Back to Journals » Orthopedic Research and Reviews » Volume 18
A Bundled-Payment Program is Associated with Improved Access to Platelet Rich Plasma for Treatment of Osteoarthritis in Women and Non-White Population Groups
Authors Sin A, Shukla A, Hung Pinto W, Hymel A, Pennings JS, Talwar R, Porras L
Received 27 March 2026
Accepted for publication 16 June 2026
Published 10 July 2026 Volume 2026:18 607381
DOI https://doi.org/10.2147/ORR.S607381
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qian Chen
Alexander Sin,1,2 Anant Shukla,1 Wikien Hung Pinto,1 Alicia Hymel,1,3 Jacquelyn S Pennings,1,3 Ruchika Talwar,4,5 Lauren Porras1
1Department of Orthopaedic Surgery, Vanderbilt University Medical Center, Nashville, TN, USA; 2Department of Family Medicine, Louisiana State University Health Sciences Center New Orleans, Lafayette, LA, USA; 3Center for Musculoskeletal Research, Vanderbilt University Medical Center, Nashville, TN, USA; 4Department of Population Health, Vanderbilt University Medical Center, Nashville, TN, USA; 5Department of Urology, Vanderbilt University Medical Center, Nashville, TN, USA
Correspondence: Lauren Porras, Department of Orthopaedic Surgery, Vanderbilt University Medical Center, 1215 21st Ave South, MCE. South Tower Ste 4200, Nashville, TN, 37232-8828, USA, Email [email protected]
Purpose: To assess whether the implementation of a novel hospital-based bundled-payment program affects access to platelet rich plasma (PRP) injections for the treatment of osteoarthritis (OA) for patients representing different population subgroups.
Patients and Methods: This was a retrospective observational study, which included patients receiving PRP injections between January 2021 and October 2024, at three outpatient orthopaedic clinics of a single hospital-based institution. Patients were excluded if they did not undergo knee, hip, or shoulder (glenohumeral) PRP injections or had insurance coverage for PRP injections. The main outcome measured was the utilization of the bundled-payment program for PRP injections and treatment failure, defined as need for additional treatment within 9 months.
Results: Among 220 patients who received PRP injections, women were more likely to use the bundled-payment program than men (37.76% women vs 18.18% men, p = 0.003). Younger patients more frequently utilized the program (53.26 ± 9.55 years vs 62.02 ± 12.75 years, p < 0.001). Non-white patients were significantly more likely to use the bundled-payment program than white patients (51.61% vs 29.14%, p = 0.014). There were no significant differences in program utilization by ethnicity, DCI, or OA severity. There was no significant difference in odds for requiring additional treatments within 9 months between patients of different racial subgroups.
Conclusion: The bundled-payment program was associated with increased access to PRP for non-white patients and women. There was no significant difference between racial subgroups in terms of requiring additional treatments within 9 months after initial PRP treatments.
Keywords: osteoarthritis, platelet-rich plasma, bundled-payment program, non-white population
Introduction
Osteoarthritis (OA) is the current leading cause of chronic pain in adults1,2 and was highlighted by the WHO Global Ageing and Health Report as a leading cause of disability in adults aged 60 years and older.3 From 1990 to 2020, there has been a 132.2% increase in prevalence of OA globally.2 In the United States, OA affects more than 21% of the US population,4 and it has been estimated that 80 billion dollars are spent annually on management of OA.5 Studies have shown that OA symptoms vary by race, ethnicity, and socioeconomic status.6 For example, Black patients with OA have been found to experience more severe pain and disability when compared to White counterparts.7 This difference was reported to be more significant in patients with lower educational attainment, or those who live in a community of higher household poverty rate,8 potentially due to worse radiographic knee OA9,10 and having less access to OA pain management options such as physical therapy or joint replacements.11 Furthermore, these patients often have worse functional outcomes and complications when they undergo total joint replacement.12 While intra-articular injections such as corticosteroids serve as an effective alternative to surgery, we lack studies that examine the differences in safety and outcomes in patients of different races, ethnicities, and socioeconomic backgrounds.12
