Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
A Case-Control Study of the MTHFR C665T Gene Polymorphism on Macrocytic Anemia Among HIV-Infected Patients Receiving Zidovudine
Authors Pertiwi D ![]() , Sofro MAU, Winarni TI, Probandari AN
, Sofro MAU, Winarni TI, Probandari AN
Received 18 April 2022
Accepted for publication 20 July 2022
Published 29 July 2022 Volume 2022:15 Pages 1633—1641
DOI https://doi.org/10.2147/JMDH.S370536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Danis Pertiwi,1 Muchlis Achsan Udji Sofro,2 Tri Indah Winarni,3 Ari Natalia Probandari4
1Department of Clinical Pathology, Faculty of Medicine, Universitas Islam Sultan Agung, Semarang, Indonesia; 2Department of Tropical and Infectious Disease, Dr. Kariadi Hospital, Semarang, Indonesia; 3Department of Anatomy, Faculty of Medicine, Universitas Diponegoro, Semarang, Indonesia; 4Department of Public Health, Faculty of Medicine, Universitas Sebelas Maret, Surakarta, Indonesia
Correspondence: Danis Pertiwi, Department of Clinical Pathology, Faculty of Medicine, Universitas Islam Sultan Agung, Semarang, 50112, Indonesia, Tel +628122910269, Email [email protected]
Background: Macrocytic anemia is the most common anemia in HIV-infected patients receiving zidovudine, and is closely related to folate and vitamin B12 deficiencies. Homocysteine > 10 μmol/L and increased MMA (methylmalonic acid) levels > 24.8 ng/mL indicate high/low folate and vitamin B12 deficiencies. Furthermore, MTHFR (Methylene-tetrahydrofolate-reductase) plays an essential role in the transmethylation of homocysteine to methionine and is related to DNA synthesis. The MTHFR C665T gene polymorphism decreases the activity of MTHFR, which culminates in homocysteinemia. Therefore, this case-control aims to assess the role of the MTHFR C665T gene polymorphism on the risk of macrocytic anemia among HIV-infected individuals receiving zidovudine.
Methods: This study was conducted using an unmatched case-control design and the participants were HIV-infected adults aged 20 to 59 years old, receiving zidovudine for four weeks and above. A sample of 232 patients was divided into case group with macrocytic anemia and the control having no anemia. Multivariate logistic regression analysis was then implemented to determine the risk factors.
Results: The results showed that there was a significant difference in the number of female and male patients namely 51.3% and 48.7%, respectively, with p< 0.001. Moreover, the mean age of the cases and control group was 41.9 ± 9.4 and 36.2 ± 8.3. Regarding education, there were significant differences between subjects with low and high education 47.8% vs 52.2% with p< 0.001. The majority of patients or 90.95% had taken AZT for more than 6 months. The logistic regression analysis test results showed that sex, age, education level, duration of AZT use, and homocysteine levels were predictors of macrocytic anemia with p< 0.05, while MTHFR C665T gene polymorphism and MMA levels were not risk factors.
Conclusion: MTHFR C665T gene polymorphism does not contribute to the incidence of macrocytic anemia among HIV-infected individuals receiving zidovudine.
Keywords: polymorphism, MTHFR C665T, macrocytic anemia, HIV, zidovudine
Introduction
Azido thymidine (AZT) or zidovudine is a nucleoside reverse transcriptase inhibitor (NRTIs) recommended by WHO and has become the primary option in HIV/AIDS therapy since 1990. The regulation of Indonesian Ministry of Health No. 87 of 2014 on Antiretroviral Treatment Guidelines includes AZT-containing regimen as the first-line alternative therapy for HIV/AIDS.1 Considering the guidelines, AZT-containing regimen has been widely used in Indonesia. However, long-term therapy is reportedly associated with macrocytic anemia, which is related to vitamin B12 and folate deficiency.2 Among PLWHA, certain HAART regimens, specifically nucleoside reverse transcriptase inhibitors such as AZT/zidovudine, stavudine (d4T), and 3TC are related to macrocytosis.3 Zidovudine is a thymidine analog that causes macrocytic anemia by interfering with DNA synthesis.4 The accumulation in cells increases intracellular reactive oxygen species (ROS) and mitochondrial toxicity,5 including erythrocyte damage.6 In addition, macrocytic anemia is linked to a lack of vitamin B12 and folate.7 Methylene-tetrahydrofolate-reductase (MTHFR) gene polymorphism is a genetic factor associated with folate and vitamin B12 levels.8 In the genetic variation, MTHFR C665T gene polymorphism incidence ranges from 24% to 53% and is affected by ethnicity and geography.9 It affects thermolability, which culminates in a 50% reduction of MTHFR enzyme activity.10 This decline leads to increased plasma homocysteine (Hcy) levels, called hyperhomocysteinemia.11 Hyperhomocysteine indicates folate and vitamin B12 deficiency and the MTHFR C665T gene polymorphism. The increased level of methylmalonic acid (MMA) is a more specific parameter for vitamin B12 insufficiency. The red blood cell differentiation requires adequate quantities of vitamin B12 and folate.12
Several factors have been found to cause the occurrence of macrocytic anemia.13 The authors have not found any studies evaluating the function of genetic variables, specifically in relation to the significance of the MTHFR gene variant C665T in the incidence of macrocytic anemia among HIV-infected patients receiving AZT-containing regimen therapy. Therefore, this study aims to investigate the effect of the MTHFR C665T gene polymorphism on the risk of macrocytic anemia among HIV-infected individuals receiving zidovudine. According to various previous studies, polymorphisms affect macrocytic anemia, but there are currently no reports on patients with HIV/AIDS receiving AZT.
