")
Back to Journals » International Medical Case Reports Journal » Volume 16
A Case Series: Effect of Comorbidities on the Outcomes of Prolotherapy Injection for Frozen Shoulder Patients
Authors Sam N , Yusuf I, Idris I, Adnan E, Haryadi RD , Hamid F, Usman MA , Johan MP, Zainuddin AA
Received 8 February 2023
Accepted for publication 26 April 2023
Published 28 April 2023 Volume 2023:16 Pages 257—263
DOI https://doi.org/10.2147/IMCRJ.S407723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Nuralam Sam,1 Irawan Yusuf,1 Irfan Idris,2 Endy Adnan,3 Ratna Darjanti Haryadi,4 Firdaus Hamid,5 Muhammad Andry Usman,6 Muhammad Phetrus Johan,6 Andi Alfian Zainuddin7
1Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia; 2Department of Physiology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia; 3Rheumatology Division, Department of Internal Medicine, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia; 4Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Airlangga University, Surabaya, Indonesia; 5Department of Microbiology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia; 6Department of Orthopedic, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia; 7Department of Public Health, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Correspondence: Nuralam Sam, Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Hasanuddin University, Perintis Kemerdekaan Street KM.11, Makassar, South Sulawesi, 90245, Indonesia, Email [email protected]
Abstract: Frozen shoulder (FS) is a disease caused by an inflammatory condition that causes severe pain and decreased range of motion by loss of glenohumeral mobility. Frozen Shoulder restricts daily life’s functional aspect, increasing morbidity. Hypertension and diabetes mellitus are risk factors that make an FS poor prognosis during treatment because of the diabetes glycation process and hypertension-enhanced vascularization. Prolotherapy injects an irritant solution into the tendon, joints, ligaments, and joint spaces to release growth factors and collagen deposition, reducing pain, restoring joint stability, and increasing the quality of life. We report 3 cases of patients with confirmed FS. Patient A with no comorbidity, patient B with diabetes mellitus, and patient C with hypertension, with all patient’s chief complaints of shoulder pain and limited ROM, and symptoms affected the general quality of daily life. This patient was provided injection with Prolotherapy treatment combined with physical therapy intervention. Patient A had significantly improved ROM to maximum after 6 weeks with relieved pain and improved shoulder function. Patients B and C showed increased ROM, still tiny, decreased pain, and improved shoulder function. In conclusion, prolotherapy demonstrated a beneficial effect in a patient with FS with comorbidities, although not to the maximum extent in patients without comorbidity.
Keywords: protherapy, frozen shoulder, comorbidity, range of motion, quality of life
Introduction
One in three people will experience shoulder pain at some point in their lifetime because the shoulder is frequently a “primary mover” for daily movement; shoulder diseases severely limit one’s ability to do daily activities.1 Frozen shoulder is a common condition that causes pain and a progressive loss of glenohumeral mobility.2,3 It is characterized by clinical signs of shoulder discomfort with progressively limited active and passive motion in addition to normal radiographic glenohumeral joint imaging caused by an inflammatory condition with the molecular mechanism that causes fibroproliferative tissue fibrosis.4,5 FS is the condition that has been restricted to clinical and functional aspects, such assessments do not allow considering all the implications that the disease can cause to the patient’s life.6 The Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) is a regional questionnaire consisting of 30 questions, rather specific to evaluate the functional capacity of the affected upper limb, also being self-administered.7
Frozen shoulder is subdivided into primary and secondary, primary also called idiopathic, and occurs without any specific trauma. Secondary can be categorized into systemic.8 Comorbidities occur in 85% of patients with FS, and 37.5% have more than three comorbidities.9 Diabetes, hypertension, shoulder injury, stroke, thyroid disease, and neck surgery are some known risk factors for its development.10 Contrary to the current opinion of many medical experts, FS does not resolve spontaneously in a significant portion of individuals, and FS can be quite disabling.11 The most common comorbidity in people with FS is diabetes and hypertension that increase the inflammatory processes leading capsular fibrosis and subsequent contracture.12–14
The development of numerous therapy approaches for FS is now underway.15 Dextrose prolotherapy injection is one of the therapeutic techniques developed and put into practice in FS8 to address the issues with conventional modalities. During treatment sessions, prolotherapy injects tiny volumes of an irritating solution into sore and deteriorated tendon insertions (entheses), joints, ligaments, and nearby joint spaces to encourage the formation of healthy cells and tissues.16,17 The therapeutic principle of prolotherapy initiates a local inflammatory cascade, which releases growth factors and collagen deposition. Induced cytokine’s role in mediating chemo-modulation, which promotes to proliferation and strengthening of new connective tissue, joint stability, and a reduction in pain and dysfunction.16–18 A major goal of prolotherapy in chronic musculoskeletal conditions is stimulating regenerative processes in the joint that restore joint stability by increasing the tensile strength of stabilizing components such as ligaments, tendons, joint capsules, menisci, and labral tissue.16
In this article, we present a report on four patients in which FS was diagnosed along with various comorbidities. This case report aims to describe the functional outcome of the patient treated with prolotherapy combined with physical therapy using Visual Analog Scale (VAS), The Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH), and Range of Motion (ROM) in order to assess the efficacy of prolotherapy in maintaining and improving the quality of life and to reduce morbidity in a patient with comorbid conditions.
