Back to Journals » Advances in Medical Education and Practice » Volume 17
A Blended Case-Based and Practical Training Framework for Graduate Ultrasound Education: A Perspective on Competency-Based Instruction
Authors Liu S, Zhu K ![]() , Ran Z
, Ran Z ![]() , Zeng F
, Zeng F ![]() , Zhu M
, Zhu M ![]() , Wang Y
, Wang Y ![]() , Wang D
, Wang D ![]()
Received 27 December 2025
Accepted for publication 28 March 2026
Published 17 April 2026 Volume 2026:17 592119
DOI https://doi.org/10.2147/AMEP.S592119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Shuang Liu,1 Kai Zhu,2 Zhicheng Ran,1 Fanfeng Zeng,1 Menghan Zhu,1 Yan Wang,1 Dongmo Wang1
1Department of Ultrasound, The Second Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, People’s Republic of China; 2Department of Radiology, The First Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, People’s Republic of China
Correspondence: Dongmo Wang, Department of Ultrasound, The Second Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, People’s Republic of China, Email [email protected]
Abstract: With the widespread application of ultrasound in disease screening, clinical diagnosis, and efficacy monitoring, the traditional model in which ultrasound examinations and diagnoses are independently performed by ultrasound physicians has increasingly struggled to meet the growing clinical demands. The gradual introduction and standardized development of the professional role of ultrasound technicians have imposed new training requirements on graduate education in medical imaging technology. Against this background, how to effectively cultivate students’ clinical thinking and technical operation abilities at the graduate level has become a significant educational challenge in ultrasound teaching reform. Based on the above educational needs, this paper proposes a competency-oriented conceptual teaching framework that integrates case-based teaching with structured practical training for ultrasound instruction in graduate programs of medical imaging technology. This framework is based on competency-based education theory and aims to bridge the gap between theoretical knowledge and practical operational skills. The framework systematically elaborates on principles for case selection and design, practical training content, and teaching methods, while constructing a closed-loop teaching structure of ‘case introduction—group discussion—skills training—reflection and summary. Meanwhile, this paper analyzes the key issues that may arise during the implementation of integ rated teaching, including complex teaching organization processes, uneven student participation, and insufficient transformation of learning outcomes, and proposes corresponding strategies, such as standardized process design, formative evaluation mechanisms, and diversified assessment methods. From the perspectives of theory and teaching design, this paper proposes a structured teaching model to provide a reference for graduate ultrasound curriculum development and teaching reform, and lays a foundation for the further practice and validation of a competency-oriented training model for ultrasound technicians.
Keywords: ultrasonography, medical education, problem-based learning, clinical practice, graduate students
Introduction
In recent years, with the continuous improvement of China’s healthcare service system and the rising health awareness among the public, ultrasound examinations have been widely adopted in disease screening, clinical diagnosis, and treatment efficacy assessment due to their non-invasive, convenient, and real-time imaging advantages.1 Traditionally, ultrasound examinations have been conducted and interpreted solely by sonographers. However, the sustained rapid growth in clinical demand for ultrasound services has exposed inefficiencies and resource constraints within this traditional model,2 making it increasingly difficult to meet the needs of the rapidly advancing field of ultrasound medicine. In contrast, developed countries like the United States have established a mature professional system for ultrasound technicians.3 Their competency has gained widespread recognition through long-term practice, significantly alleviating the supply-demand imbalance in ultrasound services while enhancing the discipline’s operational efficiency. Against this background, China has also gradually initiated standardized training programs for ultrasound technologists.4,5 However, compared with more mature international frameworks, the training of ultrasound technologists in China is still in a continuous development stage in terms of educational system structure, curriculum standards, and competency evaluation mechanisms, with certain differences existing among various institutions and regions.6 This evolving pattern brings new challenges and opportunities to the graduate education of medical imaging technology. In this context, it is necessary to explore a graduate-level ultrasound education model that can systematically integrate clinical thinking with technical skills training. This article aims to propose a competency-based conceptual education framework, combining case-based teaching with structured practical training, applied to the cultivation of graduate students in medical imaging technology. As shown in Figure 1, the framework is based on competency-oriented education theory and student-centered learning concepts, aiming to bridge the gap between theoretical teaching and practical operational skills in current training practices. This article presents a model with theoretical basis and instructional structure design, intended to provide guidance for curriculum development and teaching reform in graduate-level ultrasound education.
