to ensure consistent safety profiling. For special populations, we implemented a three-tiered evaluation system based directly on label recommendations. Finally, our economic analysis focused on calculating weekly treatment expenses, while also integrating insights from existing pharmacoeconomic studies.
Sensitivity Analysis
To assess the robustness of the comprehensive evaluation results with respect to potential variations in the weighting of the primary dimensions, a one-way sensitivity analysis was conducted. The weight assigned to each of the six primary dimensions (Efficacy, Safety, Economy, Innovation, Suitability, and Accessibility) was independently increased and decreased by ±10% and ±20% from its baseline value derived from the Delphi process. For each variation, the weights of the remaining five dimensions were adjusted proportionally so that the sum of all dimension weights remained 100%. Under every altered weighting scenario, the comprehensive score for each of the five GLP-1RAs was recalculated, and the resulting rankings were compared with the baseline ranking.
Results
Evaluation System Construction
We successfully established a comprehensive clinical evaluation system for GLP-1RA weekly formulations, comprising 6 primary dimensions, 14 secondary dimensions, and 36 tertiary indicators with complete weight assignments across all levels. The six-round Delphi process demonstrated strong expert engagement (authority coefficient=0.75; ≥0.7 indicates high reliability), with favorable importance and feasibility scores supporting the system’s robustness.28 Detailed indicator specifications and weights are presented in Table 1.
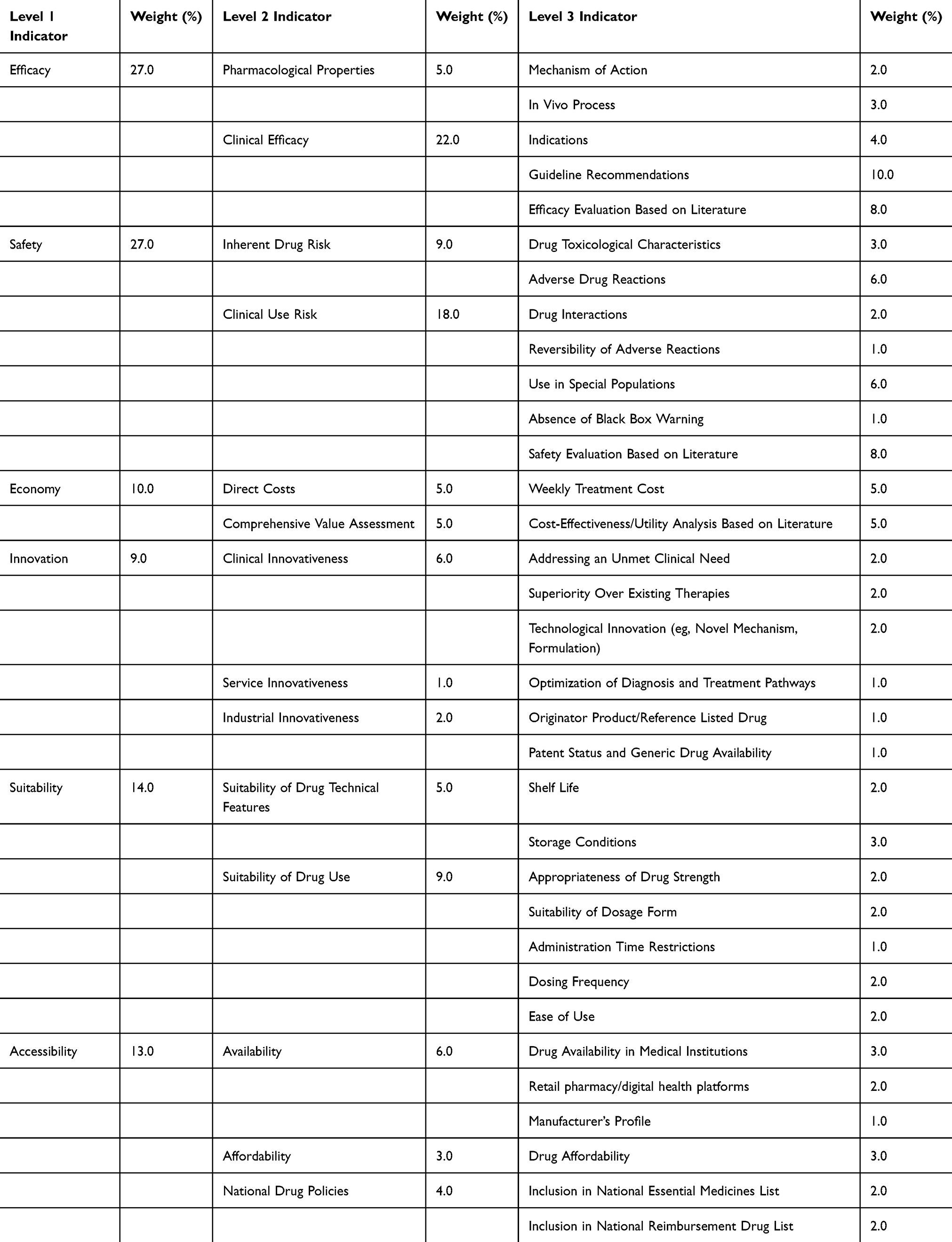 |
Table 1 Indicators and Weight Assignment of Drug Clinical Comprehensive Evaluation at All Levels |
Efficacy Evaluation
Pharmacological Properties
All five agents share the core indication of glycemic control in adults with type 2 diabetes mellitus through selective activation of the GLP-1 receptor. Tirzepatide and mazdutide further broaden their therapeutic potential through dual-receptor agonism—targeting GIP/GLP-1 and GCG/GLP-1, respectively—offering enhanced metabolic benefits beyond conventional GLP-1RAs. Semaglutide, tirzepatide, and mazdutide also carry formal approval for chronic weight management. Notably, semaglutide stands out with an additional indication for cardiovascular risk reduction in T2DM patients with established cardiovascular disease or chronic kidney disease, while tirzepatide is uniquely indicated for obesity accompanied by moderate-to-severe obstructive sleep apnea. All agents exhibit well-characterized and predictable pharmacokinetic properties.
Guideline Recommendations
Major national and international guidelines now consistently recognize once-weekly GLP-1RA formulations as foundational therapies in T2DM management. For cardiovascular risk reduction, Chinese, ADA, AHA/ACC, and ESC guidelines uniformly advise prioritizing dulaglutide, semaglutide, or tirzepatide in patients with ASCVD (Class I, Level A).29,30 In the realm of weight management, tirzepatide and semaglutide earn strong endorsements based on compelling efficacy data.8,9,30,31 For renal protection, dulaglutide and semaglutide again receive high-level guideline support.8,9,30 Polyethylene glycol loxenatide is currently recognized primarily for glucose-lowering, with broader recommendation pending results from the ongoing BALANCE-3 cardiovascular outcomes trial.32 Despite promising Phase II results suggesting superiority to semaglutide in both glycemic control and weight loss, mazdutide awaits formal guideline inclusion pending peer-reviewed publication of the DREAMS-3 trial and further evidence on cardiovascular outcomes.33
Evidence-Based Efficacy Assessment
Glucose-lowering efficacy varies meaningfully across agents. Semaglutide demonstrates powerful HbA1c reductions throughout the SUSTAIN clinical program,34–37 while dulaglutide shows sustained glycemic control across the AWARD trials.38–41 Tirzepatide reveals superior glucose-lowering compared to dulaglutide in the SURPASS-CVOT study.42 Phase II data for mazdutide confirm its HbA1c reduction exceeds that of placebo,43 whereas evidence for polyethylene glycol loxenatide, though more limited, still indicates significant placebo-adjusted HbA1c reductions of 1.02–1.34% as reported by Ying et al.44
Cardiovascular outcomes evidence also differs considerably. Both dulaglutide (REWIND)36 and semaglutide (SUSTAIN 6)45 demonstrate significant risk reduction in major adverse cardiovascular events (MACE). Tirzepatide met its primary non-inferiority endpoint versus dulaglutide in SURPASS-CVOT, with an encouraging 16% reduction in all-cause mortality risk also observed.42 Cardiovascular outcomes for polyethylene glycol loxenatide await results from BALANCE-3, though real-world data hint at potential MACE risk reduction.46 Evidence for mazdutide continues to develop through ongoing trials.