In the past decade, platelet rich plasma (PRP) has emerged as a promising non-operative treatment option for knee OA. It has been shown to have a comparable safety profile but longer lasting effect when compared to corticosteroid (CSI) and hyaluronic acid (HA) injections.13–15 It has been suggested to be a valuable alternative to total joint replacement surgery for patients of higher perioperative and postoperative complications.16 Clinically, there has also been an increasing number of sports medicine physicians across the world who are now using PRP in their practice. In a recent survey, 66.1% of all respondents reported using at least one type of orthobiologic such as PRP in their practice, and 71.6% utilized PRP for treatment of knee OA.17 While PRP seems to be a promising emerging treatment for OA, it is important to consider whether it is affordable and accessible to the general patient population. In the case of PRP, its cost can significantly vary between practices,18 depending on the clinical setting, use of anesthesia, and imaging guidance.19 Currently, insurance companies regard PRP treatments as experimental,20 resulting in out-of-pocket expenses for most patients, and this can exert a substantial financial burden on patients.18
In this study, we examined a novel hospital-based bundled-payment program that is available to employees of Vanderbilt University Medical Center, Metro Nashville Public Schools and other local self-insured employers. Through the MyOrtho Health program, all employees can enroll in an episodic bundle to receive full coverage for surgical or non-surgical care, evaluation, and treatment associated with the condition, without any copays or coinsurance in most patients.21 For the knee and hip OA bundled-payment programs, participants receive 100% coverage for imaging, medication, non-surgical treatments including corticosteroids, hyaluronic acid, PRP injections, and surgical treatments. The shoulder pain bundled-payment program has similar covered elements but does not cover PRP. The goal of this program is to expand equitable access of quality medical services to all employees of participating employers regardless of their race, ethnicity, and socioeconomic background, while reducing waste in terms of unnecessary procedures, prior authorizations, surgeries, and reduce multi-site care for common conditions. It was also created in anticipation of federal capacitated care and bundled-payment models for common conditions including OA.
This study aims to assess the differences in characteristics between patients who accessed PRP treatment via bundled-payment, and who accessed PRP treatment out-of-pocket due to insurance non-coverage through descriptive analysis, which would allow further evaluation on whether the implementation of this novel bundled-payment program may improve access to PRP for the treatment of OA for patients of population subgroups, in terms of age, gender, race, ethnicity, and their socioeconomic status.
Materials and Methods
Study Design
A retrospective chart review was performed for all patients who received PRP treatment(s) at three outpatient orthopaedic clinics of our institution for various orthopedic etiologies from January 2021 to October 2024.
Preparation of the PRP sample was conducted using an Emcyte Pure TWO 60 mL PRP kit. Following the manufacturer’s guidelines and with careful adherence to aseptic technique, 6 mL of anticoagulant was drawn into a 60 mL syringe. A total of 54 mL of whole blood was taken from the antecubital fossa of the consented patient. The anticoagulated whole blood was transferred into the first of two tubes. The sample was counterbalanced and placed into a centrifuge for 2 minutes at 4400 RPM. Upon completion, the resulting supernatant was carefully drawn from this tube and placed into the second tube, again paying close attention to aseptic technique. The second tube was counterbalanced and placed back into the centrifuge at 4400 RPM for 4 minutes.
Once complete, the excess plasma was siphoned from the tube. Average injection volume varied between 5 – 10cc of PRP. A total of 3 PRP injections were administered per patient. One injection every two weeks, under ultrasound guidance and sterile technique, by a board-certified sports medicine physician.
Study Participants
Patients with encounters where they received PRP treatment were identified using a specific institutional Current Procedural Terminology (CPT) code. The patients were included in this study if their diagnosis (The International Classification of Diseases 10th Revision, or ICD-10) code(s) associated with the PRP treatment were (i) glenohumeral OA, (ii) hip OA, or (iii) knee OA. Patients receiving PRP for non-OA conditions (eg, tendinopathies, ligament injuries) were excluded to ensure a homogenous study population. The patients’ charts were then reviewed, and data was collected regarding the patients’ insurance information and demographic information. For insurance information, it was noted if the patient was enrolled in the institutional bundled-payment program, or if they were enrolled in another form of commercial medical insurance. At the time of this study, Tricare, Federal Blue Cross, and some other smaller payers would reimburse PRP treatment, and all other insurance plans would require the patient to pay out of pocket. Patients that received reimbursement for PRP through insurance were therefore excluded from the analysis.
