Back to Journals » Medical Devices: Evidence and Research » Volume 18
A Buccal Mucosal Oximeter Accurately Measures Arterial Oxyhemoglobin Saturation
Authors Snow C, Magnison-Benoit S, Pun M, Tripp TR ![]() , Clarke A, Berghmans S, Hansen B, Transfiguracion L, Adatia S, Rawling JM, Roy S, Di Simone G, Lai ML
, Clarke A, Berghmans S, Hansen B, Transfiguracion L, Adatia S, Rawling JM, Roy S, Di Simone G, Lai ML ![]() , Mosca EV, Remmers JE, Poulin MJ
, Mosca EV, Remmers JE, Poulin MJ ![]()
Received 11 March 2025
Accepted for publication 10 June 2025
Published 11 July 2025 Volume 2025:18 Pages 387—395
DOI https://doi.org/10.2147/MDER.S527510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Connor Snow,1– 3 Shane Magnison-Benoit,1– 3 Matiram Pun,1– 3 Thomas R Tripp,1– 3 Aimee Clarke,1– 3 Sophie Berghmans,1– 3 Bradley Hansen,1– 3 Leo Transfiguracion,4 Saleema Adatia,5 Jean M Rawling,6 Steven Roy,7,8 Giovanni Di Simone,9 Ming-Lai Lai,9 Erin V Mosca,9 John E Remmers,9 Marc J Poulin1– 3,8,10,11
1Department of Physiology and Pharmacology, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada; 2Hotchkiss Brain Institute, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada; 3Faculty of Kinesiology, University of Calgary, Calgary, Alberta, Canada; 4Department of Anesthesia, Alberta Health Services, Calgary, Alberta, Canada; 5Symmetry Dental, Calgary, Alberta, Canada; 6Department of Family Medicine, University of Calgary, Calgary, Alberta, Canada; 7Department of Critical Care Medicine, University of Calgary, Calgary, Alberta, Canada; 8O’Brien Institute for Public Health, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada; 9ProSomnus Sleep Technologies, Pleasanton, CA, USA; 10Libin Cardiovascular Institute of Alberta, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada; 11Department of Clinical Neurosciences, Faculty of Medicine, University of Calgary, Calgary, Alberta, Canada
Correspondence: Marc J Poulin, HMRB-210, 3330 Hospital Drive NW Cumming School of Medicine, University of Calgary, Calgary, Alberta, T2N 4N1, Canada, Tel +1 403-220-8372, Email [email protected]
Purpose: While arterial oxyhemoglobin saturation (SaO2) decreases during sleep in many patients with sleep apnea and pulmonary diseases, personalized oximeters suitable for multi-night monitoring of SpO2 are not readily available. The present report describes a custom buccal mucosal intraoral oximeter that might provide the opportunity for such long-term monitoring given its strong accuracy in measuring SpO2 over a range of clinically relevant hypoxemia.
Patients and Methods: The intraoral buccal mucosal oximeter was constructed by encapsulating a reflectance pulse oximeter in an overlay of the maxillary dentition. Accuracy was assessed during non-motion conditions in normal participants (n = 12) made progressively hypoxic by decreasing the partial pressure of end-tidal oxygen (PETO2). CO-oximeter values of SaO2 from arterial blood constituted the “gold standard” for comparison with the buccal mucosal oximeter’s values. The oximeter’s pulse rate and an electrocardiogram (ECG) determined heart rate were also compared.
Results: Analysis of 325 paired SaO2 values from the CO-oximeter and buccal mucosal oximeter yielded the following: r = 0.95; bias = 0.72; and accuracy root-mean-square (ARMS) = 2.94%. Results from the pulse rate/ECG analysis were: r = 0.99; bias = 0.30; and ARMS = 2.08 bpm.
Conclusion: These results reveal robust accuracy of the buccal mucosal oximeter measurement of SaO2 and pulse rate, as shown by good agreement with a “gold standard” over a wide range of arterial hypoxemia. Such clinically acceptable accuracy indicates that this novel reflectance oximeter may prove useful in management of patients with sleep-induced hypoxemia by allowing for long-term monitoring of SaO2.
