")
Back to Journals » International Medical Case Reports Journal » Volume 16
A Case of ALK-Positive Anaplastic Large Cell Lymphoma of the Male Breast
Authors Wang X, Jia Z, Li J, Yang H, Sun X, Liu Y
Received 12 August 2023
Accepted for publication 2 November 2023
Published 17 November 2023 Volume 2023:16 Pages 747—755
DOI https://doi.org/10.2147/IMCRJ.S434109
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Xu Wang, Zhanli Jia, Jinze Li, Huichai Yang, Xuemei Sun, Yueping Liu
Department of Pathology, the Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050011, People’s Republic of China
Correspondence: Xu Wang; Yueping Liu, Department of Pathology, the Fourth Hospital of Hebei Medical University, No. 12 Jiankang Road, Shijiazhuang, Hebei, 050011, People’s Republic of China, Email [email protected]; [email protected]
Background: Primary breast lymphoma (PBL) is a very rare form of non-Hodgkin’s lymphoma (NHL). A primary T-cell lymphoma in the breast with no previously identified lymphomatous lesions is an even rarer form of this malignancy.
Case Presentation: A biopsy of a breast mass in a 60-year-old Caucasian man showed a morphologic-immunophenotypic profile with features characteristic of an ALK-positive (AKT+), anaplastic large cell lymphoma. Fluorescence in situ hybridization (FISH) analysis of fixed, paraffin-embedded tissue of this lesion was performed at our institution for IRF4/DUSP22 gene rearrangement. No rearrangement was detected. The patient presented with mutations in the following genes; BCOR_p.Q600X, DNMT3A_p.F609fs, NOTCH1_p.P2320fs, and IDH2_p.R140Q. However, the patient’s consultation was complicated by the fact that he had been diagnosed with breast cancer at a local hospital and had come to our institution for further consultation. The histology findings were confirmed by immunohistochemistry and FISH. Computed tomography and positron emission tomography did not reveal nodules elsewhere in the body, which allowed the staging of the patient to be completed. However, although the patient had previously received the chemotherapy CCOP regimen (ie, cyclophosphamide, vincristine, prednisolone acetate) he did not go into remission in a timely manner and relapsed after six months, followed by a drastic deterioration in his condition after four months, resulting in his death in less than one month.
Conclusion: This report of a male patient describes a case of a rare T-cell lymphoma of the breast that occurs considerably more frequently in female patients. The differential diagnosis of the histology of this tumor showed mutations that occur more often in lymphoblastic lymphoma or leukemia. This rare malignancy and associated mutations led to the death of this patient during treatment.
Keywords: tumors, lymphopoietic system, male breast, diagnostic histopathology, misdiagnosis
Background
Primary breast lymphoma (PBL) is extremely rare, accounting for approximately 0.5% of all primary breast malignancies. More than 95% of patients with a PBL are women, with only a very small number of cases reported in men, mainly in those aged between 40–70 years.1,2 While male breast lymphoma is extremely rare, cases of non-Hodgkin’s T-cell lymphoma are more unusual and even rarer. To date, only a few cases of male breast lymphoma have been reported in the literature, with most being B-cell lymphomas and not T-cell lymphomas. Anaplastic large cell lymphomas (ALCLs) occur more frequently in young women with breast grafts, especially in those with breast augmentation. The clinical presentation of male breast lymphoma is usually similar to that of more common carcinomas. In this regard, the case reported in this paper represents a misdiagnosis.
Previous clinical and pathologic features of male breast lymphoma on mammography have shown a single, well-circumscribed painless mass and/or an enlarged usually unilateral ipsilateral axillary lymph node.3–9 To our knowledge, there are only a few reports that have described genetic alterations in male breast lymphoma. In a previous retrospective study, we analyzed breast lymphomas and identified a specific case of an anaplastic large-cell lymphoma in a male patient.4–6 Histologically, the hallmark cells are very large, with abundant cytoplasm, some of which are hyaline and some either eosinophilic or basophilic. The nuclei are darkly stained and highly irregular in shape with a wreath, horseshoe, or renal pattern, some of which resemble a Reed-Sternberg pattern, typical of a hallmark cell, with scattered nuclei and small basophilic nucleoli.
