")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
A Case Series: Experience of Using 20% Potassium Hydroxide Solution to Treat Adult Sexually Transmitted Molluscum Contagiosum
Authors Achdiat PA , Rowawi R, Fatmasari D , Karisa NA, Dwipangestu G, Avriyanti E , Suwarsa O , Gunawan H
Received 2 July 2020
Accepted for publication 22 August 2020
Published 10 September 2020 Volume 2020:13 Pages 671—676
DOI https://doi.org/10.2147/CCID.S270380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Pati Aji Achdiat, Rasmia Rowawi, Dina Fatmasari, Nadila Ayu Karisa, Gilang Dwipangestu, Erda Avriyanti, Oki Suwarsa, Hendra Gunawan
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Bandung, West Java, Indonesia
Correspondence: Hendra Gunawan
Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java 40161, Indonesia
Tel +62 22 2032426
Email [email protected]
Background: Molluscum contagiosum (MC) is a benign disease of the skin and mucous membrane caused by a poxvirus. To date, there is no standard therapy used for the treatment of MC. Using 10% of potassium hydroxide (KOH) once or twice a day and 20% KOH once a day are often applicable to MC lesions both in children and adults. Nevertheless, the usage of 20% KOH twice a day still has not been reported.
Purpose: This case series aimed to show the efficacy and side effects of once- or twice-daily application of 20% KOH solution for MC lesions due to sexually transmitted infections (STIs) in adults.
Patients and Methods: Three cases of MC on the genital were applied once or twice daily and one case of MC on the face was applied twice daily using 20% KOH solution.
Results: As a result, the application of 20% KOH twice daily showed the improvement of MC lesions on the face on day 7 and MC lesions on the genital on day 20. Meanwhile, once-daily application of 20% KOH showed diminished MC lesions on genital on day 25– 31 after treatment. There were tolerable side effects that occurred in this treatment, such as stinging and burning sensation several minutes after application, erosions, and post-inflammatory hypo- and hyper-pigmentation.
Conclusion: The 20% KOH solution twice daily on MC lesions in adults is effective, practical, and inexpensive.
Keywords: 20% potassium hydroxide solution, efficacy, keratolytic, molluscum contagiosum
Introduction
Molluscum contagiosum (MC) is a disease caused by double-stranded poxvirus or called as molluscum contagiosum virus (MCV), with pathognomonic clinical features of skin-colored, pearly, or pink dome-shaped papules,1 and central umbilication.2,3 In adults, MC is often transmitted by sexual contact.4 Based on some studies, it was known that the increased incidence of MC in adults parallels to an overall increase in sexually transmitted infections (STIs).1 MC is a self-limiting disease,5 but it takes a long time from several months to several years to cure without treatment.2
The indication of MC therapy is to prevent autoinoculation, transmission to others, secondary infections, and aesthetic reasons.4 Several aspects need to be considered in deciding MC therapy, such as physical and psychological resilience to treatment, numerous lesions, patient preference, cost, availability of materials or tools, and easy on the application. Curettage has been often used in the therapy of MC.6 While destructive chemical agents such as trichloroacetic acid (TCA)3 and potassium hydroxide (KOH) have good efficacy, easy, and inexpensive for MC treatment.7
Potassium hydroxide is a compound of alkaline and dissolves keratin.8 Some studies showed that KOH had been used for MC therapy in children with various applications such as 10% once- to twice-daily application or 20% once a day application.9,10 Furthermore, one study of the MC in genital was reported using 10% and 20% KOH twice a week.11 Erythema, severe stinging, and burning sensation are the expected side effects occur with KOH treatment considering its keratolytic effect.9,12
Until recently, there were no case reports using 20% KOH twice a day for MC lesions. This case series aimed to show the efficacy and side effects once or twice daily application of 20% KOH solution for MC lesions due to STIs in adults.