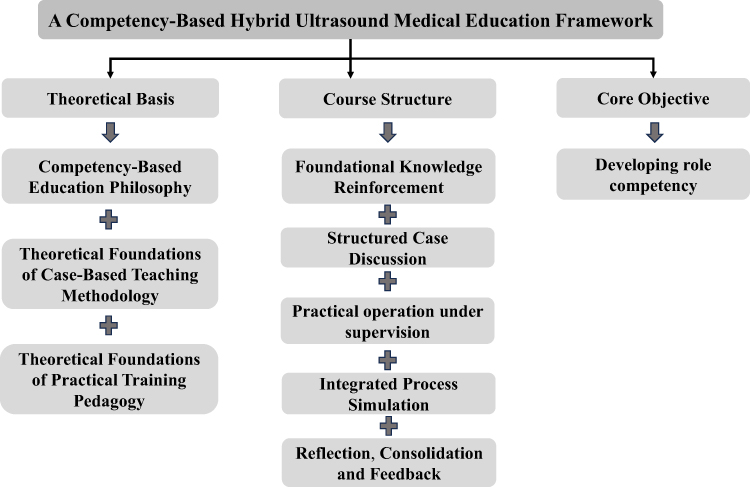 |
Figure 1 A Competency-Based Hybrid Ultrasound Medical Education Framework. |
Educational Philosophy and Theoretical Foundations
Competency-Based Education
Competency-based education has become a core concept in modern medical education.7 International educational bodies such as the World Federation for Medical Education (WFME) and the Accreditation Council for Graduate Medical Education (ACGME) emphasize outcomes-oriented training models that prioritize quantifiable competencies and align curricula with professional roles.8 CBE represents an educational paradigm shift from knowledge-centered to competency-centered learning. Its core focus moves beyond mere knowledge acquisition to emphasize observable, measurable competencies, including technical skills, clinical reasoning abilities, communication skills, and professional conduct.9 Competencies must be clearly defined, systematically developed, and measured through structured assessment tools. In ultrasound education, competency extends beyond image acquisition to encompass interpreting dynamic images in clinical contexts, effectively communicating findings, and adhering to safety and ethical standards. Thus, any pedagogical reform must explicitly define competency dimensions and align instructional strategies with evaluation systems. The integrated teaching framework proposed in this study embeds competency concepts into the teaching process, introducing structured assessment mechanisms in both formative and summative evaluations to ensure that training objectives are measurable and aligned with clinical needs.10
Theoretical Foundations
Case-based teaching effectively stimulates student engagement by presenting realistic, contextual learning scenarios, encouraging active participation and enhancing knowledge retention.11 By simulating authentic clinical situations, this approach focuses on developing students’ clinical reasoning and comprehensive judgment skills. It enables them to flexibly apply theoretical knowledge during complex ultrasound diagnostics, improving problem-solving abilities and bridging the gap between theory and practice.12 Ultrasound medicine is a discipline highly dependent on integrating image interpretation with clinical context. Traditional teaching often emphasizes knowledge transmission, with students passively receiving information. By introducing real or simulated ultrasound case scenarios, case-based teaching guides students through organizing medical histories, analyzing images, establishing diagnoses, and planning scanning approaches. This effectively trains their clinical reasoning and independent judgment skills. The method emphasizes “learning by doing,” aligning perfectly with the goal of cultivating clinical application abilities and job competency, laying a solid foundation for students’ future work on the clinical frontlines.
The application of practical training teaching methods (abbreviated as practical training methods) in medical education has not only significantly enhanced students’ learning motivation and autonomy but also promoted the deep integration of theoretical knowledge with clinical practice.13 During training, students engage in repeated hands-on procedures and critical thinking within authentic clinical scenarios, thereby effectively improving their knowledge retention and skill proficiency.14 This process holds significant importance for cultivating medical professionals with comprehensive competencies and clinical competence, implementing effective teaching supervision mechanisms, and advancing the organic integration of theory and practice in medical education.15 Ultrasound operation involves technical actions such as probe positioning, image acquisition, and equipment adjustment, requiring extensive repetitive practice to develop muscle memory and standardized procedures.16 Therefore, hands-on training is a core component for achieving job competency.