Keywords: hypoxia, oximetry, intraoral pulse oximeter, respiratory monitoring, obstructive sleep apnea, remote patient monitoring
Introduction
Monitoring of physiologic variables indicative of the presence and status of chronic disease have proven to be of considerable value in clinical management and improvement of therapeutic outcomes.1 For instance, positive airway pressure (PAP) devices used in the treatment of obstructive sleep apnea (OSA) and pulmonary diseases provide nightly monitoring of therapeutic pressures and pulmonary disturbances.2 Sleep-related declines in the oxyhemoglobin saturation of arterial blood (SaO2) are a common and important pathophysiological occurrence and are associated with an increased risk of cardiovascular events and decreased survival in patients with sleep apnea.3,4 Additionally, such nocturnal hypoxia displays substantial night-to-night variability in respiratory status during sleep.5 Thus, the need for a comfortable, accurate oximeter capable of long-term monitoring seems undeniable. An important consideration is that such monitoring must be convenient and inexpensive, features not present in currently available oximeters. The accuracy of conventional oximeters can be compromised by factors such as movement, poor perfusion, impaired thermoregulation, and ambient light interference.6–8 Importantly, SpO2 readings have been shown to be overestimated in individuals with darker skin, potentially leading to increased incidence of occult hypoxemia.9,10
ProSomnus Sleep Technologies (Pleasanton, CA) has developed a novel buccal mucosal oximeter (RPMO2 Oximeter Device). The oximeter is encapsulated in an overlay of the maxillary dentition and uses the mucosa of the buccal vestibule behind the upper lip as the reflective tissue. This device is suitable for long-term nightly monitoring as it is comfortable and rechargeable. The purpose of the present investigation is to assess the accuracy of this buccal mucosal oximeter in determining SaO2 under conditions of graded oxygenation from normoxia to severe hypoxia in normal, awake volunteers under non-motion conditions.
Materials and Methods
Study Approvals
The study protocol was designed in accordance with ISO 80601-2-61:2017 – Medical electrical equipment – Particular requirements for basic safety and essential performance of pulse oximeter equipment.11 The study was approved by the Conjoint Health Research Ethics Board (CHREB) of the University of Calgary (Calgary, Alberta, Canada; Ethics ID REB23-1003) and received Investigational Testing Authorization from Health Canada (ITA 373369). The study was registered on www.clinicaltrials.gov (NCT06267976) and the University of Calgary’s Participate in Research database. The study was conducted in accordance with the Tri-Council Policy Statement, Declaration of Helsinki, and international standards of Good Clinical Practice. All participants provided written informed consent prior to undergoing study procedures.
Participants
Twelve healthy individuals between the ages of 18 and 50 years were enrolled in the study, meeting the minimum sample size stipulated by ISO 80601-2-61:2017. All participants met the following eligibility criteria: adequate dentition for the buccal mucosal oximeter device; ability to breathe through the nose comfortably; body mass index (BMI) less than 40 kg/m2; no known history of heart, lung, kidney, or liver disease; no diagnosis of asthma or sleep apnea; no diagnosis of diabetes; no presence of a clotting disorder, hemoglobinopathy, or anemia; not pregnant or lactating; resting heart rate less than 120 bpm; blood pressure less than 150/90; and carboxyhemoglobin less than 3%. Eligibility for the study was confirmed through participant self-report, blood tests, and measurements taken in the laboratory prior to the controlled desaturation study.
Two methods were used to assess skin pigmentation: the Fitzpatrick Skin Type scale and spectrophotometry (CM-600D, Konica-Minolta, Tokyo, Japan). Measurements of the skin on the inner arm were taken in triplicate and averaged, and the individual typology angle calculated from the average value.