Clinical Cases
This study was conducted in compliance with the Declaration of Helsinki, Good Clinical Practices, and local regulatory requirements. Ethics Committee approval from Dr. Hasan Sadikin Hospital, Bandung, Indonesia (No: LB.02.01/X.6.5/219/2020) was obtained. All patients signed informed consent forms that included consent for publication of all case details and accompanying images.
Case 1
A 24-year-old female presented with erythematous papules without itch and pain around the vulva. The lesions first appeared 3 weeks prior to consultation (PTC) as one erythematous papule on the vulva, then spread to the pubic area. She admitted having promiscuity, and mostly her partners did not use condoms. Physical examination on the pubic and vulva showed erythematous papules with umbilication at the central part (Figure 1). Venereal disease research laboratory (VDRL), Treponema pallidum hemagglutination (TPHA), and human immunodeficiency virus (HIV) tests were nonreactive. The patient was treated with 20% KOH solution applied by the patient once daily before bedtime for 25 days. The patient felt a stinging sensation a short time after the first 5 minutes of the application. The MC lesions gradually subsided from day 17 after treatment, disappeared on day 25, and became post-inflammatory hyperpigmentation on day 51 of observation.
 |
Figure 1 Clinical manifestation of molluscum contagiosum on genital area before and after 20% KOH treatment. All of the MC lesions disappeared and became post-inflammatory hyperpigmentation on day 51 of observation. Abbreviations: KOH, potassium dihydroxide; MC, molluscum contagiosum. |
Case 2
A 56-year-old male presented with multiple skin-colored umbilicated papules on the pubic, penis, and scrotum without itch and pain (Figure 2). The lesion first appeared as one skin-coloured papule on the scrotum for the past 2 years PTC. One and a half years later, the papules increased in number for more than 10 papules. Six months later, papules multiplied and spread over the scrotum, penis, and pubic. There has been a history of promiscuity with nine female prostitutes since 2 years ago and had sexual contact with the prostitute who has the same lesions. Physical examination of the pubic, scrotum, and the shaft of the penis showed some papules with central umbilication. A Tzanck smear with Giemsa staining showed Henderson–Paterson’s bodies (Figure 2). While VDRL, TPHA, and HIV tests were nonreactive. The patient was treated with 20% KOH solution applied by the patient once daily for 4 weeks on the left side of the pubic, penis, and scrotum. The right side of the pubic, penis, and scrotum was treated with 80% TCA once a week, as for comparing the efficacy of MC treatment. The MC lesions on both sides gradually became smaller after 2 weeks of treatment and disappeared on day 31. The patient complained of pain and stinging sensation in 3–5 minutes after 20% KOH being used, and lesions became redness for 4–5 days. With 80% TCA solution, there were side effects such as pain and stinging sensation shortly after being used, which last about 10 seconds. Both treatments using 20% KOH and 80% TCA solutions caused side effects of hypopigmented macules.