Competency Framework for Graduate Ultrasound Education
Graduate ultrasound education must be systematically designed around clearly defined and clinically relevant competency domains.17 Based on the clinical role of sonographers and the instructional elements of the original teaching model, four interconnected core competency domains can be identified: image analysis skills, technical proficiency, communication abilities, and professional ethics. These domains collectively constitute the expected learning outcomes for graduate training and serve as the organizational framework for aligning curriculum design and assessment systems.18,19
Image Analysis
Image analysis forms the cognitive core of ultrasound practice. Unlike static imaging modalities, ultrasound examinations are dynamic and operator-dependent, requiring real-time decision-making and integration of clinical information during scanning.20 Therefore, trainees must develop the ability to synthesize patient history, clinical presentation, and dynamic imaging changes throughout the procedure.21 This competency encompasses: systematically organizing and analyzing medical history prior to scanning; identifying and accurately describing key imaging features; precisely localizing lesions; formulating diagnostic hypotheses and conducting differential diagnosis analysis; and synthesizing findings into structured, clinically meaningful diagnostic reports. The blended teaching model reinforces clinical reasoning through structured case discussions, multidimensional imaging feature analysis, and reflective summarization sessions. By guiding students to connect pathophysiological mechanisms with ultrasound manifestations, it prevents fragmented knowledge and promotes the formation of comprehensive diagnostic reasoning. Concurrently, the evaluation system provides observable and measurable assessments of clinical reasoning abilities through metrics such as imaging interpretation accuracy, diagnostic logical rigor, and report standardization—moving beyond abstract assumptions.
Technical Skills Competency
Ultrasound examination is inherently a task that relies heavily on operational techniques. Acquiring high-quality images depends on factors such as probe placement, scanning angle adjustment, equipment parameter optimization, and patient positioning cooperation. Therefore, technical skills form the operational foundation of ultrasound competency. This domain encompasses: standardized probe manipulation and ergonomic posture control; appropriate selection of probe types based on clinical indications; adjustment of imaging parameters (gain, depth, focus, Doppler settings, etc).; acquisition of standard planes and comprehensive anatomical views; adherence to safety protocols and infection control standards. The practical training component within blended learning models emphasizes repetitive hands-on practice under instructor supervision. Simulation training and structured skill drills help students develop operational proficiency and “muscle memory.” Real-time monitoring and immediate feedback mechanisms enhance skill accuracy and operational efficiency. Periodic skill assessments evaluate adherence to protocols, image quality, procedural completeness, and time management. Through systematic training, technical competence progressively improves, aligning with real clinical workflow standards.
Communication Skills
Effective ultrasound practice relies not only on technical proficiency but also on strong patient interaction and teamwork abilities. Communication skills ensure examinations proceed in a respectful, safe, and professional manner. This domain encompasses: conducting structured history-taking (chief complaint, present illness, past medical history, personal history, and family history); clearly explaining examination procedures and precautions; demonstrating empathy and active listening; conveying findings clearly and systematically; and effectively participating in team-based clinical workflows. The integrated teaching model employs role-playing group training and simulated clinical scenarios, enabling students to practice patient communication and teamwork in a controlled environment.22 Structured evaluation criteria (eg. completeness of information gathering, appropriateness of expression, demonstration of empathy, and professional demeanor) facilitate systematic assessment of communication skills, moving beyond reliance on informal observation. By embedding communication training within case discussions and practical simulations, the model ensures interpersonal competencies develop concurrently with cognitive and technical abilities.
Professional Competence
Professional competence embodies the ethical and behavioral dimensions of ultrasound competency, encompassing adherence to clinical protocols, respect for patient dignity, safety awareness, and reflective practice. Core elements include: strict compliance with clinical safety protocols during equipment operation; safeguarding patient privacy and upholding medical ethics; demonstrating accountability in report writing; responding appropriately to unexpected clinical situations; and engaging in reflective learning and continuous improvement. The evaluation system ensures professional competence is systematically assessed through comprehensive evaluation of adherence to safety protocols, professional conduct, emergency response capabilities, and completion of learning reflection logs.23,24 Simulated emergency scenarios (eg., equipment malfunction or patient discomfort) assess students’ adaptability and decision-making under pressure. Integrating professional competence into formative and summative evaluations reinforces the educational principle that “technical proficiency must be balanced with ethical responsibility.”
Course Structure Design
The course structure of this integrated teaching model ensures systematic alignment among competency objectives, teaching strategies, and assessment mechanisms.25 Unlike treating theoretical instruction and practical training as separate modules, this framework integrates both into a progressive, competency-oriented holistic structure. Courses are organized around clearly defined learning objectives and explicit competency mapping.
