Back to Journals » Infection and Drug Resistance » Volume 19
A Case of Listeria monocytogenes Meningitis (Complicated) with Hydrocephalus and Occipital Lobe Infarction
Authors Liu M, Chen Y, Xie P, Xu W, Huang S, Liu B
Received 12 May 2026
Accepted for publication 30 June 2026
Published 15 July 2026 Volume 2026:19 624063
DOI https://doi.org/10.2147/IDR.S624063
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Meiyan Liu,1,* Yuquan Chen,2,* Pin Xie,1 Weijie Xu,1 Shuiwen Huang,1 Baorong Liu1
1Department of Intensive Care Unit, Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou, Fujian, 350025, People’s Republic of China; 2Department of Hepatology, Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou, Fujian, 350025, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Baorong Liu, Department of Intensive Care Unit, Mengchao Hepatobiliary Hospital of Fujian Medical University, 66 JinTang Road, Cangshan District, Fuzhou, Fujian, 350025, People’s Republic of China, Email [email protected]
Background: Listeria monocytogenes (LM) meningitis is a rare but severe infection, particularly in immunocompromised patients, often leading to complications such as hydrocephalus, markedly increasing treatment complexity and the risk of poor outcomes.
Case Presentation: We report a case of LM meningitis in an immunocompromised patient. The illness began with fever and gastrointestinal symptoms, followed by neck stiffness and altered consciousness. LM was identified via blood culture, cerebrospinal fluid (CSF) culture, and metagenomic next-generation sequencing (mNGS). During hospitalization, the patient developed decompensated hydrocephalus and a right occipital lobe infarction, emergent external ventricular drainage (hospital day 4) and subsequent ventriculoperitoneal shunting (hospital day 44) were performed, which were potentially life-saving. After comprehensive treatment and rehabilitation, the patient was discharged on day 85 without significant neurological deficits.
Conclusion: Clinical presentation of LM meningitis may be atypical, especially in immunocompromised patients. In such patients, aggressive management of hydrocephalus-including timely CSF diversion-is potentially life-saving. Early pathogen detection through combined blood culture, CSF culture, and mNGS, together with prompt, targeted antimicrobial therapy and dynamic management of neurological complications such as hydrocephalus, is essential for improving clinical outcomes.
Keywords: Listeria monocytogenes, bacterial meningitis, hydrocephalus, cerebral infarction, case report
Introduction
Listeria monocytogenes (LM) is a Gram-positive, non-spore-forming short rod bacterium widely distributed in soil, water, and food processing environments, and can be transmitted through contaminated dairy products, meat, ready-to-eat foods, and refrigerated items.1–4 Human listeriosis primarily affects pregnant women, neonates, the elderly, and immunocompromised individuals.5–9 Among invasive listeriosis manifestations, central nervous system (CNS) involvement represents one of the most severe clinical forms, presenting as meningitis, meningoencephalitis, or rhombencephalitis, and is associated with high mortality.2,7,10–14 Clinical presentation of LM meningitis is often atypical; early symptoms may be limited to fever, gastrointestinal complaints, or mild alterations in consciousness. Definitive diagnosis relies on blood or cerebrospinal fluid (CSF) cultures and molecular pathogen detection.13 Hydrocephalus is a significant complication of bacterial meningitis, especially in severe cases, markedly increasing treatment complexity and the risk of poor outcomes.14,15 Here, we report a case of LM meningitis in an immunocompromised patient, complicated by hydrocephalus and a right occipital lobe ischemic lesion. While several cases of LM meningitis with hydrocephalus have been reported, the concurrent occurrence of hydrocephalus and occipital lobe infarction—particularly in a patient with chronic liver failure and severe immunosuppression—is rarely described. Moreover, detailed documentation of the timing and decision-making process for sequential neurosurgical interventions (EVD followed by VP shunting) is limited in the existing literature. Cerebrovascular complications, including cerebral infarction, are increasingly recognized as important sequelae of bacterial meningitis. In LM meningitis, infection-related vasculitis, endothelial injury, and cerebral hypoperfusion secondary to elevated intracranial pressure may all contribute to ischemic events. Understanding these potential mechanisms is critical for early recognition and management. The patient ultimately achieved favorable recovery following anti-infective therapy, CSF diversion procedures, and rehabilitation. By presenting this case, we aim to highlight the importance of recognizing LM meningitis in immunocompromised hosts, the potential for concurrent cerebrovascular complications, and the life-saving role of timely neurosurgical intervention for hydrocephalus.
Case Report
Patient History
A 44-year-old male was admitted to our hospital in early September 2025 with a 1-day history of fever. During the disease course, his maximum temperature reached 39.2 °C, accompanied by nausea, vomiting, and abdominal pain. On admission, pharyngeal follicles were observed, but there was no headache or limb convulsions. Initial cranial CT showed no obvious abnormalities, and due to the patient’s critical condition, brain MRI could not be performed immediately. Laboratory tests revealed elevated C-reactive protein (CRP) at 151.41 mg/L, Neutrophil percentage of 88.7%, leukopenia (WBC 3050 cells/μL), elevated procalcitonin (PCT) at 6.15 ng/mL, and hyponatremia (serum sodium 128.5 mmol/L). Stool testing showed 3+ fungal presence.