Case Description
Patient A
A fifty-eight-year-old female, entrepreneur presented with right shoulder pain during 3 months ago. With a limited range of motion at the initial evaluation and no visible crepitus on movement, the pain had slowly started in the shoulder and spread insidiously to the neck and elbow. Shoulder discomfort while exercising. There is no comorbidity from patient. The diagnosis of frozen shoulder was determined following normal photos of radiographs, mechanism of injury, past medical history and physical therapy examination and evaluation.
Upon palpation, the physical examination determined that the patient had tenderness along the deltoid region and right biceps tendon. His pain was measured based on the VAS, which was 6 out of 10. The patient’s shoulder ROM flexion 90°, extension 45°, abduction 90°, adduction 35°, internal rotation 50°, and external rotation 15° (Table 1). All the shoulder ROM was limited, consistent with the typical presentation of FS.
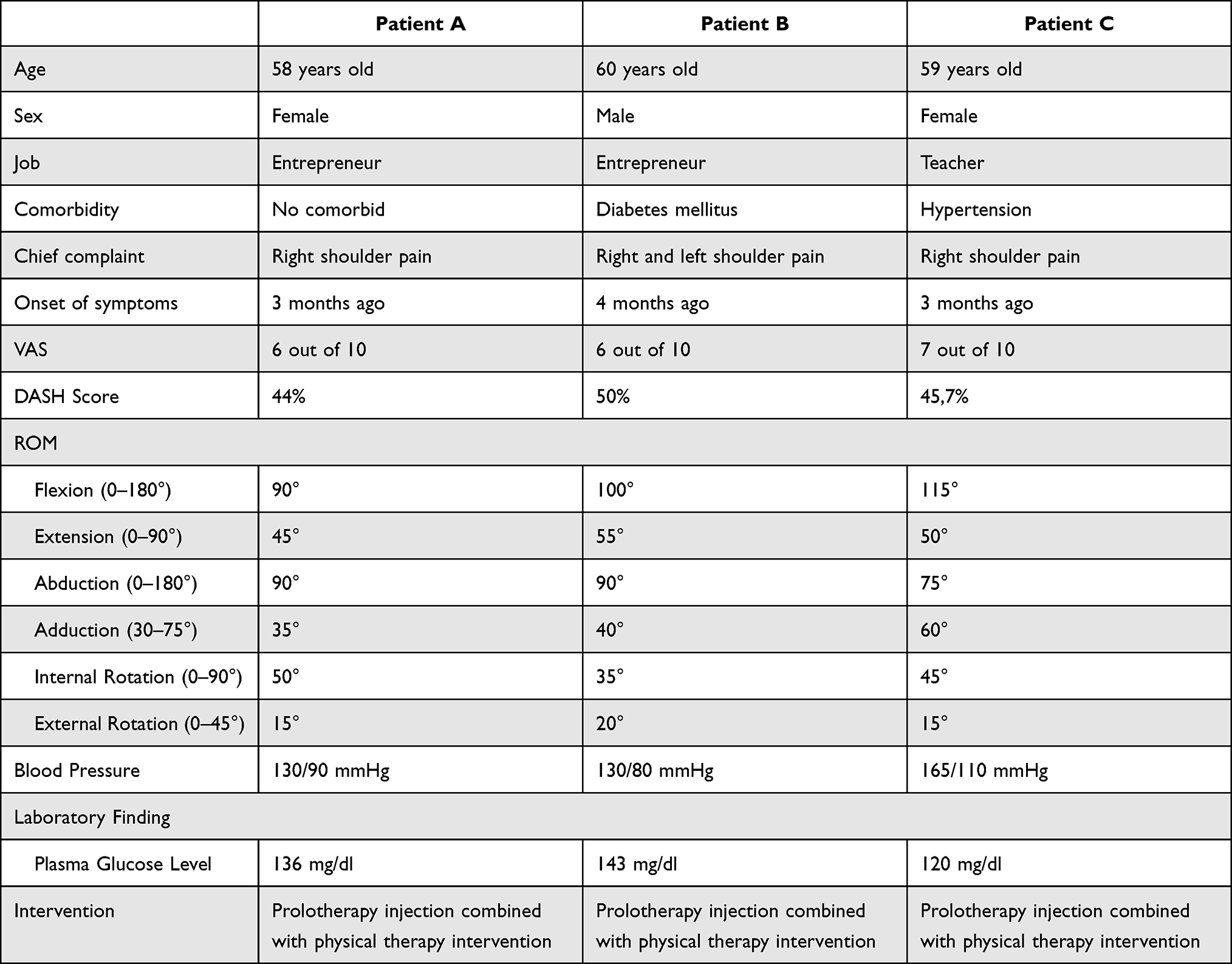 |
Table 1 Data Before Intervention of the Patients |
Patient B
A sixty-one-year-old male, entrepreneur presented with right and left shoulder pain during 4 months ago. The pain had slowly started in the shoulder and spread insidiously to the neck with cramping of the fingertip at the time of the initial evaluation, which showed a limited range of motion and no visible crepitus on movement. The patient complained of difficulty doing everyday tasks and nighttime pain awakening. The patient was previously diagnosed with type II diabetes mellitus (DM). Following the evaluation of normal radiographs, the mechanism of the injury, prior medical history, and physical therapy examination and testing, the diagnosis of a frozen shoulder was made.
Upon palpation, the physical examination determined that the patient had tenderness along the rotator cuff muscle and long head biceps tendons. His pain was measured based on the VAS, which was 6 out of 10. The patient’s shoulder ROM flexion 100°, extension 55°, abduction 90°, adduction 40°, internal rotation 35°, and external rotation 20° (Table 1). The main limitations in ROM included flexion and internal rotation, consistent with the typical presentation of FS. On laboratory findings, the plasma glucose level was 143, and after injection, prolotherapy was 160. The patient regularly takes diabetes medications.
Patient C
Right shoulder pain first appeared in a teacher who was 59 years old 3 months ago. The symptoms of these issues started gradually, but with time, they started to impact his general quality of life. The patient’s range of motion was restricted, and there was no palpable crepitus when the shoulder moved. Her pain increased while working and cooking, interfering with her nighttime sleep. Hypertension was previously identified as the patient’s condition. The diagnosis of a frozen shoulder was made after reviewing normal radiographs, the mechanism of the injury, prior medical history, and physical therapy examination and testing.
