")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Case of Granuloma Faciale Successfully Treated with Minocycline
Received 9 June 2023
Accepted for publication 11 August 2023
Published 29 August 2023 Volume 2023:16 Pages 2337—2339
DOI https://doi.org/10.2147/CCID.S425239
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Lin Liu,1,2 Yuexi He,1,2 Jianmin Chang1,2
1Department of Dermatology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Peking Union Medical College, Chinese Academy of Medical Sciences, Graduate School of Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Jianmin Chang, Department of Dermatology, Beijing Hospital, National Center of Gerontology; Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, No. 1 DaHua Road, Dong Dan, Beijing, 100730, People’s Republic of China, Tel +86-010-85133303, Email [email protected]
Abstract: Granuloma faciale (GF) is a rare chronic inflammatory dermatosis in clinical practice. The etiology is not yet clear, and it often occurs on the face. The progression of skin lesions is slow and persistent, with almost no self regression and a risk of recurrence, which may lead to disfigurement. We reported a 61-year-old male with GF who had poor reaction with topical corticosteroids and calcineurin inhibitors, but the lesions were significantly improved after systematic application of minocycline. This report describes the good clinical effect of minocycline on GF.
Keywords: granuloma faciale, minocycline, treatment
Introduction
Granuloma faciale (GF) is a chronic benign skin disease that is rarely observed in clinical practice. It is currently believed that it may be related to certain infections, ultraviolet radiation, and immune abnormalities.1 However, its precise etiology remains unclear.2 Clinical manifestations of GF include single or multiple reddish brown or purplish red nodules and plaques on the face, occasionally occurring in areas outside the face.3 The progression of skin lesions is slow and persistent, rarely self subsiding, causing a risk of disfigurement. Therefore, once diagnosed, active treatment is of paramount importance. Current treatment schemes include local, intralesional and systemic corticosteroid, local calcineurin inhibitors, systemic hydroxychloroquine, clofazimine and so on. However, due to individual differences in patient responses to various treatments, some patients often do not respond to the treatment. Therefore, the treatment of GF may be difficult.4–6 Given the anti-inflammatory properties of minocycline, such as down-regulation of proinflammatory cytokine production and inhibition of neutrophil chemotaxis, we tried to evaluate the efficacy of minocycline in the treatment of GF.
Case Report
A 61-year-old male presented with a red plaque on his left cheek for two months (Figure 1). Initially, it was a red papule, which gradually developed into a plaque, with scattered red papules on the edge of the plaque, without tenderness or photosensitivity. The patient had no symptoms of discomfort such as itching or pain. He had previously used tacrolimus and glucocorticoid drugs externally, but the treatment effect was poor. The patient has a history of diabetes. Histopathological examination revealed mild epidermal spongy edema with parakeratosis, and extensive infiltration of inflammatory cells in the dermis, including eosinophils, neutrophils, and lymphocytes. The superficial capillaries in the dermis dilated, and the blood vessel walls swelled (Figure 2). Based on these findings, the patient was diagnosed with GF and given systematic oral minocycline (100mg bid). After 3 weeks of oral administration, the plaque significantly flattened, and inflammation reduced (Figure 1).
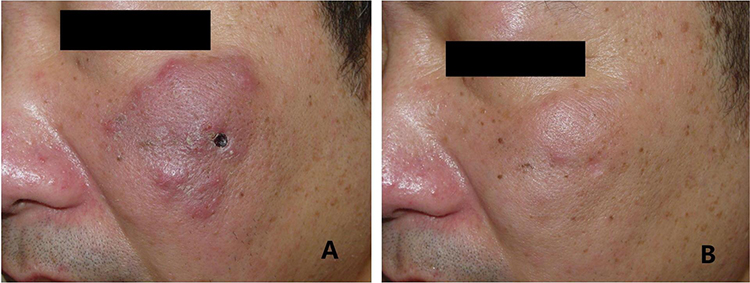 |
Figure 1 (A) Clinical manifestations before treatment (The scab is caused by the biopsy). (B) Significant improvement of the lesions after 3 weeks. |
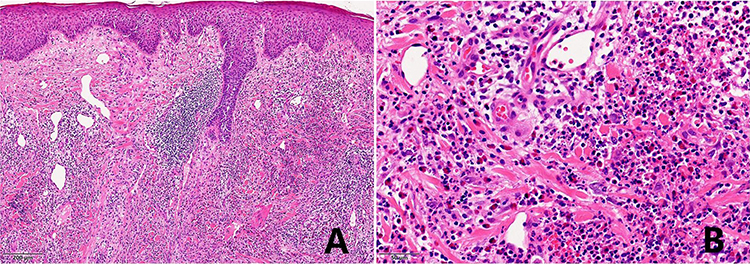 |
Figure 2 Histopathology: (A) mild epidermal spongy edema with parakeratosis (hematoxylin-eosin, x100). (B) Extensive infiltration of inflammatory cells in the dermis, including eosinophils, neutrophils, and lymphocytes. The superficial capillaries in the dermis dilated, and the blood vessel walls ssuppl welled (hematoxylin-eosin, x400). |
Discussion
GF is a rare chronic inflammatory skin disease clinically. Although some features of the lesions in GF may be helpful for clinical diagnosis, especially the presence of reddish brown (possibly attributed to hemosiderin deposition), the final diagnosis is confirmed through skin biopsy. The pathological characteristics of GF are leukocytoclastic vasculitis, accompanied by mixed inflammatory cell infiltration of neutrophils, lymphocytes, eosinophils, and other inflammatory cells around the blood vessels. A narrow non-infiltration zone (Grenz zone) can be seen between the epidermis and dermis. It is worth mentioning that these features may not necessarily exist.7 Clinically, it should be differentiated from sarcoidosis, discoid lupus erythematosus, and rosacea.8 The pathogenesis of GF is still unclear, and some patients do not respond to conventional treatments. Therefore, this poses certain challenges for the treatment of it.