Past Medical History
The patient had chronic hepatitis B (HBsAg positive) for 25 years. In December 2024, HBV DNA was 7.55×107 IU/mL. Two months prior to admission, he was hospitalized at our center and diagnosed with subacute-on-chronic liver failure and chronic hepatitis B, undergoing two plasma exchange sessions. Due to persistent hyperbilirubinemia (total bilirubin 414.1 µmol/L, direct bilirubin 290.5 µmol/L), he requested transfer to a tertiary hospital (Zhongshan Hospital, Fudan University, Shanghai) for further management. During this period, he received antiviral therapy and one month of corticosteroid therapy. Notably, the patient reported consuming leftover refrigerated food two days prior to admission.
Other Auxiliary Examinations
Screening for hepatitis C virus, syphilis, and HIV was negative. Nasal and pharyngeal swabs were negative for bacterial and fungal cultures. Smears for meningococcus, Cryptococcus, and tuberculosis were negative. Chest and abdominal CT revealed no evidence of tumors. Cardiac ultrasound and electrocardiography were unremarkable.
Treatment and Clinical Course
Upon admission, severe infection was suspected. Given his liver failure and immunocompromised status, empirical therapy with meropenem (2 g every 8 hours, IV), micafungin (100 mg once daily, IV), and ganciclovir (5 mg/kg every 12 hours) was initiated (All doses were adjusted according to the patient’s renal and hepatic function). On hospital day 2, the patient developed involuntary limb tremors, persistent fever, and neck stiffness. Neurological examination revealed neck rigidity with positive Kernig’s sign and Brudzinski’s sign. Pupils were bilateral equal and reactive to light. Muscle strength was grossly grade 4/5 in all extremities, with hyperreflexia and bilateral positive Babinski signs. No focal cranial nerve deficits were observed. CRP increased to 177.10 mg/L and PCT to 6.78 ng/mL. T-lymphocyte subset analysis revealed CD4 count of 85 cells/µL (16.65%), indicating severe immunosuppression. Concurrent CMV DNA quantification was 5.33×104 IU/mL. Blood cultures initially reported Gram-positive bacterial growth, later confirmed as Listeria monocytogenes (LM). Additionally, Pettenkofer Staphylococcus was isolated, whose clinical significance required context-specific interpretation. Based on infection risk assessment, vancomycin was added, along with thymosin alpha-1 and immunoglobulin therapy. The patient initially presented without typical meningeal signs, and cranial CT on admission showed no abnormalities. However, when neck stiffness and altered consciousness developed on hospital day 2, lumbar puncture was promptly arranged. On hospital day 3, lumbar puncture was performed; cerebrospinal fluid (CSF) opening pressure could not be accurately measured due to low pressure. CSF analysis showed WBC 321×106/L (49.9% mononuclear cells), Protein 3056 mg/L, Chloride 95.2 mmol/L, and Glucose 2.55 mmol/L. CSF culture was performed by inoculating samples onto blood agar and chromogenic agar, followed by incubation at 37°C for 48 hours. CSF culture and metagenomic next-generation sequencing (mNGS) confirmed LM, establishing the diagnosis of LM meningitis. Antimicrobial therapy was adjusted to high-dose intravenous penicillin (4 million units every 4 hours), along with mannitol for intracranial pressure management. Multidisciplinary consultation recommended short-term corticosteroids to reduce inflammatory response and potential arachnoid adhesion. On the morning of hospital day 4, the patient developed sudden consciousness impairment, with a Glasgow Coma Scale (GCS) score of 6 and increased limb muscle tone, pupillary light reflexes were sluggish. The patient was unresponsive to verbal commands but withdrew to painful stimuli. Cranial CT revealed enlargement of the bilateral lateral and third ventricles, consistent with hydrocephalus and a low-density area in the right occipital lobe suggestive of ischemic injury (Figure 1). The ventriculomegaly was characterized by dilation of the lateral and third ventricles, suggesting a communicating pattern, likely secondary to impaired CSF reabsorption due to inflammatory adhesions. That evening, the patient experienced brief right upper limb twitching, likely reflecting secondary seizure activity associated with hydrocephalus.