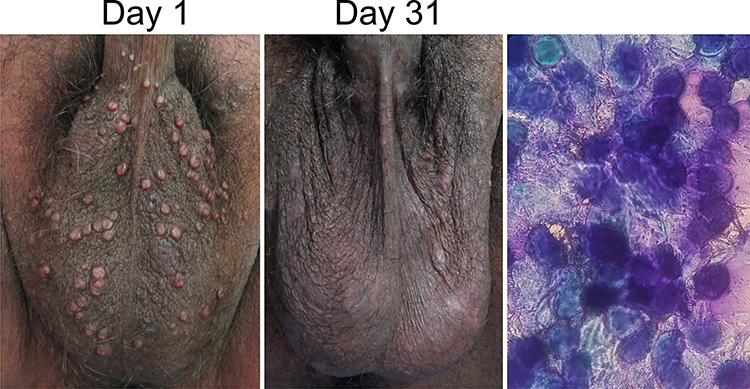 |
Figure 2 Clinical manifestation of molluscum contagiosum on genital area before and after 20% KOH (left side) and 80% TCA (right side) treatment. Basophilic, round, and anucleated masses (Henderson–Paterson bodies) were using Giemsa staining. All of the MC lesions disappeared on day 31 and leaved post-inflammatory hypopigmentation after treatment. Abbreviations: KOH, potassium dihydroxide; TCA, trichloroacetic acid; MC, molluscum contagiosum. |
Case 3
A 28-year-old male presented with multiple skin-colored papules with umbilication on the face, especially forehead and temple area, without itch and pain (Figure 3). The lesions first appeared as skin-colored papules on the forehead for the past one-month PTC. Two weeks later, the number of papules increasing and spread to the temple area. There was a history of promiscuity with female prostitutes. He had no concern of his sexual partners who also have the same lesions. Physical examination on the forehead and the temple area showed many papules with skin-colored and central umbilication. The HIV test was reactive, otherwise VDRL and TPHA tests were nonreactive. The patient was treated with 20% KOH solution applied by the patient twice daily. He complained stinging and burning sensation after 20% KOH applied for 3 minutes. The patient died due to brain toxoplasmosis on day 7 observations, but almost all the lesions became smaller.
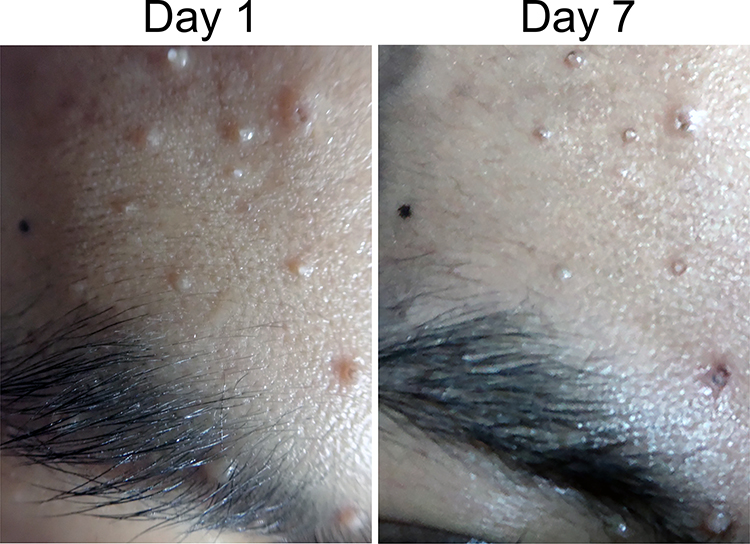 |
Figure 3 Clinical manifestation of molluscum contagiosum on the face before and after 20% KOH treatment. Some of the MC lesions were thinning on day 7. Abbreviations: KOH, potassium dihydroxide; MC, molluscum contagiosum. |
Case 4
A 26-year-old male presented with multiple skin-colored umbilicated papules on the penis, without itch and pain (Figure 4). The lesions first appeared as one skin-colored papule on the penis shaft for the past 1 month PTC. Over time, 3 weeks after, the skin lesions were spread over the base of the penis and increase in number. There was a history of promiscuity with several female prostitutes. Physical examination on the shaft and the base of the penis revealed several papules with central umbilication. VDRL, TPHA, and HIV tests were nonreactive. The patient was treated with 20% KOH solution applied by the patient twice daily for the lesions. All of the MC lesions disappeared on day 20 of observation. The patient felt a stinging sensation after 3–5 minutes application of the 20% KOH solution. Furthermore, it also caused other side effects such as erosions and post-inflammatory hypopigmentation.