Learning Objectives
Guided by competency-based education principles, learning objectives are structured across three dimensions: knowledge, technical skills, and professional attitudes. These objectives reflect both clinical practice requirements and graduate-level training standards.
Knowledge Objectives: Students should understand the principles of ultrasound physics, image formation mechanisms, and fundamental instrumentation; recognize common pathological imaging features and their clinical significance; and master standardized scanning protocols and diagnostic criteria. These objectives underpin foundational theory instruction and form the cognitive basis for developing image analysis capabilities.
Technical Skills Objectives: Students should be able to independently perform standardized ultrasound scanning procedures; select appropriate transducers based on clinical indications and adjust equipment parameters rationally; acquire high-quality diagnostic images while adhering to operational safety protocols; and complete the entire workflow from patient positioning to image optimization. This section emphasizes operational proficiency and procedural standardization, highlighting the development of psychomotor skills.
Professional and Attitudinal Objectives: Students should demonstrate effective patient communication skills and humanistic care awareness; write standardized, logically coherent ultrasound diagnostic reports; and exhibit professional responsibility and ethical awareness during examinations. These objectives transcend mere technical execution, encompassing communication abilities and professional ethics.
Competency Mapping
To ensure intrinsic consistency between teaching and assessment, the curriculum design incorporates a clear competency mapping mechanism. Each core competency domain is systematically aligned with specific teaching methods and assessment tools. For example: Image analysis skills are primarily developed through structured case discussions and evaluated via case analysis tasks and report writing;26 technical skills are reinforced through simulation training and supervised hands-on practice, assessed using structured performance rubrics; communication skills and professional conduct are cultivated through role-play training and reflective learning, evaluated using clinical assessment scales.
Curriculum Outline Structure
The course outline adopts a progressive five-stage structure that simulates real clinical ultrasound workflows, promoting the gradual integration of knowledge, skills, and critical thinking abilities.
Stage 1: Foundational Knowledge Consolidation
This stage emphasizes reinforcing theoretical foundations, including ultrasound physics, instrument principles, scanning protocols, and imaging characteristics of common diseases. Learning is supported by multimedia resources such as image databases, video demonstrations, and case summaries.27 This stage ensures students establish the cognitive framework required for subsequent clinical applications.
Stage 2: Structured Case Discussions
Real or simulated clinical cases are introduced, covering common, prevalent, and challenging conditions. Under instructor guidance, students analyze patient histories, interpret imaging findings, formulate diagnostic hypotheses, and design scanning strategies. This stage emphasizes contextualized learning and the development of clinical reasoning skills.
Stage 3: Supervised Practical Training
Following cognitive preparation, students advance to hands-on training. Instructors first demonstrate standardized procedures, then provide supervised guidance with real-time feedback and corrections on probe placement, parameter adjustments, and image acquisition.28
Repetitive practice enhances skill proficiency and achieves procedural standardization.
Phase 4: Integrated Workflow Simulation
Students complete the full ultrasound workflow: history taking, equipment preparation, image acquisition, image interpretation, and structured report writing. By integrating these components, students experience the closed-loop structure of real clinical ultrasound practice, strengthening the synergy between cognitive reasoning and technical execution.
Phase 5: Reflection, Consolidation, and Feedback
The final phase emphasizes reflection and continuous improvement. Students document challenges and insights in learning journals, while instructors provide structured feedback based on formative assessments and peer observations. This phase completes the educational cycle, facilitating long-term knowledge internalization and stable competency development.
Instructional Design
Principles for Case Selection and Design
High-quality teaching cases form the foundation of blended learning and should embody authenticity, typicality, and educational value.29 Case selection should encompass common diseases, prevalent conditions, and complex challenging cases. This progressive structure facilitates the gradual development of students’ diagnostic reasoning, advancing from basic recognition skills to comprehensive analytical abilities. Design should emphasize case completeness and diagnostic process coherence, integrating multidimensional information such as clinical manifestations (patient symptoms and signs), imaging characteristics (including typical ultrasound features and cross-sectional images), and diagnostic reasoning. Each case should be accompanied by multimedia resources, including imaging studies, video materials, and case summaries. Static ultrasound images facilitate detailed anatomical analysis, while dynamic video clips aid in understanding lesion progression and probe manipulation techniques. Concise case summaries provide a structured overview of diagnostic key points and reporting standards.