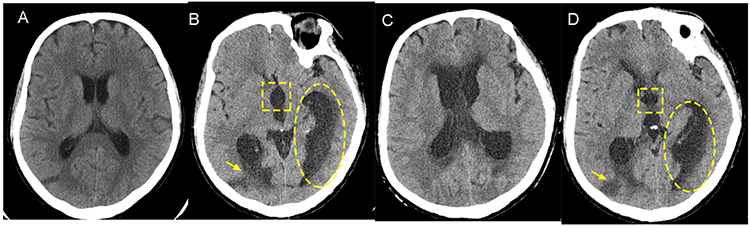 |
Figure 1 Cranial CT findings during the acute phase. (A) CT on the day of admission showing no obvious abnormalities. (B) CT findings on hospital day 4. (C) CT showing ventriculomegaly. (D) prominent dilatation of the posterior horns of the lateral ventricles. Yellow dashed boxes indicate hydrocephalus, characterized by enlargement of the bilateral lateral ventricles and third ventricle, with rounded and blunted anterior and posterior horns of the lateral ventricles (The third ventricle is indicated by yellow square dashed boxes, and the posterior horns of the lateral ventricles are indicated by yellow oval dashed boxes). Yellow arrows indicate a low-density lesion in the right occipital lobe, suggestive of ischemic injury. |
That evening, the patient was transferred to the neurosurgery department and underwent an emergency procedure: right frontal horn ventricular puncture with external ventricular drainage (EVD) and subcutaneous reservoir placement. Four days postoperatively, the patient regained clear consciousness with a GCS score of 14 (E4V4M6), pupils were equal and reactive bilaterally. Muscle strength improved to grade 4/5 in all limbs, with decreased muscle tone, although intermittent secondary seizures persisted. The daily drainage from the reservoir was approximately 100–200 mL. One week after surgery, the patient was transferred to a general ward. CSF parameters were dynamically monitored (Figure 2). The antimicrobial regimen was adjusted to ampicillin combined with amikacin, and antiepileptic therapy including oxcarbazepine, levetiracetam, valproate, and perampanel was administered. Follow-up cranial CT demonstrated a reduction in ventricular size and improvement of hydrocephalus compared to previous imaging (Figure 3).
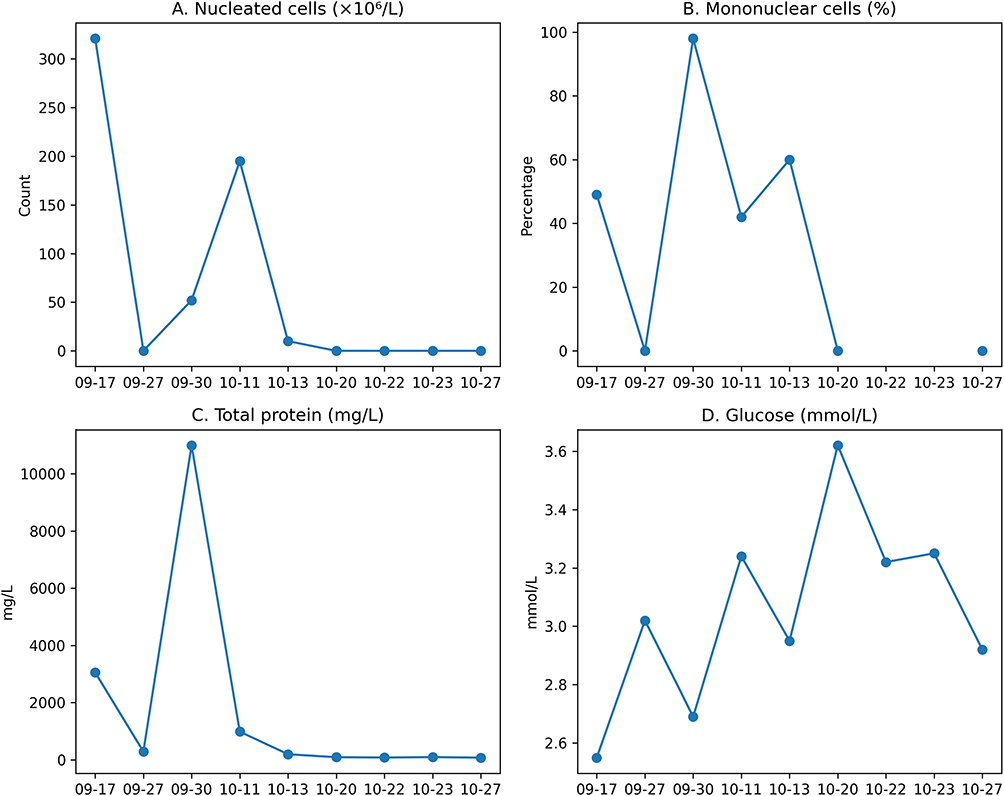 |
Figure 2 Dynamic changes of cerebrospinal fluid (CSF) routine and biochemical parameters during hospitalization.The CSF parameters gradually improved following treatment. (A) CSF white blood cell count. (B) Percentage of mononuclear cells in CSF. (C) CSF total protein concentration. (D) CSF glucose concentration. |
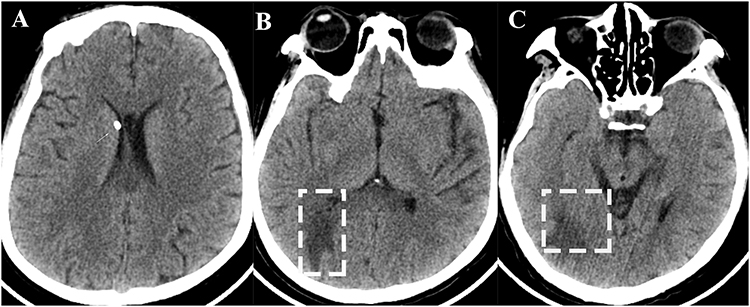 |
Figure 3 Follow-up cranial CT after treatment. Compared with previous imaging, hydrocephalus has improved, with no significant supratentorial ventricular enlargement observed. (A) CT showing partial resolution of ventriculomegaly. White arrows indicate significant improvement of hydrocephalus. (B) Axial non-contrast CT showing large fan-shaped low-density areas in the right parietal lobe (white dashed boxes). (C) Axial non-contrast CT at a lower level showing more extensive and prominent low-density areas in the bilateral occipital lobes (white dashed boxes). |
However, on hospital day 44, the patient again developed altered consciousness, presenting with lethargy and delayed responsiveness. At that time, CSF routine and biochemical parameters were largely normalized. Repeat cranial CT, however, revealed recurrent ventricular enlargement and worsening hydrocephalus (Figure 4), accompanied by reduced external ventricular drainage output. After a comprehensive preoperative assessment, the patient underwent left frontal horn ventricular puncture and left ventriculoperitoneal (VP) shunt placement the following day.
