")
Back to Journals » Research and Reports in Urology » Volume 15
A Chance Finding of High Grade Prostate Cancer in a 35-Year-Old Male – A Case Report and Outcomes of Robotic Radical Prostatectomy in Young Men with Prostate Cancer
Authors Virk A , Treacy PJ, Zhong W, Doeuk N, Doeuk C, Leslie S
Received 17 October 2023
Accepted for publication 12 December 2023
Published 20 December 2023 Volume 2023:15 Pages 571—576
DOI https://doi.org/10.2147/RRU.S445173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Amandeep Virk,1 Patrick-Julien Treacy,2 Wenjie Zhong,3,4 Norbert Doeuk,1 Celine Doeuk,5 Scott Leslie1– 3
1Department of Uro-Oncology, Chris O’Brien Lifehouse, Camperdown, NSW, Australia; 2The Institute of Academic Surgery at Royal Prince Alfred Hospital, Camperdown, NSW, Australia; 3Faculty of Medicine and Health, The University of Sydney, Camperdown, NSW, Australia; 4Faculty of Medicine and Health, The University of New South Wales, Kensington, NSW, Australia; 5Rozelle Medical Centre, Ultimo, NSW, Australia
Correspondence: Amandeep Virk, Chris O’Brien Lifehouse, 119-143 Missenden Road, Camperdown, Sydney, NSW, 2050, Australia, Tel +61421233369, Email [email protected]
Background: Prostate cancer is often considered a disease of older men and this indeed fits with its peak incidence between 65– 79 years of age. Reports of prostate cancer in men younger than 40 years of age and the outcomes of this age group following treatment are few in the literature. Here, we present the case of an unusual diagnosis of high grade prostate cancer in a very young man and outline early outcomes following treatment with robotic-assisted radical prostatectomy.
Case Presentation: A 35-year-old male, intermittently taking finasteride for hair loss, was found to have an elevated prostate-specific antigen (PSA) of 12.5ng/mL leading to an incidental diagnosis of high grade prostate cancer. Targeted trans-perineal prostate biopsy found Gleason 4+5=9 acinar adenocarcinoma, without cribriform architecture but with features suspicious for extracapsular extension. Robotic radical prostatectomy with bilateral pelvic lymph node dissection was performed and found Gleason 4+5=9 adenocarcinoma with focal cribriform architecture, extra prostatic extension and clear margins, stage pT3a N0 M0. PSA was undetectable at 12 months, continence was immediate, and the patient reported strong erections soon after surgery. Family history of prostate cancer and genetic testing were both negative.
Conclusion: This case highlights that not all clinically significant cancers will be identified by following PSA screening guidelines starting at 50 years of age (or 40 years of age for men with a family history of prostate cancer). While high grade prostate cancer in a man less than 40 years of age is uncommon, the literature suggests the incidence is increasing. Our case alongside series in the literature indicate that these men have better functional outcomes and equal oncological outcomes with early surgical intervention for localized disease when compared to the older population.
Keywords: prostate cancer, prostatectomy, robotic surgery, young men, outcomes, case report
Introduction
The functional and pathological outcomes of very young men with prostate cancer are infrequently reported in the literature. The varying definition of “young” makes comparison of existing reports more difficult. The low incidence in young men and no routine screening in the younger age groups may explain the scant reports. The Australian Institute of Health and Welfare reported that no men were diagnosed between the ages of 15–34 and only 2 men were diagnosed between the ages of 35–39 across the 12 months of 2018 nationwide.1 The peak incidence of prostate cancer in Australia is between 65–79 years of age, with the outcomes of younger populations less well studied.1 Here we report an incidentally diagnosed case of high grade prostate cancer in a 35-year-old male, detailing the pathological and early functional outcomes post robotic-assisted radical prostatectomy.
Case Presentation
A 35-year-old male presented to their GP for treatment of hot flushes on finasteride (5-alpha reductase inhibitor) for hair loss, which he had recently stopped. The finasteride was stopped because of these side effects and a subsequent baseline prostate-specific antigen (PSA) showed a raised reading of 12.5ng/mL, which prompted referral to a urologist.
Negative urine culture excluded urinary tract infection, and repeat PSA 6 weeks later demonstrated a rise to 14.6ng/mL. Digital rectal exam revealed a small, benign-feeling prostate which was non-tender. There was no family history of prostate cancer, and the patient did not have any physical or sexual activity prior to the PSA tests.