Case Presentation
A 60-year-old male patient complained of a painless mass under the nipple for more than four months. No pain, itching or nipple discharge were noted. The patient had no history of cancer and no specific family history but felt that the tumor was growing. Further immunohistochemistry investigations were recommended because a diagnosis of an invasive breast carcinoma does not exclude breast polymorphic invasive lobular carcinoma or cancer with syngenetic differentiation. The results of these investigations showed that ER, PR, HER2, E-cadherin, P120, CK5/6, and P40 were all negative, although a high expression of Ki-67 was noted. The results obtained from the local hospital that initially treated the patient showed that these immunohistochemistry results were not specific to the liquid obtained from the biopsy, with histological analysis revealing an aggressive cancer morphology. Following intradepartmental consultation, the patient was diagnosed with a highly aggressive breast cancer consistent with a triple-negative breast lesion. The patient decided to receive a new adjuvant treatment, although his relatives complained and asked for further treatment options as there were no other obvious symptoms due to the patient’s preexisting health conditions. This led to the patient seeking treatment at our hospital. An ultrasound examination carried out on admission showed that the larger gland was located below the nipple and measured 4.4 cm x 4.4 cm x 1.4 cm. Striped blood flow signals were observed in the region, with low echoes seen in the shallow fat layer measuring 1.1 cm x 0.5 cm. The results of real-time shear wave elastography are shown in Figure 1. The integrated ultrasound diagnosis based on the mammography reports and data systems (BI-RADS) was a type 4C right breast parenchymal occupying lesion.
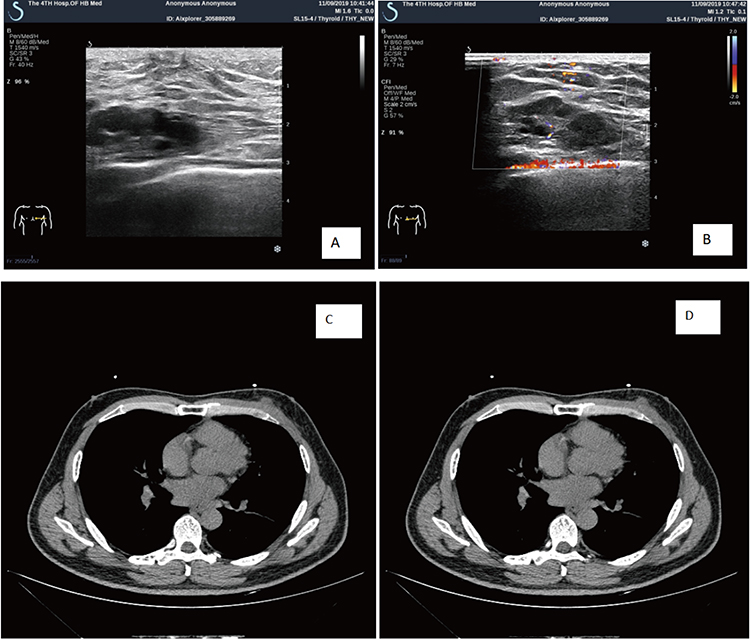 |
Figure 1 Ultrasound examination: (A) Small echoes of glands were observed deep in the right nipple. The larger lesion was located below the nipple and measured 4.4 cm x 4.4 cm x 1.4 cm. (B) Striped blood flow signals were observed in the region, while low echoes were observed in the shallow fat layer. (C and D) CT results showed a significant reduction of the tumor after treatment and the tumor was not obvious based on the mediastinum imaging results. |
Only a small number of tumor tissue biopsy samples were obtained for histology. Light microscopy showed a greater number of tumor cells and reduced stroma. The tumor cells were linear or trabecular, with some areas being monoline. The local lesions harbored a mixture of cells, with the tumor cells being large and containing fine chromatin and multiple mitotic images. The tumor cells exhibited deep staining and were disproportionate in size. As shown in Figures 2A-D, necrosis and bleeding were not observed. The results of the immunohistochemistry investigations were as follows: AE1/AE3 (-), EMA (+), S-100 (-), CD68 (-), CD3 (weak+), CD20 (-), Pax5 (-), CD30 (+), Bcl-2 (-), CD2l (-), CD23 (-), Bcl-6 (-), MUM1 (+), CD2 (-), CD4 (+), CD8 (-), CD5 (-), CD7 (-), TIA-1 (-), GrB (+), ALK (+), CD56 (-), EBER (-), and Ki-67 (70%+). Based on the above results the pathologic diagnosis was non-Hodgkin’s anaplastic large cell lymphoma in the right breast, ALK-positive (Figures 3A-F).