Methods
This study was conducted using an observational analytic method with an unmatched case-control design. The subjects were outpatients of twelve rural and urban public health service facilities with a specific clinic for HIV in Central Java Province, Indonesia. They were selected based on medical treatment namely AZT-containing regimen and laboratory test results comprising Hemoglobin (Hb), and MCV. Furthermore, demographic data including sex, age, marital status, and sexual orientation, as well as medical history and clinical data on admission were collected from medical records, interviews, and laboratory results. The sample size was calculated using a formula which suggested a minimum number of 106 subjects in each group. The consecutive sampling method was implemented to select the potential subjects of the case and control groups.
The inclusion criteria for the subjects as cases were adults (aged 20 to 59 years), receiving treatment regimens containing zidovudine for 4 weeks and above, Hb levels <12 g/dL for women and <13 g/dL for men, not currently pregnant, MCV values >96 fL, and Javanese ethnic. The inclusion criteria of subjects as controls were adults (aged 20 to 59 years), receiving treatment regimens containing zidovudine for 4 weeks and above, Hb levels ≥12 g/dL for women and ≥13 g/dL for men, not currently pregnant, and Javanese ethnic. Determination of the criteria for the duration of AZT use for 4 weeks was based on previous studies.14 The exclusion criteria were alcoholism, use of drugs including anticonvulsants and chemotherapy, hypothyroidism, hepatic cirrhosis and alcoholic hepatitis, hemodialysis, myelodysplasia syndrome, aplastic anemia, chronic kidney disease, history of GIT surgery/gastrectomy, medication non-adherence, and unwilling to be a respondent.
Measurement of Macrocytic Anemia
Hb levels were examined by cyanide-free Hb spectrophotometry method. The data were categorized based on the cut off anemia value15 into anemia Hb level <12 and <13 mg/dL for women and men, respectively, or non anemia. The Mean Corpuscular Volume (MCV) and Hb were automatically calculated using the Automatic Hematology Analyzer Sysmex XN-1000. MCV values were categorized into16 >96 fL (Macrocytosis) or 96 fL (Non macrocytosis). The homocysteine and MMA serum level were analyzed using the ELISA method. Homocysteine data were categorized according to the cut off value17,18 to be >10 mol/L or ≤.10 mol/L, while MMA was categorized based on the cut off19 being >24.8 ng/mL or 24.8 ng/mL.
Assessing Polymorphism MTHFR C655T Gene
Single Nucleotide Polymorphism (SNPs) is characterized by substitution of nucleotide base cytosine (C) to thymine (T) in the 665th c the DNA sequence of the MTHFR gene. Identification of the polymorphism was evaluated using the technique of Polymerase Chain Reaction-Restriction Fragment Length of Polymorphism (PCR-RFLP). Data were categorized into yes (C665C) or not (C665T, T665T). The MTHFR gene was amplified using the ProFlex PCR machine with a total volume of 25 µL. Each tube consisted of 2 µL of DNA template, 8.9 µL dH2O, 12.5 µL Go Taq Green Master Mix, 2 µL primer forward and reverse with a concentration of 10 µM.
Statistical Analysis
Multivariate logistic regression tests were performed to determine the risk factors of macrocytic anemia among HIV-infected patients receiving zidovudine therapy. The odds ratio (OR) was determined based on the exp (B) value of the logistic regression analysis with 95% confidence interval (95% CI), while P value of <0.05 was considered statistically significant. Data were analyzed using International Business Machines (IBM) Statistical Package for the Social Sciences (SPSS) Statistics 23.