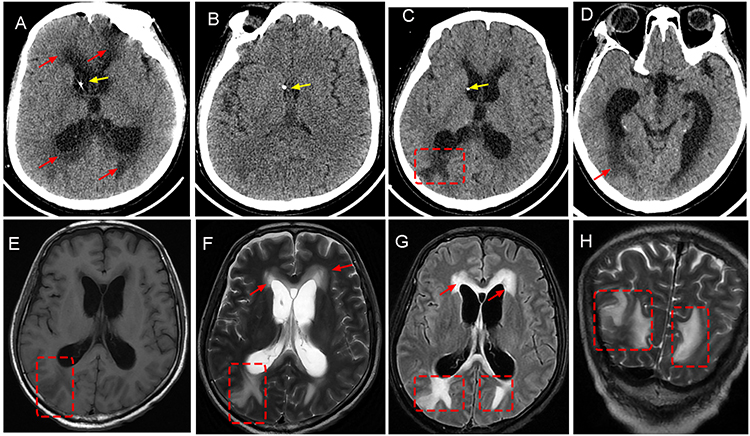 |
Figure 4 Imaging of recurrent progressive hydrocephalus. Upper panel-CT images (A–D): (A) Non-contrast CT showing marked dilation of the bilateral lateral ventricles with an intraventricular catheter (yellow arrow), compressed and thinned cerebral parenchyma, and scattered abnormal densities (red arrows). (B) CT image demonstrating an intraventricular catheter (yellow arrow) within the ventricular system. (C) CT showing hydrocephalus with periventricular low-density edema (red square), and an intraventricular catheter (yellow arrow). (D) Axial CT image of the posterior fossa showing hydrocephalus of the posterior horns of the lateral ventricles with scattered low-density lesions (red arrows). Lower panel- MRI images (E–H): (E) (T1WI), On T1-weighted imaging, a relatively well-defined hypointense (dark) area is observed in the right occipital region (red square on the left side of the image), suggesting edema or tissue loss due to infarction. (F) (T2WI), On T2-weighted imaging, the right occipital region (red square) shows a prominent patchy hyperintense (red arrows and red square) signal. (G) (FLAIR), The FLAIR sequence, which suppresses cerebrospinal fluid signal, reveals extensive periventricular hyperintense edema (red arrows and red square). (H) (DWI), The DWI sequence shows hyperintense signals in the bilateral periventricular white matter (red dashed boxes) and the right occipital lobe. |
On hospital day 54, the patient was fully conscious but developed sore throat, speech impairment, and aphonia. Based on clinical presentation and imaging, frontal lobe cerebral edema was suspected. He was treated with methylprednisolone (40 mg twice daily, intravenously) and mannitol to reduce cerebral edema and intracranial pressure. Subsequently, the patient experienced transient neurological sequelae, including drooling, involuntary lower limb tremors, and bradykinesia. With continued anti-infective therapy, antiepileptic treatment, intracranial pressure management, and rehabilitation, the patient regained the ability to speak on hospital day 71. Methylprednisolone was gradually tapered and discontinued. Follow-up MRI demonstrated improvement compared with previous scans (Figure 5). By hospital day 85, the patient had largely regained independent daily living abilities and was discharged. Neurological examination at discharge revealed orientation to person, place, and time. Cranial nerves were intact. Muscle strength was grade 4+/5 in all extremities with normal tone. Gait was stable, and coordination tests were performed normally. No residual neurological deficits were observed. During hospitalization, serum sodium, CRP, PCT, and Hemoglobin levels were dynamically monitored (Figure 6).
