Back to Journals » Infection and Drug Resistance » Volume 15
A Case of Misdiagnosed as Upper Urinary Tract Obstruction Caused by the Fungal Ball
Authors Liu J, Jiang Y, Liu Z, Song Q, Li Z
Received 28 June 2022
Accepted for publication 5 October 2022
Published 22 October 2022 Volume 2022:15 Pages 6109—6114
DOI https://doi.org/10.2147/IDR.S380291
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Jian Liu, Ying Jiang, Zhe Liu, Qun Song, Zhuo Li
Department of Urology, The First Affiliated Hospital of Hunan Normal University Hunan Provincial People’s Hospital, Changsha, People’s Republic of China
Correspondence: Zhuo Li, Tel +8615197591937, Email [email protected]
Abstract: Upper urinary tract obstruction caused by fungal balls is a rare urinary system disease. We admitted an elderly man with symptoms of urinary tract infection and diabetes mellitus. When the patient was transported into the hospital, a CT scan revealed right renal pelvis dilatation and gas buildup, routine urinalysis showing full field of view of white blood cells and middle urinary bacteria and fungi cultures came back negative, leading to the incorrect diagnosis of emphysematous pyelonephritis with Aerogenes infection. When the diagnosis is confirmed, surgery and antifungal therapy are used to deal with both the obstruction and the fungal ball.
Keywords: fungal ball, urinary tract obstruction, misdiagnosed, emphysematous pyelonephritis, infection
Introduction
The common causes of upper urinary tract obstruction are stone or tumor, while fungal ball is extremely rare. Patients with inadequate immunity, tumors, diabetes, long-term use of antibiotics or immunosuppressants are the risks for developing fungus infections.1 A classic opportunistic pathogen with a broad distribution in nature is Candida. Candida tropicalis and Aspergillus are less frequent among them, whereas Candida albicans is more prevalent.2 Fungal balls are mixed masses of fungal cells, exfoliated renal and urothelial cells, which can arise from nuclear aggregates of necrotic tissue (papillary necrosis), mucosal debris, old blood clots, and foreign or stone debris.3 The main treatment includes oral antifungal drugs, surgical debridement, adequate drainage, and renal pelvis irrigation with antifungal drugs. We present a case of a fungal ball-induced blockage of the upper urinary tract that was incorrectly identified as an infection with Aerogenes and emphysematous pyelonephritis.
Case Presentation
For more than three months, a 68-year-old man with recurring right low back discomfort, frequent urination, urgency, dysuria, white purulent pee, and infrequent low-grade fever complained. He has a background in Type 2 Diabetes Mellitus. At the time of admission, the HbA1c was 12.10%, the postprandial blood glucose level was 14.7 mmol/L, and the fasting blood glucose level was 10.7 mmol/L. His typical hypoglycemic medications included acarbose and insulin aspart. Acarbose is 50mg before lunch, insulin aspart is 10 units subcutaneously in the morning and 12 units subcutaneously before bedtime. Percussion ache in the right renal area was discovered during a physical examination. The imaging study CT (Figure 1) revealed that the right renal pelvis was noticeably dilated, and several aberrant density