Ethics
The objectives were explained to the participants and written consent was taken before the interview, also, confidentiality and privacy were kept properly. This study corresponded to the Helsinki Declaration and was approved by the Health Research Ethics Committee, School of Medicine, Diponegoro University, Semarang, Indonesia (Letter Number: 123/EC/FK-RSDK/III/2018).
Results
A total of 232 patients participated and fulfilled the inclusion criteria, and they were divided into the case and control groups with 116 each. The demographic and clinical characteristics are presented in Table 1. There was a significant difference in the number of female and male patients with p<0.001. The mean age of the cases and control groups was 41.9 ± 9.4 and 36.2 ± 8.3, while the majority of patients or 43.5% were in the age range of 30–39 years. There was a significant difference in the number of subjects based on the education level with p<0.001. The duration of AZT consumption also showed a significant difference with p<0.001. Approximately 90.95% had taken the therapy for more than 6 months, while the duration for 9.05% was less.
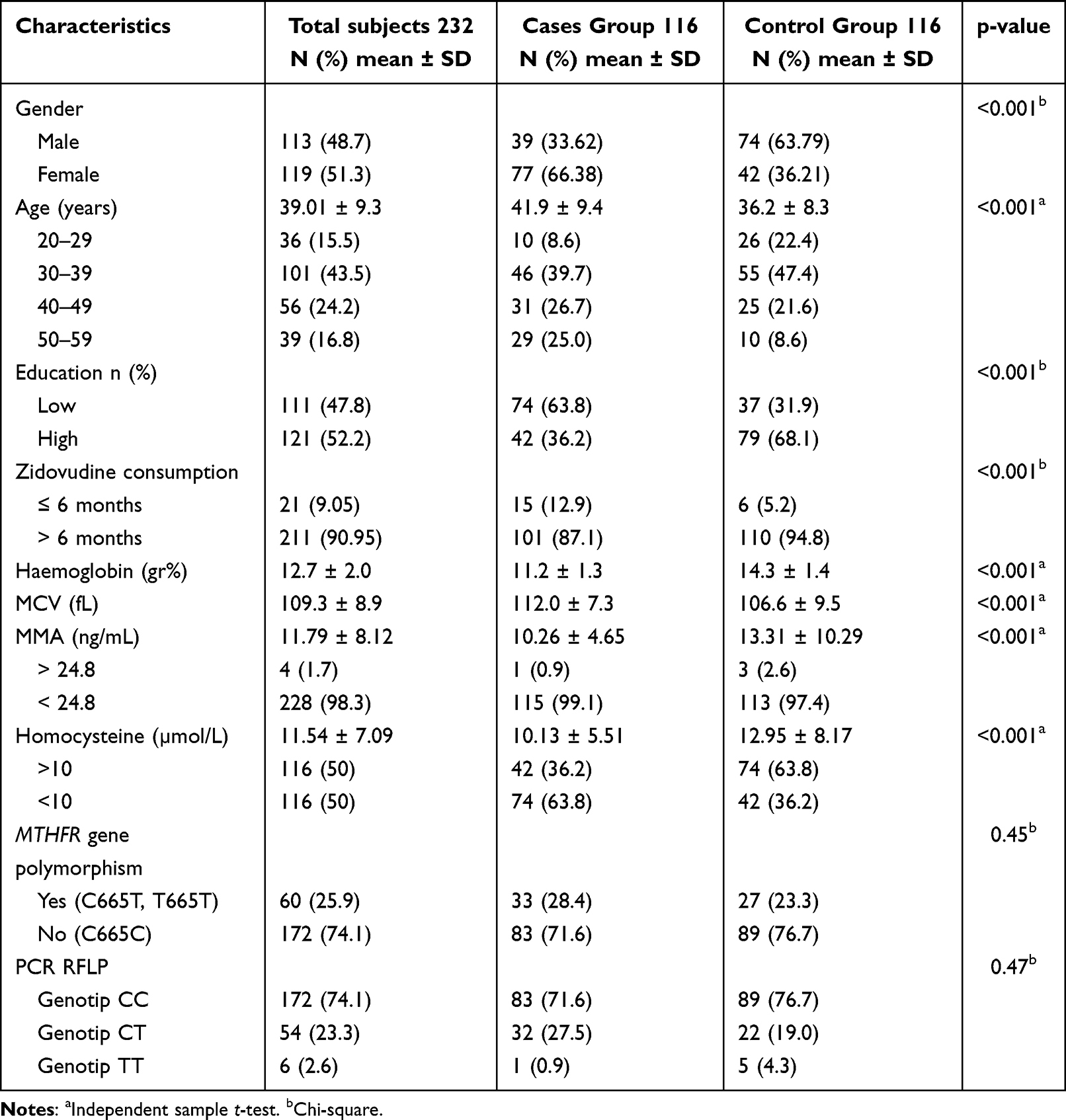 |
Table 1 Characteristic of HIV Patients Receiving Treatment Regimens Containing AZT ≥ 4 Weeks of Twelve Rural and Urban Public Health Service Facilities with Specific Clinic of HIV in Central Java Province, Indonesia |
The mean Hb level in the case and control groups was 11.2±1.3 g/dL and 14.3±1.4 g/dL, respectively. There was a significant difference in Hb levels between the two groups with p<0.001. The mean MCV of the case group was significantly higher than the control namely 11.02±7.3 vs 106.6±9.5, with p=<0.001. In addition, the mean of MMA between the two groups was significantly different with p<0.001. Based on the results, the number of MMA in both groups decreased. The mean level of homocysteine was found to be 11.54±7.09 µmol/L, and it was interpreted as homocysteinemia (>10 mol/L). The mean level in the case group at 10.13±5.51 mol/L was significantly lower than the control which is 12.95±8.17 mol/L (p<0.001).
