Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
A case of probable oxybutynin-induced increase in liver enzymes
Authors Alrawashdeh H ![]() , Madi L
, Madi L ![]() , Ahmed Elhada AH, Ahmed A
, Ahmed Elhada AH, Ahmed A ![]() , Serheed D
, Serheed D ![]()
Received 1 April 2018
Accepted for publication 12 June 2018
Published 10 September 2018 Volume 2018:14 Pages 1657—1660
DOI https://doi.org/10.2147/TCRM.S169868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Haneen Alrawashdeh,1 Lama Madi,2 Arwa Hassan Ahmed Elhada,1 Afif Ahmed,1 Dhiaddin Serheed3
1Department of Pharmacy, Women Wellness and Research Center, Hamad Medical Corporation, Doha, Qatar; 2Department of Pharmacy, Qatar Rehabilitation Institute, Doha, Qatar; 3Department of Physical Medicine and Rehab, Qatar Rehabilitation Institute, Doha, Qatar
Abstract: We describe the case of a 49-year-old male who presented to the emergency department with right-sided weakness and inability to speak. He was diagnosed with stroke and was admitted to Qatar Rehabilitation Institute after he was treated for the acute phase at Hamad General Hospital. As part of his management, he was started on oxybutynin 5 mg orally twice daily for the treatment of overactive bladder. Within a week, his liver enzymes started to increase. After a thorough medication review, oxybutynin was suspended as it was the only suspected medication to be responsible of this elevation in liver enzymes. When Naranjo Adverse Drug Reaction Probability Scale was used to assess the probability of an adverse drug reaction (ADR), a score of 6 was obtained indicating a “Probable” ADR. In conclusion, this is the first published report of oxybutynin-induced elevation in liver enzymes. Further reports are required to highlight this probable ADR and alert all health professionals about it.
Keywords: oxybutynin, liver enzymes, alanine aminotransferase, aspartate aminotransferase, adverse drug reaction, liver injury
Introduction
Urinary incontinence (UI) after stroke has serious impacts on the individual’s function outcome and mortality. It has a prevalence ranging from 32% to 79% on admission and 25%–28% at discharge.1,2 Urge, functional, and stress incontinence are post-stroke UI disorders which can be improved by occupational and physical therapy interventions.3,4 In patients with bladder incontinence who do not respond to nonpharmacological intervention such as scheduled voiding and tailored fluid restriction, antimuscarinic medications are the gold standard of pharmacological therapy, of which oxybutynin is an example.5,6
Oxybutynin has a direct antispasmodic effect and inhibits the muscarinic action of acetylcholine on smooth muscle.7 The drug has an elimination half-life of 2–5 hours and is eliminated through liver due to it is low concentration in urine.8 Common adverse effects of oxybutynin include dry mouth, blurred vision, somnolence, constipation, and delirium.9
An increase in liver enzymes is considered significant when both alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are 2–3 times higher than the baseline. The prevalence of abnormal liver enzyme was 10% in United States according to The National Health and Nutrition Examination Survey.7 Coagulopathy and alteration in the mental status may result from rapid deterioration of the liver function in a previously healthy individual. Moreover, acute liver failure may affect young people and result in death.8
Liver injury might occur because of using several medications. The incidence of drug-induced liver injury has been reported to be between 10 and 15 per 10,000–100,000 persons exposed to prescription medications.9,10 The National Institute of Health developed a searchable database “LiverTox” that links medications, herbs, and dietary supplements to liver injury.11
Oxybutynin-induced increase in liver enzymes has never been reported before; a search of the “LiverTox” database failed to identify any report.12 Moreover, a search in the Canadian adverse drug reaction monitoring database has not identified any report.14 Furthermore, a search conducted in different databases (Medline, Embase, and Cumulative Index of Nursing and Allied Health Literature) in August 2017 did not identify any related reports.
This case report represents our experience of increased liver enzymes due to the use of oxybutynin for the management of UI in a stroke patient.
Case presentation
This is a 49-year-old male with hypertension and chronic kidney disease. He presented to the Emergency Department on the 28th of March 2017 with right-sided weakness and inability to speak. He was found to have recent acute/early subacute infarct along left middle cerebral artery territory.
On 6th of April 2017, the patient was transferred to Qatar Rehabilitation Institute to be enrolled in an active rehabilitation program. Upon assessment, he was found to have global aphasia, dense right-sided weakness, maximally assisted in bed mobility and transfer, and totally assisted in activities of daily life.
During his hospital stay, he had episodes of elevated liver enzymes and the suspected medications (atorvastatin 40 mg orally daily and escitalopram 20 mg orally daily) were suspended with continuous monitoring of the liver enzymes. Liver enzymes started to decrease within few days after the suspension but did not reach the baseline. A week after suspending escitalopram, he was started on (oxybutynin 5 mg orally twice daily) for overactive bladder. Within a week of starting oxybutynin, liver enzymes increased again (Figures 1 and 2). A thorough medication review was done by the assigned clinical pharmacist and none of his medications was known to result in high liver enzymes. After discussing this with the physician, oxybutynin was the only suspected medication to be responsible of this elevation in liver enzymes as it was the newest medication added to his therapy, and hence, it was suspended.
 | Figure 1 Liver enzymes levels during hospital stay. |
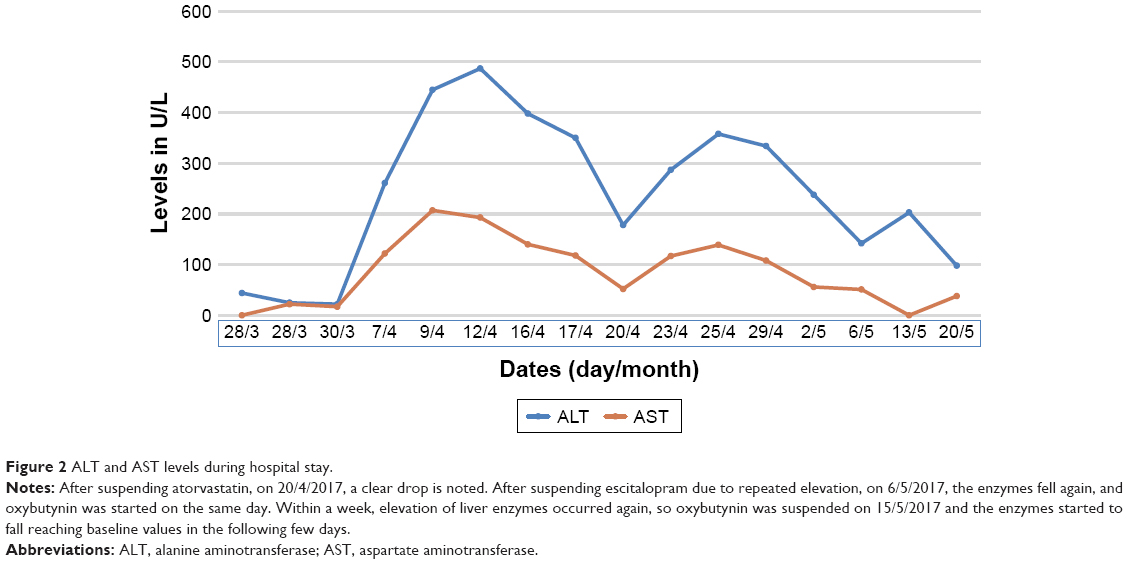 | Figure 2 ALT and AST levels during hospital stay. |
To rule out inflammatory, autoimmune, or any other underlying causes, the gastroenterology team was consulted to evaluate the case. Their primary assessment was “drug-induced hepatitis.” Their recommendations were to stop any suspected hepatotoxic medication and to do further investigations. These included full workup of hepatitis, hepatitis A virus immunoglobulin M, hepatitis C virus antibody, hepatitis E virus immunoglobulin M, antinuclear antibody, anti-smooth muscle antibody, antimitochondrial antibody, anti-liver kidney antibodies, and celiac profile – immunoglobulin A, anti-tissue transglutaminase antibodies, ceruloplasmin, and α-1 antitrypsin. All the required tests were negative and the ultrasound of the abdomen showed normal findings. Within a week of discontinuing oxybutynin, both ALT and AST were decreased to values lower than 3 times the baseline.
As the patient was lost to follow-up, consent for publication of this case was not possible. However, the case details have been sufficiently anonymized and approval for publication has been obtained from the organization’s medical research center.
Discussion
Oxybutynin-induced elevation in liver enzymes is not reported in literature. To the best of our knowledge, this is the first published report on oxybutynin-induced elevation in liver enzymes. The time course of oxybutynin prescription and discontinuation and the accompanying fluctuations in liver enzymes points out a probable adverse drug reaction (ADR).
To rate this suspected ADR, Naranjo scale was used. Naranjo scale is an ADR probability scale which was developed in 1991 by Naranjo et al13 from the University of Toronto. This scale consists of 10 questions that are answered as either “Yes/No,” or “Do not know.” Different point values (−1, 0, +1 or +2) are assigned to each answer. A score of 6 was obtained by Naranjo scale, indicating a probable oxybutynin-induced liver injury15 (Table 1).
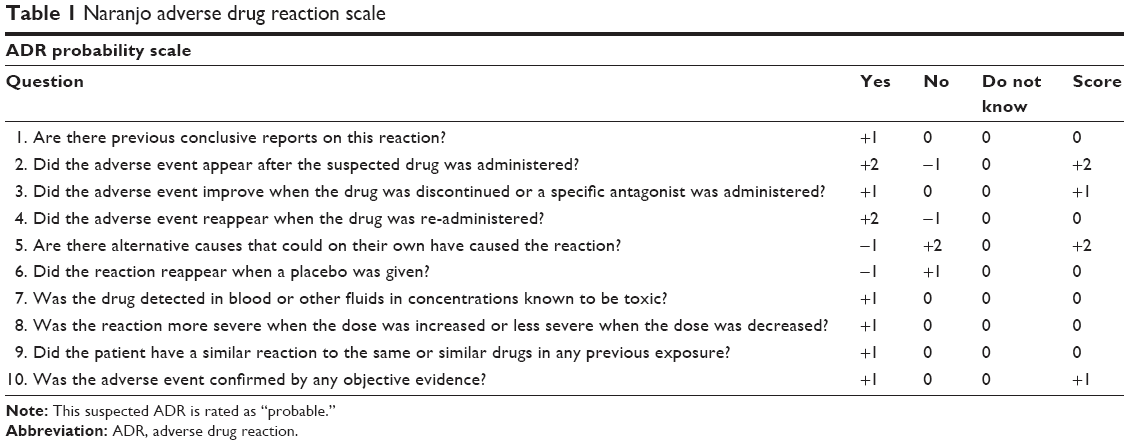 | Table 1 Naranjo adverse drug reaction scale |
Atorvastatin may induce idiosyncratic liver injury. However, it is rare but can be severe.16,17 In a meta-analysis conducted by Denus et al,20 the proportion of patients having liver function test abnormalities was low in both groups treated with statins and placebo (statins 1.14% vs placebo 1.05%, odds ratio: 1.26, 95% CI: 0.99–1.62, P=0.07).18 Although atorvastatin can cause increase in the levels of AST and ALT, it was discontinued and liver enzymes dropped accordingly before they rose again after oxybutynin was started.
Escitalopram is considered one of the antidepressants with least potential for hepatotoxicity.19,21 In this case, it was ruled out as the cause of the latest elevation in liver enzymes as the latter dropped after it was discontinued even before oxybutynin was started.
Conclusion
Our findings suspect a correlation between oxybutynin and elevations in liver enzymes. However, further controlled trials are demanded to confirm this probable ADR.
Disclosure
The authors report no conflicts of interest in this work.
References
Mehdi Z, Birns J, Bhalla A. Post-stroke urinary incontinence. Int J Clin Pract. 2013;67(11):1128–1137. | ||
Brittain KR, Peet SM, Castleden CM. Stroke and incontinence. Stroke. 1998;29(2):524–528. | ||
Agency for Health Care Policy and Research (APCHR). Urinary Incontinence Guideline Panel. Urinary Incontinence in Adults: Acute and Chronic Management. Clinical Practice Guideline. Rockville, MD: US Department of Health and Human Services; APCHR publication no. 96-0682; 1996. | ||
Abrams P, Cardozo L, Fall M, et al; Standardisation Sub-Committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21(2):167–178. | ||
Nabi G, Cody JD, Ellis G, Herbison P, Hay-Smith J. Anticholinergic drugs versus placebo for overactive bladder syndrome in adults. Cochrane Database Syst Rev. 2006;(4):CD003781. | ||
Bettez M, Tu le M, Carlson K, et al. 2012 update: guidelines for adult urinary incontinence collaborative consensus document for the Canadian urological association. Can Urol Assoc J. 2012;6(5):354–363. | ||
Yamaguchi O. Antimuscarinics and overactive bladder: other mechanism of action. Neurourol Urodyn. 2010;29(1):112–115. | ||
Hughes KM, Lang JC, Lazare R, et al. Measurement of oxybutynin and its N-desethyl metabolite in plasma, and its application to pharmacokinetic studies in young, elderly and frail elderly volunteers. Xenobiotica. 1992;22(7):859–869. | ||
Garely AD, Burrows LJ. Current pharmacotherapeutic strategies for overactive bladder. Expert Opin Pharmacother. 2002;3(7):827–833. | ||
Ioannou GN, Boyko EJ, Lee SP. The prevalence and predictors of elevated serum aminotransferase activity in the United States in 1999–2002. Am J Gastroenterol. 2006;101(1):76–82. | ||
Bernal W, Wendon J. Acute liver failure. N Engl J Med. 2013;369(26):2525–2534. | ||
Sgro C, Clinard F, Ouazir K, et al. Incidence of drug-induced hepatic injuries: a French population-based study. Hepatology. 2002;36(2):451–455. | ||
Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. | ||
Björnsson ES, Bergmann OM, Björnsson HK, Kvaran RB, Olafsson S. Incidence, presentation, and outcomes in patients with drug-induced liver injury in the general population of Iceland. Gastroenterology. 2013;144(7):1419–1425. | ||
Chang CY, Schiano TD. Review article: drug hepatotoxicity. Aliment Pharmacol Ther. 2007;25(10):1135–1151. | ||
Health Canada. Canadian Adverse Drug Reaction Monitoring Program Database. Ottawa, ON: Health Canada. Available from: http://cvp-pcv.hc-sc.gc.ca/arq-rei/index-eng.jsp. Accessed April 27, 2018. | ||
LiverTox [webpage on the Internet]. Adverse Drug Reaction Probability Scale (Naranjo); 2017. Available from: https://livertox.nih.gov/Narajo.html. Accessed January 9, 2018. | ||
Björnsson E, Jacobsen EI, Kalaitzakis E. Hepatotoxicity associated with statins: reports of idiosyncratic liver injury post-marketing. J Hepatol. 2012;56(2):374–380. | ||
Hey-Hadavi JH, Kuntze E, Luo D, Silverman P, Pittman D, Lepetri B. Tolerability of atorvastatin in a population aged ≥65 years: a retrospective pooled analysis of results from fifty randomized clinical trials. Am J Geriatr Pharmacother. 2006;4(2):112–122. | ||
de Denus S, Spinler SA, Miller K, Peterson AM. Statins and liver toxicity: a meta-analysis. Pharmacotherapy. 2004;24(5):584–591. | ||
Voican CS, Corruble E, Naveau S, Perlemuter G. Antidepressant-induced liver injury: a review for clinicians. Am J Psychiatry. 2014;171(4):404–415. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.