Buccal Mucosal Oximeter
The buccal mucosal oximeter is a reflectance oximeter encapsulated in the anterior curvature of a custom overlay of the maxillary dentition as shown in Figure 1. The overlay, which is customized to the user’s dentition, is made from a translucent, US pharmacopeia medical grade class VI rate polymer. The battery and circuit board lie on the mucosal aspect of the incisors and canines. The photoplethysmography (PPG) unit, a 3 × 6 × 3 mm cube, is positioned high in the buccal vestibule, 20 mm lateral to the midline and 10 mm above the inferior margin of the appliance. The position of the PPG unit in the buccal vestibule ensures good contact with the buccal mucosa and minimizes ambient light interference. Light-emitting and photo-detecting diodes are separated from the external surface of the overlay by a 0.3 mm clear wall. The three light-emitting diodes shine light at wavelengths of 525 (green), 660 (red), and 940 (infrared; IR) nm with maximal optical power output of 4.5, 7.3, and 5.3 mW, respectively, through the wall at the apposed buccal mucosa. During operation, some of the emitted light is absorbed by arterial blood and some is reflected. Oxygenated hemoglobin absorbs more infrared light than red light, while deoxygenated hemoglobin does the opposite. When more light is absorbed, it will reflect less, as detected by the photodiode in the PPG unit. The differences in light absorption and reflection allow for calculation of the percentage of oxygen in the blood by comparing the reflection levels detected by the photodiode of each of the three wavelengths. Each light signal contains an alternating component (AC) and strong offset component (DC). The calculation of SpO2 is based on the ratio of the AC to DC component of the red and infrared PPG reflected signals. Pulse rate is calculated from the AC component of the green PPG signal that corresponds to pulsatile changes in blood volume. The device detects the peaks in the green light signal, each peak representing a pulse. The time intervals between these peaks, i.e., inter-beat intervals, are averaged over a set period of time.
 |
Figure 1 The buccal mucosal oximeter device. The photoplethysmography (PPG) unit is indicated by the green arrows. |
Test Protocol
A 20-gauge Arrow® arterial line catheter (Teleflex Medical, Plymouth, MN) was inserted into the participant’s left radial artery under ultrasound guidance (Butterfly iQ+, Butterfly Network, Inc., Burlington, MA). The catheterization area was prepared using chlorhexidine 2%. A small amount (0.1–0.2 mL) of lidocaine 2% was injected into the area prior to catheterization to facilitate insertion of the arterial catheter. Arterial samples were collected in safePICO syringes (Radiometer Medical, Brønshøj, Denmark) using a SafeSet Blood Sampling Kit (ICU Medical, Inc., San Clemente, CA) with a dead space of 0.7 mL from the sampling port to the hub of the arterial line catheter. This minimized the mixing of normal saline 0.9% solution and ensured that the blood sample was free of any contaminants. Arterial samples were analyzed using two CO-oximeters (ABL837 and ABL80 Flex OSM; Radiometer Medical, Brønshøj, Denmark). The use of two CO-oximeters minimized the time for trans-wall diffusion of O2 and CO2 during the interval between sample withdrawal and analysis. The mean time between sample withdrawal and analysis was less than 60 seconds.
Testing was performed with participants semi-recumbent under non-motion conditions. Participants breathed from a blowby gas manifold with inspired gas composition controlled by the output of a dynamic end-tidal controller.12 Participants breathed exclusively nasally through an interface applied to the nares (Nuance Pro, Respironics Inc., Murraysville, PA). Gas was continuously sampled from the tubing connecting the interface to the manifold and fed to a mass spectrometer (AMIS 2000 Medical Mass Spectrometer, Innovision A/S, Odense, Denmark) for measurement of O2, CO2, and N2 fractional concentrations. These values were transmitted to a control computer for regulation of the partial pressures of end-tidal O2 (PETO2) and CO2 (PETCO2). The dynamic end-tidal forcing system compared the measured values of PETO2 and PETCO2 to the desired end-tidal targets and automatically adjusted, on a breath-by-breath basis, the inspired gas mixture as required to maintain the desired PETO2 and PETCO2. End-tidal and inspired values of O2 and CO2 were monitored continuously by study personnel.