Polymorphisms in the MTHFR C665T gene were discovered in 60 or 25.9% of patients. There were 33 (28.4%) of patients with polymorphisms in the case group and 27 (23.3%) in the control. The gene polymorphism was not statistically different between the two groups with p=0.45.
Based on the Restriction Fragment Length Polymorphism (RFLP) Polymerase Chain Reaction (PCR) examination of the MTHFR C665T gene, 172 (74.1%) were considered to have CC genotype specifically homozygote wild type, 54 (23.3%) had CT (heterozygote), and 6 (2.6%) had TT, the homozygote mutant type. The CC genotype and CT were found the case group with 83 (71.6%) and 32 (27.5%) while in the control with 89 (76.7%) and 22 (19.0%), respectively. The smallest number of genotypes, namely TT, was found in 1 subject or 0.9% of the case group and 5 or 4.3% in the control.
Table 2 shows the distribution of alleles in the case and control groups of HIV-infected patients. The frequency of C allele in the case group was 85.3% and the T allele was 14.77%. Meanwhile, in the control group, the frequency of the C and T allele was 86.2% and 13.8%, respectively.
 |
Table 2 Alleles Distribution of HIV Patients Receiving Therapy of Regimens Containing AZT ≥ 4 Weeks in Twelve Rural and Urban Public Health Service Facilities with Specific Clinic of HIV in Central Java Province, Indonesia |
As shown in Figure 1, lane L shows the ladder marker, lanes 116, 117, 122, and 125 homozygous wild type namely CC genotype revealed a product size of 294 bp. Lanes 118, 120, 121, 123, and 124 heterozygous namely CT genotype showed a product size of 294 bp, 168 bp, and 126 bp, while Lane 119 homozygous mutant or TT genotype showed 168 bp and 126 bp.
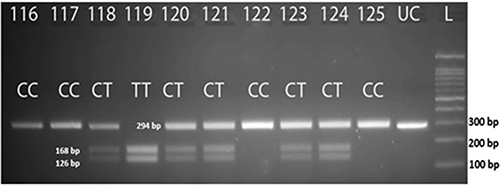 |
Figure 1 PCR-RFLP product of the MTHFR C665t genotype which was digested with the HinF1 enzyme. |
The different locations of the base cut identified using the restriction enzyme HinF1 indicated the existence of the MTHFR C665T gene polymorphism. The following observation of DNA sequencing was carried out on six subjects namely 3, 93, 97, 100, 148, and 174 to confirm the substitution of a single nucleotide base, C to T. Based on the results of PCR-RFLP, CC genotypes, CT, and TT were found in subjects number 97 and 148, 100 and 174, as well as 3 and 93, respectively. The sequencing results were in accordance with the PCR-RFLP result.
The DNA sequencing results of the MTHFR C665T gene polymorphism are shown in Figure 2. A-1 arrows indicate forward nucleotide C sequences, A-2 indicate reverse nucleotide G sequences, B-1 arrows indicate CT nucleotide forward sequences and B-2 arrows indicate GA reverse. Meanwhile, C-1 arrows indicate T nucleotide forward sequences and C-2 arrows indicate A reverse.
 |
Figure 2 Results of DNA sequencing of the MTHFR C665T gene polymorphism. |
The logistic regression analysis results presented in Table 3 show several predictors of macrocytic anemia such as gender, age, education level, duration of AZT use, and homocysteine levels with p<0.05. In contrast, MTHFR C665T gene polymorphism and MMA levels were not found to be risk factors with p>0.05.