 |
Figure 4 Clinical manifestation of molluscum contagiosum on the genital area before and after 20% KOH treatment. All of the MC lesions disappeared on day 20 after 20% KOH application and leaved erosion and post-inflammatory hypopigmentation. Abbreviations: KOH, potassium dihydroxide; MC, molluscum contagiosum. |
Discussion
Molluscum contagiosum is a viral infection caused by MCV, which is the species of the Molluscipox virus genus in the family Poxviridae.3,13 MCV infection occurs worldwide with a prevalence of 5–11%,4 and the incidence has increased significantly in the last few decades.1 The incubation period of this virus ranging from 1 week to 6 months,2 with a mean time of 2–3 months. Transmission of MC can occur directly through the skin to skin contact with sexual or non-sexual routes.4 MC often presents with pearly or pink dome-shaped papules1 with a central umbilication containing a white mass called a molluscum body.2,3 The number of papules is usually less than 20 papules, but some may have over 100 papules.3 Patients with HIV infection have prevalence rates ranging from 1.7% to 4.0% and increased infection rates. The majority of MC lesions in HIV patient occurs on the face and neck area, while the anogenital infection is uncommon.13
The diagnosis of MC is based on the characteristic of skin lesions.13 Other examinations such as histopathological and cytological examinations are only for confirmation when atypical lesions appear.13,14 Tzanck smear examination with Giemsa staining1 shows the molluscum bodies (Henderson–Paterson bodies) in the form of basophilic, round, and anucleated masses.4
Molluscum contagiosum managements are physical therapy, chemical agents, immunomodulators, and antiviral.6 Some of the physical therapies are cryotherapy, curettage, tape stripping, and laser carbon dioxide (CO2).3,6 The destructive chemical agents such as TCA, cantharidin, benzoyl peroxide,3 salicylic acid, tretinoin, podophyllotoxins, podophyllin, and KOH can be used for treating MC.6
The KOH solution is a strong base with keratolytic effect, lyses proteins and lipids, and penetrates deeply and destroys the skin because it dissolves keratin.9,15 It destroys skin cells around the virus. Therefore, the immune system of the body can recognize the virus. The lesions will be inflamed and disappeared within 1–5 weeks.14 The KOH solution can be used with a one-time to two-times frequency per day using cotton swabs until the lesions are inflamed, or superficial ulceration was formed, and the molluscum bodies break out from the papule.3 Some of the advantages of KOH solution for MC therapy are effective, readily available, practical because they can be used by patients, minimal side effects, and inexpensive.9,15 Based on some studies using 20% KOH toward 24 MC lesions in children, all of the MC lesions were disappearing with an average time of 17 days, and there were side effects such as pain and stinging sensation for about 1–2 minutes after being used. The inflammation may occur on the lesions in 5–7 days and leave the hypopigmented macules.9 KOH had been used for MC therapy for children that varies from 10% once to twice daily application and 20% once a day application.9,10 Nevertheless, the usage of 20% KOH twice a day still has not been reported. Maluki et al2 reported MC treatment using 20% KOH solution with different frequency application. This study consisted of 90 patients divided into three groups. The first group used a 20% KOH solution once daily compared to the second group using a 20% KOH solution once a week on the lesions, and the third group simply pricked the lesion. The effectiveness of each therapy was 94.4%, 86.4%, and 75%, respectively.2 Furthermore, Singla et al11 reported the use of KOH 10% and 20%, twice a week for MC in genital. The 20% KOH was better than 10% KOH in genital MC in females.11 These study results showed that more frequent the application of 20% KOH solution made the healing of the MC lesions faster. In this case series, we demonstrated that the application of 20% KOH solution twice daily showed the improvement of MC lesions on the face on day 7 (Case 3) and MC lesions on the genital on day 20 (Case 4). Meanwhile, once-daily application of 20% KOH showed diminished of MC lesions on genital on day 25 and day 31 after treatment in Case 1 and Case 2, respectively.