Weight loss effects span a wide spectrum. Tirzepatide leads the field with substantial reductions of 11–13% in the SURPASS and SURMOUNT trials,47–54 followed by semaglutide with 6–8% weight loss in the SUSTAIN program.34–37 Phase II data for mazdutide indicate approximately 7% placebo-adjusted weight loss,43 while dulaglutide (3–4.5% in AWARD)38–41 and polyethylene glycol loxenatide (3–5% as secondary endpoints)44,46 show more moderate effects, with the latter limited by its current evidence base.
In the area of apnea management, only tirzepatide currently possesses Phase III evidence (SURMOUNT-OSA) demonstrating significant improvement in the apnea-hypopnea index (AHI).55 The GLORY-OSA trial for mazdutide remains ongoing, while the other agents have not been systematically evaluated for OSA. For a complete comparative scoring across all efficacy endpoints, please refer to Table 2.
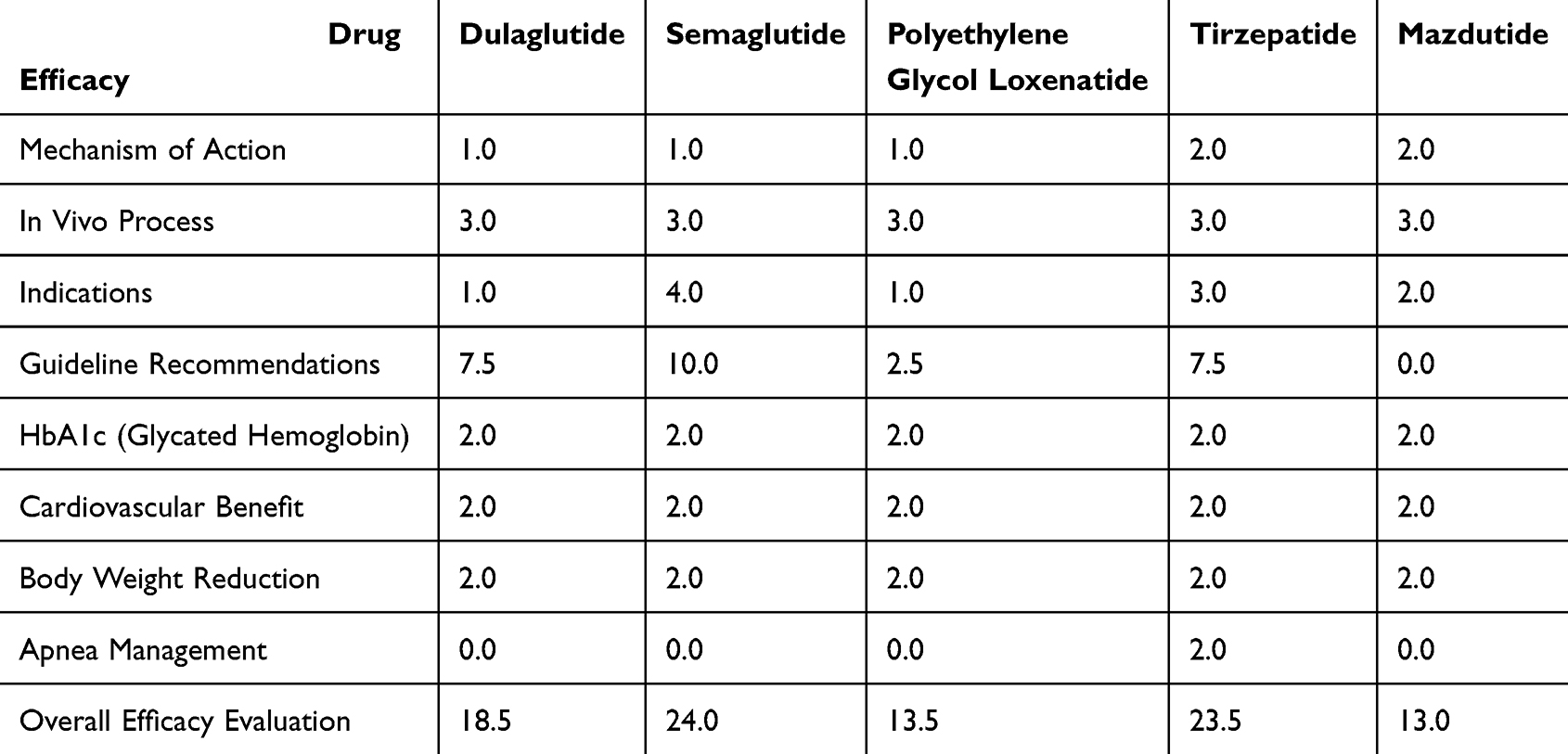 |
Table 2 Results of the Efficacy Evaluation for the Five Once-Weekly GLP-1RA Formulations |
Safety Evaluation
Toxicological Profile
Non-clinical data show generally consistent safety characteristics across all five agents. Standard genetic toxicity tests returned negative results for semaglutide, polyethylene glycol loxenatide, tirzepatide, and mazdutide. Dulaglutide, as an Fc-fusion protein, was exempt from such testing based on regulatory guidelines. All compounds demonstrated increased incidence of thyroid C-cell tumors in rodent models, though the clinical relevance of these findings in humans remains uncertain. Animal reproductive studies suggest potential risks to embryonic development across the class.
Adverse Event Spectrum
The safety profile across this drug class remains favorable overall, though we observed notable differences between agents. Mild-to-moderate gastrointestinal events—including nausea, diarrhea, vomiting, and abdominal distension—represent the most frequently reported adverse effects. These typically occur in >10% of patients, mainly during the dose-escalation phase, and tend to subside during maintenance treatment. Mazdutide showed the highest incidence (63%), while polyethylene glycol loxenatide demonstrated the lowest (13–28%, varying by dose). Tirzepatide maintained consistently elevated GI event rates across doses (~56%). Most events were mild to moderate (CTCAE grades 1–2, >80%), with severe (grade 3) events being uncommon (<5%) and no grade 4–5 events reported. GI symptoms were generally transient and resolved during continued therapy.
Serious adverse event risk remains reassuringly low. Pancreatitis was infrequently reported with dulaglutide, semaglutide, and tirzepatide (0.07–0.3%). Acute kidney injury and severe hypersensitivity reactions were rare (<0.1%). Polyethylene glycol loxenatide and mazdutide showed particularly favorable profiles in these areas, with minimal events reported. Hypoglycemia risk remained low during monotherapy for all agents, increasing only modestly when combined with insulin or sulfonylureas, without frequent severe episodes.
Drug-Drug Interactions
All five agents delay gastric emptying, which may affect how well other oral drugs are absorbed. That said, clinically meaningful interactions with commonly used medications—such as atorvastatin and warfarin—appear infrequent. We still advise careful monitoring when administering narrow-therapeutic-index drugs or emergency medications that require rapid absorption.