Multiparametric MRI found a PIRADS 4 lesion in the anterior zone of the prostate (see Figure 1). PSMA PET identified focal and markedly increased tracer uptake in the anterior zone of the prostate concordant with the MRI lesion (see Figure 2). The SUVmax on the PSMA PET scan was 23.5, consistent with a site of active tumor. There was no evidence of lymphadenopathy or metastatic disease. Targeted trans-perineal prostate biopsies found Gleason 4+5=9 (Grade Group 5) acinar adenocarcinoma in 8 of 8 biopsy cores involving 80% of the total material sampled. No cribriform architecture was identified but there were features suspicious of extra prostatic extension on the biopsy. Sperm banking was completed and a robotic-assisted radical prostatectomy was performed with a novel RoboSling vascularized continence sling, an aggressive bilateral nerve spare and a bilateral pelvic lymph node dissection, without complication.2 Pathology demonstrated Gleason 4+5=9 adenocarcinoma with focal cribriform architecture, 0.6mm of extracapsular extension at the apex anteriorly, and clear margins, stage pT3a N0 M0 (see Figure 3).
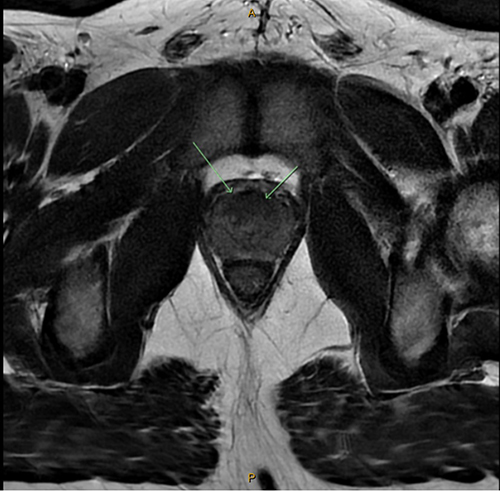 |
Figure 1 MRI image of the prostate lesion on axial T2-weighted imaging (green arrows indicate the lesion). |
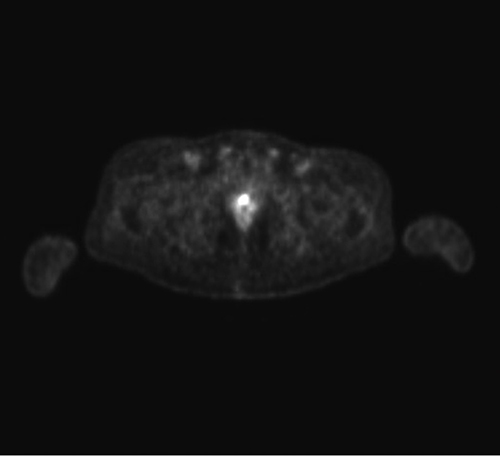 |
Figure 2 PSMA PET image of the prostate lesion. |
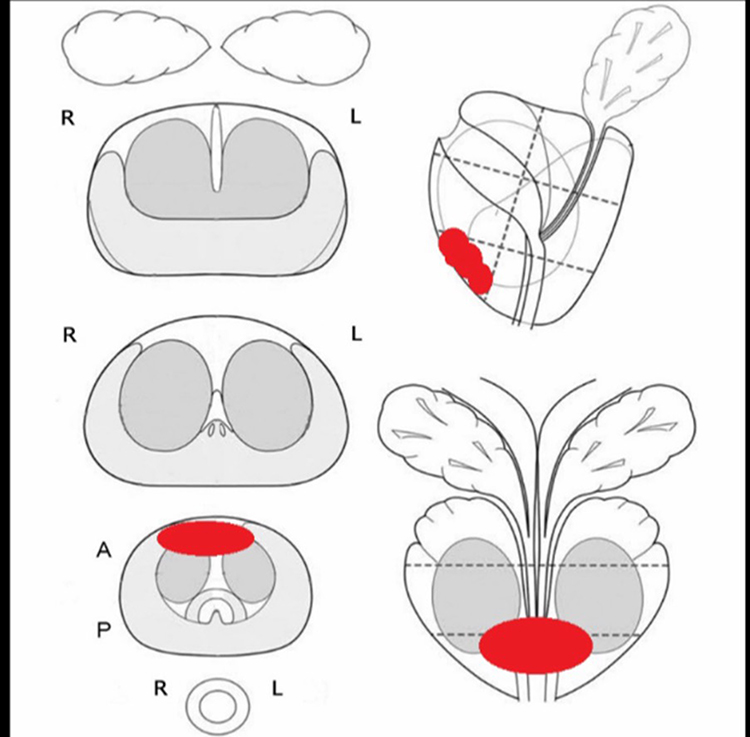 |
Figure 3 Schematic of the prostate lesion (red shading highlights the location of the lesion within the prostate gland). |
At 12-month follow-up, the patient had an undetectable PSA, complete continence with 0 daily pad use, and reported erections rigid enough for penetration with acupuncture and daily Tadalafil (phosphodiesterase-5 inhibitor) for penile rehabilitation. The patient’s father has since been diagnosed with Gleason 6 prostate cancer at the age of 67, screening having been prompted by the patient’s diagnosis. On further history from relatives, his maternal grandmother had a history of breast cancer at age 89. Genetic testing, including BRCA1, BRCA2, PALB2 and TP53, was performed in the context of the high grade disease at a young age and did not identify a heritable cause. Please see Figure 4 for a treatment timeline schematic.