Side effects of KOH treatment such as erythema, severe stinging, burning sensation, and erosion are expected to occur, considering its keratolytic effect and could leave post-inflammatory hypo- and hyperpigmentation.9,12 In this case series, all of the patients who received 20% KOH treatment suffered stinging and burning sensation for 3–5 minutes after application. In one case (Case 2), the MC lesions became redness for 4–5 days after application, while in Case 4, the erosions occurred after 20 days application. Additionally, in Case 1, 2, and 4, all the patients had post-inflammatory hypopigmentation and in Case 3, the patient had post-inflammatory hyperpigmentation. Further investigations with a large number of subjects need to be done to see the efficacy and side effects of the 20% KOH applied twice daily.
Conclusion
It may be concluded from this case series that 20% KOH solution applied twice daily are effective for MC treatment in adults with tolerable side effects. Furthermore, this treatment is practical because it can be applied by the patient and inexpensive.
Acknowledgments
The authors would like to thank the staff of Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java Indonesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Piggott C, Friedlander SF, Wynnis T. Poxvirus infection. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffel DJ, Wolff K, editors. Fitzpatrick’s Dermatology in General Medicine.
2. Maluki AH, Kadhum QJ. Treatment of molluscum contagiosum by potassium hydroxide solution 20% with and without pricking and by pricking alone: a comparative study with review of literature. Int J Dermatol Clin Res. 2015;1(2):031–041.
3. Chen X, Anstey AV, Bugert J. Molluscum contagiosum virus infection. Lancet Infect Dis. 2013;13(10):877–888.
4. Tyring SK. Molluscum contagiosum: the importance of early diagnosis and treatment. Am J Obstet Gynecol. 2003;189(3):S12–6.
5. Nguyen HP, Franz E, Stiegel KR, et al. Treatment of molluscum contagiosum in adult, pediatric, and immunodeficient populations. J Cutan Med Surg. 2014;18(5):299–306.
6. Al-Sudany NK, Abdulkareem DR. A comparative study of topical 10% KOH solution and topical 25% podophyllin solution as home-base treatments of molluscum contagiosum. J Dermatol Surg. 2016;20(2):107–114.
7. Audisio TM, Pelliza P, Maria N, et al. Molluscum contagiosum: therapeutic response to trichloroacetic acid in pregnant patients. J Low Genit Tract Dis. 2009;13(4):252–255.
8. Meza-romero R, Navarrete-dechent C, Downey C. Molluscum contagiosum: an update and review of new perspectives in etiology, diagnosis, and treatment. Clin Cosmet Investig Dermatol. 2019;12:373.
9. Mahajan BB, Pall A, Gupta RR. Topical 20% KOH an effective therapeutic modality for molluscum contagiosum in children. Indian J Dermatol Venereol Leprol. 2003;69(2):175–177.
10. Can B, Topaloglu F, Kavala M, et al. Treatment of pediatric molluscum contagiosum with 10% potassium hydroxide solution. J Dermatolog Treat. 2014;25(3):246–248.
11. Singla C, Mahajan BB, Kaur T, et al. Genital molluscum contagiosum in females-therapeutic efficacy and comparative evaluation of topical 10% and 20% potassium hydroxide. Indian J Sex Transm Dis AIDS. 2018;39(2):102.
12. Muzaffar F, Faiz F. Comparison of 5% potassium hydroxide with 10% potassium hydroxide solution in treatment of molluscum contagiosum: a comparative study. J Pak Assoc Dermatol. 2016;24(4):337–341.
13. Douglas JM. Molluscum contagiosum. In: Holmes KK, Sparling PF, Stamm WE, Piot P, Wasserheit JN, Corey L, editors. Sexually Transmitted Diseases.
14. Goyal V, Maheshwari AK, Goyal S, et al. A comparative study of efficacy of 10% KOH, trichloroacetic acid (TCA) and 0.05% tretinoin for the treatment of molluscum contagiosum. Sch J App Med Sci. 2014;2(4A):1196–1198.
15. Qureshi A, Zeb M, Jalal-ud-din M, et al. Comparison of efficacy of 10% potassium hydroxide solution versus cryotherapy in treatment of molluscum contagiosum. J Ayub Med Coll Abbottabad. 2016;28(2):382–385.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.