Each study was carried out during six contiguous seven-minute periods. After an initial period of normoxia, five periods of progressive hypoxia were produced by clamping the PETO2 to predetermined targets. During each of these periods, the PETO2 was held constant at 90.1, 63.8, 53.0, 46.4, 41.6, and 37.9 torr, producing SaO2 values of approximately 97%, 92%, 87%, 82%, 77%, and 72%, respectively.13 Each PETO2 target value was pre-programmed into the dynamic end-tidal forcing system, and then held at the target value for seven minutes. After the SpO2 from a reference transmittance pulse oximeter (Model 3900, Datex-Ohmeda, Louisville, CO) reached a steady value in the first four minutes, five arterial samples were withdrawn, each at least 20 seconds apart, during the subsequent three minutes. Throughout the study, the PETCO2 was held within 3 torr of resting values to eliminate hypocapnia caused by the hypoxic ventilatory response and achieve the desired arterial oxygen desaturation profile.14 If a CO-oximeter SaO2 value below 65% was observed, the participant was returned to breathing room air and the remainder of the protocol was discontinued. A three-lead ECG was used to collect heart rate data (Micromon 7142B, Kontron Medical SAS, Toulon, France).
Two types of data pairs were obtained at the time of each blood sample. Specifically, SaO2/SpO2 data pairs were derived from the CO-oximeter and buccal mucosal oximeter, respectively, and heart rate and pulse rate data pairs were obtained from the ECG and buccal mucosal oximeter, respectively. The SaO2 pairs and pulse rate pairs were separately subjected to regression, Bland-Altman, and accuracy root-mean-square (ARMS) analyses. SaO2 pairs were excluded if a fluctuation of the reference oximeter signal in the 20 seconds preceding the start of the sampling period exceeded 3.5%, if the CO-oximeter value was less than 67%, or if the data were otherwise determined to be technically inadequate due to instrumentation or device issues.