According to the physical examination, the patient felt soreness along the biceps tendons, glenohumeral joint, and deltoid region. His VAS score of 7 out of 10 was used to assess his pain level. The patient’s shoulder has a range of motion (ROM) of 115° flexion, 50° extension, 75° abduction, 60° adduction, 45° internal rotation, and 15° external rotation (Table 1). Extension, internal, and external rotation were the main ROM restrictions, consistent with how FS is typically presented. After prolotherapy injections, the tension measure was 165/110 mmHg compared to 150/110 mmHg before intervention. The patient takes hypertension medication regularly.
Treatment and Intervention
All the patients were provided with the same treatment and intervention with a prolotherapy injection containing 15% dextrose, with a disposable syringe of 10 mL containing 4 mL of 15% dextrose, 1 mL of lidocaine, and 5 mL of distilled water. The injection point on the rotator cuff includes the supraspinatus, infraspinatus, teres minor, and subscapularis. Intraarticular injection of the glenohumeral joint, subacromial bursa, long head biceps tendon, and acromioclavicular joint performed by a qualified physician. Injections were administered four times in week 0, week 2, week four, and week 6. Injection combined with a physical intervention consisted of shoulder strengthening exercise, gentle stretching, and ultrasound diathermy with frequency 3 MHZ, duty cycle 50%, pulsed mode, 3W/cm2 for five minutes of the shoulder region. In performing frozen shoulder exercise, stretch to the point of tension but not pain. There are seven stretches and strengthening exercises for building muscle; 1) Swing the arm in a short circle to perform the pendulum stretch, 2) The towel stretch, which involves holding one end of a three-foot towel behind the back and grabbing the other end with the other hand while holding it horizontally, 3) Finger walk by facing a wall from a distance of three-quarters of an arm, 4) Cross-body reach, in which the afflicted arm is raised at the elbow and brought up and across the body using the good arm, 5) Armpit stretch, using the good arm, lift the affected arm onto a shelf about breast high, gently bend your knees, opening up the armpit, the deep knee being slight, 6) Outward rotation, which involves holding a rubber exercise band between hands and rotating the affected arm’s lower portion outward two to three inches while holding the position for five to ten seconds, 7) To perform an inward rotation, stand next to a closed door, wrap one end of a rubber exercise band around the doorknob, hold the other end in the affected arm’s hand while maintaining a 90-degree angle at the elbow, and pull the band two to three inches toward body while holding for five to ten seconds. The patient also provides a home exercise program with muscle stretching and shoulder strengthening by ROM exercise.
