")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
A Case of Eosinophilic Pustular Folliculitis Misdiagnosed as Eczema
Authors Li Y , Yang X, Lu J, Chen K, Wu W , Zhang M, Li W
Received 20 October 2023
Accepted for publication 18 January 2024
Published 24 January 2024 Volume 2024:17 Pages 199—204
DOI https://doi.org/10.2147/CCID.S445760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Yuan Li,1,2 Xianxu Yang,3 Jiejie Lu,1 Kai Chen,3 Weiwei Wu,3 Ming Zhang,3 Wanni Li1
1Department of Cosmetic Dermatology, The Fifth People’s Hospital of Hainan Province, Haikou, Hainan, People’s Republic of China; 2Department of Dermatology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 3Department of Dermatology, The Fifth People’s Hospital of Hainan Province, Haikou, Hainan, People’s Republic of China
Correspondence: Wanni Li, Department of Cosmetic Dermatology, The Fifth People’s Hospital of Hainan Province, No. 8 Longhua Road, Longhua District, Haikou, 570100, Hainan, People’s Republic of China, Email [email protected]
Abstract: Eosinophilic pustular folliculitis (EPF) is a rare skin disease. The typical skin lesions of classic EPF are localized on the upper limbs’ face, trunk, and extensor surfaces. However, when the skin lesions initially appear on the palms and soles, it is not easy to diagnose as EPF. Here, we report a case of a male patient who presented with erythematous plaques, pustules, and crusted erosions on the hands and feet, which were misdiagnosed as eczema ten years ago. Over ten years, the patient experienced recurrent erythematous patches with bumps and itching on the face, trunk, and extremities after improving the hand and foot lesions. A histopathological biopsy was performed to establish a definitive diagnosis, revealing pustules formed by eosinophilic infiltrates within the hair follicles. The diagnosis was confirmed as eosinophilic pustular folliculitis. The patient was treated with oral indomethacin at a dosage of 75mg/day, resulting in the disappearance of the skin lesions. After a 3-month follow-up, no recurrence was observed.
Keywords: eosinophilic pustular folliculitis, indomethacin
Introduction
Eosinophilic pustular folliculitis (EPF) was initially identified by Ofuji in 1970.1 This condition is characterized by recurrent clusters of aseptic papules and pustules situated on circumscribed red plaques. These lesions are typically pruritic and often coincide with peripheral blood eosinophilia. Predominantly affecting the face, trunk, and extremities, EPF is commonly found in seborrheic skin areas and occasionally on the palmoplantar region.2 Despite the absence of hair follicles in the palmoplantar area, EPF may still manifest in this region. Aoyama and Tagami conducted a comprehensive review of 207 EPF cases from Japanese literature, revealing that 38 cases (18%) exhibited palmoplantar lesions. Among these, 16 cases (8%) initially presented with lesions on the palmoplantar area, later extending to other areas after an average of 26 months.3 Notably, none of these cases received an initial EPF diagnosis when the lesions were confined solely to the palmoplantar region. Consequently, when pustules emerge on the palmoplantar region, it is crucial to consider the potential presence of EPF, in addition to palmoplantar pustulosis. While instances of EPF solely involving the palmoplantar area are scarcely documented in the literature, we present a case in which eosinophilic pustular folliculitis initially manifested on the palms of both hands. In the early stages, the lesions were erroneously diagnosed as “eczema”.
Clinical Presentation
The patient, a male, 35 years old, has been experiencing recurrent erythematous patches with bumps and itching on the face, trunk, hands, and feet for ten years, with a recent onset of 1 month. Ten years ago, the patient initially presented with erythematous plaques, pustules, crusted erosions, exudation, and crusted scabs on the hands and feet, accompanied by mild itching. The patient was diagnosed at an external clinic with 1) eczema and 2) skin infection and was treated with oral prednisone 30mg/day, oral cefradine, and topical corticosteroid cream, which resulted in symptom improvement. However, over ten years after the hand and foot rash resolution, the patient experienced recurrent erythematous patches, plaques, and bumps on the face, neck, back, hands, and feet, accompanied by mild itching. Multiple visits to external clinics resulted in a diagnosis of “generalized eczema” and treatment with topical corticosteroids, oral doxycycline, and topical corticosteroid ointment, which provided temporary relief but led to relapses shortly after discontinuation. One month ago, the symptoms recurred with extensive erythematous patches, plaques, and bumps on the face, neck, back, and hands and feet, mild itching, facial swelling, without fever, joint pain, cough, sputum, abdominal pain, or diarrhea. The patient had not received any treatment and sought further medical attention at our hospital, where a preliminary diagnosis of generalized eczema was made. Treatment was initiated with Tripterygium wilfordii glycosides 20mg, three times a day; levocetirizine tablets 5mg, once a day; ketotifen tablets 1mg, once every evening; and compound glycyrrhizin tablets 50mg, three times a day. After one week of oral medication, there was no improvement, leading to the patient’s admission to the hospital. The patient has no significant medical history, family history, or history of marriage and childbirth. The patient denies any drug allergies.