The primary endpoints of the study were to: 1) evaluate the SpO2 accuracy of the buccal mucosal oximeter during non-motion conditions over the range of 70–100% SaO2 by comparing the buccal mucosal oximeter-derived SpO2 values to SaO2 values determined by an arterial blood sample specimen analyzed by CO-oximetry; and 2) evaluate the pulse rate accuracy of the buccal mucosal oximeter over the range collected during the study by comparison to ECG heart rate.
Results
Anthropomorphic data for the 12 participants appear in Table 1. Three participants were judged to have melanotic skin pigmentation by spectrophotometric methods and/or the Fitzpatrick scale.
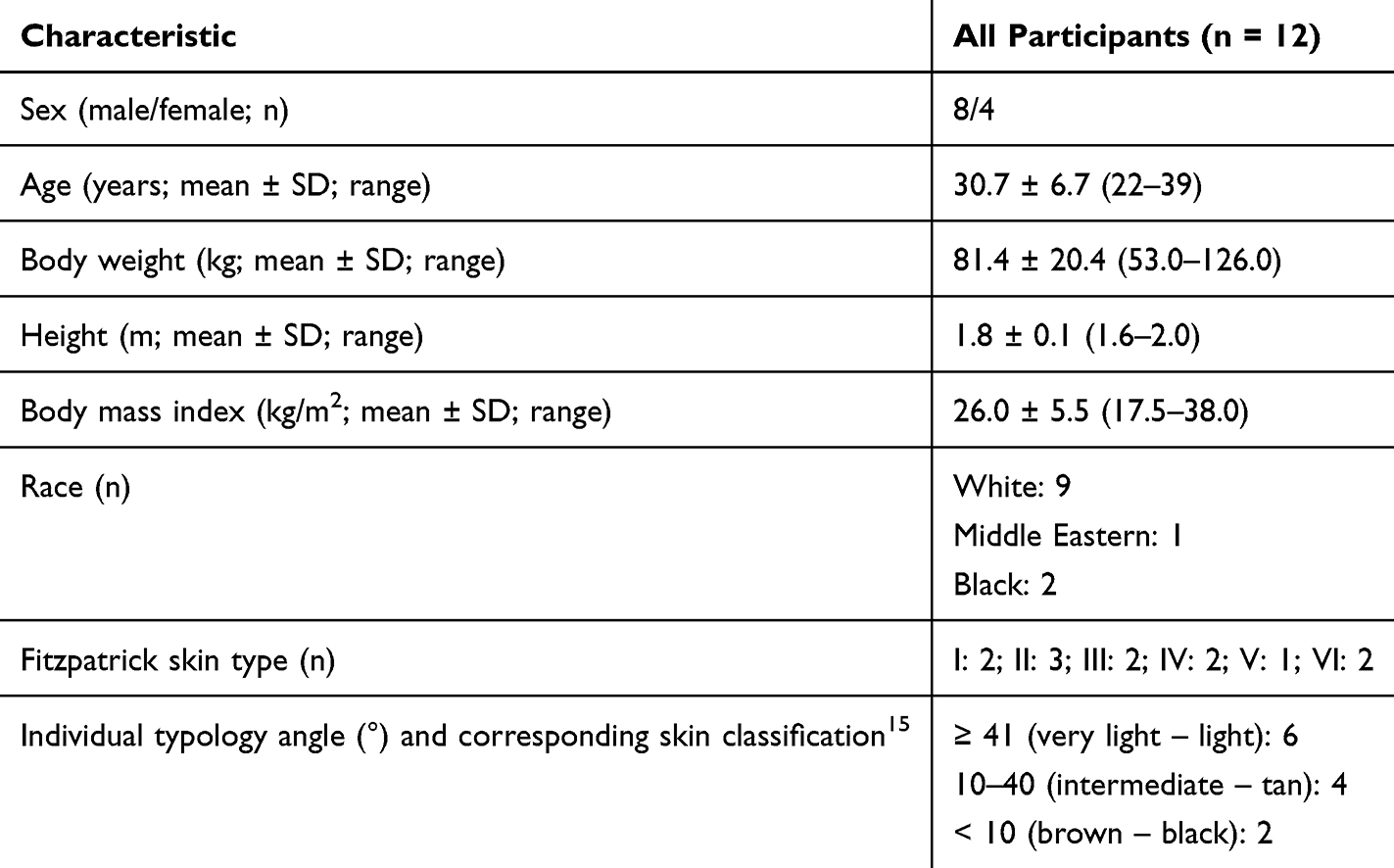 |
Table 1 Participant Baseline Data |
A total of 374 arterial samples were collected from the 12 participants. Twenty-eight data pairs were excluded due to unavailable SpO2 data attributed to a technical malfunction and an operator error. Nine data pairs were excluded due to variation greater than 3% in the reference oximeter prior to sampling during a given stage. An additional 12 data pairs were excluded due to CO-oximeter SaO2 values below 67%. As these exclusion criteria applied to SpO2 and not pulse rate, the 21 excluded data pairs described above were included in the analysis of pulse rate accuracy. Statistical analyses were performed on the remaining 325 SpO2/SaO2 and 346 pulse rate/ECG data pairs.
A representative trace of signals from the reference and buccal mucosal oximeters from a study of a single participant is provided in Figure 2. The figure shows close approximation of the two signals as the values decrease stepwise to produce six consecutive and contiguous plateaus of progressively more severe hypoxia. The mean PETO2 values and the mean CO-oximeter SaO2 values observed during each plateau for all participants are shown in Figure 3. These mean values agree well with the desired PETO2 and projected SaO2 values outlined in the Methods.