 |
Figure 2 (A) A small number of tumor tissue biopsies were obtained, with more tumor cells and reduced stroma observed by light microscopy. (B) The tumor cells were linear or trabecular, and some areas were monoline. (C) The local lesions included a mixture of cells. (D) The tumor cells were large with fine chromatin and multiple mitotic images. The cells also exhibited deep staining and were disproportionate in size, with no necrosis or bleeding being observed. |
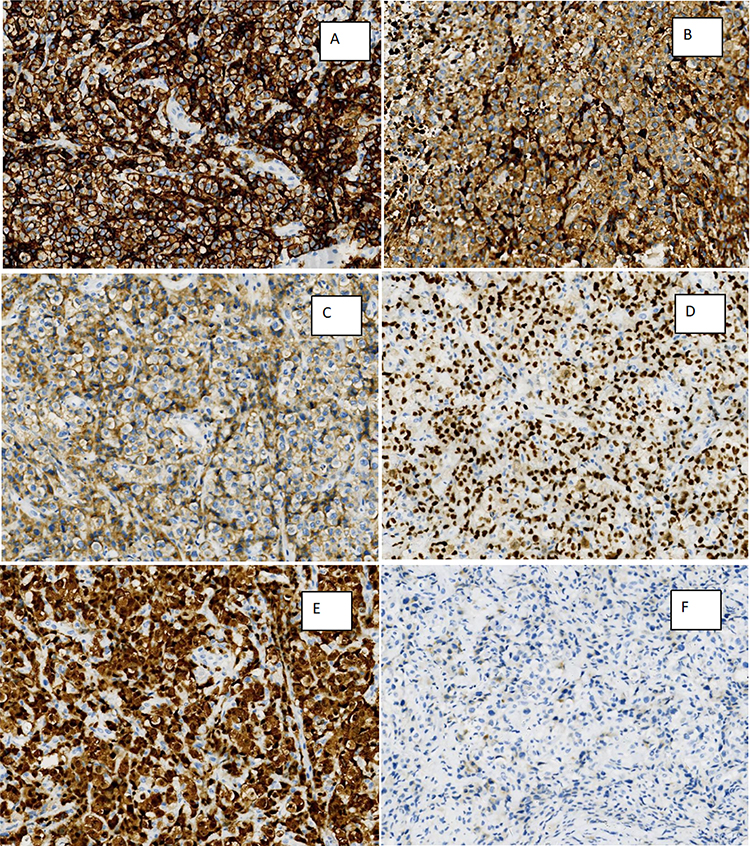 |
Figure 3 All the stains were obtained using the MaxVision method (A) The CD30 results showing diffuse positive cells; (B) GrB outline of a positive cell membrane; (C) diffuse CD4 cell membrane staining; (D) MUM1 staining showing negative staining of the tumor cell nuclei; (E) ALK staining showing positive diffuse staining of the cells; (F) EMA staining showing weakly positive staining of the tumor cells. |
Interphase fluorescence in situ hybridization (FISH) analyses were then performed using the two-color fusion probes IRF4 and DUPS22, obtained from Ambipycin Pharmaceuticals Co., Ltd., Guangzhou, China. Where possible, at least 100 nuclei were evaluated for each probe. The FISH analyses were evaluated and recorded using ISIS Digital Image Analysis version 5.0 (MetaSystems, Altusheim, Australia). To analyze the whole genome for imbalance, DNA was extracted from the FFPE material using the QIAmp DNA FFPE tissue kit (Qiagen, Lab Division, America) and processed using the Oncoscan™ FFPE express 3.0 kit (Affymetrix, Santa Clara, CA, USA). Processing involved analysis of copy number aberrations (CNA) and constructing copy TuScan algorithms using Nexus Express for Oncoscan 3 software (Beijing Yuxin Biotechnology Co., China). The human reference genome GRCh37/hg19 was used for gains and deletions smaller than 100 Kb or containing less than 20 probes, and CNN-LOH for those smaller than 5000 Kb or containing deletion regions not considered in the analyses. Molecular cytogenetic analysis using interphase fluorescence in situ hybridization (FISH) analysis showed that the vast majority of cells in the tissue sections had chromosomal breakpoints that affected the fusion of the IRF4 motif and DUPS22, and chromosomal breakpoints that affected the DUPS22 motif. We also detected an additional signal for the nonrecombinant allele, suggesting a gain in the DUPS22 locus (Figure 4B). In addition, we observed a gain in the IRF4 locus without breaks. Based on these results and with reference to the current classification of lymphoma of the World Health Organization (WHO), we changed the diagnosis to “non-Hodgkin’s mesenchymal metaplastic large cell lymphoma, ALK-positive”. This malignancy was not associated with an IRF4/DUPS22 rearrangement. Chromosomal imbalance mapping using the Oncoscan™ Chromosomal Imbalance Mapping platform revealed mutations in the following genes: BCOR_p.Q600X, DNMT3A_p.F609fs, NOTCH1_p.P2320fs, and IDH2_p.R140Q (Figure 4A). Finally, we attempted to sequence the whole exome of the tumor, although unfortunately, this failed due to technical reasons.