Physical examination showed good general condition and no abnormalities in the heart, lungs, and abdomen. Dermatologic examination showed large infiltrative erythema and swollen plaques with indistinct margins on both cheeks of the face, irregular erythema with scattered pinhead-sized bumps on the neck, and indistinct erythema with pinhead-sized pimples on the back, some of which were semi-annular in shape. Diffuse erythematous desquamation is observed on the hands and feet, with scattered pinpoint-sized pustules (Figure 1A–F). Laboratory tests showed routine blood: leukocytes: 10.2×109/L, eosinophils: 1.36×109/L (0.02–0.5×109/L), eosinophil ratio: 13.3% (0.5–5%), total IgE, syphilis three, HIV antibodies, liver and kidney function, electrolytes, blood glucose, lipids did not show significant abnormalities. Fungal microscopy of the facial erythema reveals a small number of spores, while fungal microscopy of the buttocks, hands, and feet is negative. Chest CT scan shows no abnormalities. Skin biopsy of the back erythema reveals mild edema of the epidermal keratinocytes, abundant eosinophilic infiltration with a small number of neutrophils and lymphocytes around the hair follicles and sebaceous glands in the dermis, pustule formation with eosinophilic infiltrates within the hair follicles, and a small amount of inflammatory cell infiltration around the superficial dermal blood vessels (Figure 2A and B). Acid-fast staining is negative. Based on the above findings, the diagnosis is eosinophilic pustular folliculitis (classic type). After discharge, the patient is treated with oral indomethacin 75mg/day. After ten days of treatment, the erythematous patches on the face, neck, and trunk mostly disappear, the pustules dry up, and a small number of adherent scales are observed (Figure 3A–D). Follow-up, peripheral blood eosinophil count returns to normal. The patient continues to take oral indomethacin 75mg/day, and after one month of treatment, the symptoms subside. Medication is stopped, and no recurrence is observed during a 3-month follow-up.
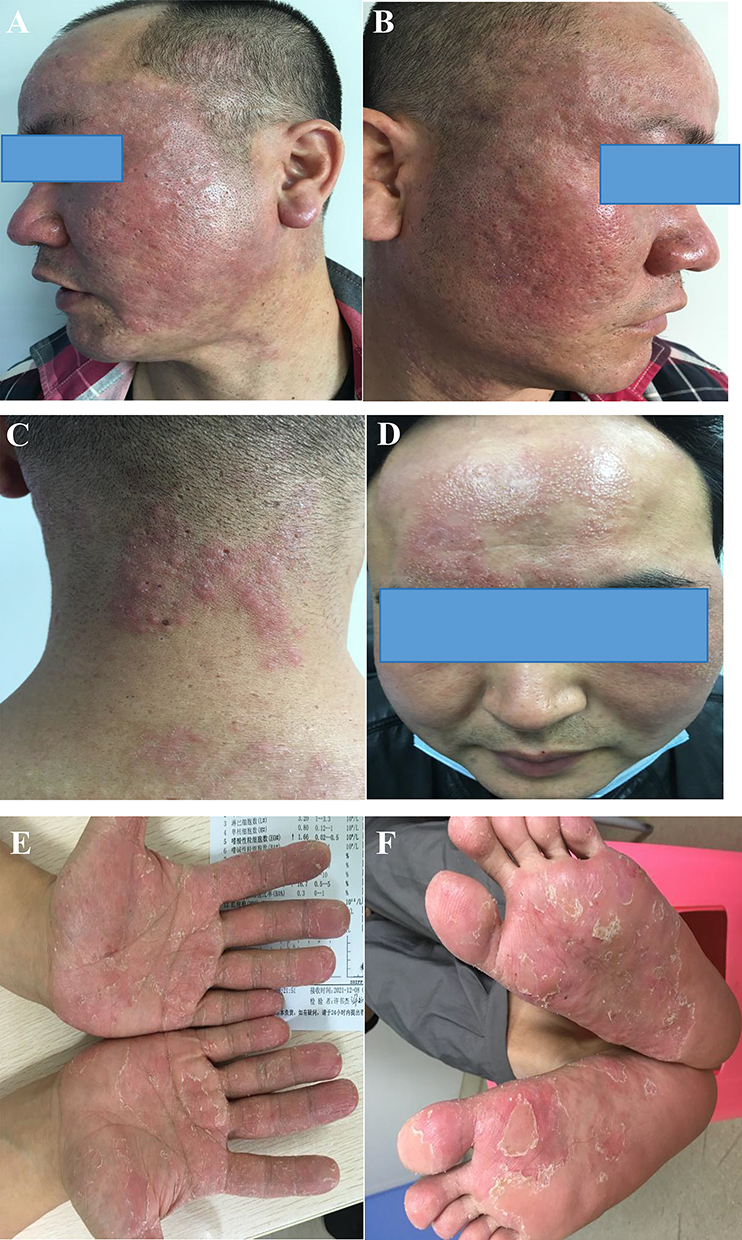 |
Figure 1 (A and B) Large infiltrative erythematous and swollen plaques with indistinct margins are seen on the face; (C) irregular erythematous plaques with scattered pinhead-sized pustules on the neck; (D) indistinct erythematous plaques with pinhead-sized pustules on some of the erythematous plaques are seen on the back, and some of the erythematous plaques are semi-annular in shape. (E and F) Diffuse erythematous desquamation with scattered pinhead-sized pustules overlying both hands and feet. |
 |
Figure 2 (A) Mild edema of epidermal acanthocytes and a large number of eosinophils and a small number of neutrophil lymphocyte-dominated infiltrates around the hair follicle sebaceous gland in the dermis (HE×200x) (B) Eosinophil-formed abscess in the hair follicle and a small number of inflammatory cell infiltrates around the superficial dermal vessels (HE×400). |
 |
Figure 3 (A–D) Largely disappeared skin lesions on the back of the face and neck. |