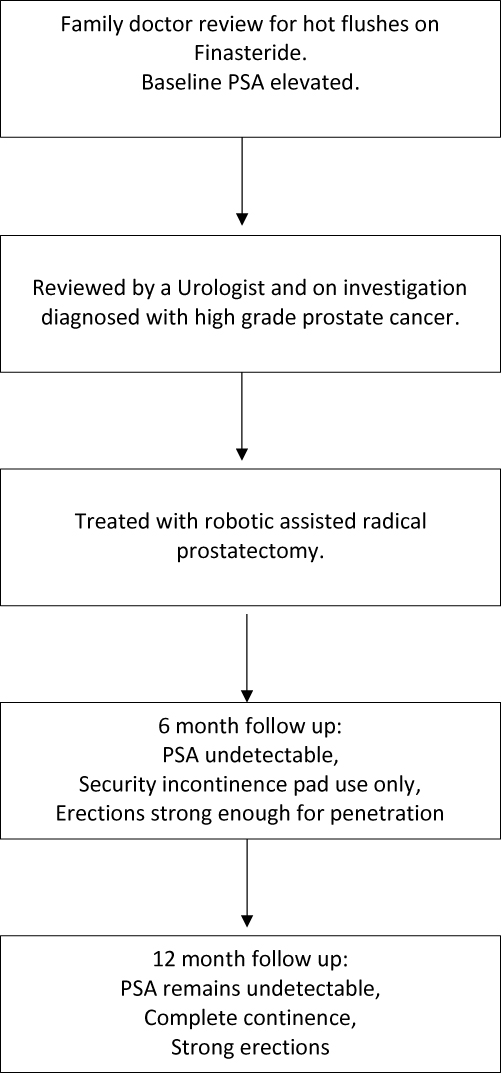 |
Figure 4 Treatment timeline. |
Discussion
This case report highlights one of the youngest diagnoses of prostate cancer managed with robotic-assisted radical prostatectomy described in the literature so far. Our patient had a history of 5-alpha reductase inhibitor (5-ARI) use for 12 months and was diagnosed with a high grade prostate cancer at a young age. The use of a 5-ARI for 3–6 months has been associated with a 50% reduction in PSA levels.3 In this context, any PSA levels checked after commencement of a 5-ARI should be adjusted on interpretation and perhaps all men prescribed a 5-ARI should have a PSA checked prior to commencing treatment. Clinical trials on finasteride and dutasteride (5-ARI medications) demonstrated a reduced risk of developing low grade prostate cancer but a small increase in the risk of developing high grade disease.4 More recently, a large population-based cohort study in Sweden found no increase in the risk of developing a high grade prostate cancer with 5-ARI and found a reduction in prostate cancer mortality with an increasing effect with longer 5-ARI exposure.3
With a lower incidence of prostate cancer in young men compared to older age groups, understandably there are few studies describing their outcomes post robotic-assisted radical prostatectomy (RARP). Bhat et al retrospectively analyzed 2243 men under the age of 55 and 245 men under the age of 45.5 They found men under the age of 45 had lower comorbidity scores, better baseline erectile function but higher rates of positive family history for prostate cancer compared to men aged 51–55.5 Younger men had smaller prostate size and higher rates of favorable, organ-confined disease. Continence rates were similar at 12 months but erectile function at 12 months was superior in the younger men. This is explained by the better pre-operative erectile function scores, with more favorable organ-confined disease allowing for more aggressive nerve sparing to be performed in the younger patient population.5,6 Biochemical recurrence rates were not significantly different for younger men.5,6
The Prostate Cancer Foundation of Australia recommends PSA screening every second year for men aged 50 to 69 and testing from the age of 40 years for men with high-risk family history.7 Protocols establishing a younger screening age would allow for early detection of clinically significant cancer and allow for intervention in the younger population which has better functional outcomes. However, earlier screening would conversely risk increasing the rate of overdiagnosis of prostate cancer per death prevented, and could also result in additional unnecessary procedures and associated patient anxiety.7
A recent review of data from the US National Cancer Institute and Institute for Health Metric and Evaluation by Bleyer et al found an increasing incidence of prostate cancer in men between the ages of 15 and 40 years within the United States and globally.8 The relationship between the increasing incidence of diagnosis and PSA testing remains unclear.8 They found a worse 5-year relative survival and a higher incidence of distant metastases at diagnosis in young men in the United States.8 This may be due to incomplete staging in younger men and late detection as a result of delayed diagnosis.8
This case report and review draws attention to men under the age of 40 who are diagnosed with prostate cancer, despite being below the age cut off for screening. Chance diagnoses of this nature, outside of systematic screening protocols, can be considered as case-finding.9,10 This is where PSA testing is offered to a patient for reasons such as obtaining a baseline level on a 5-ARI or a general practitioner recommendation regarding patient profiling.9,10 We outline the short-term functional and oncological outcomes for such men under the age of 40 when managed with robotic-assisted radical prostatectomy for localized disease. A limitation of reports in the literature is short follow-up duration. Long-term oncological outcomes following robotic radical prostatectomy in this age group are lacking.