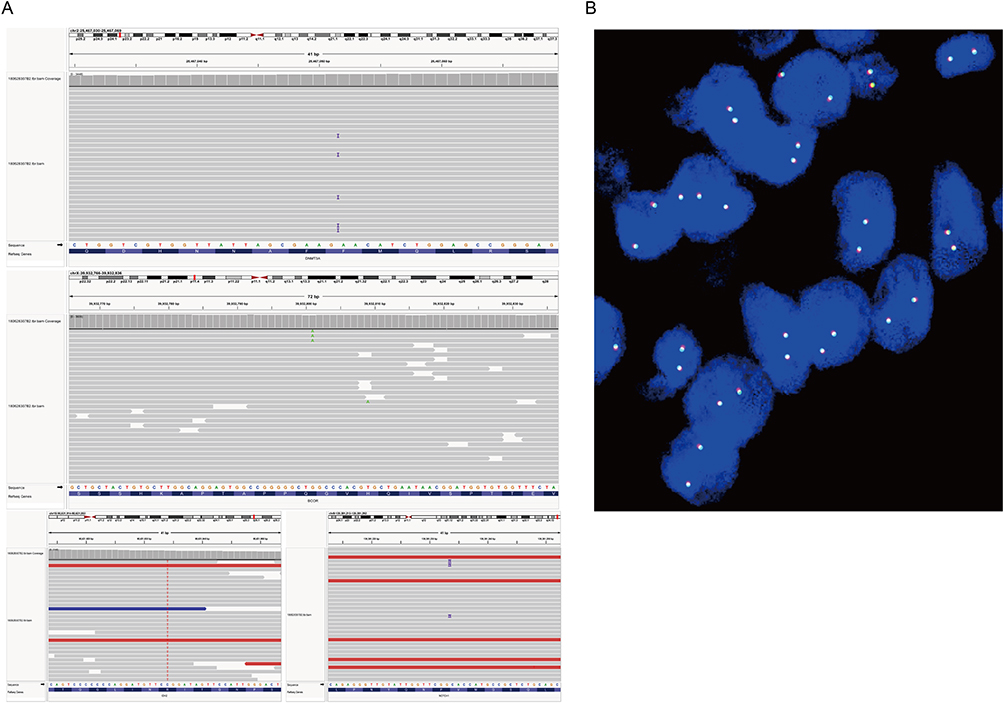 |
Figure 4 (A) BCOR_p.Q600X, DNMT3A_p.F609fs, NOTCH1_p.P2320fs, IDH2_p.R140Q gene mutations; (B) The tumor was not associated with IRF4/DUPS22 rearrangement. |
Discussion
Breast lymphoma is a rare form of non-Hodgkin’s lymphoma with an incidence of 0.4%-0.7% and is classified either as a PBL or secondary breast lymphoma (SBL).1 The incidence of PBLs is lower at 0.04% −1.10% compared with 1.7% to 2.2% for extra nodular lymphomas. The majority of PBL cases (97% to 99%) are diagnosed in women, with the most common pathologic type being non-Hodgkin diffuse large B-cell lymphoma (DLBCL).2 Non-Hodgkin anaplastic large cell lymphomas are extremely rare.3,4 The etiological role and pathogenesis of estrogen in this disease are unknown, although several papers have reported an association with estrogen levels.5 In particular, male patients receiving hormone therapy for prostate cancer experience a disbalance between estrogen and androgen levels, which is also a marker of uneven breast development in some men. PBL presents clinically as a single active breast nodule or lobular mass, with most patients reporting no obvious pain or only mild tenderness. Rapid development of these nodules or masses is associated with a poor prognosis.6–8 At present, imaging examinations for PBL mainly involve ultrasound. The present case needs to be distinguished from breast cancer, which is characterized by an irregular hypoechoic region, often accompanied by calcification and burrs, and can be accompanied by sound dizziness or “crab-like” changes.9 Only four cases of primary lymphoma of the male breast have been reported in the literature.8–11 A recent large Phase II cohort study10,11 showed that women treated with estrogen had a 29% greater risk of developing NHL (excluding PBL) than women who had never received such treatment. One report described ER positivity in PBL, whereas other reports showed the opposite result.12,13
The differential diagnosis of PBL includes the following cellular characteristics. (1) Invasive pleomorphic lobular carcinoma of the breast. The cancer cells are large and pleomorphic and express CK, EMA, P120, but not E-cadherin, CD30, and ALK. (2) Invasive breast cancer, pleomorphic type of non-special type. Extensive cell polymorphism, cell and nucleus enlargement, and cell strangeness. The cancer cells express CK, EMA, p120, E-cadherin, but not ALK and CD30. (3) Diffuse large B-cell lymphoma - anaplastic subtype. The tumor cells have large nuclei and are strangely polymorphic, with some being similar to RS or ALCL cells. Most cells express CD30 but may also express CD20, CD79a, PAX5, and other B-cell markers. (4) ALK-positive large B-cell lymphoma. The tumor cells are large with a single form of diffuse hyperplasia and express ALK and EMA, but not CD30. (5) Pleomorphic rhabdomyosarcoma. The cell morphology is polymorphic, and cytoplasmic eosinophilic rhabdomyosarcoma can be seen. The cells express desmin, MyoD1, myogenin, and other myogenic markers. (6) Primary ALCL in the skin. The tumor mainly involves the dermis, although pro-epidermal infiltration can be seen. Most tumor cells have an alloplastic form, with > 75% of cells expressing CD30 and generally do not express ALK and EMA. (7) Myeloid sarcoma. Diffuse undifferentiated tumor cells with irregular nuclei and certain atypia. The cells express MPO and CD34, but not CD30 and T cell markers. (8) Breast implant-associated ALCL. A history of implants, negative ALK, and an inert clinical course. (9) Peripheral T-cell lymphoma, non-specific type. The tumor cells are generally not anaplastic, although some cases have a generally weak or focal expression of CD30, but no expression of ALK or EMA.