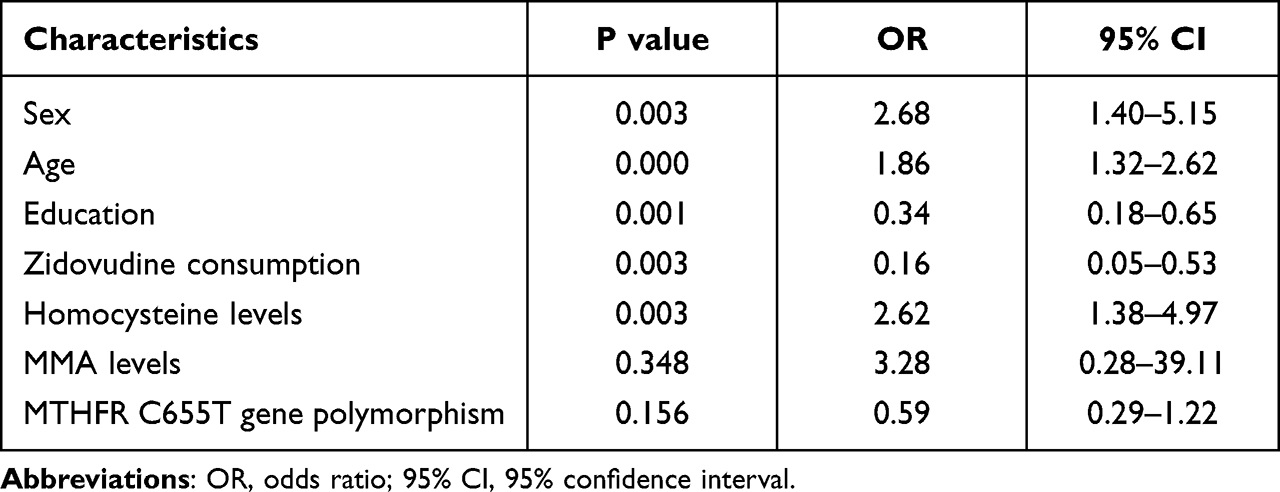 |
Table 3 Results of Logistic Regression Analysis |
Discussion
Anemia in HIV-infected patients is normally caused by chronic disease or the use of HIV drugs such as zidovudine. Meanwhile, Vitamin B12 and folate insufficiency are the most common causes of macrocytic anemia. Moreover, zidovudine is the most common HIV medicine that causes macrocytic anemia. A rise in homocysteine and MMA levels in the blood can be used to determine the presence of these illnesses.20 Anemia usually develops 4 to 12 weeks after starting zidovudine medication.14 After six months of treatment, there was a high prevalence of macrocytic anemia (80.6%).21
In most cases, hematological damage occurs within 3–6 months and is reversible.22 Anemia was more frequent in females than males among HIV-infected patients who received zidovudine due to blood loss during menstruation and lack of iron consumption from pregnancy to delivery.23,24 Adediran et al discovered that using thymidine analog treatment namely zidovudine, or stavudine was more related to macrocytosis in HIV patients than to the infection itself.25 Furthermore, disorders of erythrocyte nucleus maturation can cause delays in cell division causing cells to become larger, leading to macrocytosis. This condition can be caused by folate and vitamin B12 deficiency.13 Vitamin B12 has two functions, first, it acts as a coenzyme for biochemical processes as methyl B12. Second, it acts as a cofactor for methionine synthase, which is responsible for the methylation of homocysteine into methionine using 5-methyltetrahydrofolate (MTHF/methyl THF) as a methyl donor. The second function is deoxyadenosyl B12 (Ado B12), which converts MMA to succinyl Co-A. When an individual experiences a vitamin B12 deficiency, the circulating MMA levels will rise. MMA is a biomarker that is frequently used to evaluate the functional status of B12 vitamin because it is more stable than serum B12 vitamin. Also, the concentration of MMA increases before B12 vitamin level declines in the blood.26 Homocysteine and MMA levels are measured to detect the existence of B12 vitamin insufficiency. When there is vitamin B12 deficiency, homocysteine and MMA levels will increase.12,25,27,28
MTHFR, or methylenetetrahydrofolate reductase, is responsible for folate distribution and increased plasma total homocysteine concentration.29–31 The C665T gene polymorphism causes MTHFR to be thermolabile, decreasing enzyme activity, leading to lower 5-MTHF, vitamin B12, and folate levels, as well as increased homocysteine, and hypomethylation of genomic DNA.28,31–33 This implies that hereditary and non-genetic variables affect macrocytic anemia together with other genetic factors such as genes encoding the enzymes methionine synthase (MS)/5-methyltetrahydrofolate-homocysteine methyltransferase (MTR) and methylene-tetrahydrofolate dehydrogenase (MTHFD1), which play roles in homocysteine and folate metabolic pathways, and other physical interactions.34 In addition, the enzyme cystathionine synthase (CBS), the transcobalamin 2 receptor (TCN2), and methionine synthase reductase, all together affect homocysteine metabolism (MTRR).35 Non-genetic variables such as folate level, riboflavin status, therapeutic effect, and age also contribute to the risk of MTHFR C665T gene polymorphism.36
Based on the results, the gene polymorphism did not play a role in the incidence of macrocytic anemia in HIV patients receiving AZT-containing regimen therapy. Previous studies discovered that the MTHFR C665T gene polymorphism is not significantly linked with anemia. However, it was strongly connected with folate and vitamin B12 insufficiency, indicating that genetics does not contribute significantly to the risk of anemia.37 It was also reported that the MTHFR C665T gene polymorphism will cause MTHFR to become thermolabile and reduce the enzyme activity, thereby decreasing 5-MTHF, vitamin B12 and folate levels as well as increasing serum homocysteine and genomic DNA hypomethylation.8,32,33,38,39 A previous study stated that the gene polymorphism did not play a role in increasing homocysteine levels >10 mol/L. This might be due to the complex metabolic pathway of the homocysteine and the MTHFR enzyme which is only one of several enzymes involved in the pathway.40
The deficiency of folate and vitamin B12 causes disturbances in the maturation of the erythrocyte nucleus that affects the delay in cell division leading to macrocytic anemia.13,41 However, other studies also stated that macrocytic anemia in HIV-infected patients receiving zidovudine might indicate drug non-adherence.3 According to a previous report, ARV therapy can increase serum vitamin B12 levels in HIV-infected patients.42 This is consistent with the results obtained in this study which showed that the MTHFR C665T gene polymorphism was not a strong contributing factor to the increase of macrocytic anemia risk.
Investigations on the role of the MTHFR C665T gene polymorphism in the incidence of macrocytic anemia among HIV-infected patients receiving zidovudine therapy are limited. In Indonesia, there is a cultural aspect which limits studies on this area of HIV. The results obtained provide a new perspective for further investigations on the causes of macrocytic anemia among HIV-infected patients receiving zidovudine, which in turn can serve as a guide in preventing future occurrences. In addition, the results present a new protocol for controlling macrocytic anemia, with hematological monitoring in the first 6 months of using zidovudine.
The limitation of this study was that the examination of Hb levels before and after the use of zidovudine was not performed. Vitamin B intake which might influence the incidence of macrocytic anemia was also not evaluated.
Conclusions
The MTHFR C665T gene polymorphism did not contribute to the incidence of macrocytic anemia among HIV-infected individuals receiving zidovudine. Polymorphism is related to ethnicity, therefore, its influence on macrocytic anemia might be different from one race to another. Further study on other ethnicity needs to be conducted to confirm this assumption. There is also a need to consider non-genetic factors that can affect homocysteine metabolic pathways such as vitamin B intake.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ministry of Health Republic of Indonesia. Regulation of Indonesian ministry of health No. 87 of 2014 on antiretroviral treatment guidelines. Indonesian Ministry of Health; 2015:2004–2006.
2. Parkes-Ratanshi R, Katende D, Levin J, et al. Development of severe anemia and changes in hemoglobin in a cohort of HIV-infected Ugandan adults receiving zidovudine-, stavudine-, and tenofovir-containing antiretroviral regimens. J Int Assoc Provid AIDS Care. 2015;14(5):455–462. doi:10.1177/2325957414557264
3. Kufel WD, Hale CM, Sidman EF, Orellana CE, Miller CD. Nucleoside Reverse Transcriptase Inhibitor (NRTI) associated macrocytosis. Int J Virol AIDS. 2016;3:18. doi:10.23937/2469-567X/1510018
4. Barik S. Megaloblastic anemia: a drug-induced disorder. J Blood Dis Transfus. 2016;7:1–3.
5. Deavall DG, Martin EA, Horner JM, Roberts R. Drug-induced oxidative stress and toxicity. J Toxicol. 2012;2012:1–13. doi:10.1155/2012/645460
6. Cheng Y, Ren X, Gowda ASP, et al. Interaction of Sirt3 with OGG1 contributes to repair of mitochondrial DNA and protects from apoptotic cell death under oxidative stress. Cell Death Dis. 2013;4(7):e731. doi:10.1038/cddis.2013.254
7. Mahajan S, Aundhakar S. A study of the prevalence of serum vitamin B12 and folic acid deficiency in Western Maharashtra. J Fam Med Prim Care. 2015;4(1):64. doi:10.4103/2249-4863.152255
8. Haloi A, Das D. Vitamin B12 gene polymorphisms and chronic diseases. J Nutr Disord Ther. 2014;4:2.
9. Rajagopalan P, Jahanshad N, Stein JL, et al. Common folate gene variant, MTHFR C677T, is associated with brain structure in two independent cohorts of people with mild cognitive impairment. NeuroImage Clin. 2012;1(1):179–187. doi:10.1016/j.nicl.2012.09.012
10. Micheal S, Qamar R, Akhtar F, Khan MI, Khan WA, Ahmed A. MTHFR gene C677T and A1298C polymorphisms and homocysteine levels in primary open angle and primary closed angle glaucoma. Mol Vis. 2009;15:2268–2278.
11. Pramukarso DT, Faradz SM, Sari SH, Hadisaputro S. AB068. Association between MTHFR C677T and carotid intima medial thickness progression in post-ischemic stroke patient. Ann Transl Med. 2015;3(Suppl 2). doi:10.3978/j.issn.2305-5839.2015.AB068
12. Carmel R. Megaloblastic anemias: disorders of impaired DNA synthesis. In: Wintrobe’s Clinical Hematology. Lippincott Williams and Wilkins; 2014:2140–2183.
13. Veda P. Evaluation of macrocytosis in routine hemograms. Indian J Hematol Blood Transfus. 2013;29:26–30. doi:10.1007/s12288-011-0142-7
14. Kiragga AN, Castelnuovo B, Nakanjako D, Manabe YC. Baseline severe anaemia should not preclude use of zidovudine in antiretroviral-eligible patients in resource-limited settings. J Int AIDS Soc. 2010;13(1):42. doi:10.1186/1758-2652-13-42
15. World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. World Health Organization; 2011.
16. Obirikorang C, Issahaku RG, Osakunor DNM, Osei-Yeboah J. Anaemia and iron homeostasis in a cohort of HIV-infected patients: a cross-sectional study in Ghana. AIDS Res Treat. 2016;2016:1–8. doi:10.1155/2016/1623094
17. Fenech M. Folate (vitamin B9) and vitamin B12 and their function in the maintenance of nuclear and mitochondrial genome integrity. Mutat Res–Fundam Mol Mech Mutagen. 2012;733(1–2):21–33. doi:10.1016/j.mrfmmm.2011.11.003
18. Guo S, Pang H, Guo H, et al. Ethnic differences in the prevalence of high homocysteine levels among low-income rural Kazakh and Uyghur adults in far western China and its implications for preventive public health. Int J Environ Res Public Health. 2015;12(5):5373–5385. doi:10.3390/ijerph120505373
19. Jeruszka-Bielak M, Isman C, Schroder TH, Li W, Green TJ, Lamers Y. South asian ethnicity is related to the highest risk of vitamin b12 deficiency in pregnant Canadian women. Nutrients. 2017;9(4):1–13. doi:10.3390/nu9040317
20. Goyal V, Vaish P, Deshmukh A, Mishra J, Deshmukh G. Hematological study (Blood and bone marrow) in HIV patients. Int J Contemp Med. 2016;4:94–99. doi:10.5958/2321-1032.2016.00020.6
21. Tadele A. Prevalence of Zidovudine induced megaloblastic anemia among HIV/AIDS patients attending University of Gondar Hospital, Northwest Ethiopia. In:
22. Ejeliogu EU, Oguche S, Ebonyi AO, et al. Zidovudine-induced anaemia in human immunodeficiency virus infected children on highly active anti-retroviral therapy in Jos, Nigeria. J Adv Med Pharm Sci. 2014;1:1–10. doi:10.9734/JAMPS/2014/11241
23. Assefa M, Abegaz WE, Shewamare A, Medhin G, Belay M. Prevalence and correlates of anemia among HIV infected patients on highly active anti-retroviral therapy at Zewditu Memorial Hospital, Ethiopia. BMC Hematol. 2015;15(1):1–8. doi:10.1186/s12878-015-0024-6