Special Populations
All five agents are contraindicated during pregnancy and lactation. Only dulaglutide carries formal approval for use in adolescents (≥10 years); the other agents lack adequate safety and efficacy data in patients under 18. Most elderly patients do not require dose adjustment. For renal impairment, no dose adjustment is needed in mild-to-moderate cases. In severe renal impairment, dulaglutide, semaglutide, and mazdutide should be used with caution; tirzepatide should be avoided. Polyethylene glycol loxenatide may continue to be used without dose adjustment, though individual assessment is recommended. For hepatic impairment, no adjustment is required in mild-to-moderate cases. In severe impairment, monitoring is advised for polyethylene glycol loxenatide, and caution is recommended for other agents in the absence of formal dosing guidance.
Literature-Based Safety Assessment
Recent network meta-analyses by Yao56 and Xie57,58 support the overall safety profile described above. Yao’s work further clarifies that GI tolerability differs between agents: nausea and vomiting were more typical with dulaglutide, semaglutide, and tirzepatide, whereas polyethylene glycol loxenatide and mazdutide were associated with milder symptoms.56 Xie’s analysis confirms that overall adverse event rates, serious adverse events, hypoglycemia, and treatment discontinuation were comparable to placebo. Mild-to-moderate gastrointestinal events emerged as the primary safety consideration across the class.57,58 Comprehensive safety scores across all evaluated dimensions are as detailed in Table 3.
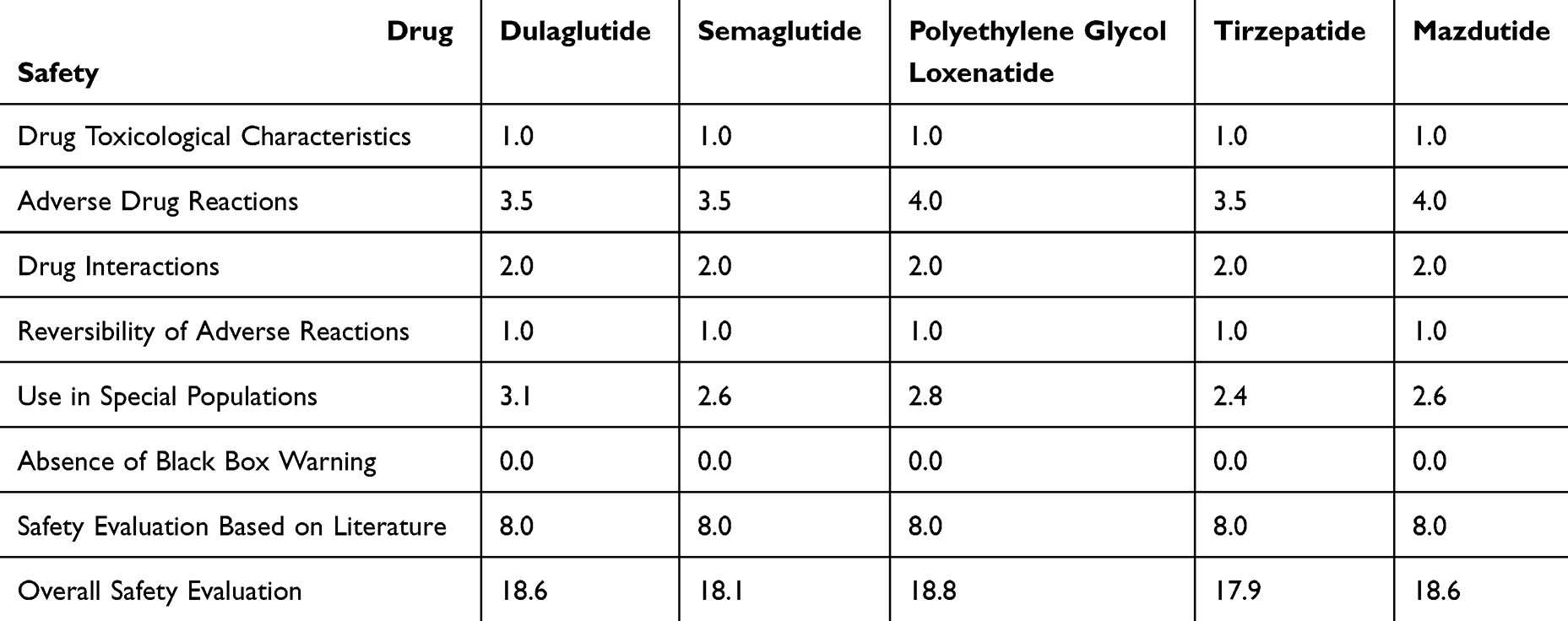 |
Table 3 Results of the Safety Evaluation for the Five Once-Weekly GLP-1RA Formulations |
Economic Evaluation
Weekly Treatment Costs
Substantial variation exists in the weekly drug costs of the five agents, according to data from relevant Chinese pharmaceutical procurement platforms as of September 2025. The specific weekly costs are as follows: dulaglutide (123.35 CNY), polyethylene glycol loxenatide (139.00 CNY), semaglutide (179.00 CNY), mazdutide (730.00 CNY), and tirzepatide (939.50 CNY). This price disparity is largely attributable to inclusion in the National Reimbursement Drug List (NRDL), which has led to significant price reductions for dulaglutide, polyethylene glycol loxenatide, and semaglutide following national negotiations. In contrast, the newer agents (tirzepatide and mazdutide), having only recently entered the market and not yet undergone the national price negotiation process, maintain substantially higher price points.
Cost-Utility Analysis
In pharmacoeconomic evaluations, drug price is a pivotal yet volatile factor, susceptible to significant temporal shifts following price negotiations and substantial cross-national disparities. Given that these variations can yield divergent or even contradictory conclusions, our analysis strategically prioritized the most recent China-specific pharmacoeconomic studies to ensure the assessment reflected current local pricing and the domestic healthcare system perspective. The evidence synthesized demonstrates semaglutide’s cost-effectiveness advantage over dulaglutide under updated NRDL pricing59 and its superior long-term economy compared to polyethylene glycol loxenatide.60 For the dulaglutide versus polyethylene glycol loxenatide comparison, while no direct pharmacoeconomic study was identified, dulaglutide’s lower unit price combined with its superior efficacy in reducing HbA1c, body weight, and fasting blood glucose as shown in a network meta-analysis56 supports the inference of its more favorable cost-effectiveness profile. Although robust pharmacoeconomic data are lacking for tirzepatide and mazdutide, their substantial cost premiums (7.6x and 5.9x that of dulaglutide, respectively) present significant economic challenges, culminating in the comprehensive ranking: semaglutide > dulaglutide > polyethylene glycol loxenatide > mazdutide > tirzepatide, with detailed scoring in Table 4.
 |
Table 4 Results of the Economy Evaluation for the Five Once-Weekly GLP-1RA Formulations |
Innovation Evaluation
Our multi-dimensional assessment brings into clear view the distinct innovative profiles that differentiate these therapies. Tirzepatide and mazdutide stand out as notable advances in pharmacology, achieving dual-receptor agonism that delivers metabolic benefits exceeding the scope of conventional GLP-1RAs. Dulaglutide and semaglutide, meanwhile, have cemented their foundational role in modern care through landmark cardiovascular outcome trials, securing their status as standards for managing patients with ASCVD.
A leap in patient-centered design is embodied by semaglutide’s oral formulation, which marks a genuine departure from injectable peptides. The underlying technological strategies are equally diverse: semaglutide relies on fatty acid side-chain modification for prolonged action; dulaglutide and mazdutide adopt Fc-fusion technology that capitalizes on natural FcRn recycling; tirzepatide integrates engineered amino acids paired with fatty acid chains; and polyethylene glycol loxenatide reflects home-grown innovation through its PEGylation strategy. Together, these advances have collectively shifted T2DM management away from complex daily regimens toward simple weekly dosing—a change that tangibly supports sustained treatment adherence and improves day-to-day life. For a complete analysis across all innovation criteria, see Table 5.