Progress notes were completed every two weeks, which consisted of goniometric measurements with the following prime mover muscle of the shoulder joint, shoulder flexion starting position bony landmarks for goniometer alignment by the lateral aspect of the acromion process, lateral midline of thorax, lateral humeral epicondyle, shoulder extension with the lateral aspect of the acromion process, lateral midline of thorax, lateral humeral epicondyle, shoulder abduction with the anterior aspect of the acromion process, midline of sternum, medial humeral epicondyle, shoulder adduction with the anterior aspect of the acromion process, midline of sternum, medial humeral epicondyle, shoulder internal and external rotation with olecranon and styloid processes of the ulna. Reassessment of goals and patient-reported pain. DASH score was given to measure the functional improvements at the initial and final evaluation (Tables 2–4).
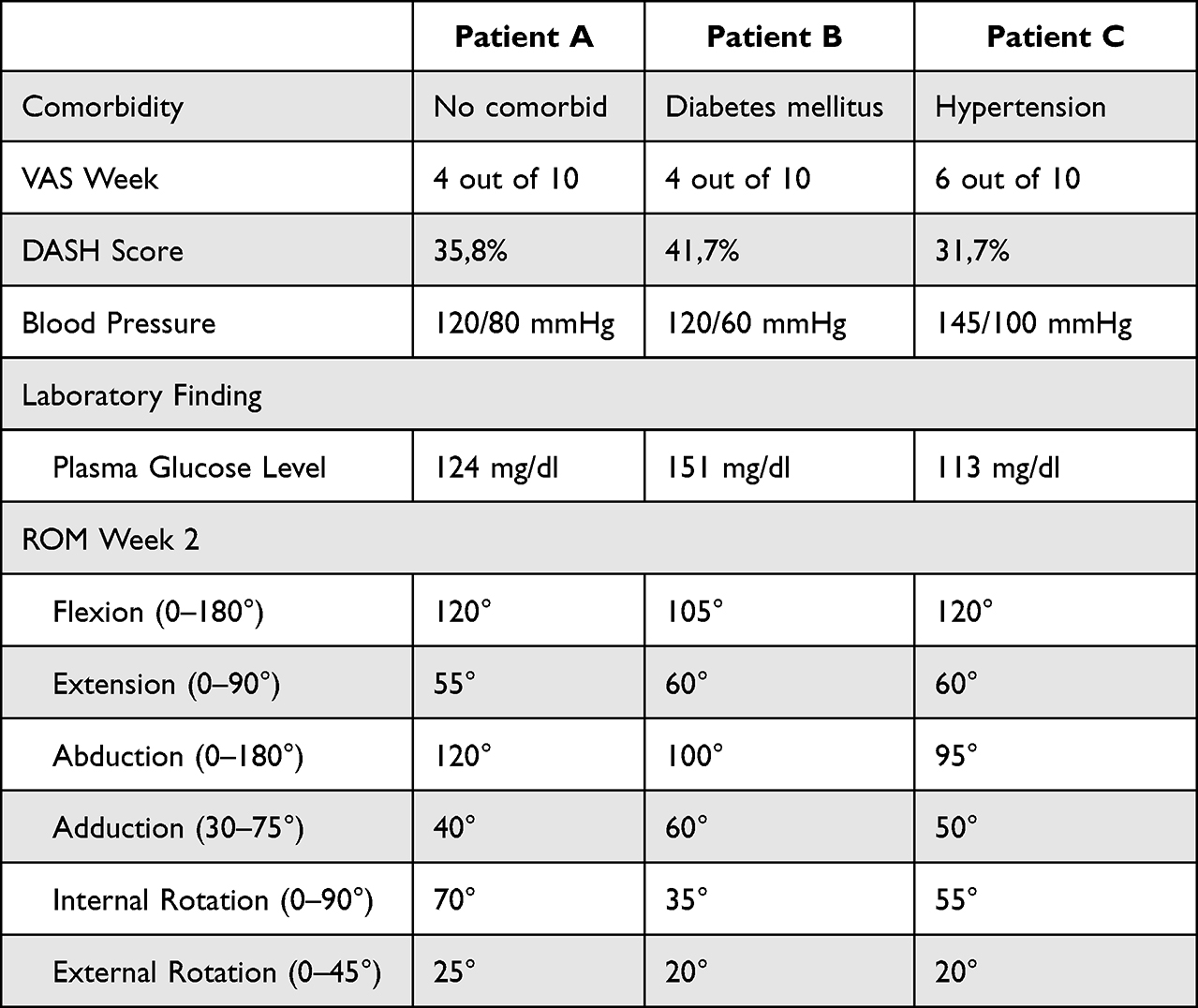 |
Table 2 Data After Intervention of the Patients in Weeks 2 |
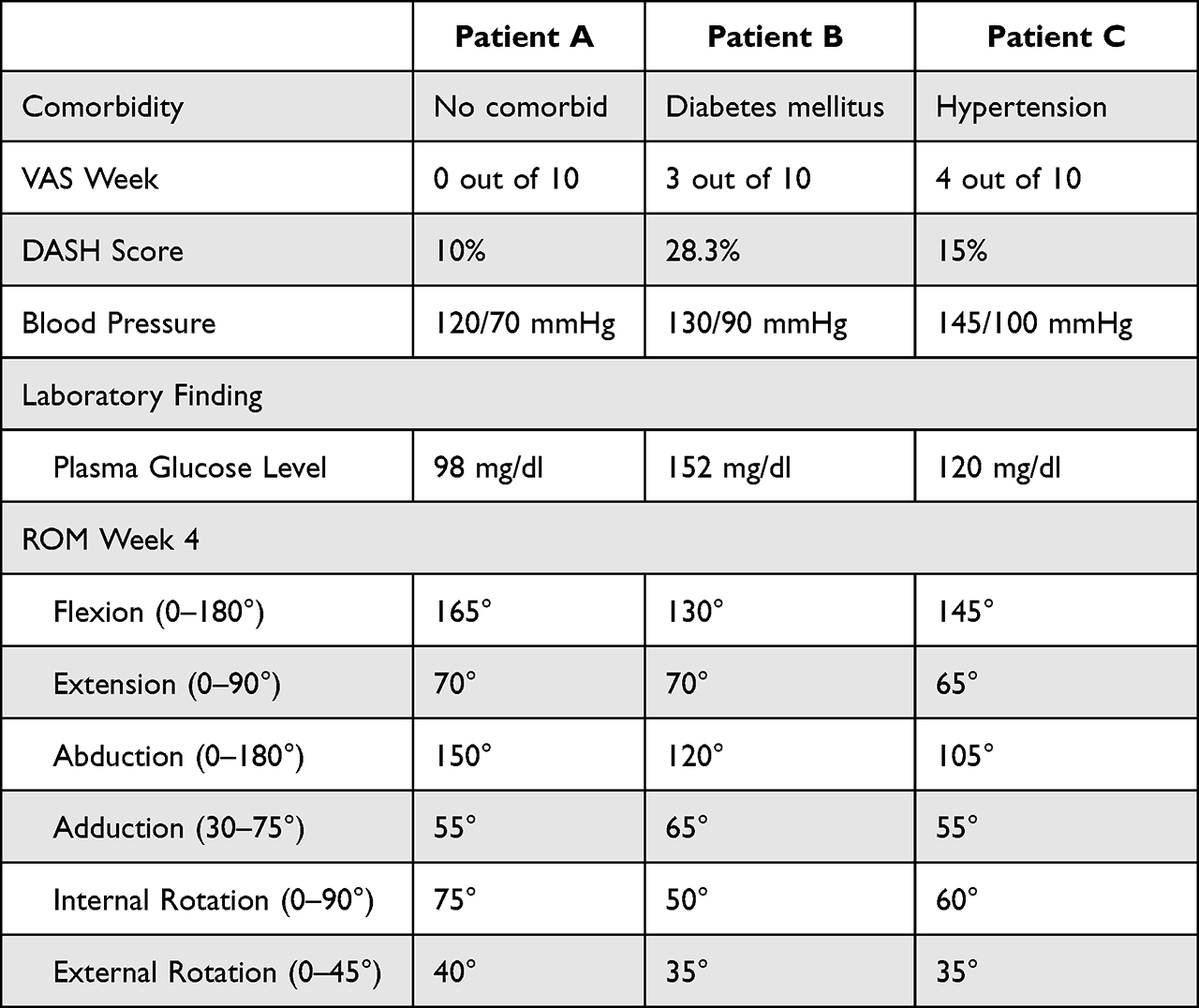 |
Table 3 Data After Intervention of the Patients in Weeks 4 |