Study Outcomes
To assess the differences in characteristics between patient groups, the patients were separated into (i) enrollees of the bundled-payment program (bundled-payment group) who received PRP treatments covered by the program, and (ii) paying out-of-pocket for PRP treatments (out-of-pocket group). For demographic information, the age, gender, race, and ethnicity of the patient were recorded. The patient’s home zip code information was also recorded and converted into a Distressed Communities Index (DCI) score to determine the patient’s DCI quintile, divided into prosperous area (1st quintile), comfortable area (2nd quintile), mid-tier area (3rd quintile), at-risk area (4th quintile), and distressed area (5th quintile).22
After collecting insurance and demographic data, patients were stratified according to OA severity using the Kellgren-Lawrence grading system, which was categorized by the interpretation of corresponding x-rays by radiologists and confirmed by an additional Sports Medicine fellow. In the case of discrepancy, final grading was determined by a board-certified sports medicine physician.
In terms of secondary outcome measures, according to current literature, most individuals receiving PRP for treatment of knee OA have reported sustained therapeutic effects in terms of improvement in function and reduction in pain.23 Therefore, this study defined treatment failure as a patient requiring additional treatments (CSI, HA, or PRP injection) at or before 9 months after the initial PRP injection(s). Patient charts were reviewed at 3, 6, 9, and 12 months following their initial PRP injection to detect if there were any additional treatments in the same joint where PRP was injected during the initial visit. Racial subgroup analysis was performed to detect a difference in clinical outcomes.
Statistical Analysis
Differences in the demographic characteristics (age, gender, race, ethnicity) and DCI between bundled-payment group and out-of-pocket group were then analyzed statistically using univariate analyses: Pearson’s Chi-squared and Fisher’s exact tests were used for categorical variables due to sample size considerations, while Wilcoxon rank sum tests were applied for continuous variables given their non-parametric distribution. Patients without DCI due to incompatible zip code were excluded from the DCI analysis.
For secondary outcomes, multivariable logistic regression models were used to assess the relationship between race and the need for additional PRP, CSI, or HA treatment by 9 months after initial PRP injection, while controlling for OA severity. Patients without a specified race were excluded from these models.
R version 4.2 was used for statistical analyses in this study.24
This study complies with the Declaration of Helsinki. The study protocol was reviewed by Vanderbilt University Medical Center’s Investigational Review Board and was deemed exempt based on materials being collected from the already existing medical record without any of the 18 HIPAA identifiers (IRB #240123).
Results
A total of 569 unique patient records were retrieved and confirmed to have received PRP treatments from 2021 to 2024 at the study institution. Of those queried, 220 patients received PRP treatment(s) for hip, knee, and glenohumeral OA, and were therefore included in the final analysis (Figure 1). Overall, there were 140 patients (63.64%) who received knee PRP injections, 86 were self-pay and 54 through the bundled-payment program. For hip PRP injections, there were overall 53 patients (24.09%), 39 were self-pay and 14 through the bundled-payment program. For glenohumeral injections there were 27 patients (12.27%), and all (27) of them were self-pay as the shoulder bundled-payment program does not cover PRP at the time of this study.
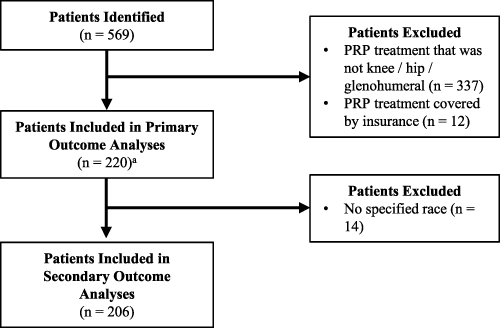 |
Figure 1 Flow Diagram showing Inclusion and Exclusion of Study Population. aDue to incompatible zip codes, 4 patients did not have a Distressed Community Index and were excluded from the corresponding analysis. |
Patient Demographics
Of the 220 patients, 143 (65%) were women and 77 (35%) were men. Mean age was 59.31 ± 12.50. Most patients were white (175, 84.95%), followed by Black (29, 14.08%), Middle Eastern (1, 0.49%), and American Indian (1, 0.49%). There were 14 patients (6.36% of the sample) who did not have a declared race. For the purposes of analysis, the Black, Middle Eastern, and American Indian patients were combined into one group (“non-white”). For ethnicity, 182 (94.79%) were not Hispanic or Latino/a, and 10 (5.21%) were Hispanic or Latino/a. Ethnicity data were unavailable for 28 patients, representing 12.7% of the sample. In terms of DCI, the mean DCI Score was 33.85 ± 26.65 (0 to 100, higher meaning more distressed). For DCI quintiles, 88 (40.74%) patients lived in a prosperous area (1st quintile), 42 (19.44%) in a comfortable area (2nd quintile), 42 (19.44%) in a mid-tier area (3rd quintile), 32 (14.81%) in an at-risk area (4th quintile), and 12 (5.56%) in a distressed area (5th quintile). There were 4 patient records without DCI due to incompatible zip code (areas with <500 people or PO Box zip codes).