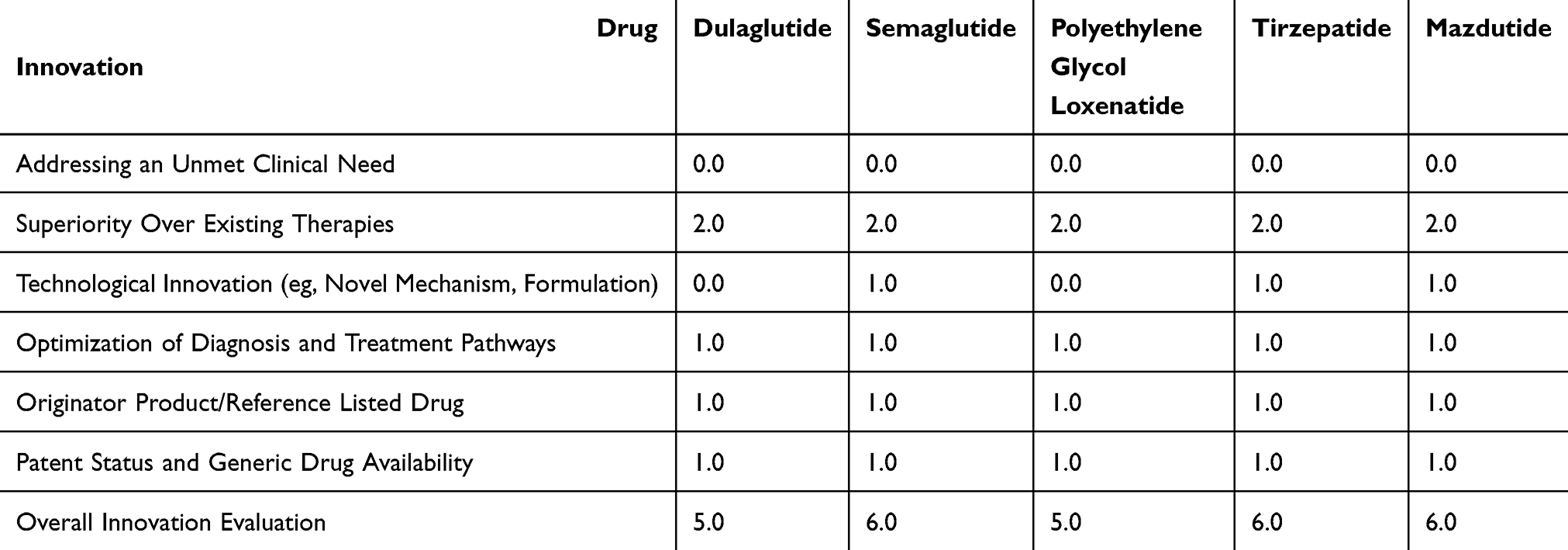 |
Table 5 Results of the Innovation Evaluation for the Five Once-Weekly GLP-1RA Formulations |
Suitability Evaluation
All five agents share a clinically friendly profile, being supplied as injectable solutions with straightforward storage needs (2–8°C refrigeration, no freezing). Among them, semaglutide stands out with the longest shelf life—36 months compared to the standard 24 months for its counterparts. Each product comes with a thoughtfully designed pre-filled pen, making administration straightforward and supporting reliable self-management. The shared once-weekly subcutaneous schedule, which does not require planning around meals, meaningfully lowers the treatment burden and strongly encourages consistent, long-term use. For a full breakdown across all suitability metrics, please refer to Table 6.
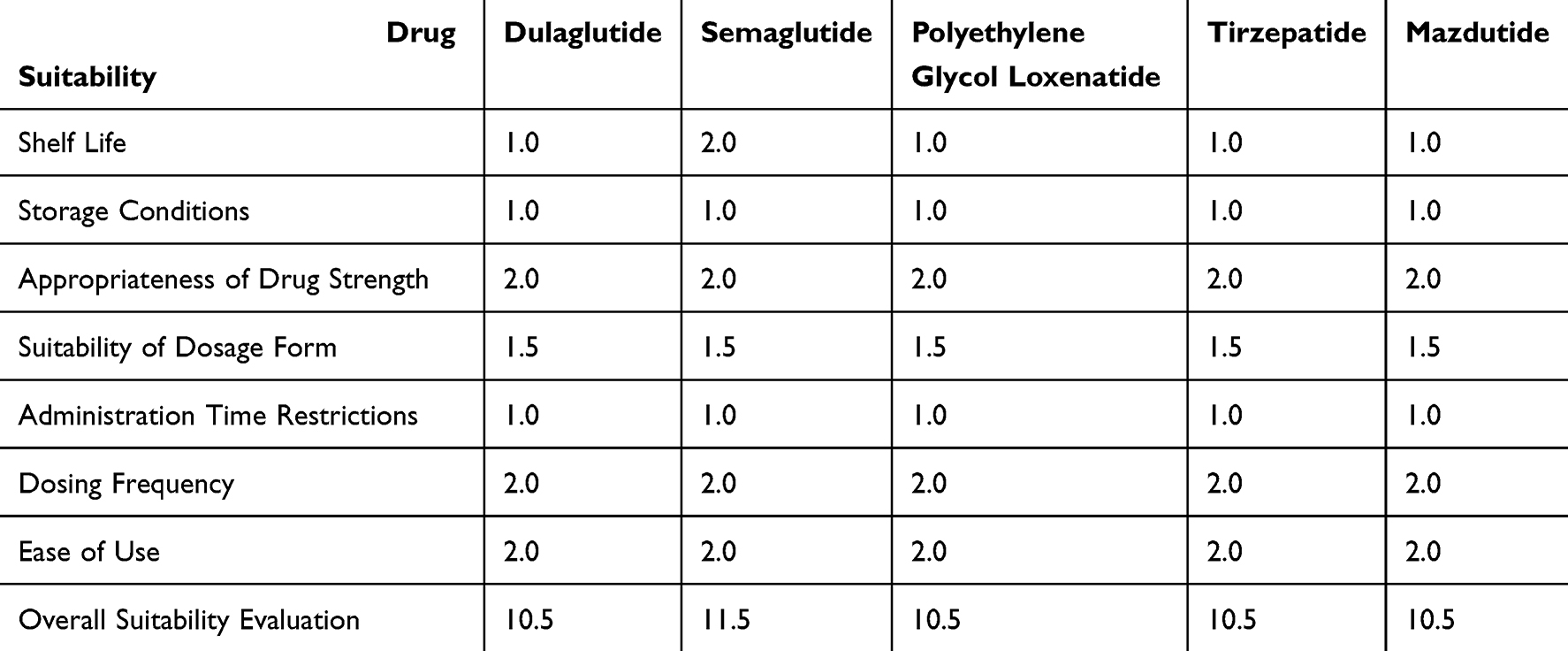 |
Table 6 Results of the Suitability Evaluation for the Five Once-Weekly GLP-1RA Formulations |
Accessibility Evaluation
Availability
Recent reforms in China’s healthcare policy, particularly dynamic updates to the NRDLand the relaxation of institutional drug procurement rules, have meaningfully broadened patient access to innovative therapies. Against this favorable backdrop, the availability of long-acting weekly GLP-1RAs within Chinese medical institutions continues to grow. Earlier entrants with proven cardiovascular benefits—dulaglutide and semaglutide—now enjoy widespread adoption in secondary and tertiary hospitals. Meanwhile, the domestically developed polyethylene glycol loxenatide is steadily gaining ground, with its hospital presence expanding. Newer agents such as tirzepatide and mazdutide are creatively navigating initial formulary barriers by increasingly turning to retail pharmacy networks and digital health platforms, thereby offering patients alternative pathways to treatment even before full hospital integration.