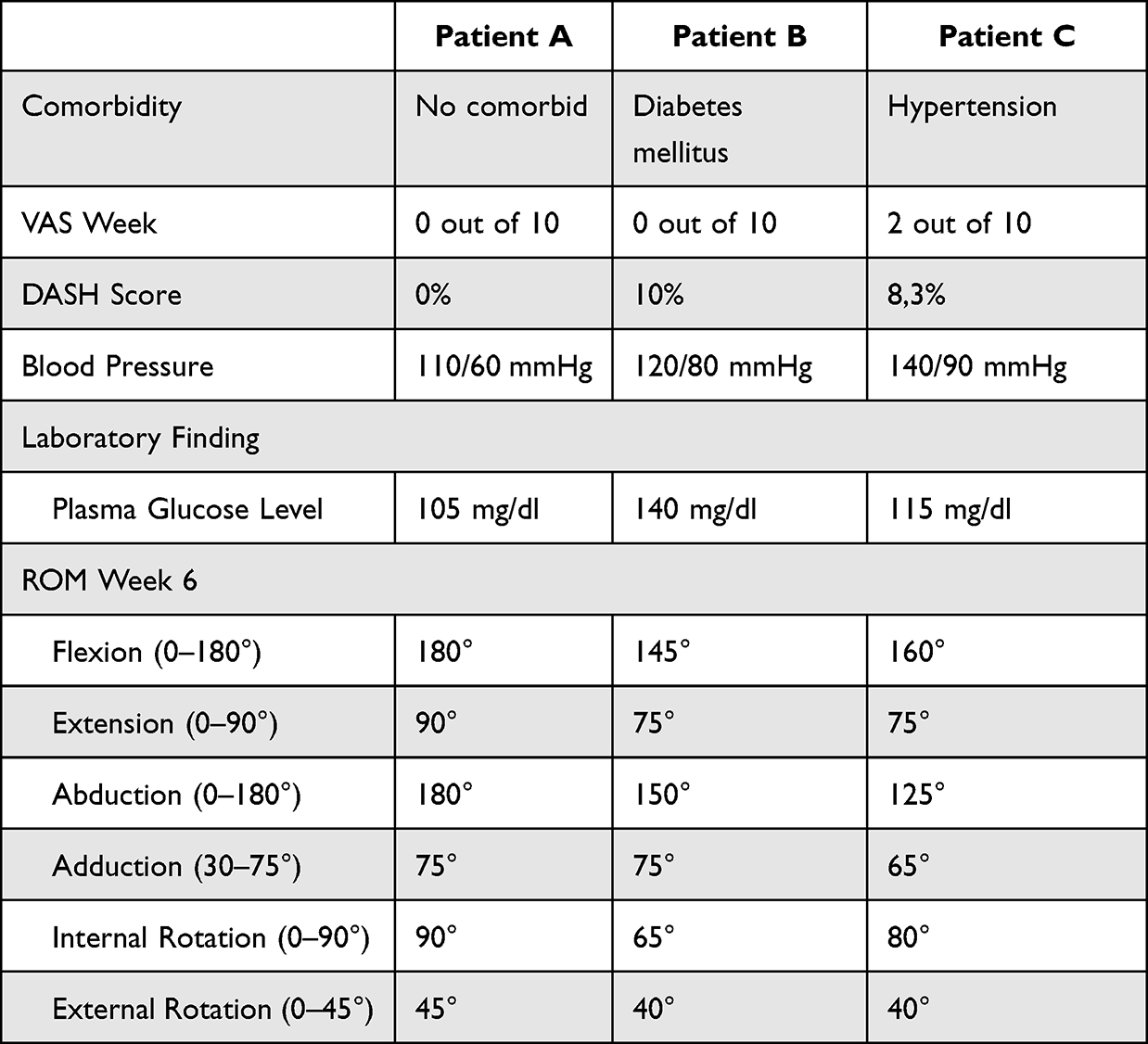 |
Table 4 Data After Intervention of the Patients in Weeks 6 |
Discussion
Both patients were diagnosed with frozen shoulders, as indicated in Table 1, characterized by pain and a limited range of motion, particularly in external rotation.19 FS in generally divided into three stages, freezing (pain and reduced ROM) for 10–36 weeks, frozen (stiffness predominates) for 4–12 months and thawing (symptoms resolve) for 5–24 months or more.20 Both individuals were approaching the point of freezing.