24. Agarwal V, Kochhar A, Sachdeva R. Sensory and nutritional evaluation of sweet milk products prepared using stevia powder for diabetics. Stud Ethno-Med. 2010;4(1):9–13. doi:10.1080/09735070.2010.11886357
25. Adediran A, Osunkalu V, Wakama T, et al. Impact of HIV infection and zidovudine therapy on RBC parameters and urine methylmalonic acid levels. Interdiscip Perspect Infect Dis. 2016;2016:1–5. doi:10.1155/2016/5210963
26. TL Pedersen, WR Keyes, Shahab-Ferdows S, LH Allen, JW Newman. Methylmalonic acid quantification in low serum volumes by UPLC-MS/MS. J Chromatogr B Analyt Technol Biomed Life Sci. 2011;879(19):1502–1506. doi:10.1016/J.JCHROMB.2011.03.039
27. Sukriti S, Tauseef M, Yazbeck P, Mehta D. Mechanisms regulating endothelial permeability. Pulm Circ. 2014;4(4):535–551. doi:10.1086/677356
28. Das D. Vitamin B12 gene polymorphisms and chronic diseases. J Nutr Disord The. 2014;4(2):1–5. doi:10.4172/2161-0509.1000149
29. Mihiretie H, Taye B, Tsegaye A. Magnitude of anemia and associated factors among pediatric HIV/aids patients attending Zewditu Memorial Hospital art clinic, Addis Ababa, Ethiopia. Anemia. 2015;2015:1–6. doi:10.1155/2015/479329
30. Zhou B, Lu Y, Hajifathalian K, et al. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4·4 million participants. Lancet. 2016;387(10027):1513–1530. doi:10.1016/S0140-6736(16)00618-8
31. Nair M, Choudhury MK, Choudhury SS, et al. Association between maternal anaemia and pregnancy outcomes: a cohort study in Assam, India. BMJ Global Health. 2016;1(1):e000026. doi:10.1136/bmjgh-2015-000026
32. Leclerc D, Sibani S, Rozen R. Molecular Biology of Methylenetetrahydrofolate Reductase (MTHFR) and overview of mutations/polymorphisms. In: Madame Curie Bioscience Database. 2013;1–18.
33. Al-Batayneh KM, Zoubi MSA, Shehab M, et al. Association between MTHFR 677C>T polymorphism and vitamin B12 deficiency: a case control study. J Med Biochem. 2018;7:1–7.
34. Rahimi Z, Bozorgi M, Rahimi Z, et al. MTHFR C677T polymorphism is associated with the risk of breast cancer among Kurdish population from western Iran. Int J Cancer Manag. 2019;12(3). doi:10.5812/ijcm.67895
35. Mitchell ES, Conus N, Kaput J. B vitamin polymorphisms and behavior: evidence of associations with neurodevelopment, depression, schizophrenia, bipolar disorder and cognitive decline. Neurosci Biobehav Rev. 2014;47:307–320. doi:10.1016/j.neubiorev.2014.08.006
36. Ueland P, Rozen R. MTHFR Polymorphisms and Disease. Eurekah Landes Bioscience; 2005.
37. Sukla KK, Nagar R, Raman R. Vitamin-B12 and folate deficiency, major contributing factors for anemia: a population based study. e-SPEN J. 2014;9(1):e45–e48. doi:10.1016/j.clnme.2013.11.003
38. Ni J, Zhang L, Zhou T, et al. Association between the MTHFR C677T polymorphism, blood folate and vitamin B12 deficiency, and elevated serum total homocysteine in healthy individuals in Yunnan Province, China. J Chin Med Assoc. 2017;80:147–153. doi:10.1016/j.jcma.2016.07.005
39. Li W-X, Dai S-X, Zheng -J-J, Liu J-Q, Huang J-F. Homocysteine metabolism gene polymorphisms (MTHFR C677T, MTHFR A1298C, MTHFR A2756G and MTHFR A66G) jointly elevate the risk of folate deficiency. Nutrients. 2015;7:6670–6687. doi:10.3390/nu7085303
40. Rai V. Evaluation of the MTHFR C677T polymorphism as a risk factor for colorectal cancer in Asian populations. Asian Pac J Cancer Prev. 2016;16(18):8093–8100. doi:10.7314/APJCP.2015.16.18.8093
41. Hoffbrand AV, Moss PAH. Essential Haematology.
42. Owiredu W, Quaye L, Amidu N, Addai-Mensah O. Prevalence of anaemia and immunological markers among Ghanaian HAART-naïve HIV-patients and those on HAART. Afr Health Sci. 2011;11(1):1–14.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.