Patient Perspective
Our patient felt lucky that this chance diagnosis was made, allowing him to receive early surgical intervention and subsequent peace of mind. He also felt fortunate to be diagnosed in the era of robotic surgery and was thankful for the quick recovery time this afforded him.
Conclusion
The literature suggests that the incidence of prostate cancer in young men is increasing globally. However, the detection of prostate cancer in young men remains uncommon due to current screening strategies. These men, when compared to the older population, have better functional outcomes and equal oncological outcomes following early surgical intervention for localized disease. Early screening protocols could potentially benefit young men with clinically significant disease but, conversely, would result in overdiagnosis and overtreatment at the population level.
Abbreviations
PIRADS score, Prostate Imaging–Reporting and Data System score; PSMA PET, Prostate Specific Membrane Antigen Positron Emission Tomography; SUVmax, maximum Standardized Uptake Value.
Ethics Approval and Consent to Participate
This investigation was performed following the principles of the Declaration of Helsinki. Ethics Committee approval was not required.
Consent for Publication
Written informed consent was obtained from the patient for the use of case details and images for this publication.
Funding
The authors received no funding for the research, authorship or publication of this article.
Disclosure
The authors declare that they have no competing interests.
References
1. Australian Institute of Health and Welfare. Cancer data in Australia. Canberra: Australian Institute of Health and Welfare; 2022. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia.
2. Leslie S, Jackson S, Broe M, et al. Improved early and late continence following robot-assisted radical prostatectomy with concurrent bladder neck fascial sling (RoboSling). BJUI Compass. 2023;4(5):597–604. doi:10.1002/bco2.225
3. Björnebo L, Nordström T, Discacciati A, et al. Association of 5α-reductase inhibitors with prostate cancer mortality. JAMA Oncol. 2022;8(7):1019–1026. doi:10.1001/jamaoncol.2022.1501
4. Chau CH, Figg WD. Revisiting 5α-reductase inhibitors and the risk of prostate cancer. Nat Rev Urol. 2018;15(7):400–401. doi:10.1038/s41585-018-0018-9
5. Bhat KRS, Onol FF, Moschovas MC, et al. Robotic-assisted radical prostatectomy in young adults: age-stratified oncological and functional outcomes. J Robot Surg. 2022;16(5):1057–1066. doi:10.1007/s11701-021-01334-0
6. Samadi DB, Sebrow D, Hobbs AR, et al. Clinicopathological, functional, and immediate oncologic outcome assessment in men aged≤50 years with prostate cancer after robotic prostatectomy. Urol Oncol. 2017;35(1):
7. Prostate Cancer Foundation of Australia and Cancer Council Australia PSA Testing Guidelines Expert Advisory Panel. Clinical practice guidelines PSA testing and early management of test-detected prostate cancer. Sydney: Cancer Council Australia; 2023. Available from: https://wiki.cancer.org.au/australia/Guidelines:PSA_Testing.
8. Bleyer A, Spreafico F, Barr R. Prostate cancer in young men: an emerging young adult and older adolescent challenge. Cancer. 2020;126(1):46–57. doi:10.1002/cncr.32498
9. Department of Health and Aged Care. Population-based screening framework. Canberra: Australian Government Department of Health and Aged Care; 2018. Available from: https://www.health.gov.au/resources/publications/population-based-screening-framework?language=en.
10. Kannan A, Kirkman M, Ruseckaite R, Evans SM. Prostate cancer awareness, case-finding, and early diagnosis: interviews with undiagnosed men in Australia. PLoS One. 2019;14(3):e0211539. doi:10.1371/journal.pone.0211539
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.