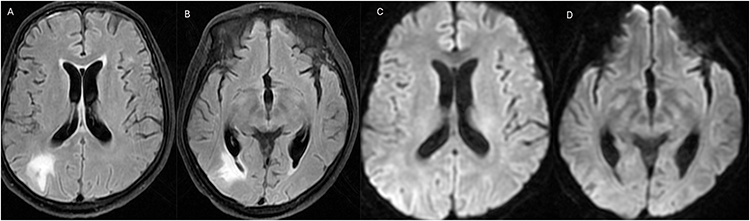 |
Figure 5 Follow-up MRI after treatment. Ventricular hydrocephalus has further improved compared with previous imaging. (A) (contrast-enhanced T1WI), abnormal enhancement in the right occipital lobe with bilateral ventriculomegaly. (B) (contrast-enhanced T1WI), enhancing lesion in the right occipital lobe with bilateral ventriculomegaly. (C) (FLAIR), bilateral ventriculomegaly (hydrocephalus). (D) (DWI), restricted diffusion in the right occipital lobe with bilateral ventriculomegaly. |
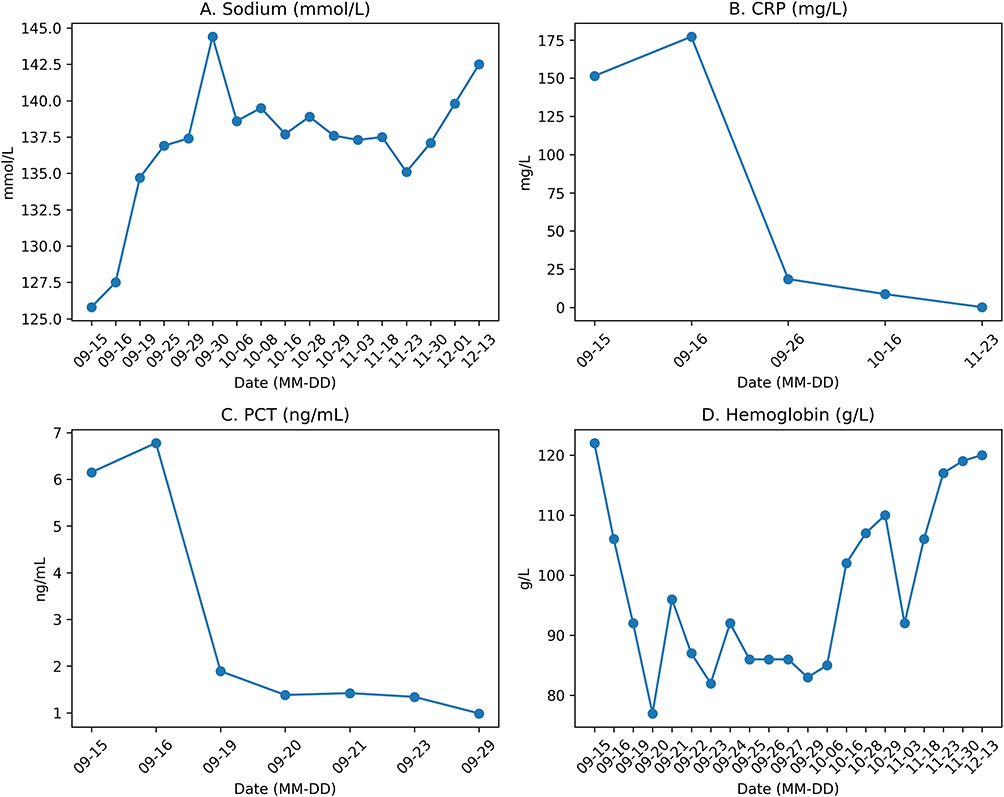 |
Figure 6 Dynamic changes of relevant laboratory parameters during hospitalization. Longitudinal changes in serum sodium (A), C-reactive protein (B), procalcitonin (C), and hemoglobin (D) during hospitalization. Serial measurements from admission to discharge are shown. Overall, all parameters demonstrated a gradual improvement over time. (MM-DD indicates the date of measurement.). |
Discussion
Compared with common bacterial meningitis pathogens such as Streptococcus pneumoniae and Neisseria meningitidis, Listeria monocytogenes (LM) exhibits stronger neurotropism and intracellular survival, allowing hematogenous dissemination into the central nervous system (CNS) and leading to meningitis, meningoencephalitis, or rhombencephalitis.16,17 In this case, the patient had subacute-on-chronic liver failure, recent prolonged corticosteroid use, and significant CD4+ T-cell depletion, representing a typical high-risk host. Additionally, the patient reported consumption of leftover refrigerated food prior to admission, providing an epidemiological clue for LM infection. This case highlights that in immunocompromised patients presenting with fever and gastrointestinal symptoms that subsequently progress to CNS involvement, LM should be considered early in the differential diagnosis.
Neuroinvasiveness is a central determinant of the pathogenicity of Listeria monocytogenes (LM). The process by which LM crosses the blood-brain barrier and the blood-CSF barrier is associated with virulence factors, including the internalin family, as well as hypervirulent clones.2,18–20 Unlike many community-acquired bacterial meningitis pathogens, LM is intrinsically resistant to cephalosporins. Therefore, if empirical therapy does not cover LM, targeted treatment may be delayed.21–23 In this case, the patient initially received broad-spectrum empirical therapy. Following confirmation of LM by blood culture, CSF culture, and metagenomic next-generation sequencing (mNGS), the antimicrobial regimen was promptly adjusted to target LM. This highlights the importance of combining multiple pathogen-detection methods. Notably, when CSF culture yield is influenced by prior antibiotic use, timing of specimen collection, and specimen quality, mNGS provides a crucial complement for early and precise diagnosis.