Given that breast development is the most common cause of breast masses in male patients, a mammogram avoids the need for further imaging in most cases. Ultrasound-guided and coarse-needle puncture biopsies are superior to fine-needle puncture, with these procedures performed by a surgical pathologist to assess the immune phenotype and identify any changes in cancer cell types, cellular proteins, or genes. Our patient presented with four mutations, BCOR_p.Q600X, DNMT3A_p.F609fs, NOTCH1_p.P2320fs, and IDH2_p.R140Q. The BCOR gene mutation is seen mainly in cases of acute granulocytic leukemia, NK/T-cell lymphoma, myelodysplastic syndromes, and other diseases, while the DNMT3A gene mutation is more commonly seen in cases of acute granulocytic leukemia, aplastic anemia, and T-lymphoblastoid lymphoma. The NOTCH1 gene mutation is seen mainly in T-lymphoblastoid lymphoma and chronic lymphocytic leukemia, while the IDH2 gene mutation is seen mainly in cases of acute granulocytic leukemia, angioimmunoblastic T-cell lymphoma, and myelodysplastic syndromes.14–17 Based on the mutation analysis of the above genes, our patient’s poor clinical prognosis and rapid progression were related to mutations of the relevant genes. We consider these mutations to be related directly to the development of primary or naive hematopoietic cell tumors of the bone marrow, which was one of the primary reasons for the rapid progression of the patient’s disease. As a result of this mutation, the biological behavior of this lymphoma mimicked that of a highly malignant lymphoma. The patient’s clinical status deteriorated dramatically after another relapse and he died within a short period of time. Extensive sequencing of the tumor exon was therefore not possible due to this short time frame and also the paucity of tissue collected at biopsy.18–20 We also performed a PET/CT to assess tumor metabolism and possible distant metastasis. However, the patient despite having previously received the CCOP chemotherapy regimen (ie, cyclophosphamide, vincristine, prednisolone acetate) did not achieve remission in a timely manner and relapsed after six months. His condition then deteriorated drastically after four months and he died in less than one month. Given the rarity of reported cases of PBL, numerous pathologists were consulted to obtain the final diagnosis. Assessment of morphological features and the application of assistive devices were necessary prerequisites for obtaining an accurate diagnosis. Although breast implant-associated ALCL is currently receiving increasing attention, it is important to note that lymphomas involving breast tissue are not limited to those associated with breast implants. Our review of the literature identified 12 similar cases of systemic ALCL with no prior history of involvement in other tissues.17–26 All available clinical information on similar cases is summarized in Table 1. This review of reported cases showed that anaplastic large cell lymphoma occurred in the breast, jejunum, ileum, lung, central nervous system including the cerebellum, skeletal muscle, bone, bladder, and other sites. However, gene rearrangement of IRF4/DUSP22 was performed in only a few of the reported cases and detection of more gene sequences was not carried out, possibly due to limitations in the testing conditions of the laboratories. Therefore, the detection of a gene mutation in our extremely rare case of a male breast anaplastic large cell lymphoma is a very important finding that provides the basis for clinical treatment of this malignancy.