Practical Training Content and Methods
Practical training courses should incorporate specific case studies, enabling students to integrate theory with practice during their learning. Key training focuses include: standardized acquisition of ultrasound images, proficient use of equipment, recognition of common images and development of diagnostic reasoning, as well as completion of a comprehensive ultrasound report.30,31 Through these exercises, students progressively master the entire workflow—from operation and diagnosis to report writing—truly uniting knowledge with skills. In teaching methodologies, diverse approaches can be employed to enhance realism and engagement. For instance, students can observe and practice in clinical settings to directly understand ultrasound examination procedures.17 Instructors can guide students through repeated hands-on practice using simulated scenarios and interactive exercises, enabling timely identification and correction of errors. Additionally, group collaboration can be introduced, where students divide tasks and simulate clinical team workflows.32 This not only hones communication and teamwork skills but also accelerates adaptation to clinical environments. Instructors should also utilize case studies to guide students in multi-faceted analysis—integrating medical history, symptoms, and imaging characteristics to foster comprehensive clinical reasoning. Coupled with periodic assessments and feedback evaluating procedural compliance, image quality, diagnostic accuracy, and report completeness, this approach drives continuous improvement.
Implementation Process
In implementing blended learning, the “design-implementation-feedback-optimization” cycle must be consistently applied throughout to form a complete teaching loop.33 This ensures learning objectives are genuinely achieved and continuously refined through practice. The instructional implementation process, as illustrated in Figure 2, encompasses multiple critical stages: case introduction, scenario construction, case discussion, skill practice, reflective reporting, and instructor evaluation. This closed-loop approach gradually develops replicable and adaptable teaching models, enabling steady and sustained improvements in course quality.
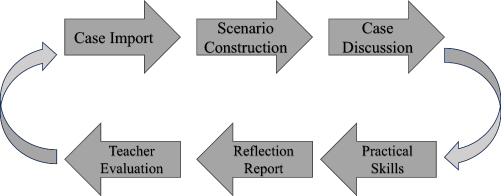 |
Figure 2 Closed-loop teaching process in blended learning models. |
Challenges and Countermeasures in Teaching Practice
The Integration of Teaching Processes Is Complex
In deeply integrating case-based teaching with practical training, instructional organization must encompass multiple critical stages, including case introduction, scenario construction, case discussion, skill practice, reflective reporting, and instructor evaluation. While this multi-module, multi-stage instructional design comprehensively enhances students’ clinical reasoning and operational skills, it presents significant challenges in practice: First, the numerous transitional links and complex workflow may lead to unstable teaching pacing, redundant segments, or blurred instructional focus without systematic design and unified rhythm control. Second, differences in teaching philosophies, content interpretation, and instructional approaches among various teaching teams may compromise overall teaching consistency and student learning experiences, particularly evident in collaborative or interdisciplinary teaching settings. To address these issues, teaching and research offices or educational administrative departments should spearhead the development of standardized teaching process templates. This template should outline core objectives, content sequencing, teaching method selections, and evaluation mechanisms for each instructional phase, emphasizing implementation priorities and considerations at every stage to ensure content flows seamlessly and progressively.
Uneven Levels of Student Engagement
The integrated teaching model emphasizes a “student-centered” pedagogical philosophy, advocating for the full development of students’ initiative, exploratory spirit, and collaborative abilities through guidance in authentic contexts and practical tasks. However, in actual teaching practice, significant disparities exist among students in terms of knowledge foundations, learning capacities, desire for expression, and willingness to participate,34 presenting practical challenges to the effective implementation of integrated teaching. To effectively enhance overall student engagement and motivation, structured formative assessments and diversified evaluation mechanisms should first be integrated into the instructional system.35 Assessment should focus not only on final outcomes but also on comprehensive aspects such as proactive involvement, problem analysis, and solution capabilities demonstrated throughout the learning process. Linking evaluation results to course grades, learning portfolios, or phased incentives can institutionally stimulate students’ initiative and sense of responsibility. In the classroom, teachers should actively assume the roles of “facilitators” and “coordinators,” acknowledging individual differences and adapting arrangements flexibly. They should encourage relatively introverted or academically struggling students to engage in appropriate hands-on practice. Through sustained attention and personalized guidance, the participation enthusiasm and learning confidence of every student can be gradually enhanced, transforming inclusive education into a truly student-centered platform where everyone has opportunities and experiences growth.