One of the most notable clinical issues in this case was the sequential occurrence of hydrocephalus and right occipital lobe ischemic lesions. Existing evidence suggests that a pathophysiological association between these two phenomena is possible; however, as a single-case observation, it is insufficient to establish hydrocephalus as a definitive causal factor for the infarction. Based on the literature and the patient’s clinical course, several potential mechanisms can be considered. First, bacterial meningitis can induce infection-related vasculitis or endothelial injury, leading to vascular narrowing, local thrombosis, and increased vulnerability of cerebral perfusion.24,25 Second, hydrocephalus may elevate intracranial pressure, further reducing cerebral perfusion pressure and predisposing vulnerable brain regions to ischemia.26 Third, local mass effects resulting from ventricular enlargement may additionally compromise adjacent brain tissue and microcirculation. In this case, systematic cerebrovascular imaging and perfusion studies were not performed, making it difficult to delineate the relative contribution of infectious vasculitis, hypoperfusion, and local mechanical factors. Therefore, a more cautious interpretation is that hydrocephalus and occipital lobe ischemic lesions may be associated. This underscores that in LM meningitis patients presenting with deteriorating consciousness, clinicians should be alert to both decompensated intracranial pressure and cerebrovascular complications. Importantly, we acknowledge that the patient’s clinical presentation and recovery cannot be attributed solely to LM meningitis. The right occipital lobe infarction, as demonstrated by imaging, likely contributed substantially to the neurological deficits observed during hospitalization. The pathophysiological mechanisms underlying this infarction are likely multifactorial, encompassing infection-related vasculitis, reduced cerebral perfusion pressure secondary to hydrocephalus, and local mechanical compression from ventricular enlargement. While LM infection served as the initial trigger, the subsequent cerebrovascular event and hydrocephalus together shaped the complex clinical trajectory. The absence of comprehensive cerebrovascular imaging (eg, MR angiography or perfusion studies) prevents definitive differentiation among these possibilities. Therefore, the clinical picture in this case should be interpreted as a complication of severe LM meningitis rather than a direct manifestation of the infection itself. We caution against overinterpreting the relationship and acknowledge that the occipital infarction may have resulted from multifactorial mechanisms, rather than hydrocephalus alone.
Clinical manifestations of central nervous system (CNS) infection caused by Listeria monocytogenes (LM) are often nonspecific and may include fever, nausea, vomiting, altered mental status, or only mild meningeal irritation.27,28 In this case, the patient did not initially present with typical headache, and cerebrospinal fluid (CSF) opening pressure was not elevated during the early lumbar puncture, highlighting that the absence of classic signs of meningitis should not delay diagnosis. On the other hand, hydrocephalus is a significant complication of severe LM meningitis. Previous case series have reported a non-negligible incidence, and its occurrence often indicates a more severe clinical course, prolonged treatment duration, and may necessitate repeated CSF diversion procedures.15,28–30 In this patient, both external ventricular drainage and ventriculoperitoneal shunting were required, underscoring the complexity of managing such complications.
Furthermore, this case highlights the value of dynamic laboratory monitoring. The patient developed hyponatremia early in the disease course, which gradually resolved as infection control was achieved and neurological status improved. Cerebrospinal fluid (CSF) analysis showed decreased chloride, markedly elevated protein, and relatively modest increases in cell count. This pattern is consistent with previous reports of LM meningitis but may be confused with tuberculous or fungal meningitis.13 Therefore, in immunocompromised hosts with CNS infection, a single CSF result is often insufficient for differential diagnosis. Comprehensive evaluation should integrate pathogen detection, imaging evolution, and serial CSF assessments.
Regarding the use of corticosteroids, whether they should be routinely combined with treatment for LM meningitis remains controversial.31–35 In this case, the patient had already received prolonged corticosteroid therapy prior to LM onset due to liver failure, representing a high-risk host for infection. After disease onset, short-term corticosteroid therapy was administered following multidisciplinary evaluation, aiming to reduce inflammatory response and potential arachnoid adhesions. Based on this case, corticosteroid use in LM meningitis should be strictly individualized, carefully balancing potential benefits against the risk of immunosuppression, rather than applying protocols established for other bacterial meningitis indiscriminately. Overall, the key aspects of management in this case included early recognition of LM, timely adjustment of targeted antimicrobial therapy, dynamic assessment of hydrocephalus with prompt CSF diversion when indicated, along with seizure control, intensive care support, and early rehabilitation.
This case has several limitations. First, as a single-case observation, it cannot establish a direct causal relationship between hydrocephalus and cerebral infarction. Second, complete cerebrovascular imaging and perfusion data were not obtained, preventing further differentiation among infectious vasculitis, hypoperfusion, and other potential mechanisms. Third, some treatment decisions were influenced by the patient’s critical condition and transport constraints, making it difficult to follow an ideal management pathway. Despite these limitations, this case offers several clinically relevant lessons: (1) LM meningitis should be considered in immunocompromised patients with atypical presentations; (2) hydrocephalus and cerebrovascular complications may coexist and require prompt recognition; and (3) timely neurosurgical intervention can be life-saving even in severely affected patients. The detailed clinical trajectory and management decisions presented here provide practical guidance for clinicians encountering similar complex cases.