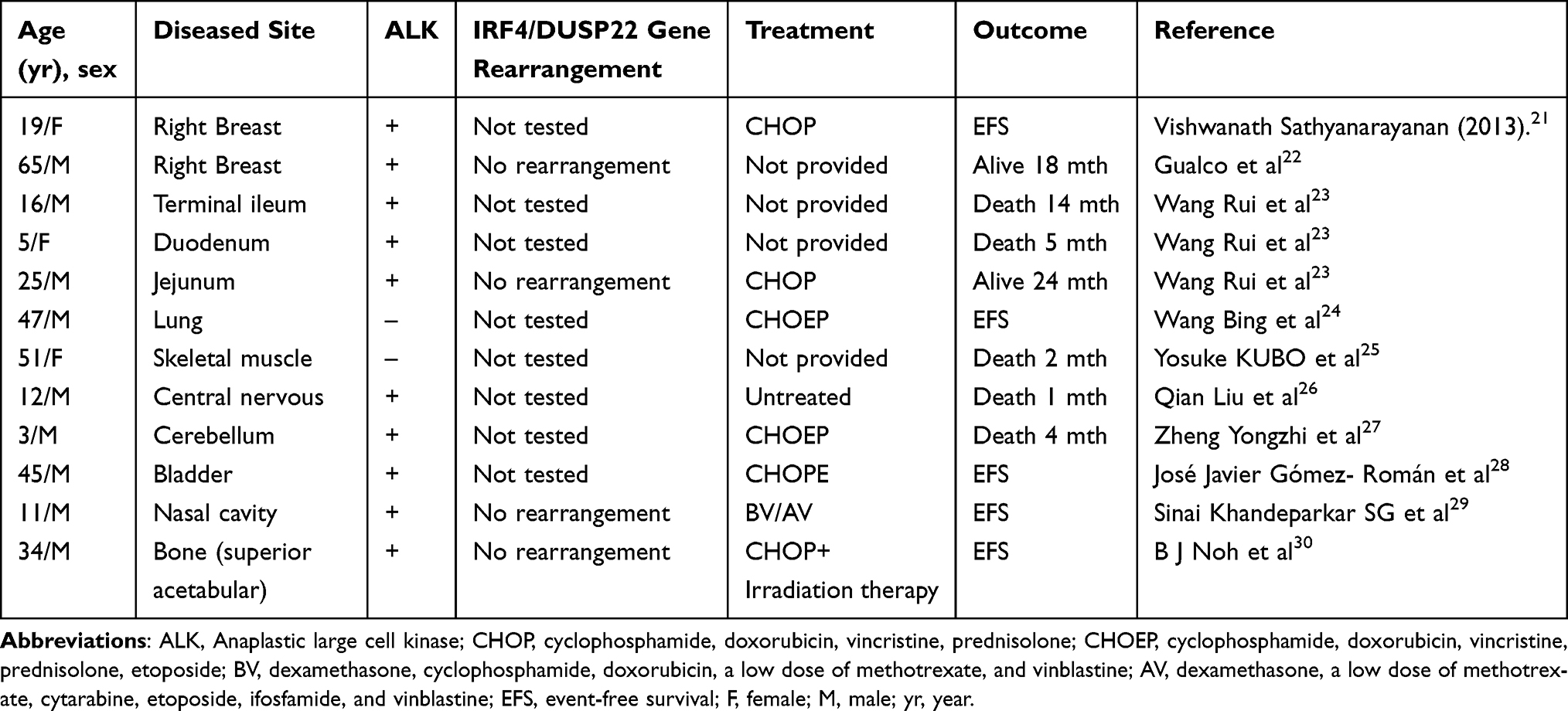 |
Table 1 Patient Information for Systemic ALCL Involving Rare Sites |
Conclusion
The rarity of breast T-cell lymphoma, especially male breast T-cell lymphoma and the histologic differential diagnosis of this tumor were accompanied by mutations in the following genes: BCOR_p.Q600X, DNMT3A_p.F609fs, NOTCH1_p.P2320fs, and IDH2_p.R140Q. Mutations in these genes are found more frequently in lymphoblastoid lymphoma or leukemia. An accurate pathological diagnosis through a detailed history, including imaging is therefore a prerequisite for the correct treatment of the tumor, although genetic testing can explain the prognosis and regression of the tumor in a more profound way. The presence of the genetic mutations associated with regression of the tumor were the main reasons that led to the death of this patient during treatment.