Diabetes mellitus is a disease that typically coexists with FS. Patients with diabetes may get FS at an incidence of 10.8% to 30%, with a tendency toward more severe symptoms and treatment resistance.21 According to a systematic review in 2021, it provides that people with diabetes experience worse outcomes from frozen shoulders than those without diabetes. Diabetes’ prognostic significance in FS was demonstrated by poor ROM outcomes, low pain outcomes, and moderate multidimensional clinical scores.22 Diabetes associated with a frozen shoulder is that glycation processes may cause changes in capsule tissue and consequently lead to the development of a frozen shoulder.21,22 Tables 2–4 show the detailed that patient with diabetes takes a longer time to increase ROM than non-comorbid patient.
A risk factor for developing a frozen shoulder is hypertension.23 Univariate analysis of the Cao, 2022 study revealed a strong connection between hypertension and the start of a frozen shoulder (p = 0.009).24 The mechanism arising from inflammation, with cytokine proliferation leading to an increase in fibroblast proliferation, blood flow increasing in patients with hypertension, and enhanced vascularization, may explain the patient’s pain.25 In our case, patients with hypertension showed more painful than non-comorbid patients.
The presence of comorbidities in the frozen shoulder causes a worsening prognosis in the treatment process. Using prolotherapy in a patient with comorbidities has been shown to reduce pain and increase the quality of life, which is almost the same as in patients without comorbidities. Prolotherapy injections cause local tissue irritation that triggers an immediate inflammatory response, enhances fibroblast proliferation and promotes the production of collagen, which promotes tissue renewal and repair.26 After prolotherapy, Jensen et al27,28 revealed increased inflammatory agents at the injection sites and considerable ligament or cartilage structure growth. High glucose levels activate platelet-derived growth factor (PDGF), which boosts TGF-beta gene expression and triggers DNA synthesis in human mesangial cells. High glucose levels stimulate human mesangial cells to express connective tissue growth factors and other genes.26–28 Our report showed that the patient injected with prolotherapy with comorbid diabetes and hypertension did affect the healing process in the patient.
Conclusion
In a patient with a comorbid frozen shoulder, prolotherapy, and physical therapy exhibited the same potential benefits for improved range of motion, dramatically reduced discomfort, and improved quality of life. A patient with a comorbid frozen shoulder may benefit from prolotherapy, which has effects that last till full recovery. However, it takes longer to complete recovery compared to non-comorbid patients.
Data Sharing Statement
The data used to support the findings of this study will be available from the corresponding author upon reasonable request.
Ethical Review
After receiving permission from Hasanuddin University with protocol number UH219070463 obtained ethics approval.
Consent for Publication
The patients provided written informed consent for the publication of this case series. The consent included case-specific information and any accompanying images.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Ryu K, Dongchan K, Lim G, Kim E, Lee SH. Ultrasound-guided prolotherapy with polydeoxyribonucleotide for painful rotator cuff tendinopathy. Pain Res Manag. 2018;2018:5. doi:10.1155/2018/8286190
2. Challoumas D, Biddle M, McLean M, Millar NL. Comparison of treatments for frozen shoulder: a systematic review and meta-analysis. JAMA Netw Open. 2020;3(12):e2029581. doi:10.1001/jamanetworkopen.2020.29581
3. Lho YM, Ha E, Cho CH, et al. Inflammatory cytokines are overexpressed in the subacromial bursa of frozen shoulder. J Shoulder Elbow Surg. 2013;22(5):666–672. doi:10.1016/j.jse.2012.06.014
4. Akbar M, McLean M, Garcia-Melchor E, et al. Fibroblast activation and inflammation in frozen shoulder. PLoS One. 2019;14(4):e0215301. doi:10.1371/journal.pone.0215301
5. Linsell L, Dawson J, Zondervan K, et al. Prevalence and incidence of adults consulting for shoulder conditions in UK primary care; patterns of diagnosis and referral. Rheumatology. 2006;45(2):215–221. doi:10.1093/rheumatology/kei139
6. Dupeyron A, Gelis A, Sablayrolles P, Bousquet PJ, Julia M, Herisson C. Heterogeneous assessment of shoulder disorders: validation of the standardized index of shoulder function. J Rehabil Med. 2010;42(10):967–972. doi:10.2340/16501977-0627
7. Fernandes MR. Correlation between functional disability and quality of life in patients with adhesive capsulitis. Acta Ortop Bras. 2015;23(2):81–84. doi:10.1590/1413-78522015230200791
8. Lee HV, Lee SJ, Nazarian A, Rodriguez EK. Adhesive capsulitis of the shoulder: review of pathophysiology and current clinical treatments. Shoulder Elbow. 2016;9(2):75–84. doi:10.1177/1758573216676786
9. Cohen C, Ejnisman B. Epidemiology of frozen shoulder. In: Shoulder Stiffness. Heidelberg: Springer Berlin; 2015:21–30.