Discussion
Eosinophilic pustular folliculitis (EPF) is classified into classic type, immunosuppression-related type, and infantile type.4 The classic type is commonly seen in Japanese individuals, with an average onset age of 35–40 years and a male-to-female ratio of 2.64:1. The immunosuppression-related type is less common. It is mainly associated with HIV infection, hematological malignancies, or other tumors. The infantile type mostly occurs in children under one year old, with a higher prevalence in male infants, and 70% of patients develop symptoms within six months after birth.5,6 The etiology and pathogenesis of this disease are not yet fully understood. It has been reported that EPF can be associated with human immunodeficiency virus, autoimmune diseases, and autologous peripheral blood stem cell and allogeneic bone marrow stem cell transplantation.7 Some researchers believe that the occurrence of EPF is a hypersensitive reaction of the body to external antigens. Studies have suggested a relationship between classic EPF and sebum overproduction and sex hormones, while others propose an abnormal response to saprophytic microorganisms.8 The typical skin lesions of classic EPF are localized on the upper limbs’ face, trunk, and extensor surfaces. They present as pruritic annular or serpiginous plaques with follicular papules and pustules, expanding outward while regressing centrally.9 An analysis of 207 reported cases of EPF in Japanese literature found that 38 cases (18%) had involvement of the palms and soles, with 16 cases (8%) showing initial lesions in these areas, followed by involvement of other sites an average of 26 months later. None of the cases with isolated involvement of the palms and soles were diagnosed as EPF.3 We hypothesize that the previous lesions on the patient’s extremities were probably the initial manifestation of the disease, which was misdiagnosed as “eczema” without histopathological biopsy and resolved with corticosteroids. Zhang Huifeng reported a rare case of EPF occurring on the palms, confirmed by skin biopsy in China.10
Patients generally present with mild pruritus or no itching, although the infantile and HIV-related types can manifest with severe itching. Laboratory examinations often show mild leukocytosis and varying degrees of eosinophilia since the pustules in patients are formed by the accumulation of eosinophils. Therefore, bacterial cultures from the pus are usually negative.11,12 Skin histopathological examination reveals mild intercellular edema of the epidermal keratinocytes, edema between the epithelial cells of the hair follicles, significant infiltration of eosinophils around the hair follicles and sebaceous glands, formation of eosinophilic abscesses within the follicles, and infiltration of other cells such as neutrophils and monocytes. Inflammatory cell infiltration is observed around the dermal blood vessels.13 The histopathological findings, in this case, are highly consistent with the changes seen in eosinophilic pustular folliculitis.