Ethical Statement and Consent to Participate
The study was reviewed and approved by the Ethics Committee of The Fourth Hospital of Hebei Medical University (approval number, 2022KS023. The study did not involve interaction with human subjects and/or the use of personally identifiable information. There was no need for informed consent to be obtained from the patient for the use of existing pathological materials in the study and identifiable patient information was not disclosed in the manuscript.
Availability of Supporting Data
The source of data for all the Figures and Tables is provided in the paper. No new datasets have been generated or analyzed for this article.
Informed Consent Statement: Informed consent was obtained from the patient involved in this study. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Consent for Publication
All the authors agree to the publication of this article.
Acknowledgments
We acknowledge the excellent technical assistance of the members of the tumor genetics laboratory at the Institutes of Human Genetics in Hebei Medical University, particularly Zi Zhang, Fei Lu, Xudi Liu, Yongjun Wang, Huichai Yang, Huazi Hao, and HongLei Wang, and also the team of the Lymph Node Registry, Beijing Friendship Hospital, particularly Xiaoge Zhou and Jianlan Xie.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work reported in this article did not receive funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Vitiello P, Sica A, Ronchi A, Caccavale S, Franco R, Argenziano G. PrimaryCutaneous B-Cell Lymphomas: an Update. Front Oncol. 2020;10:651.doi. doi:10.3389/fonc.2020.00651
2. Zeming L, Sichao C, Liang G. Recent advances and recommendations in breast prosthesis-associated anaplastic large cell lymphoma. Chin J Plast Surg. 2021;37:8.
3. Jia R, Sen R, Baohua Y. Clinicopathological features of lymphohematopoietic tumors in mammary needle biopsy. Chin J Pathol. 2018;47:10.
4. Xiaoke Z, Xuemei W, Zhiguang C. Ultrasound manifestations of male primary breast lymphoma: a case of Chinese medical imaging technology. Chin J Med Imaging Techno. 2021;37(9):56.
5. Duman BB, Berksoy S, Güvenç B, Ergin M. Lymphoma of the breast in a male patient. Med Oncol. 2011;28:S490–S493.DOI. doi:10.1007/s12032-010-9675-0
6. Ishibashi N, Hata M, Mochizuki T, et al. Radiation therapy for primary breast lymphoma in male gynecomastia: a rare case report and review of the literature. Int J Hematol. 2016;104(4):519–524. doi:10.1007/s12185-016-2026-y
7. Swerdlow SH. Cutaneous Marginal Zone Lymphomas. Semin Diagn Pathol. 2014:85
8. Huifang Y, Pangning H, Jing H. A case of ALK-positive anaplastic large cell lymphoma complicated with hemophagocytic syndrome. Chine Clin Oncol. 2021;26(4):57.
9. Ran P, Hui L, Yongzhen H, Chen M, Dong A. FDG PET/CT of Primary Breast Lymphoma in a Man. Clin Nucl Med. 2022;47(5):447–448. doi:10.1097/RLU.0000000000003978
10. Fitzpatrick MJ, Massoth LR, Marcus C. JAK2 Rearrangements Are a Recurrent Alteration in CD30+ Systemic T-Cell Lymphomas With Anaplastic Morphology. Am J Surg Pathol. 2021;45(7):895–904. doi:10.1097/PAS.0000000000001708
11. Amador C, Feldman AL. How I Diagnose Anaplastic Large Cell Lymphoma Am. J Clin Pathol. 2021;155(4):479–497. doi:10.1093/ajcp/aqab012
12. Campanale A, Di Napoli A, Ventimiglia M. Chest wall infiltration is a critical prognostic factor in breast implant-associated anaplastic large-cell lymphoma affected patients. Eur J Cancer. 2021;148:277–286. doi:10.1016/j.ejca.2021.01.041
13. Di Napoli A, Greco D, Scafetta G. IL-10, IL-13, Eotaxin and IL-10/IL-6 ratio distinguish breast implant-associated anaplastic large-cell lymphoma from all types of benign late seromas. Cancer Immunol Immunother. 2021;70(5):1379–1392. doi:10.1007/s00262-020-02778-3