 |
Figure 2 Tracing from a single controlled desaturation study in one participant. Blue: buccal mucosal oximeter; black: reference oximeter (Datex-Ohmeda Model 3900). CO-oximeter values are indicated by pink circles. Six plateaus of controlled end-tidal PO2 are shown, each terminated by a blood pressure measurement artifact (vertical black lines). |
 |
Figure 3 Box plot of SaO2 values measured by CO-oximeter analysis of arterial blood samples drawn during each plateau versus observed PETO2 values. |
Regression and Bland-Altman analyses are shown in Figure 4 for SpO2 and Figure 5 for pulse rate. Buccal mucosal SpO2 correlated strongly with CO-oximeter SaO2 (r = 0.95). Bland-Altman analysis for SpO2/SaO2 pairs showed a bias of 0.72 and upper and lower 95% limits of agreement of 6.31 and −4.86, respectively. Buccal mucosal oximeter pulse rate correlated strongly with ECG heart rate (r = 0.99). Bland-Altman analysis for pulse rate/ECG pairs showed a bias of 0.30 and upper and lower 95% limits of agreement of 4.34 and −3.73, respectively.
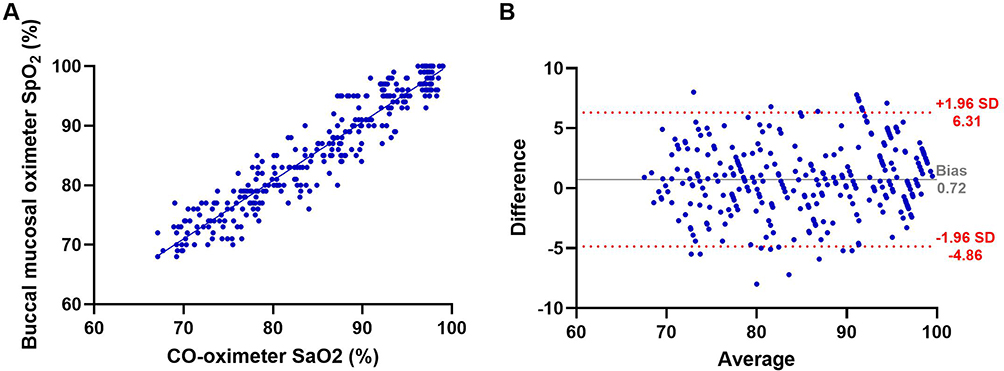 |
Figure 4 (A) Linear regression through all valid data pairs for SaO2 measured by CO-oximetry and SpO2 of the simultaneously recorded buccal mucosal oximeter signal (r = 0.95; n = 325); (B) Bland-Altman plot of agreement of CO-oximeter SaO2 and buccal mucosal oximeter SpO2 data pairs (bias: 0.72; upper 95% limit of agreement: 6.31; lower 95% limit of agreement: −4.86; n = 325). Bias is indicated by the horizontal grey line; upper and lower 95% limits of agreement are indicated by the red dashed lines. |
 |
Figure 5 (A) Linear regression through all valid data pairs for heart rate measured by the ECG and pulse rate of the simultaneously recorded buccal mucosal oximeter signal (r = 0.99; n = 346); (B) Bland-Altman plot of agreement of ECG heart rate and buccal mucosal oximeter pulse rate data pairs (bias: 0.30; upper 95% limit of agreement: 4.34; lower 95% limit of agreement: −3.73; n = 346). Bias is indicated by the horizontal grey line; upper and lower 95% limits of agreement are indicated by the red dashed lines. |
The ARMS for SpO2 was 2.94% over the range of 70–100% SaO2. The ARMS by decade is shown in Table 2. The ARMS for pulse rate was 2.08 bpm over the range observed in the study (50–109 bpm).
 |
Table 2 SpO2 Accuracy of the Buccal Mucosal Oximeter Over the Full Range Tested (70–100% SaO2) and by Decade |
Discussion
We describe here a novel oximeter design, namely: a reflectance pulse oximeter encapsulated in a custom overlay of the maxillary dentition with the upper lip buccal mucosa being the reflective tissue. This design may confer several advantages over conventional oximeters, transmittance or reflectance. Embedding the oximeter in an overlay of the maxillary dentition provides a self-contained, isolated location for the PPG, battery, and circuit board while producing no discomfort to the user. Apposing the optical surface of the PPG to the mucosa of the upper lip provides a highly vascular target region for photometric measurements producing relatively large pulse modulation in the reflected optical signals. Locating the optical unit high in the buccal vestibule behind the upper lip provides mechanical stability and minimizes the possibility of ambient light contamination. Furthermore, this region has good thermal stability, and the mucosa contains relatively little melanin pigmentation compared to the skin.