Affordability
In China, inclusion in the NRDL remains the single most critical factor shaping treatment affordability. For the three agents currently listed—dulaglutide, semaglutide, and polyethylene glycol loxenatide—significant price reductions following national negotiation, coupled with insurance coverage, have brought patient out-of-pocket costs within a more manageable range. Relative to the 2024 national disposable income per capita (CNY 41,314), co-payments for these therapies account for approximately 6% to 9% of an individual’s annual income. In stark contrast, agents not yet on the NRDL, namely tirzepatide and mazdutide, must be paid for entirely out-of-pocket. Their annual treatment cost represents a staggering 92% to 118% of the average income, presenting a profound financial barrier for most patients. Unsurprisingly, the affordability ranking mirrors NRDL status directly: dulaglutide (6%) > polyethylene glycol loxenatide (7%) > semaglutide (9%) > mazdutide (92%) > tirzepatide (118%). Detailed metrics are available in Table 7.
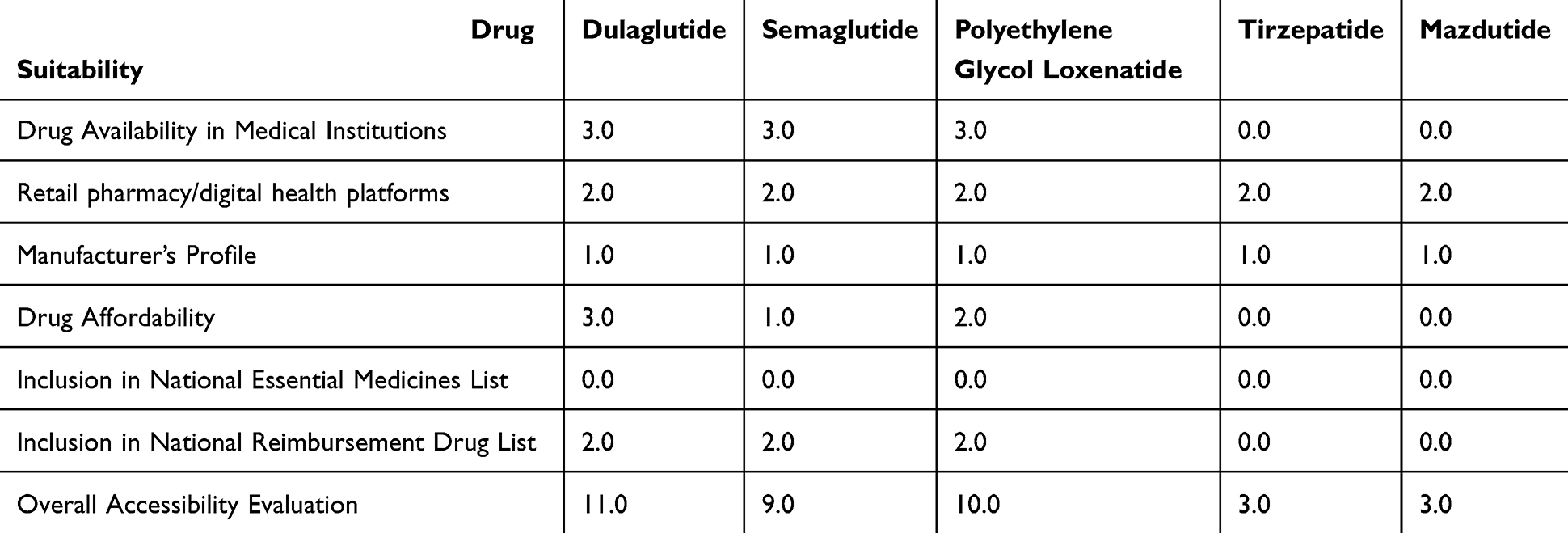 |
Table 7 Results of the Accessibility Evaluation for the Five Once-Weekly GLP-1RA Formulations |
Comprehensive Scoring Outcomes
Our integrated six-dimensional evaluation, as detailed in Figure 1, reveals the following overall scores: semaglutide (76.6), dulaglutide (72.6), polyethylene glycol loxenatide (64.8), tirzepatide (62.9), and mazdutide (55.1). Applying pre-defined thresholds,25,26 we classify semaglutide and dulaglutide as “Strong Recommendations” for priority use in clinical practice. Polyethylene glycol loxenatide and tirzepatide each secure a “Conditional Recommendation,” supporting their application in contexts where individual patient factors align with their specific profiles. Mazdutide, while not currently meeting the threshold for formal recommendation, holds promise due to its innovative mechanism and deserves continued assessment.
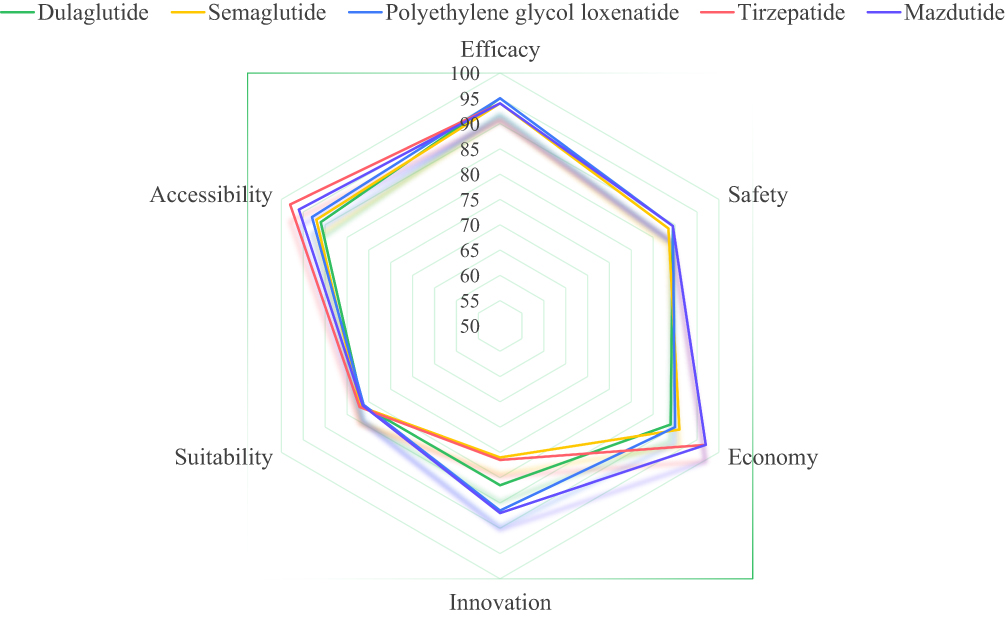 |
Figure 1 Radar Chart of the Six-Dimensional Comprehensive Evaluation for Five Once-Weekly GLP-1RA Formulations. |
Sensitivity Analysis Results
The one-way sensitivity analysis demonstrated that the overall ranking of the five long-acting GLP-1RAs was robust to plausible changes in the dimension weights. Semaglutide and dulaglutide retained their first and second positions, respectively, across all tested scenarios (±10% and ±20% variation for each primary dimension), thereby reinforcing their classification as “Strong Recommendations.” No rank reversal was observed for these two agents under any of the weighting adjustments. The positions of the remaining three agents (tirzepatide, polyethylene glycol loxenatide, and mazdutide) relative to one another remained consistent with the original “Conditionally Recommended” or “Not Recommended” categorizations in the vast majority of scenarios. These results confirm that the key conclusions of the comprehensive evaluation are not sensitive to reasonable uncertainty in the weighting of the six primary dimensions.