10. Itoi E, Arce G, Bain GI, et al. Shoulder stiffness: current concepts and concerns. Arthroscopy. 2016;32:1402–1414. doi:10.1016/j.arthro.2016.03.024
11. Wong CK, Levine WN, Deo K, et al. Natural history of frozen shoulder: fact or fiction? A systematic review. Physiotherapy. 2017;103:40–47. doi:10.1016/j.physio.2016.05.009
12. Cucchi D, Marmotti A, De Giorgi S, et al. Risk factors for shoulder stiffness: current concepts. Joints. 2017;5(04):217–223. doi:10.1055/s-0037-1608951
13. Sözen T, Başaran NÇ, Tınazlı M, et al. Musculoskeletal problems in diabetes mellitus. Eur J Rheumatol. 2018;5(4):258–265. doi:10.5152/eurjrheum.2018.18044
14. Dyer BP, RathodMistry T, Burton C, et al. Diabetes as a risk factor for the onset of frozen shoulder: a systematic review and meta-analysis. BMJ Open. 2023;13:e062377. doi:10.1136/bmjopen-2022-062377
15. Kim Y-S, Kim J-M, Lee Y-G, Hong O-K, Kwon H-S, Ji J-H. Intercellular Adhesion Molecule-1 (ICAM-1, CD54) is increased in adhesive capsulitis. J Bone Joint Surg Am. 2013;95(4):
16. Hauser RA, Lackner JB, Steilen-Matias D, Harris DK. A systematic review of dextrose prolotherapy for chronic musculoskeletal pain. Clin Med Insights Arthritis Musculoskelet Disord. 2016;9:139–159. PMID: 27429562; PMCID: PMC4938120. doi:10.4137/CMAMD.S39160
17. Goswami A. Prolotherapy. J Pain Palliat Care Pharmacother. 2012;26(4):376–378. PMID: 23216178. doi:10.3109/15360288.2012.734900
18. DeChellis DM, Cortazzo MH. Regenerative medicine in the field of pain medicine: prolotherapy, platelet-rich plasma therapy, and stem cell therapy-theory and evidence. Tech Reg Anesth Pain Manag. 2011;15(2):74–80. doi:10.1053/j.trap.2011.05.002
19. Ramirez J. Adhesive capsulitis: diagnosis and management. Am Fam Physician. 2019;99(5):297–300. PMID: 30811157.
20. Hanchard N, Goodchild L, Thompson J, et al. Evidence-based clinical guidelines for the diagnosis, assessment and physiotherapy management of contracted (frozen) shoulder: a quick reference summary. Physiotherapy. 2012;98:117–120. doi:10.1016/j.physio.2012.01.001
21. Pandey V, Madi S. Clinical guidelines in the management of frozen shoulder: an update! JOIO. 2021;55:299–309. doi:10.1007/s43465-021-00351-3
22. Dyer BP, Burton C, Rathod-Mistry T, et al. Diabetes as a prognostic factor in frozen shoulder: a systematic review. Arch Rehabil Res Clin Transl. 2021;3(3):100141. ISSN 2590-1095. doi:10.1016/j.arrct.2021.100141
23. Selley RS, Johnson DJ, Nicolay RW, et al. Risk factors for adhesive capsulitis requiring shoulder arthroscopy: a clinical retrospective case series study. J Orthop. 2020;19:14–16. doi:10.1016/j.jor.2019.11.024
24. Cao W, Chen J, Pu J, Fan Y, Cao Y. Risk factors for the onset of frozen shoulder in middle-aged and elderly subjects within 1 year of discharge from a hospitalization that involved intravenous infusion: a prospective cohort study. Front Med. 2022;9:911532. PMID: 35795630; PMCID: PMC9251169. doi:10.3389/fmed.2022.911532
25. Sarasua SM, Floyd S, Bridges WC, et al. The epidemiology and etiology of adhesive capsulitis in the US medicare population. BMC Musculoskelet Disord. 2021;22(1). doi:10.1186/s12891-021-04704-9
26. Seven MM, Ersen O, Akpancar S, et al. Effectiveness of prolotherapy in the treatment of chronic rotator cuff lesions. Orthop Traumatol Surg Res. 2017;103(3):427–433. doi:10.1016/j.otsr.2017.01.003
27. Jensen K, Rabago D, Best TM, et al. Early inflammatory response of knee ligaments to prolotherapy in a rat model. J Orthop Res. 2008;26(6):816–823. doi:10.1002/jor.20600
28. Jensen KT, Rabago D, Best TM, et al. Longer term response of knee ligaments to prolotherapy in a rat injury model. Am J Sports Med. 2008;36(7):1347–1357. doi:10.1177/0363546508314431
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.