Conclusion
LM meningitis may present with atypical symptoms but can progress rapidly in immunocompromised hosts, which is a key risk factor to recognize. Aggressive management of hydrocephalus (including timely CSF diversion) is potentially life-saving in these patients. Combined blood culture, cerebrospinal fluid (CSF) culture, and metagenomic next-generation sequencing (mNGS) facilitate early diagnosis. Timely, targeted antimicrobial therapy, close monitoring of hydrocephalus, and prompt CSF diversion when indicated are crucial for improving prognosis. Although hydrocephalus and occipital lobe infarction were observed concurrently in this patient, the available evidence does not support a causal relationship between them. This association should therefore be interpreted with caution. Nevertheless, in patients with deteriorating consciousness or focal neurological deficits, clinicians should also be alert to potential concomitant cerebrovascular complications.
Ethics Approval and Consent to Participate
Informed consent for publication was obtained from the patient and his family. Institutional approval was not required to publish this case report.
Patient Consent for Publication
Written informed consent for publication of this case report was obtained from the patient and their family.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Díaz-Martínez C, Bolívar A, Mercanoglu Taban B, Kanca N, Pérez-Rodríguez F. Exploring the antibiotic resistance of Listeria monocytogenes in food environments - a review. Crit Rev Microbiol. 2025;51(5):731–9. doi:10.1080/1040841X.2024.2412007
2. Koopmans MM, Brouwer MC, Vázquez-Boland JA, van de Beek D. Human Listeriosis. Clin Microbiol Rev. 2023;36(1):e0006019. doi:10.1128/cmr.00060-19
3. Allende A, Allende A, Allende A, et al; EFSA Panel on Biological Hazards (BIOHAZ). Listeria monocytogenes contamination of ready-to-eat foods and the risk for human health in the EU. EFSA J. 2018;16(1):e05134. doi:10.2903/j.efsa.2018.5134
4. Phelps CC, Vadia S, Arnett E, et al. Relative roles of Listeriolysin O, Inla, and InlB in Listeria monocytogenes uptake by host cells. Infect Immun. 2018;86(10). doi:10.1128/iai.00555-18
5. Vallejo P, Cilla G, López-Olaizola M, Vicente D, Marimón JM. Epidemiology and clinical features of listeriosis in Gipuzkoa, Spain, 2010–2020. Front Microbiol. 2022;13:894334. doi:10.3389/fmicb.2022.894334
6. Sun L, Cai H, Wu Y, et al. Ampicillin-induced resistant variants of Listeria monocytogenes: effects on growth, survival, and virulence. Food Res Int. 2025;221(Pt 4):117537. doi:10.1016/j.foodres.2025.117537
7. Chen SY, Lee JJ, Chien CC, et al. High incidence of severe neurological manifestations and high mortality rate for adult Listeria monocytogenes meningitis in Taiwan. J Clin Neurosci. 2020;71:177–185. doi:10.1016/j.jocn.2019.08.072
8. Niu Y, Li W, Xu B, et al. Risk factors associated with food consumption and food-handling habits for sporadic listeriosis: a case-control study in China from 2013 to 2022. Emerg Microbes Infect. 2024;13(1):2307520. doi:10.1080/22221751.2024.2307520
9. Ricci A, Allende A, Bolton D, et al. Listeria monocytogenes contamination of ready-to-eat foods and the risk for human health in the EU. EFSA J. 2018;16(1). doi:10.2903/j.efsa.2018.5134
10. Fan Z, Xie J, Li Y, Wang H. Listeriosis in mainland China: a systematic review. Int J Infect Dis. 2019;81:17–24. doi:10.1016/j.ijid.2019.01.007
11. Mota MI, D’Alessandro B, Braga V, et al. Genomic analysis of Listeria monocytogenes diversity over a 10-year period in Uruguay. Sci Rep. 2025;15(1):38361. doi:10.1038/s41598-025-22190-0
12. Senay TE, Ferrell JL, Garrett FG, et al. Neurotropic lineage III strains of Listeria monocytogenes disseminate to the brain without reaching high titer in the blood. mSphere. 2020;5(5):e00871–20. doi:10.1128/mSphere.00871-20
13. Kou X, An D. A 48-year-old man with fever, nauseous, vomiting, and dizzy: a CARE case report. Medicine. 2024;103(31):e39015. doi:10.1097/MD.0000000000039015
14. Engelen-Lee JY, Koopmans MM, Brouwer MC, Aronica E, van de Beek D. Histopathology of Listeria Meningitis. J Neuropathol Exp Neurol. 2018;77(10):950–957. doi:10.1093/jnen/nly077
15. Kasanmoentalib ES, Brouwer MC, van der Ende A, van de Beek D. Hydrocephalus in adults with community-acquired bacterial meningitis. Neurology. 2010;75(10):918–923. doi:10.1212/WNL.0b013e3181f11e10