foci and gas buildup in the right renal pelvis and calyx. The results of the laboratory tests revealed that the blood routine leukocyte count was 11*10^9, the C-reactive protein level was 56, and the urine routine leukocyte count was the full field, but the midstream pee fungus culture was negative, and included 9.06 umol/l of blood urea nitrogen and 99.00 umol/l of serum creatinine. Emphysematous Pyelonephritis with Aerogenes Infection and Urinary Tract Obstruction was the preoperative diagnosis that was intended. Following empiric antibiotic therapy, the patient’s fever and right waist discomfort continued to worsen, and his urine production fell from 1500mL to 450mL. A urinary tract obstruction may be present if there are more severe clinical symptoms and a continued decrease in urine production. Under general anesthesia, ureteroscopy and removal of ureteral infections, as well as cystoscopy and removal of bladder infections, were carried out to clear the blockage and identify the source of infection. White spherical infections (Figures 2 and 3) were discovered during emergency surgery in the right renal pelvis, right ureter, and bladder. Negative pressure suction was employed during a right percutaneous nephrostomy to remove the infection since the infection in the renal pelvis could not be eliminated. Candida tropicalis was identified in bacterial and fungal cultures of the postoperative renal pelvis drainage, although bacterial cultures were negative. According to a drug susceptibility test (Table 1), fluconazole, a sensitive antifungal medication, was administered following surgery. Fluconazole 300mg was infused into the renal pelvis for two weeks following the procedure, and fluconazole 400mg was administered orally once daily while in the hospital, by the results of the medication susceptibility test. The final diagnosis was urinary tract blockage brought on by fungal balls after the intraoperative observations, renal pelvis infection bacterial and fungal culture results, and CT auxiliary investigation were combined. At the same time, there should be concomitant Candida tropicalis-caused fungal emphysematous pyelonephritis. The postoperative CT scan of the urinary system (Figure 4) revealed clear lesions, and the right stoma tube and urine bag were clear in color. The renal drainage tube was removed after the urine culture’s results were negative, and the patient was then released from the hospital. One month after discharged, when the weekly urine fungal culture was negative, the DJ tube was withdrawn. Six months following discharge, a follow-up examination revealed no signs of a fungal infection recurrence.
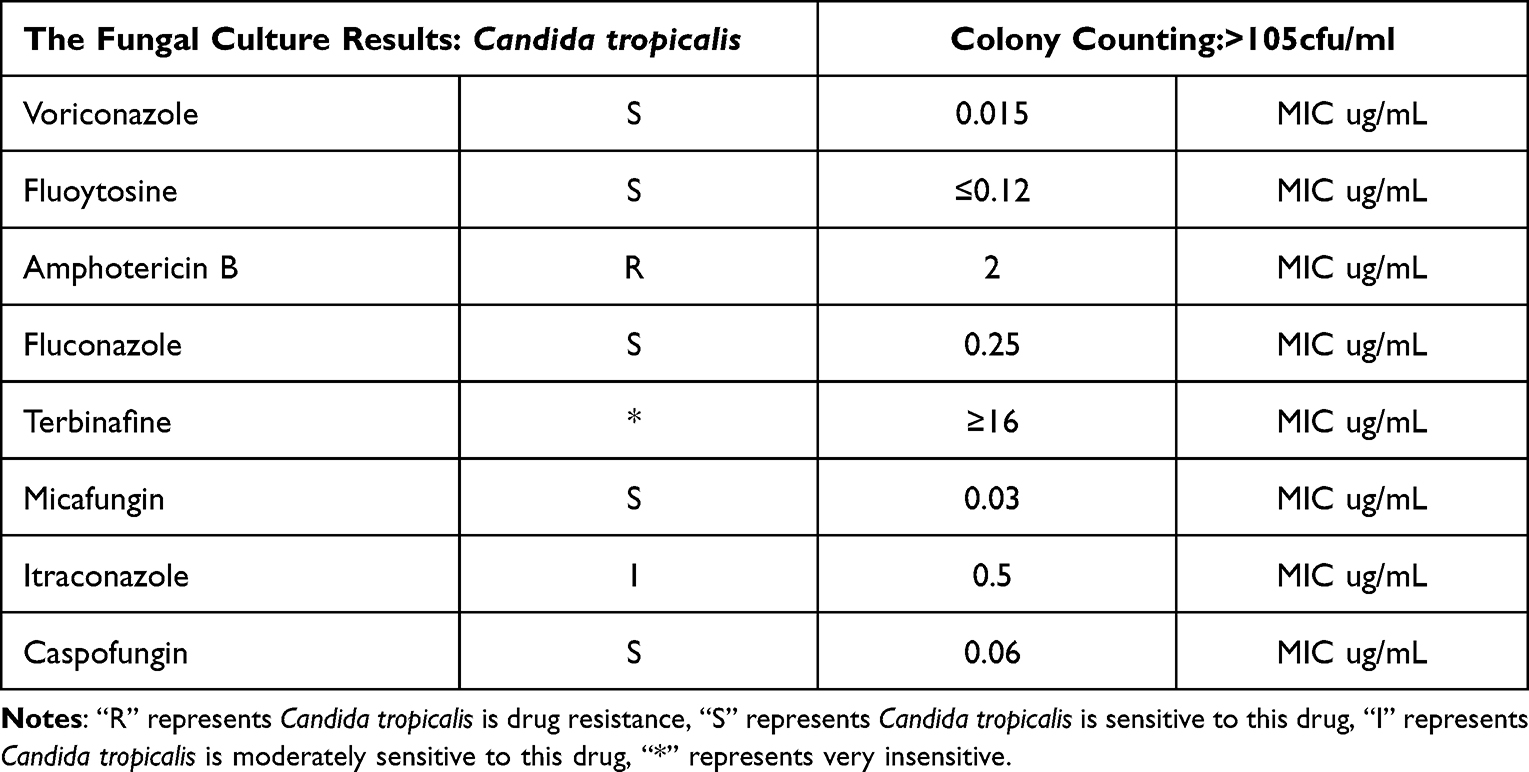 |
Table 1 Anti-Fungal Susceptibility Test |
 |
Figure 1 (A) In the bilateral kidneys in the contrast-enhanced CT window, the side marked with red represents the right renal pelvis, and the pneumopelvic shadow in the renal pelvan be seen at the red arrow, while the dilatation of the left renal pelvis is not obvious on the right side, and there is no obvious gas accumulation. (B) In contrast-enhanced CT windows in different slices, right pneumopelvic shadow is seen at the red arrow, and plenty of air and infected shadows are seen in the renal pelvis. (C) In the unenhanced CT window, the CT value of the right renal pelvis can be seen at the two red marks compared with the CT value of the infection in the renal pelvis. |
 |
Figure 2 The red arrow symbol represents the fungal infection in the renal pelvis in the surgical field. |
 |
Figure 3 A portion of yellowish-white nodular infection was surgically removed from the right renal pelvis. |
 |
Figure 4 (A) In the CT window, the red arrows point to the DJ tubes placed in the kidneys and bladder (B) in different slices of the CT window, the DJ tube of the kidney is indicated by the red arrow. |
Discussion
According to research, some patients with urinary tract fungal infections often have diabetes. Urinary tract fungal infection is a relatively uncommon type of urinary tract infection that typically affects people with low immunity, malignant tumors, diabetes, long-term use of antibiotics and immunosuppressive agents, etc.4 In nature, Candida is extensively dispersed and can parasitism the mucous membranes of the human skin, mouth, gastrointestinal tract, vagina, and anus.1,5,6 Urinary tract stone frequently results in fungal infection, but only fungal balls seldom clog the urinary tract.3 At the ureteropelvic junction, fungal ball infections are more prevalent.2 When a routine urine test reveals that the white blood cells are packed with visual fields, when a CT scan reveals an obvious infection and gas buildup in the right renal pelvis, when a mid-segment urine fungal culture is negative, and when the symptoms do not improve after receiving a course of antibiotics, the diagnosis of gas-producing bacteria-type emphysematous pyelonephritis is made. According to reports, ultrasound and CT examination of upper urinary tract obstruction due to fungal ball infection showed predominantly dilated renal pelvis with one or more hyperechoic areas in the kidney.7,8 The appearance of pneumoshadows in right renal pelvis and the inability to collect fungal cultures of the infectious agent in the renal right pelvis both cast doubt on the initial diagnosis. This was adjusted due to decrease urine output and symptoms that were not alleviated. The ultimate diagnosis was upper urinary tract blockage caused by fungal balls based on the findings at surgery, CT scan the results, and culture results of infectious substances in the renal pelvis. Cause of pneumoshadows in the renal pelvis is believed that Candida tropicalis-caused fungal emphysematous pyelonephritis is what causes numerous gas accumulation in the renal pelvis.9,10
Patients with type 2 diabetes mellitus frequently have high blood sugar levels for extended periods, which decrease leukocyte chemotaxis, adhesion, and bactericidal activity, which impairs immune system function.11 Patients’ glycemic control over the course of 8 to 12 weeks is frequently assessed using their glycosylated hemoglobin A1c (HbA1c).12 This patient’s Hb1Ac was 12.10%, above the normal range. The HbA1c usually shows the unsatisfactory past blood sugar management. So, low body resistance and poor blood sugar regulation make people more susceptible to fungal ball infections, and problems with glucose metabolism can make illnesses worse. Additionally, it has been claimed that the pH and content of urine are related to urinary tract infections caused by Candida tropicalis.13
It is crucial to quickly and accurately diagnose urinary tract blockage brought on by a fungus in the urinary tract. Ureteroscopy and DJ tube placement as internal drainage, and Percutaneous nephroscopy with indwelling nephrostomy tube as external drainage. Two ways provide us with a better basis for positive diagnosis and treatment. The method of internal drainage + exterior drainage is decisively employed to clear the fungal balls in the renal pelvis, ureter, and bladder to the greatest extent and try to manage the infection as much as possible to relieve the urinary tract obstruction caused by fungal balls.14,15 Among them, the negative pressure suction approach was used to maintain the lower perfusion pressure in the renal pelvis and ureter and limit the systemic inflammatory reaction or even septic shock to prevent the fungus from entering the blood during the operation.15,16 Low postoperative fungemia incidence is achieved by maintaining negative pressure in the renal pelvis and rapidly removing the fungal ball.17 Following the procedure, fluconazole intravenous infusion, and continuous renal pelvis lavage were employed to effectively prevent and treat the Candida tropicalis fungus.18,19 Fluconazole 300mg was infused into the renal pelvis for two weeks following the procedure, and fluconazole 400mg was administered orally once daily while in the hospital, and Fluconazole 400mg was continued for four weeks after discharge.18,20 Regarding the experience of such situations. Firstly, the primary goal is prompt drainage and antifungal therapy to remove the obstruction produced by an infection in the urinary system. Second, in order to promote postoperative recovery in those with weak immunity and uncontrolled diabetes blood sugar, immunity must be increased and blood sugar must be stabilized. Last but not least, urinary stones are complicated by a fungal infection, and the infection is simple to relapse after migration. Antifungal drugs should be prescribed after surgery. After the double-J tube was taken out following discharge, oral fluconazole was continued for an additional two weeks to avoid recurrence. Bacterial and fungal cultures were reviewed every week for a month. Regular eye exams should be performed since endophthalmitis has been linked to recurrent fungal infections.21
Conclusion
First, internal drainage and external drainage can be used to relieve obstruction and remove the fungal balls. During the surgery, negative pressure suction of the renal pelvis can reduce the chance of postoperative infection. Second, elderly people with long-term unstable blood sugar control are a high risk factor for urinary tract fungal infection. Finally, fluconazole intrarenal infused postoperatively is successful in treating fungal balls.
Informed Consent Statement
Our department has told the patient that his clinical data and personal details would be used for the report, and the patient voluntarily accepted and agreed to use it in the literature report. The patient provided his written informed consent to participate in this report.
Disclosure
The authors have no conflict of interest with any institution or individual. Our institution had approved to publish the case details.
References
1. Ng KP, Kuan CS, Kaur H, et al. Candida species epidemiology 2000–2013: a laboratory-based report. Trop Med Int Health. 2015;20(11):1447–1453. doi:10.1111/tmi.12577
2. Kauffman CA. Diagnosis and management of fungal urinary tract infection. Infect Dis Clin North Am. 2014;28(1):61–74. doi:10.1016/j.idc.2013.09.004
3. Tan WP, Turba UC, Deane LA. Renal fungus ball: a challenging clinical problem. Urologia. 2017;84(2):113–115. doi:10.5301/uro.5000201
4. Dembner AG, Pfister RC. Fungal infection of the urinary tract: demonstration by antegrade pyelography and drainage by percutaneous nephrostomy. AJR Am J Roentgenol. 1977;129(3):415–418. doi:10.2214/ajr.129.3.415
5. Barchiesi F, Orsetti E, Gesuita R, Skrami E, Manso E; Candidemia Study Group. Epidemiology, clinical characteristics, and outcome of candidemia in a tertiary referral center in Italy from 2010 to 2014. Infection. 2016;44(2):205–213. doi:10.1007/s15010-015-0845-z
6. Kenney PJ. Imaging of chronic renal infections. AJR Am J Roentgenol. 1990;155(3):485–494. doi:10.2214/ajr.155.3.2117344
7. Kale H, Narlawar RS, Rathod K. Renal fungal ball: an unusual sonographic finding. J Clin Ultrasound. 2002;30(3):178–180. doi:10.1002/jcu.10049
8. Kawashima A, Sandler CM, Goldman SM, et al. CT of renal inflammatory disease. Radiographics. 1997;17(4):851–66;discussion 867–8. doi:10.1148/radiographics.17.4.9225387
9. Brieland J, Essig D, Jackson C, et al. Comparison of pathogenesis and host immune responses to Candida glabrata and Candida albicans in systemically infected immunocompetent mice. Infect Immun. 2001;69(8):5046–5055. doi:10.1128/IAI.69.8.5046-5055.2001
10. Ideguchi S, Yamamoto K, Ikeda A, et al. A case of bilateral emphysematous pyelonephritis caused by Candida albicans. J Infect Chemother. 2019;25(4):302–306. doi:10.1016/j.jiac.2018.10.011
11. Peleg AY, Weerarathna T, McCarthy JS, Davis TM. Common infections in diabetes: pathogenesis, management and relationship to glycaemic control. Diabetes Metab Res Rev. 2007;23(1):3–13. doi:10.1002/dmrr.682
12. Zhang XW, Zhang XL, Xu B, Kang LN. Comparative safety and efficacy of insulin degludec with insulin glargine in type 2 and type 1 diabetes: a meta-analysis of randomized controlled trials. Acta Diabetol. 2018;55(5):429–441. doi:10.1007/s00592-018-1107-1
13. Hansen CR, Pressler T, Nielsen KG, et al. Inflammation in Achromobacter xylosoxidans infected cystic fibrosis patients. J Cyst Fibros. 2010;9(1):51–58. doi:10.1016/j.jcf.2009.10.005
14. Zhang Z, Wang X, Chen D, et al. Minimally invasive management of acute ureteral and severe infection caused by upper urinary tract calculi. J Xray Sci Technol. 2020;28(1):125–135. doi:10.3233/XST-190576
15. Wu ZH, Liu TZ, Wang XH, et al. Double-sheath vacuum suction versus vacuum-assisted sheath minimally invasive percutaneous nephrolithotomy for management of large renal stones: single-center experience. World J Urol. 2021;39(11):4255–4260. doi:10.1007/s00345-021-03731-4
16. Li P, Huang Z, Sun X, et al. Comparison of vacuum suction sheath and non-vacuum suction sheath in minimally invasive percutaneous nephrolithotomy: a meta-analysis. J Invest Surg. 2022;35(5):1145–1152. doi:10.1080/08941939.2021.1995538
17. Woloshuk A, Lee M, Assmus M, et al. A case of ureteral fungal mass removal in a patient taking empagliflozin. CEN Case Rep. 2021;10(4):603–607. doi:10.1007/s13730-021-00616-8
18. Abdeljaleel OA, Alnadhari I, Mahmoud S, et al. Treatment of renal fungal ball with fluconazole instillation through a nephrostomy tube: case report and literature review. Am J Case Rep. 2018;23(1):1179–1183. doi:10.12659/AJCR.911113
19. Fisher JF. Candida urinary tract infections--epidemiology, pathogenesis, diagnosis, and treatment: executive summary. Clin Infect Dis. 2011;52(Suppl 6):S429–32. doi:10.1093/cid/cir108
20. Manosuthi W, Chetchotisakd P, Nolen TL, et al. Monitoring and impact of fluconazole serum and cerebrospinal fluid concentration in HIV-associated cryptococcal meningitis-infected patients. HIV Med. 2010;11(4):276–281. doi:10.1111/j.1468-1293.2009.00778.x
21. Pappas PG, Kauffman CA, Andes DR, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin Infect Dis. 2016;62(4):e1–50. doi:10.1093/cid/civ933
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.