Evaluation System
To comprehensively evaluate the teaching effectiveness of the integrated case-based and practical training model, an educational assessment system centered on “multidimensional evaluation” and “process-outcome integration” should be established.36 This system should encompass multiple dimensions including knowledge mastery, skill proficiency, critical thinking abilities, teamwork, and clinical competence, thereby reflecting the developmental trajectory of graduate students throughout their educational journey.
Formative Assessment
Integrated teaching emphasizes process participation and continuous development, thus incorporating elements such as learning attitudes during instruction into assessment (Table 1). Specific methods include:①Classroom Performance Records, Instructors document the quality and frequency of student contributions during case analysis and clinical discussions;②Learning journals, Students write reflective summaries at each stage, documenting practical insights and cognitive gains;③ Periodic task scoring, Quantified assessment of stage outcomes through methods like in-class quizzes.
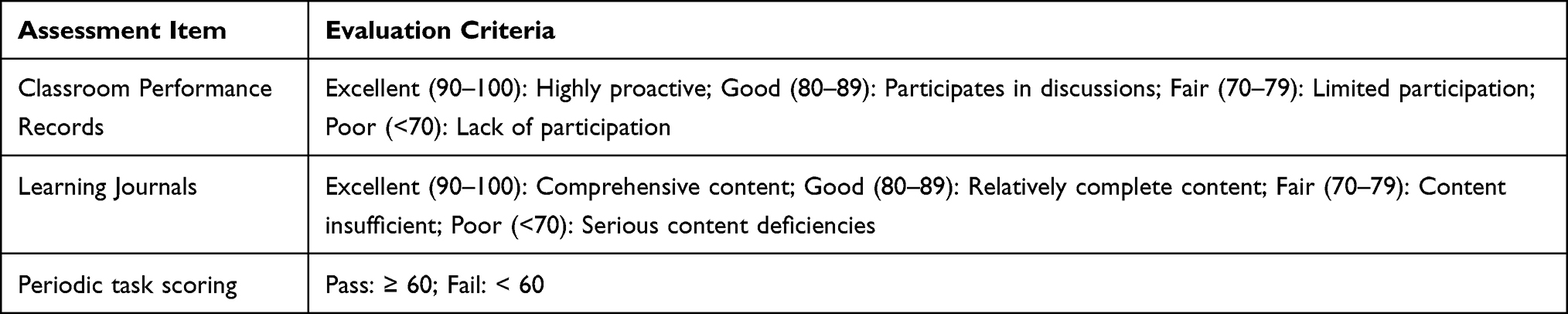 |
Table 1 Formative Assessment Checklist |
Summative Assessment
At the conclusion of integrated teaching, a systematic and comprehensive evaluation of student learning outcomes should be conducted, with the core objective being to thoroughly assess students’ learning achievements. Clinical skills assessments may be implemented,37 incorporating multifaceted evaluation criteria to assess students’ performance in operational skills, professional competence, and clinical adaptability. This establishes a holistic, multidimensional teaching evaluation system that fully embodies the principle of integrating process and outcome (Table 2). Specific methods are as follows:
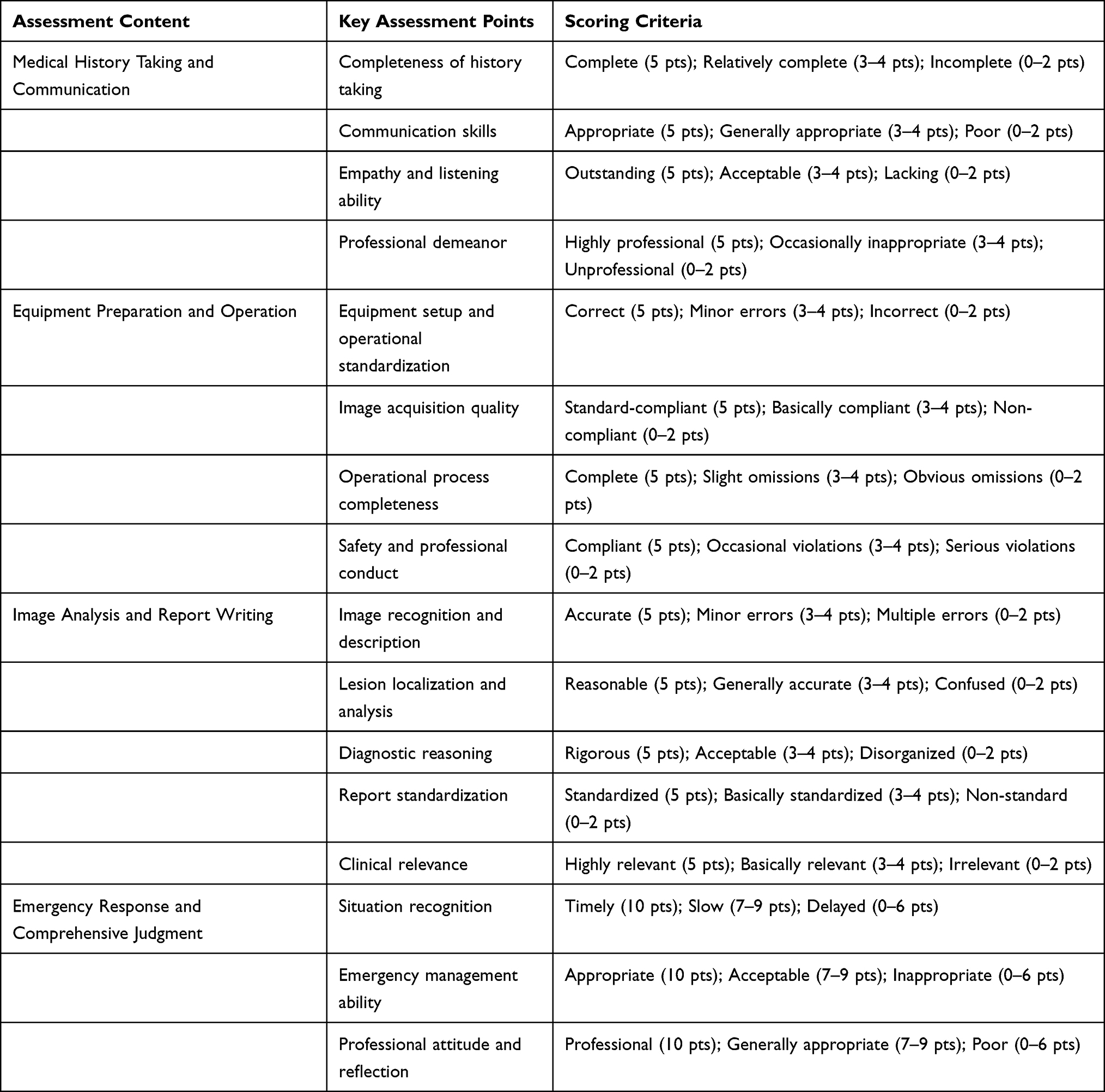 |
Table 2 Clinical Skills Assessment Form |
Medical History Taking and Communication—Assessing Professional Competence