Existing reported effective treatment schemes include topical corticosteroid and calcineurin inhibitors, systematic application of dapsone, hydroxychloroquine, clofazimine and colchicines, etc. Laser, cryotherapy, and surgery have also been reported. However, the treatment of GF still faces difficulties, and different patients have different reactions to treatment methods. Lindhaus et al carried out a systematic review on the treatment of GF, and a total of 94 patients were retrieved. Topical or injected corticosteroid are commonly used, but 42% of people have no effect. Attention should be paid to the problem of skin atrophy. External tacrolimus seems to be a good treatment option, and all patients have shown good results. The results of oral dapsone treatment also vary, and it is important to be vigilant about the side effects of the drug.
Minocycline can exert anti-inflammatory effects in different diseases by inhibiting various immune cells, downregulating the migration of neutrophils across endothelium mediated by the vascular intercellular adhesion molecule-1/ICAM-1 pathway, inhibiting neutrophil chemotaxis, and alleviating tissue damage.9 Our patient had a short course of disease, with a large number of neutrophils infiltrated pathologically and the vascular wall swollen. He also had poor response to external drugs. In view of this, considering the anti-inflammatory and anti neutrophil chemotaxis effects of minocycline, we gave the patient minocycline orally and achieved particularly ideal results. After 3 weeks of treatment, the patient’s lesions had significantly improved, and the treatment effect was also satisfactory. During the treatment process, the patient did not experience any discomfort. However, due to the possibility of recurrence of GF, follow-up of the patient is still necessary after the lesions subsided. Notwithstanding the promising results so far, long-term follow-up is required to verify the efficacy of this therapy. This paper has certain limitations. Since there is only one patient, the effectiveness of minocycline in treating GF needs more samples to be confirmed.
Conlusion
Due to the low incidence rate of GF, most of the treatment experiences of GF come from case reports and case series. This case provides an alternative method for the treatment of GF. To our knowledge, this is the first case report of minocycline successfully treating facial granuloma.
Consent Statements
Written informed consent was provided by the patient to have the case details and accompanying images published. Institutional approval was not required to publish the case details.
Funding
There is no funding to report.
Disclosure
No potential conflict of interest was reported by the author(s).
References
1. Marcoval J, Moreno A, Peyr J. Granuloma faciale: a clinico-pathological study of 11 cases. J Am Acad Dermatol. 2004;51:269–273. doi:10.1016/j.jaad.2003.11.071
2. Barnadas MA, Curell R, Alomar A. Direct immunofluorescence in granuloma faciale: a case report and review of literature. J Cutan Pathol. 2006;33(7):508–511. doi:10.1111/j.1600-0560.2006.00451.x
3. Loi C, Abbenante D, Misciali C, et al. Extrafacial granuloma faciale presenting as an annular plaque of the scalp. Int J Dermatol. 2022;61(4):e144–e6. doi:10.1111/ijd.15778
4. Gil FS, Parente J, Aranha J. Resolution of granuloma faciale with topical tacrolimus. Int J Dermatol. 2020;59(2):e29–e31. doi:10.1111/ijd.14664
5. Alsorori E, Kiss N, Medvecz M, et al. A case of granuloma faciale successfully treated with systemic dapsone. Dermatol Ther. 2020;33(1):e13162. doi:10.1111/dth.13162
6. Lindhaus C, Elsner P. Granuloma Faciale Treatment: a Systematic Review. Acta Derm Venereol. 2018;98(1):14–18. doi:10.2340/00015555-2784
7. Ortonne N, Wechsler J, Bagot M, et al. Granuloma faciale: a clinicopathologic study of 66 patients. J Am Acad Dermatol. 2005;53:1002–1009. doi:10.1016/j.jaad.2005.08.021
8. Ludwig E, Allam JP, Bieber T, et al. New treatment modalities for granuloma faciale. Br J Dermatol. 2003;149(3):634–637. doi:10.1046/j.1365-2133.2003.05550.x
9. Parenti A, Indorato B, Paccosi S. Minocycline affects human neutrophil respiratory burst and transendothelial migration. Inflamm Res. 2017;66(2):107–109. doi:10.1007/s00011-016-0999-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.