Discussion
Our evaluation, which specifically targeted long-acting weekly GLP-1RAs, identifies semaglutide and dulaglutide as the top-performing agents. This finding aligns well with prior studies that applied earlier editions of A Quick Guideline for Drug Evaluation and Selection in Chinese Medical Institutions.61,62 Notably, while those earlier analyses included both short- and long-acting GLP-1RAs, our work focused exclusively on the weekly formulations that now form the therapeutic backbone of modern T2DM management. This specific focus, coupled with the inclusion of the newest agents (tirzepatide and mazdutide), allows us to provide a timely and clinically pertinent update that reflects the rapid evolution of this drug class.
A deeper interpretation of the six-dimensional scores reveals the distinct value proposition of each agent. Semaglutide claimed the top position primarily on the strength of its exceptional Efficacy score, supported by superior data and strong guideline endorsements for glycemic control, weight loss, and cardio-renal protection. Dulaglutide, in contrast, achieved its high ranking through a remarkably balanced profile, with its strongest contributions in Safety and Economy, positioning it as a versatile and cost-effective cornerstone for T2DM management. The evaluation further illuminates the critical trade-offs inherent in drug value. Tirzepatide presents a striking example of this dichotomy, achieving top-tier scores in Efficacy and Innovation, yet counterbalanced by its lowest scores in Economy and Accessibility, creating a “high-efficacy, high-cost” profile that currently constrains its widespread use. Conversely, Mazdutide’s primary limitation is its immature evidence base. Despite a promising Innovation score and a solid Safety profile, its overall standing is hampered by the absence of published Phase III results, ongoing accumulation of cardiovascular outcomes data, and a consequent lack of formal guideline recognition. Polyethylene Glycol Loxenatide occupies a unique niche, with primary advantages in strong Accessibility and acceptable Economy, though its utility for patients at highest CV risk is limited by the lack of confirmed cardiovascular outcome benefit within the Efficacy dimension. These nuanced findings provide a multi-dimensional blueprint for institutional formulary decisions, strongly endorsing the preferential selection of semaglutide and dulaglutide, while facilitating a more informed, patient-centric application strategy for conditionally recommended drugs.
This study establishes a pragmatic evaluation framework by integrating two complementary methodological paradigms. We built upon the efficient, quantitative structure of the A Quick Guideline for Drug Evaluation and Selection in Chinese Medical Institutions (Second Edition) and enriched it with the systematic principles of the Guideline for the Workflow Clinical Comprehensive Evaluation of Drugs. This hybrid model effectively balances the need for a standardized, rapid assessment with the depth required for a comprehensive multi-dimensional comparison. This approach enables a focused and contemporary evaluation of the dominant long-acting weekly GLP-1RAs. More importantly, it provides a structured, transparent, and sustainable mechanism for clinicians and healthcare policymakers to incorporate new evidence and agents as they emerge.
The quantitative scores and categorical recommendations (eg, Strong Recommendation, Conditionally Recommended) generated here provide a transparent, multi-dimensional evidence base for decision-making. Hospital Pharmacy and Therapeutics (P&T) Committees can utilize this profile for formulary management, while the results can also inform broader policy discussions regarding drug access and reimbursement.
This study has several limitations. First, the economic and accessibility scores are sensitive to drug pricing and inclusion status in the NRDL, which are dynamic factors. Second, as a snapshot evaluation based on evidence available up to September 2025, its conclusions may evolve with the publication of new key randomized controlled trial (RCT) results (eg, DREAMS-3 for mazdutide, BALANCE-3 for polyethylene glycol loxenatide) and updates to major diabetes management guidelines. These factors collectively underscore the need for regular, dynamic re-evaluation of chronic disease therapies.
Conclusion
This study applied a standardized six-dimensional framework to evaluate long-acting GLP-1RAs in China, identifying semaglutide and dulaglutide as the agents with the strongest comprehensive value and solidifying their status as preferred “Strong Recommendation” choices. This finding is grounded in a direct, quantitative comparison across all six assessment dimensions.
The implications of this work are twofold. Primarily, it provides an evidence-based, multi-criteria ranking to directly guide therapeutic selection and institutional drug procurement. Furthermore, by synthesizing methodologies from A Quick Guideline for Drug Evaluation and Selection in Chinese Medical Institutions and the Guidelines for the Workflow of Clinical Comprehensive Evaluation of Drugs, it establishes a transferable methodological template for the systematic assessment of other chronic disease therapies.
To maintain its utility, this evaluation should be revisited periodically to incorporate emerging long-term outcome data, real-world evidence, and changes in key determinants of access, particularly drug pricing and NRDL inclusion status.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding or first author on reasonable request.
Author Contributions
Chen, Qiying: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing – Original Draft, Writing – review and editing. Chen, Tianyu: Conceptualization, Methodology, Data Curation, Investigation, Formal Analysis, Validation Writing – Original Draft, Writing – review and editing. Chen, Xi: Methodology, Writing – Review and Editing, Investigation, Visualization. Lin, Weicheng: Methodology, Data Curation, Formal Analysis, Writing – Original Draft, Writing – review and editing, Investigation, Supervision. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Startup Fund for Scientific Research, Fujian Medical University (Grant Number:2022QH1124).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Holman RR, Clark A, Rorsman P. β-cell secretory dysfunction: a key cause of type 2 diabetes. Lancet Diabetes Endocrinol. 2020;8(5):370. doi:10.1016/S2213-8587(20)30119-4
2. Shao X, Wang Y, Huang S, et al. Development and validation of a prediction model estimating the 10-year risk for type 2 diabetes in China. PLoS One. 2020;15(9):e0237936. doi:10.1371/journal.pone.0237936
3. Li X, Xue Y, Dang Y, et al. Association of Non-Insulin-Based Insulin Resistance Indices with Risk of Incident Prediabetes and Diabetes in a Chinese Rural Population: a 12-Year Prospective Study. Diabetes Metabol Syndrome Obesity. 2022;15:3809–14. doi:10.2147/DMSO.S385906
4. Sharma A, Zheng Y, Ezekowitz JA, et al. Cluster Analysis of Cardiovascular Phenotypes in Patients With Type 2 Diabetes and Established Atherosclerotic Cardiovascular Disease: a Potential Approach to Precision Medicine. Diabetes Care. 2022;45(1):204–212. doi:10.2337/dc20-2806
5. Wong ND, Sattar N. Cardiovascular risk in diabetes mellitus: epidemiology, assessment and prevention. Nat Rev Cardiol. 2023;20(10):685–695. doi:10.1038/s41569-023-00877-z
6. Mader A, Haeberli D, Larcher B, et al. Contribution of type 2 diabetes to major adverse cardiovascular events (MACE) in a long-term observational study with different stages of atherosclerosis. Sci Rep. 2025;15(1):2792. doi:10.1038/s41598-024-84985-x
7. Ke J, Ruan X, Wu K, et al. Prospective cohort studies underscore the association of abnormal glycemic measures with all-cause and cause-specific mortalities. iScience. 2024;27(7):110233. doi:10.1016/j.isci.2024.110233
8. Chinese Diabetes Society. Guideline for the prevention and treatment of diabetes mellitus in China (2024 edition). Chin J Diabet. 2025;17(1):16–139. doi:10.3760/cma.j.cn115791-20241203-00705.