In clinical practice, it is important to differentiate this disease from conditions such as annular pustular psoriasis, acne, tinea corporis, and rosacea.14 Pathologically, it should be distinguished from facial eosinophilic granuloma, follicular mucinosis, and follicular tufted granuloma.15 Annular pustular psoriasis presents as circular erythema with larger and more numerous pustules, rapid progression, and the formation of abscesses or pus lakes, accompanied by fever and increased neutrophils as severe complications.15,16 Acne is characterized by the presence of comedones and the absence of inflammatory plaques.15,16 Tinea corporis manifests as scaly papules that can merge into annular or semicircular shapes with positive fungal tests.15,16 Rosacea primarily has a burning sensation, and the skin lesions are not annular.15,16 Facial granuloma often appears as single or multiple asymptomatic brownish-red to purplish plaques with fewer pustules. Histologically, there may or may not be an infiltrative zone in the superficial epidermis, predominantly composed of eosinophils and mixed inflammatory cells, possibly accompanied by vasculitis changes. The infiltration does not center around the hair follicles.15,16 In follicular mucinosis and tufted granuloma, abundant mucin deposition can be observed within the hair follicles, showing positive staining with alcian blue.15,16
The etiology of eosinophilic folliculitis remains unclear, potentially linked to immune system abnormalities.15,16 It is characterized by red papules around hair follicles, accompanied by small papules. Histopathologically, perifollicular eosinophilic infiltration is observed. In contrast, mycosis fungoides, primarily caused by fungal infections, can affect the skin, nails, and hair, presenting as erythema, desquamation, and itching. Histopathological findings may include the presence of fungi. Notably, histopathologic differences exist between follicular mucinosis and eosinophilic folliculitis in mycosis fungoides. Follicular mucinosis entails mucus deposition around the hair follicle, forming a mucus sac, accompanied by mild lymphocytic infiltrate. In eosinophilic folliculitis, an inflammatory disease, histopathologic features predominantly display perifollicular eosinophilic infiltrate, characterized by leukocytes with a high number of eosinophilic granules in their cytoplasm.15,16 Therefore, analyzing histopathologic features aids in distinguishing between these two diseases.
There are several treatment options for this condition. The first-line treatment drug is indomethacin, while second-line treatments include corticosteroids, tetracycline, colchicine, retinoids (such as isotretinoin), tacrolimus, salicylic acid, and ultraviolet irradiation. Among them, tetracycline-class drugs (minocycline or doxycycline) are considered second-line treatments for classical EPF.17 Considering that the patient had been using doxycycline and corticosteroids repeatedly for a long time, and the condition had recurred, after the pathological diagnosis, the patient was switched to treatment with indomethacin (75mg/day), commonly known as Xiaofentong, for one month, which showed good results. Nakahigashi suggested that prostaglandin D2 can stimulate sebaceous gland cells to produce chemotactic factor-3, which attracts eosinophils to the perifollicular region of the sebaceous gland. Indomethacin, on the other hand, inhibits the cyclooxygenase in sebaceous cells, reducing the production of prostaglandin D2 and eosinophil-activating chemotactic factor-3, thereby exerting a therapeutic effect through interaction with prostaglandin D2 receptors.18 In addition, there have been reports from Japan on using traditional Chinese medicine, Chaihu Lingtang, to treat eosinophilic pustular folliculitis. Chaihu Lingtang has immunosuppressive and corticosteroid-like effects and is widely used in allergic and autoimmune diseases. It is worth considering and learning from traditional Chinese medicine practitioners.17
Ethics Statement
The publications of images were included in the patient’s consent for publication of the case. The Hospital Ethics Committees of the Fifth People’s Hospital of Hainan Province approved to publish the case details.
Consent Statement
Informed consent was provided by the patient for publication of the case.