14. Papaemmanuil E, Gerstung M, Bullinger L, et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia[J]. N Engl J Med. 2016;374(23):2209–2221. doi:10.1056/NEJMoa1516192
15. Liang S, Zhou X, Pan H, et al. Prognostic value of DNMT3A mutations in myelodysplastic syndromes: a meta-analysis. Hematology. 2019;24(1):613–622. doi:10.1080/16078454.2019.1657613
16. Bond J, Touzart A, Leprêtre S, et al. DNMT3A mutation is associated with increased age and adverse outcome in adult T-cell acute lymphoblastic leukemia[J]. Haematologica. 2019;104(8):1617–1625. doi:10.3324/haematol.2018.197848
17. Liu RB, Guo JG, Liu TZ, et al. Meta-analysis of the clinical characteristics and prognostic relevance of NOTCH1 and FBXW7 mutation in T-cell acute lymphoblastic leukemia[J]. Oncotarget. 2017;8(39):66360–66370. doi:10.18632/oncotarget.18576
18. Gerbe A, Alame M, Dereure O. Systemic, primary cutaneous, and breast implant-associated ALK-negative anaplastic large-cell lymphomas present similar biologic features despite distinct clinical behavior. Virchows Arch. 2019;475(2):163–174. doi:10.1007/s00428-019-02570-4
19. Menter T, Ballova V, Caspar C. ALK-negative anaplastic large cell lymphoma arising in the thrombus of an aortic prosthesis preceeded by clonally related lymphomatoid papulosis. Virchows Arch. 2019;474(6):763–767. doi:10.1007/s00428-019-02531-x
20. Belludi CK, Qian ET, Tolle JJ, Brown RM, Thompson MA, Juskevicius R. Anaplastic Large Cell Lymphoma Manifesting as Pleural Effusion in a Patient with Long-Standing Eosinophilia. Lab Med. 2019;50(1):87–92. doi:10.1093/labmed/lmy035
21. Sathyanarayanan V, Nagendrappa Lokesh K. Anaplastic lymphoma kinase (ALK) positive anaplastic large cell lymphoma (ALCL) of breast in a patient without a breast implant. Ann Saudi Med. 2014;34(6):551–554. doi:10.5144/0256-4947.2014.551
22. Gualco G, Chioato L, J. W, Weiss LM, Bacchi CE. Primary and secondary T-cell lymphomas of the breast: clinico-pathologic features of 11 cases. Appl Immun Mol Morphol. 2009;17(4):301–306. doi:10.1097/PAI.0b013e318195286d
23. Rui W, Yuqiao X, Ling C. Clinicopathological analysis of 3 cases of primary ALK-positive anaplastic large cell lymphoma of the small intestine. J Clin Exp Pathol. 2022;38(8):17.
24. Bing W, Liu L, Dacheng J. One case of primary pulmonary ALK-negative anaplastic large cell lymphoma. Chine Clin Oncol. 2021;26(12):87.
25. Kubo Y, Aoi J, Johno T, et al. A case of anaplastic large cell lymphoma of skeletal muscle. J Dermato. 2014;41(11):999–1002. doi:10.1111/1346-8138.12641
26. Liu Q, Chen X, Gandi L, et al. Primary central nervous system ALK-positive anaplastic large cell lymphoma with CD56 abnormally expression in a Chinese child: challenge in diagnostic practice. Int J Immunopathol Pharmacol. 2020;34:2058738420941756. doi:10.1177/2058738420941756
27. Yongzhi Z, Chen Y, Hao Z, et al. A case of primary central nervous system anaplastic lymphoma kinase-positive anaplastic large cell lymphoma in a child and literature review [J]. Leukemia·Lymphoma. 2021;30(9):550–554.
28. Gómez‐Román JJ, Cobo MLC, Val‐Bernal JF. Anaplastic lymphoma kinase-positive anaplastic large cell lymphoma presenting as a bladder neoplasm. Pathol Int. 2008;58(4):249–252. doi:10.1111/j.1440-1827.2008.02219.x
29. Sinai Khandeparkar SG, Bagale P, Pathade S, Gogate B, Battin S. ALK-positive anaplastic large T-cell lymphoma presenting primarily as a sinonasal mass with pseudoproptosis: a case report. Indian J Cancer. 2021;58(4):592–597. doi:10.4103/ijc.IJC_304_20
30. Noh BJ, Han CS, Park JS, et al. ALK-positive anaplastic large-cell lymphoma with primary bone involvement: a rare case and review of the literature. Malays J Pathol. 2018;40(2):161–167.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.