9. American Diabetes Association Professional Practice Committee. Pharmacologic Approaches to Glycemic Treatment: standards of Care in Diabetes-2025. Diabetes Care. 2025;48(Suppl 1):S181–S206. doi:10.2337/dc25-S009.
10. Kosiborod MN, Petrie MC, Borlaug BA, et al. Semaglutide in Patients with Obesity-Related Heart Failure and Type 2 Diabetes. N Engl J Med. 2024;390(15):1394–1407. doi:10.1056/NEJMoa2313917
11. Jastreboff AM, le Roux CW, Stefanski A, et al. Tirzepatide for Obesity Treatment and Diabetes Prevention. N Engl J Med. 2025;392(10):958–971. doi:10.1056/NEJMoa2410819
12. Gentilella R, Pechtner V, Corcos A, Consoli A. Glucagon-like peptide-1 receptor agonists in type 2 diabetes treatment: are they all the same? Diabetes/Metab Res Rev. 2019;35(1):e3070. doi:10.1002/dmrr.3070
13. Fineman MS, Cirincione BB, Maggs D, Diamant M. GLP-1 based therapies: differential effects on fasting and postprandial glucose. Diabetes Obesity Metab. 2012;14(8):675–688. doi:10.1111/j.1463-1326.2012.01560.x
14. Polonsky WH, Arora R, Faurby M, Fernandes J, Liebl A. Higher Rates of Persistence and Adherence in Patients with Type 2 Diabetes Initiating Once-Weekly vs Daily Injectable Glucagon-Like Peptide-1 Receptor Agonists in US Clinical Practice (STAY Study). Diabetes Therapy. 2022;13(1):175–187. doi:10.1007/s13300-021-01189-6
15. Harris KB, McCarty DJ. Efficacy and tolerability of glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes mellitus. Therapeutic Adv Endocrinol Metabol. 2015;6(1):3–18. doi:10.1177/2042018814558242
16. Kalayci A, Januzzi JL, Mitsunami M, Tanboga IH, Karabay CY, Gibson CM. Clinical features modifying the cardiovascular benefits of GLP-1 receptor agonists: a systematic review and meta-analysis. Eur Heart J Cardiovasc Pharmacother. 2025;11(6):552–561. doi:10.1093/ehjcvp/pvaf037
17. Handelsman Y. Diabetes, cardiorenal, and metabolic multispecialty practice recommendations and early intensive management of cardio-renal-metabolic disease. Am J Manag Care. 2024;30(10 Suppl):S189–S196. doi:10.37765/ajmc.2024.89671
18. Jiao R, Lin C, Bai S, et al. The correlations between steady-state concentration, duration of action and molecular weight of GLP-1RAs and their efficacy and gastrointestinal side effects in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. Expert Opinion Pharmacother. 2023;24(4):511–521. doi:10.1080/14656566.2023.2181693
19. Rabbani SAT, El-Tanani M, Matalka II, et al. Tirzepatide: unveiling a new Dawn in dual-targeted diabetes and obesity management. Expert Rev Endocrinol Metabol. 2024;19(6):487–505. doi:10.1080/17446651.2024.2395540
20. Son JW, le Roux CW, Blüher M, Nauck MA, Lim S. Novel GLP-1-Based Medications for Type 2 Diabetes and Obesity. Endocrine. 2025;Reviews:bnaf036. doi:10.1210/endrev/bnaf036
21. Salamah HM, Marey A, Elsayed E, et al. Efficacy and safety of polyethylene glycol loxenatide in type 2 diabetic patients: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. 2023;13(1):19041. doi:10.1038/s41598-023-46274-x
22. Kang YM, Punov V, Lim S, Nauck MA. Comparative efficacy and tolerability of currently approved incretin mimetics: a systematic analysis of placebo-controlled clinical trials. Diabetes Obesity Metab. 2025;27(7):3736–3746. doi:10.1111/dom.16398
23. Utta D, Chatterjee S, Datta PK, Mohindra R, Sharma M. Role of novel glucagon-like peptide-1 receptor analogue polyethylene glycol loxenatide in type 2 diabetes: a systematic review and meta-analysis. Indian J Endocrinol Metab. 2023;27(5):377–386. doi:10.4103/ijem.ijem_162_23
24. Ji L, Jiang H, An P, et al. Mazdutide (IBI362), a weekly-dose GLP-1 and glucagon receptor dual agonist, in Chinese adults with overweight or obesity: a randomised, placebo-controlled, multiple ascending dose phase 1b study. EClinicalMedicine. 2021;39:101088. doi:10.1016/j.eclinm.2021.101088
25. Li Z, Duan R, Shi L, et al. Guideline for the workflow of clinical comprehensive evaluation of drugs. China Pharm. 2025;36(19):2353–2365. doi:10.6039/j.issn.1001-0408.2025.19.01
26. Zhao Z, Dong Z, Liu J. A quick guideline for drug evaluation and selection in Chinese medical institutions (the 2nd ed). Herald Med. 2023;42(4):447–456. doi:10.3870/j.issn.1004-0781.2023.04.001
27. Zhang C, Ma EL, Liu BL, Wu B, Gu ZC, Lin HW. Framework Development for Clinical Comprehensive Evaluation of Drugs-a Study Protocol Using the Delphi Method and Analytic Hierarchy Process. Front Pharmacol. 2022;13:869319. doi:10.3389/fphar.2022.869319
28. Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS One. 2011;6(6):e20476. doi:10.1371/journal.pone.0020476
29. Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: a Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023;148(9):e9–e119. doi:10.1161/CIR.0000000000001168
30. ESC Scientific Document Group, Marx N, Federici M, Schütt K, et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023;44(39):4043–4140. doi:10.1093/eurheartj/ehad192
31. National Clinical Practice Guideline on Obesity Management Editorial Committee, Zhang Z, Ji L. National Clinical Practice Guideline on Obesity Management (2024 Edition). Chinese Circulation J. 2025;40(1):6–30. doi:10.3969/j.issn.1000-3614.2025.01.002
32. Xie Y, Kuang J, Li Q, et al. Impact of polyethylene glycol loxenatide on cardiovascular outcomes in patients with type 2 diabetes: study protocol for a multicentre, randomised, double-blind, placebo-controlled trial (BALANCE-3). BMJ Open. 2023;13(5):e069080. doi:10.1136/bmjopen-2022-069080
33. Luo Y, Jiang H, Shi B, et al. Mazdutide versus Semaglutide for the treatment of type 2 diabetes and obesity: rationale, design and baseline data of DREAMS-3 Phase 3 trial. Contemporary Clinical Trials. 2025;108150. doi:10.1016/j.cct.2025.108150.