Primary Outcome: Bundled-Payment Subgroup and Out-of-Pocket Subgroup Analysis
We performed descriptive analysis between different demographic subgroups (gender, age, race, ethnicity, DCI score and quintile) and detected some statistically significant differences between the bundled-payment group and out-of-pocket group, associated with certain demographic characteristics. Findings are summarized in Table 1.
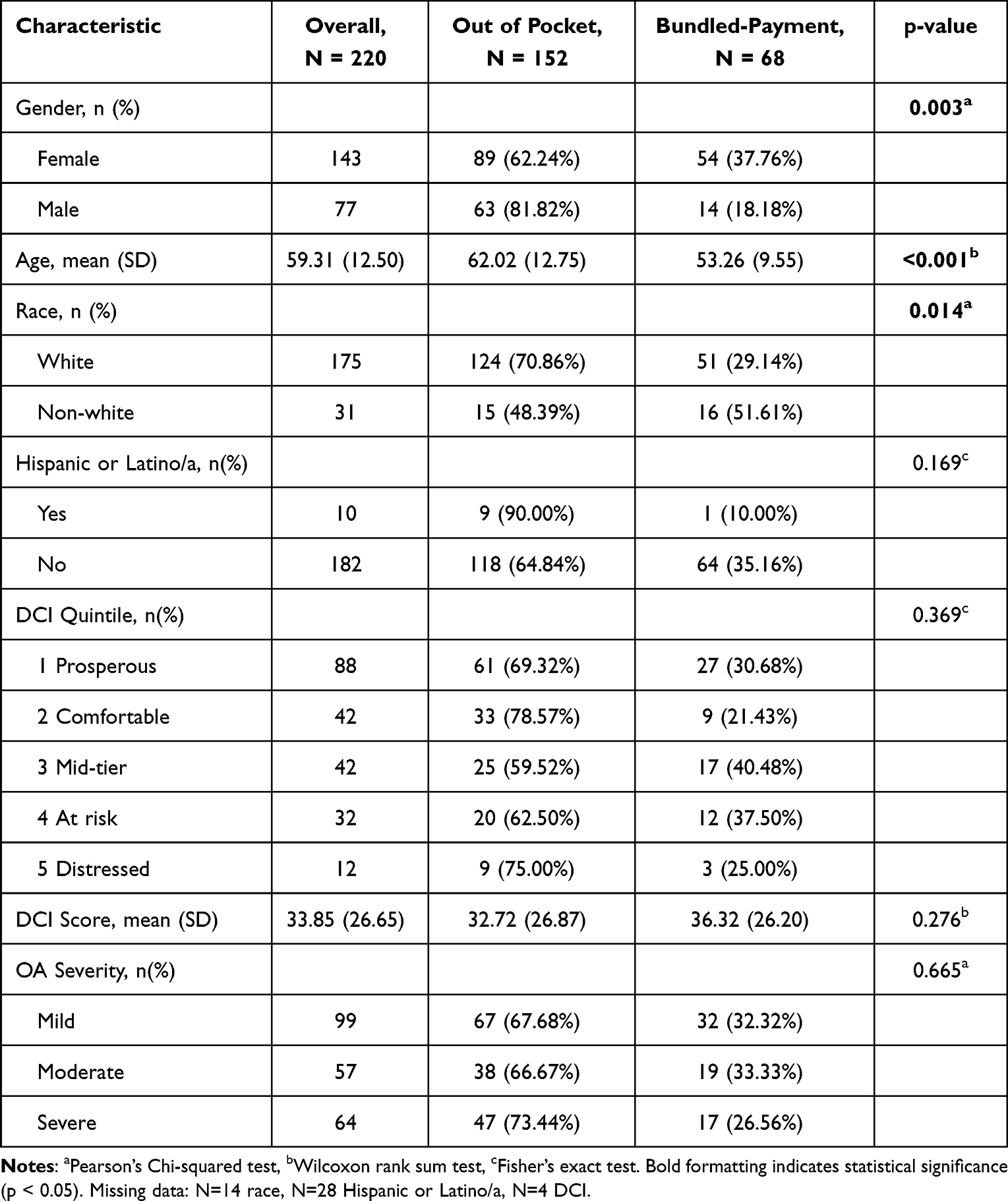 |
Table 1 Patient Characteristics |
Female patients (37.76%) were more likely to receive PRP treatments through the bundled-payment program compared to men (18.18%). This association was statistically significant (p = 0.003). Patients who received PRP treatment and enrolled in the bundled-payment program were on average younger (53.26 ± 9.55) than those paying out of pocket (62.02 ± 12.75). This association was statistically significant (p < 0.001). Non-white patients (51.61%) were more likely to receive PRP treatments through the bundled-payment program compared to White patients (29.14%). This association was statistically significant (p = 0.014). No significant association was found between different DCI quintiles (p = 0.369). This finding persisted when analyzing the continuous DCI score (p = 0.276).