Funding
This project is supported by Hainan Province Clinical Medical Center.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Ofuji S, Ogino A, Horio T, Oseko T, Uehara M. Eosinophilic pustular folliculitis. Acta Derm Venereol. 1970;50(3):195–203.
2. Dodia P, Cook C. Eosinophilic Pustular Folliculitis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
3. Aoyama H, Tagami H. Eosinophilic pustular folliculitis starting initially only with palmoplantar pustular lesions. Report of a case and review of the literature. Dermatology. 1992;185(4):276–280. doi:10.1159/000247468
4. Shi W, Lu Y, Zhou F, He H, Jiang J, Xue X. Infantile eosinophilic pustular folliculitis in a child aged 7 years: a case report. Clin Cosmet Invest Dermatol. 2023;16:717–720. doi:10.2147/CCID.S404316
5. Li Y, Nie R, Cao X, Wan C. Classic eosinophilic pustular folliculitis in an immunocompetent patient with syphilis: are they related? Clin Cosmet Invest Dermatol. 2023;16:67–70. doi:10.2147/CCID.S393841
6. Umegaki-Arao N, Tanemoto S, Tanese K, et al. Eosinophilic pustular folliculitis with palmoplantar lesions and nail deformity. J Dermatol. 2020;47(10):e357–e359. doi:10.1111/1346-8138.15503
7. Marzano AV, Genovese G. Eosinophilic dermatoses: recognition and management. Am J Clin Dermatol. 2020;21(4):525–539. doi:10.1007/s40257-020-00520-4
8. Ichimura R, Kamiya K, Komine M, et al. Possible interaction between eosinophils and other immune cells in the pathomechanism of eosinophilic pustular folliculitis. Int J Dermatol. 2022;61(12):e499–e501. doi:10.1111/ijd.16203
9. Monastirli A, Antoniades G, Kapranos N, Pasmatzi E, Badavanis G, Tsambaos D. Classic form of eosinophilic pustular folliculitis in an immunocompetent girl: rapid and complete resolution after low-dose oral indomethacin treatment. Dermatol Online J. 2017;23(11):
10. Huifeng Z, Shixiang Z, Min G, et al. A case of eosinophilic pustular folliculitis specifically on the palm of the hand. Chin J Dermatol Venereol. 2012;26(05):432–433.
11. Guo W, Qian G, Zhang C. Eosinophilic pustular folliculitis of infancy. Arch Dis Child Fetal Neonatal Ed. 2022;21:323930. doi:10.1136/archdischild-2022-323930
12. Kanaki T, Hadaschik E, Esser S, Sammet S. Eosinophilic pustular folliculitis (EPF) in a patient with HIV infection. Infection. 2021;49(4):799–801. doi:10.1007/s15010-020-01543-z
13. Fertitta L, Bodemer C, Molina T, Frassati-Biaggi A, Fraitag S, Leclerc-Mercier S. Eosinophilic pustular folliculitis of infancy: a histologic assessment of 43 cases. Am J Dermatopathol. 2022;44(6):395–403. doi:10.1097/DAD.0000000000002006
14. Katoh M, Nomura T, Miyachi Y, Kabashima K. Eosinophilic pustular folliculitis: a review of the Japanese published works. J Dermatol. 2013;40(1):15–20. doi:10.1111/1346-8138.12008
15. Fujiyama T, Tokura Y. Clinical and histopathological differential diagnosis of eosinophilic pustular folliculitis. J Dermatol. 2013;40(6):419–423. doi:10.1111/1346-8138.12125
16. Nomura T, Katoh M, Yamamoto Y, Miyachi Y, Kabashima K. Eosinophilic pustular folliculitis: a proposal of diagnostic and therapeutic algorithms. J Dermatol. 2016;43(11):1301–1306. doi:10.1111/1346-8138.13359
17. Nomura T, Katoh M, Yamamoto Y, Miyachi Y, Kabashima K. Eosinophilic pustular folliculitis: a published work-based comprehensive analysis of therapeutic responsiveness. J Dermatol. 2016;43(8):919–927. doi:10.1111/1346-8138.13287
18. Nakahigashi K, Doi H, Otsuka A, et al. PGD2 induces eotaxin-3 via PPARγ from sebocytes: a possible pathogenesis of eosinophilic pustular folliculitis. J Allergy Clin Immunol. 2012;129(2):536–543. doi:10.1016/j.jaci.2011.11.034
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.