34. Sorli C, Harashima SI, Tsoukas GM, et al. Efficacy and safety of once-weekly semaglutide monotherapy versus placebo in patients with type 2 diabetes (SUSTAIN 1): a double-blind, randomised, placebo-controlled, parallel-group, multinational, multicentre phase 3a trial. Lancet Diabetes Endocrinol. 2017;5(4):251–260. doi:10.1016/S2213-8587(17)30013-X
35. Ahrén B, Masmiquel L, Kumar H, et al. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as an add-on to metformin, thiazolidinediones, or both, in patients with type 2 diabetes (SUSTAIN 2): a 56-week, double-blind, phase 3a, randomised trial. Lancet Diabetes Endocrinol. 2017;5(5):341–354. doi:10.1016/S2213-8587(17)30092-X
36. Ji L, Dong X, Liu M, et al. Efficacy and safety of once-weekly semaglutide versus once-daily sitagliptin as add-on to metformin in patients with type 2 diabetes in SUSTAIN China: a 30-week, double-blind, phase 3a, randomized trial. Diabetes Obesity Metab. 2021;23(2):404–414. doi:10.1111/dom.14232
37. Pratley RE, Aroda VR, Lingvay I, et al. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018;6(4):275–286. doi:10.1016/S2213-8587(18)30024-X
38. Wysham C, Blevins T, Arakaki R, et al. Efficacy and safety of dulaglutide added onto pioglitazone and metformin versus exenatide in type 2 diabetes in a randomized controlled trial (AWARD-1). Diabetes Care. 2014;37(8):2159–2167. doi:10.2337/dc13-2760
39. Umpierrez G, Tofé Povedano S, Pérez Manghi F, Shurzinske L, Pechtner V. Efficacy and safety of dulaglutide monotherapy versus metformin in type 2 diabetes in a randomized controlled trial (AWARD-3). Diabetes Care. 2014;37(8):2168–2176. doi:10.2337/dc13-2759
40. Nauck M, Weinstock RS, Umpierrez GE, Guerci B, Skrivanek Z, Milicevic Z. Efficacy and safety of dulaglutide versus sitagliptin after 52 weeks in type 2 diabetes in a randomized controlled trial (AWARD-5). Diabetes Care. 2014;37(8):2149–2158. doi:10.2337/dc13-2761
41. The AWARD-11 Investigators, Frias JP, Bonora E, Nevarez Ruiz L, et al. Efficacy and Safety of Dulaglutide 3.0 mg and 4.5 mg Versus Dulaglutide 1.5 mg in Metformin-Treated Patients With Type 2 Diabetes in a Randomized Controlled Trial (AWARD-11). Diabetes Care. 2021;44(3):765–773. doi:10.2337/dc20-1473
42. Fadini GP. Can Dual Incretin Receptor Agonists Exert Better Cardiovascular Protection than Selective GLP-1 Receptor Agonists? Highlights from SURPASS-CVOT. Diabetes Therapy. 2025;16(10):1893–1898. doi:10.1007/s13300-025-01784-x
43. Zhang B, Cheng Z, Chen J, et al. Efficacy and Safety of Mazdutide in Chinese Patients With Type 2 Diabetes: a Randomized, Double-Blind, Placebo-Controlled Phase 2 Trial. Diabetes Care. 2024;47(1):160–168. doi:10.2337/dc23-1287
44. Shuai Y, Yang G, Zhang Q, et al. Efficacy and safety of polyethylene glycol loxenatide monotherapy in type 2 diabetes patients: a multicentre, randomized, double-blind, placebo-controlled phase 3a clinical trial. Diabetes Obesity Metab. 2021;23(1):116–124. doi:10.1111/dom.14198
45. REWIND Investigators, Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019;394(10193):121–130. doi:10.1016/S0140-6736(19)31149-3
46. Li J, Tian Y, Li L, et al. Once-weekly glucagon-like peptide receptor agonist polyethylene glycol loxenatide protects against major adverse cardiovascular events in patients with type 2 diabetes: a multicenter ambispective cohort study (FLYING trial). MedComm. 2025;6(2):e70094. doi:10.1002/mco2.70094
47. Rosenstock J, Wysham C, Frías JP, et al. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): a double-blind, randomised, phase 3 trial. Lancet. 2021;398(10295):143–155. doi:10.1016/S0140-6736(21)01324-6
48. The SURPASS-2 Investigators, Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med. 2021;385(6):503–515. doi:10.1056/NEJMoa2107519
49. Ludvik B, Giorgino F, Jódar E, et al. Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3): a randomised, open-label, parallel-group, phase 3 trial. Lancet. 2021;398(10300):583–598. doi:10.1016/S0140-6736(21)01443-4
50. The SURPASS-4 Investigators, Del Prato S, Kahn SE, Pavo I, et al. Tirzepatide versus insulin glargine in type 2 diabetes and increased cardiovascular risk (SURPASS-4): a randomised, open-label, parallel-group, multicentre, phase 3 trial. Lancet. 2021;398(10313):1811–1824. doi:10.1016/S0140-6736(21)02188-7
51. The SURMOUNT-4 Investigators, Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205–216. doi:10.1056/NEJMoa2206038
52. The SURMOUNT-2 Investigators, Garvey WT, Frias JP, Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2023;402(10402):613–626. doi:10.1016/S0140-6736(23)01200-X
53. Wadden TA, Chao AM, Machineni S, et al. Tirzepatide after intensive lifestyle intervention in adults with overweight or obesity: the SURMOUNT-3 phase 3 trial. Nat Med. 2023;29(11):2909–2918. doi:10.1038/s41591-023-02597-w
54. The SURMOUNT-4 Investigators, Aronne LJ, Sattar N, Horn DB, et al. Continued Treatment With Tirzepatide for Maintenance of Weight Reduction in Adults With Obesity: the SURMOUNT-4 Randomized Clinical Trial. JAMA. 2024;331(1):38–48. doi:10.1001/jama.2023.24945
55. The SURMOUNT-OSA Investigators, Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity. N Engl J Med. 2024;391(13):1193–1205. doi:10.1056/NEJMoa240488
56. Yao H, Zhang A, Li D, et al. Comparative effectiveness of GLP-1 receptor agonists on glycaemic control, body weight, and lipid profile for type 2 diabetes: systematic review and network meta-analysis. BMJ. 2024;384:e076410. doi:10.1136/bmj-2023-076410
57. Xie Z, Hu J, Gu H, Li M, Chen J. Comparison of the efficacy and safety of 10 glucagon-like peptide-1 receptor agonists as add-on to metformin in patients with type 2 diabetes: a systematic review. Front Endocrinol. 2023;14:1244432. doi:10.3389/fendo.2023.1244432
58. Xie Z, Zheng G, Liang Z, Li M, Deng W, Cao W. Seven glucagon-like peptide-1 receptor agonists and polyagonists for weight loss in patients with obesity or overweight: an updated systematic review and network meta-analysis of randomized controlled trials. Metabolism. 2024;161:156038. doi:10.1016/j.metabol.2024.156038
59. Hu Y, Zou H, Shen Y, et al. Long- and Short-Term Cost-Effectiveness of Once-Weekly Semaglutide versus Dulaglutide for the Treatment of Type 2 Diabetes in China: a Hypothetical Modeling Exercise. Diabetes Therapy. 2025;16(5):915–929. doi:10.1007/s13300-025-01716-9
60. Liu L, Ruan Z, Ung COL, et al. Long-Term Cost-Effectiveness of Subcutaneous Once-Weekly Semaglutide Versus Polyethylene Glycol Loxenatide for Treatment of Type 2 Diabetes Mellitus in China. Diabetes Therapy. 2023;14(1):93–107. doi:10.1007/s13300-022-01336-7
61. Xie Z, Li J, Yang S, Deng W, Chen J. A health technology assessment based on Chinese guidelines: glucagon-like peptide-1 receptor agonist in the treatment of type 2 diabetes complicated with cardiovascular disease. Therapeut Clin Risk Manage. 2022;18:889–900. doi:10.2147/TCRM.S375067
62. Xie Z, Hu J, Li M, Hu X, Chen J. Health technology assessment: evaluation of 7 glucagon-like peptide-1 receptor agonists for the treatment of type 2 diabetes mellitus. Risk Management Healthcare Policy. 2024;17:1053–1067. doi:10.2147/RMHP.S455897
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessing Clinical Inertia on Implementing Clinical Guideline Recommendations in Patients with Type 2 Diabetes: A Clinician Survey Study
Stephenson JJ, Witkowski N, Smith JL, Wong AC, Bengtson LG, Willey VJ
Diabetes, Metabolic Syndrome and Obesity 2026, 19:573007
Published Date: 23 March 2026