In addition to overcoming these limitations, the buccal mucosal oximeter’s estimates of SaO2 and pulse rate are reassuringly accurate and meet the performance goals of the United States Food and Drug Administration for reflectance pulse oximeters.16
A potential limitation of the current oximeter design, yet to be fully evaluated is the lack of attachment between the optical surface of the PPG and the vestibular surface of the mucosa. Protrusion of the PPG optical surface beyond the anterior overlay surface acts to stabilize the two surfaces, but movement may cause artifacts in the recorded SpO2 values. While no issues with signal integrity were present in our study, further investigation is needed to determine the accuracy of the device under motion conditions. Another potential limitation, seen in most conventional oximeters, is contamination of ambient light reaching the PPG optical surface. However, such ambient light contamination was not a source of error in our study, even in participants with relatively short upper lips.
The most significant design challenge posed by buccal mucosal oximetry is to minimize the distance between the PPG diodes and the biological surface, the so-called air gap. This is a cardinal challenge in most oximetry applications.17 The design and technology of the buccal mucosal oximeter overcomes this problem by covering the PPG diodes with a thin, optically competent wall with satisfactory optical properties.
The buccal mucosal oximeter is a personalized, reusable device designed to be used for long-term, continuous monitoring of sleep apnea or other pulmonary diseases. Due to it being a custom device, it is likely not cost-effective for use in single-night sleep testing or other limited duration situations. Additional studies are required to assess the long-term accuracy and stability of the buccal mucosal oximeter in a real-world setting as the present study assessed accuracy of the device in comparison with a gold standard under experimental conditions.
Conclusion
A rigorous evaluation of a novel buccal mucosal pulse oximeter reveals strong accuracy of an oximeter suitable for nightly monitoring of arterial oxyhemoglobin saturation. This buccal mucosal oximeter offers promising clinical utility in the management of patients experiencing sleep-induced hypoxia by providing comfortable, personalized, long-term monitoring of arterial oxyhemoglobin saturation. Of particular interest is the application of this oximeter in patients with OSA, where studies have shown substantial night-to-night variation in SaO2, suggesting that multi-night monitoring might contribute to clinical management.
Data Sharing Statement
The dataset presented in this article is not readily available due to reasons related to the status of regulatory approval. Requests to access the dataset should be directed to the corresponding author (Dr. Marc J. Poulin; [email protected]).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Conjoint Health Research Ethics Board of the University of Calgary (protocol REB23-1003, approved April 2, 2024). The study approved Investigational Testing Authorization from Health Canada (ITA #373369, approved March 21, 2024).
Acknowledgments
The authors thank Dr. Trevor Day for his valuable input on study design, Ms. Randa Salem and Ms. Mylinh Hoang for providing Butterfly IQ+ ultrasound devices for the study, and Dr. Martin MacInnis for providing a CO-oximeter for the study.
Funding
This research was funded by ProSomnus Sleep Technologies.
Disclosure
C.S., S.M.B., M.P., A.C., S.B., B.H., and J.M.R. have no conflicts of interest to declare for this work. TRT was funded by the Natural Sciences and Engineering Research Council (NSERC) of Canada- Canadian Graduate Scholarship - doctoral award during the conduct of this research. This funding paid for his stipend as a graduate student. L.T., S.A., and S.R. received payment in exchange for services provided for the study from Prosomnus. M.J.P. received funding from ProSomnus Sleep Technologies to conduct the study. G.D., M.L., E.V.M., and J.E.R are employees of ProSomnus Sleep Technologies and were involved in study design, data analysis, data collection, data interpretation, and writing of the manuscript. In addition, G.D. has a patent “Methods for sensing physiological change and related devices” pending to ProSomnus Sleep Technologies and M.L. has a patent 2024-10-07 Filed Provisional Application 133174-0012PV01(8707877.1) pending to ProSomnus Sleep Technologies.