The assessment primarily evaluates students’ communication skills and humanistic care awareness. Evaluation components include conducting a simulated patient history interview (covering chief complaint, present illness, past medical history, personal history, and family history), while simultaneously assessing students’ communication techniques, verbal expression, listening abilities, and professional etiquette. Scoring criteria encompass completeness of information gathering, communication effectiveness, and adherence to professional standards, aiming to evaluate students’ interpersonal communication and professional competence.
Equipment Preparation and Operation—Assessing Professional Operational Skills
The assessment focuses on evaluating students’ proficiency in the standardized use and operation of ultrasound equipment. Evaluation components include device startup, parameter settings, probe selection, patient positioning, image acquisition, and adherence to safety protocols. Scoring criteria comprehensively assess procedural compliance, image quality, time efficiency, and safety awareness, reflecting students’ professional competency in real clinical practice.
Image Analysis Report—Assessing Analytical Skills
Through typical case studies or ultrasound images, assess students’ abilities in image recognition, lesion localization, and diagnostic analysis. Students must complete image observation, feature description, diagnostic reasoning, and standardized report writing within a specified time limit. Scoring criteria include image interpretation accuracy, report standardization, logical reasoning, and clinical relevance to comprehensively evaluate students’ ability to apply theoretical knowledge to clinical practice.
Adaptability and Comprehensive Judgment—Assessing Overall Competence
By simulating complex or unexpected clinical scenarios (such as equipment malfunctions, patient discomfort, or limited image quality), this assessment focuses on evaluating students’ emergency response capabilities, problem-solving skills, and comprehensive decision-making abilities. Scoring criteria encompass reaction speed, treatment strategies, and professional attitude, reflecting students’ overall competence in integrating knowledge and skills within real clinical settings.