16. Drevets DA, Bronze MS. Listeria monocytogenes: epidemiology, human disease, and mechanisms of brain invasion. FEMS Immunol Med Microbiol. 2008;53(2):151–165. doi:10.1111/j.1574-695X.2008.00404.x
17. Liang JJ, He XY, Ye H. Rhombencephalitis caused by Listeria monocytogenes with hydrocephalus and intracranial hemorrhage: a case report and review of the literature. World J Clin Cases. 2019;7(4):538–547. doi:10.12998/wjcc.v7.i4.538
18. Banovic F, Schulze S, Abu Mraheil M, et al. Different involvement of vimentin during invasion by Listeria monocytogenes at the blood-brain and the blood-cerebrospinal fluid barriers in vitro. Int J Mol Sci. 2022;23(21):12908. doi:10.3390/ijms232112908
19. Maury MM, Tsai YH, Charlier C, et al. Uncovering Listeria monocytogenes hypervirulence by harnessing its biodiversity. Nat Genet. 2016;48(3):308–313. doi:10.1038/ng.3501
20. Liu C, Ma X, Jia B, et al. Function analysis of LIPI-4 in Listeria monocytogenes reveals a key role of flagella formation in the regulation of virulence. Virulence. 2025;16(1):2543144. doi:10.1080/21505594.2025.2543144
21. Dickstein Y, Oster Y, Shimon O, et al. Antibiotic treatment for invasive nonpregnancy-associated listeriosis and mortality: a retrospective cohort study. Eur J Clin Microbiol Infect Dis. 2019;38(12):2243–2251. doi:10.1007/s10096-019-03666-0
22. Halfman C, Slate L, Yamamoto J, Jones S. Immunocompromised Child on Infliximab: a Case Report of Listeria monocytogenes Meningitis. Clin Pract Cases Emerg Med. 2020;4(4):530–532. doi:10.5811/cpcem.2020.7.48053
23. Maertens De Noordhout C, Devleesschauwer B, Maertens De Noordhout A, et al. Comorbidities and factors associated with central nervous system infections and death in non-perinatal listeriosis: a clinical case series. BMC Infect Dis. 2016;16:256. doi:10.1186/s12879-016-1602-3
24. Vergouwen MD, Schut ES, Troost D, van de Beek D. Diffuse cerebral intravascular coagulation and cerebral infarction in pneumococcal meningitis. Neurocrit Care. 2010;13(2):217–227. doi:10.1007/s12028-010-9387-5
25. Jia Y, Wang W, Wang X, Jiao L, Wang Y. Staphylococcus aureus meningitis complicated with intracranial hemorrhage and cerebral infarction: a case report. Int J Neurosci. 2022;132(12):1221–1224. doi:10.1080/00207454.2021.1879064
26. Pensato U, Demchuk AM, Menon BK, et al. Cerebral infarct growth: pathophysiology, pragmatic assessment, and clinical implications. Stroke. 2025;56(1):219–229. doi:10.1161/STROKEAHA.124.049013
27. Chen L, Pei M, Wang X, et al. Analysis of a case report of meningitis caused by Listeria monocytogenes. Front Med (Lausanne). 2024;11:1440225. doi:10.3389/fmed.2024.1440225
28. Li C, Liu M, Ji Y, et al. Clinical characteristics and prognostic indicators in Listeria monocytogenes meningoencephalitis: a retrospective case series and literature review. BMC Neurol. 2025;25(1):420. doi:10.1186/s12883-025-04410-2
29. Bodilsen J, Schønheyder HC, Nielsen H. Hydrocephalus is a rare outcome in community-acquired bacterial meningitis in adults: a retrospective analysis. BMC Infect Dis. 2013;13:321. doi:10.1186/1471-2334-13-321
30. Ueno A, Ikawa M, Maeda K, et al. Persistent severe cerebral edema with neutrophil infiltration following Listeria meningitis. Intern Med. 2022;61(22):3431–3434. doi:10.2169/internalmedicine.8291-21
31. Brouwer MC, McIntyre P, Prasad K, van de Beek D. Corticosteroids for acute bacterial meningitis. Cochrane Database Syst Rev. 2015;2015(9):CD004405. doi:10.1002/14651858.CD004405.pub5
32. Brouwer MC, van de Beek D. Adjunctive dexamethasone treatment in adults with Listeria monocytogenes meningitis: a prospective nationwide cohort study. EClinicalMedicine. 2023;58:101922. doi:10.1016/j.eclinm.2023.101922
33. van Veen KEB, Brouwer MC, van der Ende A, van de Beek D. Bacterial meningitis in patients using immunosuppressive medication: a population-based prospective nationwide study. J Neuroimmune Pharmacol. 2017;12(2):213–218. doi:10.1007/s11481-016-9705-6
34. McGill F, Heyderman RS, Michael BD, et al. The UK joint specialist societies guideline on the diagnosis and management of acute meningitis and meningococcal sepsis in immunocompetent adults. J Infect. 2016;72(4):405–438. doi:10.1016/j.jinf.2016.01.007
35. Charlier C, Perrodeau É, Leclercq A, et al; MONALISA study group. Clinical features and prognostic factors of listeriosis: the MONALISA national prospective cohort study. Lancet Infect Dis. 2017;17(5):510–519. doi:10.1016/S1473-3099(16)30521-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.