References
1. Aguiló J, Moussaoui D, Chon K, Bailón RE. Robust, reliable, and continuous assessment in health: the challenge of wearable and remote technologies. Front Physiol. 2023;14:1281426. doi:10.3389/fphys.2023.1281426
2. Stepnowsky C, Zamora T, Barker R, Liu L, Sarmiento K. Accuracy of positive airway pressure device-measured apneas and hypopneas: role in treatment followup. Sleep Disord. 2013;2013:314589. doi:10.1155/2013/314589
3. Azarbarzin A, Sands SA, Stone KL, et al. The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the osteoporotic fractures in men study and the sleep heart health study. Eur Heart J. 2019;40(14):1149–1157. doi:10.1093/eurheartj/ehy624
4. Trzepizur W, Blanchard M, Ganem T, et al. Sleep apnea-specific hypoxic burden, symptom subtypes, and risk of cardiovascular events and all-cause mortality. Am J Respir Crit Care Med. 2022;205(1):108–117. doi:10.1164/rccm.202105-1274OC
5. Stöberl AS, Schwarz EI, Haile SR, et al. Night-to-night variability of obstructive sleep apnea. J Sleep Res. 2017;26(6):782–788. doi:10.1111/jsr.12558
6. Petterson MT, Begnoche VL, Graybeal JM. The effect of motion on pulse oximetry and its clinical significance. Anesth Analg. 2007;105(6 Suppl):S78–S84. doi:10.1213/01.ane.0000278134.47777.a5
7. Jubran A. Pulse oximetry. Crit Care. 2015;19(1):272. doi:10.1186/s13054-015-0984-8
8. Tekin K, Karadogan M, Gunaydin S, Kismet K. Everything about pulse oximetry-part 1: history, principles, advantages, limitations, inaccuracies, cost analysis, the level of knowledge about pulse oximeter among clinicians, and pulse oximetry versus tissue oximetry. J Intensive Care Med. 2023;38(9):775–784. doi:10.1177/08850666231185752
9. Al-Halawani R, Charlton PH, Qassem M, Kyriacou PA. A review of the effect of skin pigmentation on pulse oximeter accuracy. Physiol Meas. 2023;44(5):05TR01. doi:10.1088/1361-6579/acd51a
10. Cabanas AM, Fuentes-Guajardo M, Latorre K, León D, Martín-Escudero P. Skin pigmentation influence on pulse oximetry accuracy: a systematic review and bibliometric analysis. Sensors. 2022;22(9):3402. doi:10.3390/s22093402
11. ISO 80601-2-61:2017. Medical electrical equipment - Part 2-61: particular requirements for basic safety and essential performance of pulse oximeter equipment. Published online 2017.
12. Kolb JC, Ainslie PN, Ide K, Poulin MJ. Protocol to measure acute cerebrovascular and ventilatory responses to isocapnic hypoxia in humans. Respir Physiol Neurobiol. 2004;141(2):191–199. doi:10.1016/j.resp.2004.04.014
13. Severinghaus JW. Simple, accurate equations for human blood O2 dissociation computations. J Appl Physiol. 1979;46(3):599–602. doi:10.1152/jappl.1979.46.3.599
14. Steinback CD, Poulin MJ. Ventilatory responses to isocapnic and poikilocapnic hypoxia in humans. Respir Physiol Neurobiol. 2007;155(2):104–113. doi:10.1016/j.resp.2006.05.006
15. Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(Suppl 3):33–40. doi:10.1111/bjd.12529
16. The Food and Drug Administration (FDA). Pulse Oximeters - Premarket Notification Submissions [510(k)s]: Guidance for Industry and Food and Drug Administration Staff.
17. Barker SJ. “Motion-resistant” pulse oximetry: a comparison of new and old models. Anesth Analg. 2002;95(4):967–972. doi:10.1097/00000539-200210000-00033
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.