Secondary Outcome: Racial-Subgroup Outcome Analysis
In this study, treatment failure was defined as requiring additional treatments (CSI, HA, or another PRP injection) by 9 months after the first PRP treatment. Outcome data was compared between groups (white, non-white) to determine if the patient’s race was associated with higher odds of treatment failure.
At 9 months, 12 patients (5.83%) received additional PRP treatment, 48 patients (23.30%) received CSI, and 21 patients (10.19%) received HA injections (Table 2 and Table 3).
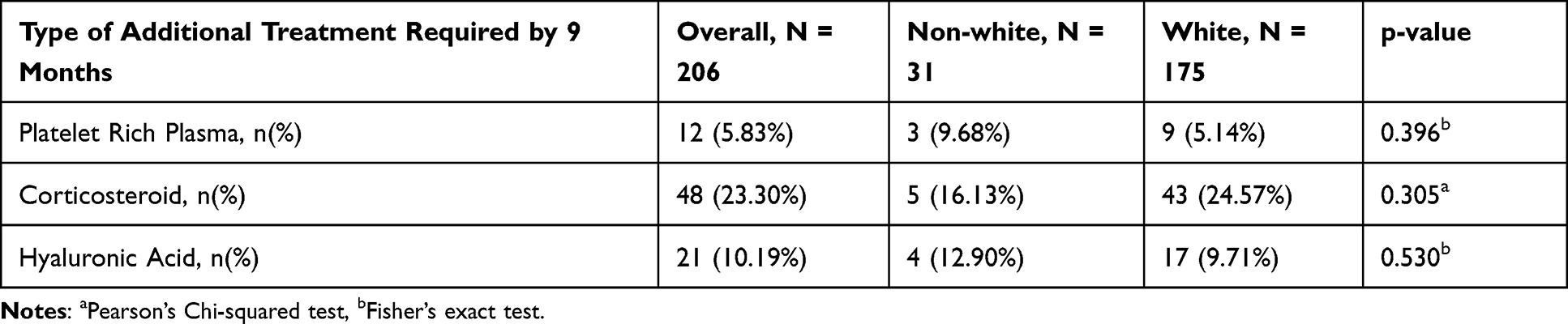 |
Table 2 Patients Requiring Additional Treatment(s) by 9 Months |
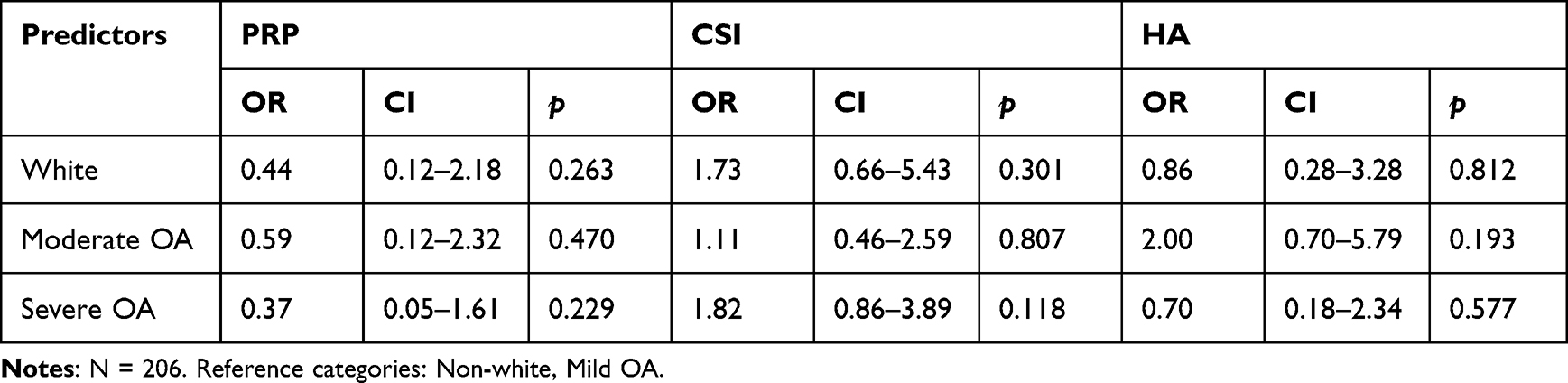 |
Table 3 Logistic Regression Models Predicting Odds of 9-Month Treatment for Race When Controlling for OA Severity |
While adjusting for OA severity (Table 2), the differences between groups were not found to be statistically significant. There were no statistically significant differences for requiring corticosteroid injections (p = 0.301) and hyaluronic acid injections (p = 0.812).
Discussion
OA is a widespread and debilitating condition that affects individuals across all demographic groups, but studies have shown that patients from different population subgroups often experience different access to treatment options. Patients from historically underserved communities often face greater challenges in obtaining care, leading to increased pain, functional limitations, and fewer non-surgical treatment options. Given the financial barriers that often limit treatment choices such as PRP, bundled-payment programs may serve as a model for increasing access to PRP injections, potentially mitigating some disparities in non-surgical OA treatment. While existing research has extensively examined the effectiveness and safety of PRP for OA, less attention has been given to ensuring broad and equitable access to this treatment.
It is also important to improve the validity of a study by ensuring adequate representation from different demographic groups. In the past, orthopaedic research has been found to be lacking in representing minority groups such as non-white population and individuals from impoverished countries. There has been a recent call for ensuring better representation and reporting of all demographic groups in orthopedic studies,25,26 especially for research on emerging therapies such as PRP. While this study is limited by its retrospective design and therefore unable to intentionally include minority groups, and 14 patients did not report their race, the final analysis included more than 15% of non-white population (31/206) which is comparable to most other biologics studies that report on patient demographics.25 This study also intentionally included detailed reporting of patient demographics, which is important for evaluating its external validity and applicability in other clinical settings.
This study evaluated the impact of a hospital-based bundled-payment program designed to reduce healthcare costs, limit waste, distribute resources equitably, and allow orthopaedic procedures such as PRP therapy to become more accessible to all eligible patients with knee, hip, and shoulder OA.21 Our data analysis indicated that this program may be associated with increased utilization of PRP among women and Black patients, demonstrating the potential of structured payment models to improve access, as opposed to insurance coverage or paying out-of-pocket. Understandably, the results of this study can only be applied to individuals who are eligible to enroll in the bundled-payment program. There was limited participation among individuals from the most economically disadvantaged areas, suggesting that financial constraints, such as for the transportation and other costs for the clinic visit, and time loss from work due to the visit and the procedure, still play a role in healthcare decisions.
When adjusting for OA severity, the likelihood of receiving a follow-up PRP injection did not differ significantly among racial groups. This can be interpreted as PRP injections being effective across different racial groups. Future research should investigate the potential for PRP as an important treatment alternative for certain population subgroups, such as Black patients and patients of lower socioeconomic status and education level, which have been reported to have worse clinical outcomes with other orthopedic treatments for OA. The findings of this study also support the novel bundled-payment program as a means to provide affordable, equitable, and consistently effective treatment opportunities across the population. Younger patients were more likely to participate in the program, suggesting that such initiatives may encourage earlier intervention for this progressive condition. While the long-term effects of earlier PRP treatment on OA progression remain an area for further study, our findings suggest that alternative payment structures can play a role in broadening access to non-surgical care. It is important to note that while the mean age in the bundled-payment group is lower (53.26 ± 9.55) as compared to that of the out-of-pocket group (62.02 ± 12.75), the members of that group still belonged to an older working demographic, aligning with broader labor force trends.
By reducing cost-related barriers, bundled-payment programs offer a practical approach to expanding treatment options for OA patients, allowing more individuals to pursue effective non-surgical interventions. Employers and healthcare institutions may consider similar models to help patients access high-quality care without unnecessary financial strain.
There are a few limitations to our study. As this study is a retrospective observational study, we are unable to actively ensure more equal representation from different population subgroups. There was an imbalance in group sizes in terms of race, and for the purposes of analysis, the Black, Middle Eastern, and American Indian patients were combined into one group. Due to this limitation, the findings of this study should be interpreted with caution. There was also lower patient participation from the most impoverished areas (14.81% from at-risk area and 5.56% from distressed area). Some variables, such as BMI, which may reveal intersectional effects of other social determinants of health, were not included in this study. Regarding OA severity grading, the radiographs were initially read by different radiologists, which may lead to a difference in reporting style, such as using a mild/moderate/severe scale or the Kellgren-Lawrence grading for OA. Our team utilized a Sports Medicine fellow to manually confirm all radiographic readings and assigned each patient with a corresponding OA severity systematically using the Kellgren-Lawrence grading to minimize any heterogeneity in this aspect. Some patients had missing demographic data. For example, 14 out of 220 patients did not have an associated race, and 28 out of 220 patients did not have an associated ethnicity. There were also patients with zip codes that were not compatible with conversion to DCI due to the zip code belonging to a PO box, or the zip code having too small of a population. Lastly, the analysis of the relationship between race and treatment failure was limited, due to the small number of observed treatment failures (12, 21, or 48 depending on the outcome), and the fact that white patients greatly outnumber non-white patients. Future studies with larger sample sizes could apply multivariate regression models to further assess interactions between demographic factors and treatment access.
Conclusion
Our retrospective chart review of the MyOrtho Health program from 2021 to 2024 demonstrated that implementing a hospital-based bundled-payment model increased access to platelet-rich plasma (PRP) therapy for non-white and female patients with shoulder, knee, and hip OA. Patients utilizing the bundled-payment program tended to be younger, which still represented the older one-third of the US labor force. We found no significant differences in access among patients from lower socioeconomic backgrounds, suggesting that financial barriers may persist despite the bundled-payment model.
There was no significant difference between groups in terms of requiring additional treatments within 9 months after initial PRP treatments when controlling for OA severity.
Future studies should evaluate the long-term impact of novel bundled-payment programs on OA outcomes. Employers and healthcare institutions may consider adopting similar models to enhance access to evidence-based, non-surgical OA treatments.
Disclosure
Dr Ruchika Talwar reports Consulting fees from CG Oncology, Immunity Bio, outside the submitted work. This study did not receive any funding, and the authors have no conflicts of interest to disclose.
References
1. Briggs AM, Cross MJ, Hoy DG, et al. Musculoskeletal health conditions represent a global threat to healthy aging: a report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist. 2016;56(Suppl 2):S243–8. doi:10.1093/geront/gnw002
2. Collaborators GBDO. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/S2665-9913(23)00163-7
3. World Health Organization. World Report on Ageing and Health. 2015. Available from: http://www.who.int/ageing/events/world-report-2015-launch/en/.
4. Helmick CG, Felson DT, Lawrence RC, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part I. Arthritis Rheum. 2008;58(1):15–25. doi:10.1002/art.23177
5. Dieleman JL, Baral R, Birger M, et al. US spending on personal health care and public health, 1996–2013. JAMA. 2016;316(24):2627–2646. doi:10.1001/jama.2016.16885
6. Callahan LF, Cleveland RJ, Allen KD, Golightly Y. Racial/ethnic, socioeconomic, and geographic disparities in the epidemiology of knee and hip osteoarthritis. Rheum Dis Clin North Am. 2021;47(1):1–20. doi:10.1016/j.rdc.2020.09.001
7. Vaughn IA, Terry EL, Bartley EJ, Schaefer N, Fillingim RB. Racial-ethnic differences in osteoarthritis pain and disability: a meta-analysis. J Pain. 2019;20(6):629–644. doi:10.1016/j.jpain.2018.11.012
8. Thompson KA, Terry EL, Sibille KT, et al. At the intersection of ethnicity/race and poverty: knee pain and physical function. J Racial Ethn Health Disparities. 2019;6(6):1131–1143. doi:10.1007/s40615-019-00615-7
9. Callahan LF, Shreffler J, Siaton BC, et al. Limited educational attainment and radiographic and symptomatic knee osteoarthritis: a cross-sectional analysis using data from the Johnston County (North Carolina) Osteoarthritis Project. Arthritis Res Ther. 2010;12(2):R46. doi:10.1186/ar2956
10. Callahan LF, Cleveland RJ, Shreffler J, et al. Associations of educational attainment, occupation and community poverty with knee osteoarthritis in the Johnston County (North Carolina) osteoarthritis project. Arthritis Res Ther. 2011;13(5):R169. doi:10.1186/ar3492
11. Booker S, Herr K, Tripp-Reimer T. Patterns and perceptions of self-management for osteoarthritis pain in African American Older Adults. Pain Med. 2019;20(8):1489–1499. doi:10.1093/pm/pny260
12. Reyes AM, Katz JN. Racial/ethnic and socioeconomic disparities in osteoarthritis management. Rheum Dis Clin North Am. 2021;47(1):21–40. doi:10.1016/j.rdc.2020.09.006
13. Chang KV, Hung CY, Aliwarga F, Wang TG, Han DS, Chen WS. Comparative effectiveness of platelet-rich plasma injections for treating knee joint cartilage degenerative pathology: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2014;95(3):562–575. doi:10.1016/j.apmr.2013.11.006
14. Laudy AB, Bakker EW, Rekers M, Moen MH. Efficacy of platelet-rich plasma injections in osteoarthritis of the knee: a systematic review and meta-analysis. Br J Sports Med. 2015;49(10):657–672. doi:10.1136/bjsports-2014-094036
15. Pojala CV, Toma S, Costache C, et al. The potential of intra-articular therapies in managing knee osteoarthritis: a systematic review. Clin Pract. 2024;14(5):1970–1996. doi:10.3390/clinpract14050157
16. Rajan PV, Ng MK, Klika A, et al. The cost-effectiveness of platelet-rich plasma injections for knee osteoarthritis: a markov decision analysis. J Bone Joint Surg Am. 2020;102(18):e104. doi:10.2106/JBJS.19.01446
17. Noback PC, Donnelley CA, Yeatts NC, et al. Utilization of orthobiologics by sports medicine physicians: a survey-based study. J Am Acad Orthop Surg Glob Res Rev. 2021;5(1):
18. Tiao J, Wang K, Herrera M, et al. There is wide variation in platelet-rich plasma injection pricing: a United States Nationwide Study of top orthopaedic hospitals. Clin Orthop Relat Res. 2024;482(4):675–684. doi:10.1097/CORR.0000000000002864
19. Dhillon RS, Schwarz EM, Maloney MD. Platelet-rich plasma therapy - future or trend? Arthritis Res Ther. 2012;14(4):219. doi:10.1186/ar3914
20. Piuzzi NS, Ng M, Kantor A, et al. What is the price and claimed efficacy of platelet-rich plasma injections for the treatment of knee osteoarthritis in the United States? J Knee Surg. 2019;32(9):879–885. doi:10.1055/s-0038-1669953
21. Health V. Vanderbilt Health’s MyOrthoHealth Brochure. 2025.
22. Data from: The Economic Innovation Group’s Distressed Communities Index (DCI). 2016–2020.
23. Costa LAV, Lenza M, Irrgang JJ, Fu FH, Ferretti M. How does platelet-rich plasma compare clinically to other therapies in the treatment of knee osteoarthritis? A systematic review and meta-analysis. Am J Sports Med. 2023;51(4):1074–1086. doi:10.1177/03635465211062243
24. Team RC. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. Available from: https://www.R-project.org/.
25. Sin A, Hollabaugh W, Porras L. Narrative review and call to action on reporting and representation in orthobiologics research for knee osteoarthritis. PM R. 2025;17(1):88–95. doi:10.1002/pmrj.13214
26. George J, Gautam D, Sugumar PA, Janardhanan R, Kabra A, Malhotra R. Uneven global and racial representation in major orthopaedic clinical trials: trends over a decade. J Clin Orthop Trauma. 2022;29:101894. doi:10.1016/j.jcot.2022.101894
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Network Analysis of Osteoarthritis Progression Using a Steiner Minimal Tree Algorithm
Xie Y, Shao F, Ji Y, Feng D, Wang L, Huang Z, Wu S, Sun F, Jiang H, Miyamoto A, Wang H, Zhang C
Journal of Inflammation Research 2024, 17:3201-3209
Published Date: 18 May 2024