In summary, this evaluation system employs a “multi-station, tiered, comprehensive” design that balances multidimensional assessment criteria—theoretical knowledge, practical skills, and professional conduct—transitioning from singular outcome-based evaluation to a combined “process-outcome” approach. It provides a systematic foundation for scientifically assessing teaching effectiveness through integrated learning outcomes.
Teaching Feedback and Continuous Improvement Mechanism
Establish a teaching feedback and continuous improvement mechanism to promptly gather feedback on student learning progress and teaching effectiveness, identify issues in course design and implementation, and make targeted adjustments to teaching content and methods.38 This approach aims to meet students’ individual needs and promote faculty professional development. Through a feedback-improvement cycle, it achieves continuous enhancement and optimization of teaching quality. Specific methods are as follows: ①Student Satisfaction Survey, Collect student feedback on course content, organization, and instructor performance; ②Teaching Research and Revision, Periodically update the teaching case repository, practical training procedures, and evaluation criteria based on assessment data to drive continuous course improvement.
Conclusion and Outlook
The integrated case-based and hands-on training model offers an innovative and effective teaching approach for ultrasound instruction in medical imaging technology graduate programs. By incorporating real or simulated clinical cases alongside scenario-based task-driven learning and systematic skill training, this model establishes a structured teaching framework aligned with contemporary competency-based medical education principles. It fosters deep integration between theoretical learning and practical application. Its pedagogical philosophy aligns with competency-based training objectives, helping cultivate high-caliber ultrasound technicians with both solid theoretical foundations and proficient technical skills. This addresses modern clinical demands for precise diagnosis and efficient examinations. Simultaneously, it provides theoretical grounding and practical design references for medical imaging curriculum reform. With rapid advancements in educational technology, the integration of digital and simulated tools holds promise for optimizing and innovating blended learning frameworks. In ultrasound education, integrating these technologies does not aim to replace authentic clinical practice but rather to form a powerful supplement and extension to supervised scanning and case discussions. By constructing a more systematic and structured training environment, digital and analog tools enhance the repeatability of the teaching process and standardize feedback. When strategically incorporated into the overall teaching system, they contribute to improving the scalability, standardization, and long-term sustainability of postgraduate ultrasound education. Future empirical research is needed to evaluate this model’s implementation effectiveness, learner performance, and long-term educational impact across diverse institutional settings. Through continuous refinement and validation, this framework holds promise for advancing standardized, sustainable ultrasound education.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Miao JH. The art and science of ultrasound imaging: medical applications of ultrasound in diagnosis and therapy and its impact on patient care. Cardiovasc Diagn Ther. 2023;13(1):109–11. doi:10.21037/cdt-22-537
2. Tao X, Li J, Gu Y, et al. A national quality improvement program on ultrasound department in China: a controlled cohort study of 1297 public hospitals. Int J Environ Res Public Health. 2022;20(1):397. doi:10.3390/ijerph20010397
3. Harrison G, Kraus B, Martins Dos Santos R, et al. The role of radiographers in ultrasound: a survey of the national societies within the European Federation of Radiographer Societies (EFRS). Radiography. 2021;27(3):761–767. doi:10.1016/j.radi.2021.02.003
4. Williams I, Baird M, Schneider M. Comparison between radiographers with sonography education working in remote Australia and radiologists’ interpretation of ultrasound examinations. Med Radiat Sci. 2022;69(3):293–298. doi:10.1002/jmrs.576
5. Yujia Y, Jingyi Z, Dongme W, et al. Training of high-level undergraduate ultrasound technicians based on innovative clinical thinking training. China Continuing Med Edu. 2024;16(13):6–10.
6. Hou J, Michaud C, Li Z, et al. Transformation of the education of health professionals in China: progress and challenges. Lancet. 2014;384(9945):819–827. doi:10.1016/S0140-6736(14)61307-6
7. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. doi:10.3109/0142159X.2010.501190
8. Swing SR. The ACGME outcome project: retrospective and prospective. Med Teach. 2007;29(7):648–654. doi:10.1080/01421590701392903
9. Holmboe ES, Sherbino J, Long DM, et al. The role of assessment in competency-based medical education. Med Teach. 2010;32(8):676–682. doi:10.3109/0142159X.2010.500704
10. Iwy M, