Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Case of Neutrophilic Dermatoses-Sweet’s Syndrome Coexisting with SAPHO Syndrome
Authors Ma M, Wei S, Yin D, Li W, Li C ![]()
Received 11 January 2023
Accepted for publication 20 March 2023
Published 27 March 2023 Volume 2023:16 Pages 739—742
DOI https://doi.org/10.2147/CCID.S404390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Mingwei Ma,1,* Shufeng Wei,2,* Dan Yin,2 Weizhong Li,2 Chen Li2
1School of Clinical Medicine, Peking Union Medical College Hospital (PUMC and CAMS), Beijing, 100730, People’s Republic of China; 2Department of Rheumatology, Fangshan Hospital Beijing University of Chinese Medicine, Beijing, 102401, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chen Li, Department of Rheumatology, Fangshan Hospital, Beijing University of Chinese Medicine, No. 4, Chengguan Health Road, Fangshan District, Beijing, People’s Republic of China, Tel +86 13810988688, Email [email protected]
Abstract: SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome is a rare disease characterized by osteoarticular and cutaneous manifestations. SAPHO syndrome mostly involves the skin, mainly presented as palmoplantar pustulosis and severe acne. Sweet’s syndrome (SS) is a neutrophilic dermatosis of unknown cause, which may be caused by autoinflammation. So far, SAPHO syndrome complicated with SS has been rarely reported worldwide. Here, we present a rare case diagnosed in our hospital with detailed clinical information. This patient presented pain and swelling in her right leg. Later, she developed red papules on her right lower eyelid and a skin biopsy showed diffuse lymphocytic and neutrophilic infiltration in the superficial dermis. She was diagnosed with SAPHO syndrome and SS according to medical history and examination. These two diseases share parts of autoinflammatory signaling pathways and might be different variations of the spectrum of autoinflammatory diseases. Through this case, we aim to provide a new horizon for the regulation of neutrophils in SAPHO syndrome and skin lesions like SS.
Keywords: SAPHO syndrome, Sweet’s syndrome, autoinflammation disease
Introduction
Synovitis, acne, pustulosis, hyperostosis and osteitis (SAPHO) syndrome is a spectrum of rare disease with osteoarticular and skin lesions as its manifestations.1 Most patients with SAPHO syndrome have cutaneous involvement, mainly manifested as palmoplantar pustulosis and severe acne. It is generally considered an autoinflammatory syndrome, which was supported by the elevation of a series of proinflammatory cytokines, such as tumor necrosis factor (TNF)-α, interleukin (IL)-1, IL-8, IL-17, and IL-18.2 Sweet’s syndrome (SS), an acute febrile neutrophilic dermatosis, is characterized by fever, painful red papules, nodules and plaques, elevated peripheral blood leucocytes and neutrophil infiltration in the dermis.3 The adaptive immune system including IL-17, IL-1β, and inflammasome activation has a significant role in neutrophil recruitment and activation.4 The association of SAPHO syndrome with SS has rarely been reported.
Here, we present a case of neutrophilic dermatoses including SS in a patient with SAPHO syndrome with detailed information.
Case Report
A 48-year-old female complained of intermittent pain and swelling in her right leg in 2010. Due to the lack of standardized diagnosis and treatment, the symptoms persisted. In August 2018, she developed fever without obvious cause. Three days later, several rice-sized red papules appeared on her left lower eyelid, gradually forming a painful edematous erythema with a central blister (Figure 1A), with pressure pain and no exudation. A skin biopsy was performed and showed slight thickening of the epidermis, diffuse lymphocytic and neutrophilic infiltration in the superficial dermis, and dilated and congested blood vessels (Figure 1C). Laboratory tests showed elevated WBC, neutrophil, ESR and C-reactive protein, and ANA, RF, and HLA-B27 were all negative. The diagnosis of SS was made. The patient was treated with topical dexamethasone and the erythema gradually disappeared (Figure 1B) but symptoms of bone pain persisted. Osteomyelitis was considered and the pain and swelling were relieved after receiving zoledronic acid. In January 2019, the pain recurred and the symptoms were not relieved by intermittent oral celecoxib. Through systematic imaging examinations and laboratory tests, we excluded malignant tumor and infectious diseases. X-ray and CT examination (Figure 2A and B) showed diffuse bone thickening in the upper and lower segments of the right fibula, suggesting chronic osteomyelitis; MRI examination (Figure 2C and D) suggested limited bone marrow edema in the right fibula; 99mTc-MDP whole-body bone scintigraphy (Figure 2E and F) showed abnormal radioactive concentrations on the right fibula, and fusion tomography demonstrated thickening of the bone cortex, suggesting an inflammatory lesion. Physical examination showed swelling and tenderness in the right leg without ulceration and sinus formation. Combined with symptoms and imaging examinations, the diagnosis of SAPHO syndrome was made, and etoricoxib 60 mg/d and sulfasalazine 2 g/d were received. The pain and swelling in the right leg disappeared at the follow-up in March 2022.
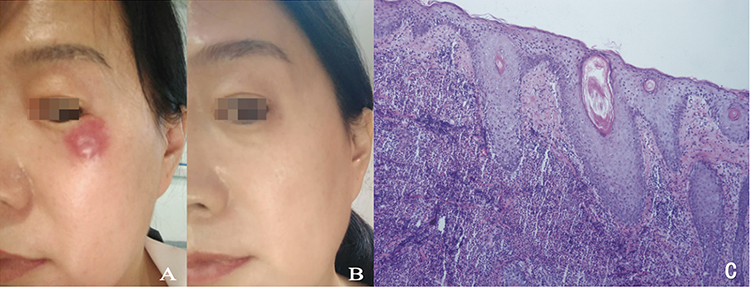 |
Figure 1 Sweet syndrome manifestation (A) edematous erythema on the left lower eyelid with a central blister; (B) Facial skin lesions subsided 1 month after treatment (C) Histopathological examination of the skin lesion (HE 40×) showed slightly increased epidermis thick, diffuse infiltration of lymphocytes and neutrophils in the superficial dermis, vasodilation and congestion. |
 |
Figure 2 Imaging examination of SAPHO syndrome (A and B) X-ray and CT examination showed diffuse bone thickening in the upper and lower segments of the right fibula. (C and D) MRI examination suggested limited bone marrow edema in the right fibula; (E and F) 99mTc-MDP whole-body bone scintigraphy showed abnormal radioactive concentrations on the right fibula, and fusion tomography demonstrated thickening of the bone cortex. |
Discussion
SAPHO syndrome is considered a rare autoinflammatory disease. The cases of SAPHO syndrome complicated by SS mainly focused on chronic recurrent multifocal osteomyelitis in children and were relatively rare in adults.5 This patient developed typical skin lesion and fever with elevated WBC, neutrophil, CRP and glucocorticoid treatment was effective, additionally skin pathology indicated SS, thus meeting diagnostic criteria of SS.6 The diagnosis of SS was made. According to the widely used diagnostic criteria for SAPHO syndrome proposed by Khan in 1994,1 the patient was diagnosed with SAPHO.
There has been previous case report of neutrophilic dermatoses coexisting with SAPHO syndrome.7 Both SAPHO and neutrophilic dermatoses are characterized by sterile inflammatory, so they may have a potential association. SS and SAPHO have previously been believed to be triggered by a low-virulence persistent pathogen, and sustained by an autoimmune response.5 In neutrophilic dermatoses, autoinflammation may play a significant role. Neutrophilic diseases may be considered autoinflammatory in origin based on the overexpression of pro-inflammatory cytokines like IL-1β, IL-17 and TNF-α, which promote neutrophil recruitment. Dysregulation of neutrophil homeostasis can lead to excessive inflammation and skin lesions.8,9 SAPHO syndrome and SS share part of the inflammatory signaling pathway and have an immunological basis. The expressions of IL-1, TNF-α, IL-8, IL-17 were significantly high in both SS and SAPHO patients10.2,11 The pathogenesis of these two diseases may involve some of the same inflammatory molecules such as inflammasome, TNF-α, IL-1, and IL-17.12 Over-expression of cytokines/chemokines and molecules amplifying the inflammatory pathway supports the theory that SAPHO and SS are autoinflammatory diseases. SAPHO syndrome and SS may be considered different variations of the spectrum of autoinflammatory diseases.
As for treatment, NSAIDs are currently chosen as first-line medications, DMARDs, targeted drugs, bisphosphonate, etc. have also been frequently reported.13 For SS with limited lesions, topical corticosteroids may be effective and targeted therapy with IL-1 and TNF-α inhibitors could also be used.13 In cases of refractory and insufficient responses to glucocorticoid treatment, efficacy of IL‐1 inhibition has been reported.14 It took 10 years from the onset of the disease to the diagnosis of SAPHO syndrome. The patient was treated with etoricoxib and sulfasalazine for SAPHO syndrome and topical dexamethasone for SS, and her symptoms were effectively relieved, with no recurrence at long-term follow-up. Correct diagnosis and timely and rational medication can improve the symptoms of patients and avoid unnecessary surgery.
As for limitation, the coexistence of the two diseases was observed, but the underlying mechanisms and causality, as well as treatment strategies, are lacking in studies with larger samples.
This case suggests a potential association between SAPHO syndrome and SS and may imply that they belong to family of autoinflammatory diseases, which is worthy of further exploration in the relevant mechanism and use of medications.
Ethics Approval and Consent to Participate
This work was approved by the medical ethics committee of Fangshan Hospital of Beijing University of Chinese Medicine with the following reference numbers: FZJ JS-2021-002.
Consent to Participate
Informed consent to participate in the study was obtained from all participants.
Consent Statement
Written informed consent was provided by patient to have the case details and any accompanying images published. Institutional approval was not required to publish the case details.
Funding
This work was supported by the National Natural Science Foundation of China (grant number: 82074246).
Disclosure
The authors declare no conflict of interest.
References
1. Kahn MF, Khan MA. The SAPHO syndrome. Baillieres Clin Rheumatol. 1994;8(2):333–362. doi:10.1016/S0950-3579(94)80022-7
2. Liu S, Tang M, Cao Y, et al. Synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome: review and update. Ther Adv Musculoskelet Dis. 2020;12:1759720x20912865. doi:10.1177/1759720X20912865
3. Sweet RD. An acute febrile neutrophilic dermatosis. Br J Dermatol. 1964;76:349–356. doi:10.1111/j.1365-2133.1964.tb14541.x
4. Agrawal A, Arif SH, Kumarasan K, et al. Sweet’s syndrome: an update. Curr Pediatr Rev. 2022;18(4):265–273. doi:10.2174/1573396318666220223100208
5. Tlougan BE, Podjasek JO, O’Haver J, et al. Chronic recurrent multifocal osteomyelitis (CRMO) and synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome with associated neutrophilic dermatoses: a report of seven cases and review of the literature. Pediatr Dermatol. 2009;26(5):497–505. doi:10.1111/j.1525-1470.2009.00984.x
6. Dabade TS, Davis MD. Diagnosis and treatment of the neutrophilic dermatoses (pyoderma gangrenosum, Sweet’s syndrome). Dermatol Ther. 2011;24(2):273–284. doi:10.1111/j.1529-8019.2011.01403.x
7. Sone Y, Namiki T, Tokoro S, et al. A case of neutrophilic dermatoses including pyoderma gangrenosum as a continuous disease spectrum to SAPHO syndrome. Clin Exp Dermatol. 2018;43(7):829–831. doi:10.1111/ced.13620
8. Marzano AV, Borghi A, Wallach D, et al. A comprehensive review of neutrophilic diseases. Clin Rev Allergy Immunol. 2018;54(1):114–130. doi:10.1007/s12016-017-8621-8
9. Marzano AV, Ortega-Loayza AG, Heath M, et al. Mechanisms of inflammation in neutrophil-mediated skin diseases. Front Immunol. 2019;10:1059. doi:10.3389/fimmu.2019.01059
10. Marzano AV, Fanoni D, Antiga E, et al. Expression of cytokines, chemokines and other effector molecules in two prototypic autoinflammatory skin diseases, pyoderma gangrenosum and Sweet’s syndrome. Clin Exp Immunol. 2014;178(1):48–56. doi:10.1111/cei.12394
11. Heath MS, Ortega-Loayza AG. Insights Into the pathogenesis of Sweet’s Syndrome. Front Immunol. 2019;10:414. doi:10.3389/fimmu.2019.00414
12. Murthy AS, Leslie K. Autoinflammatory skin disease: a review of concepts and applications to general dermatology. Dermatology. 2016;232(5):534–540. doi:10.1159/000449526
13. Chamot AM, Benhamou CL, Kahn MF, et al. Acne-pustulosis-hyperostosis-osteitis syndrome. Results of a national survey. 85 cases. Rev Rhum Mal Osteoartic. 1987;54(3):187–196. French.
14. Satoh TK, Mellett M, Contassot E, et al. Are neutrophilic dermatoses autoinflammatory disorders? Br J Dermatol. 2018;178(3):603–613. doi:10.1111/bjd.15105
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.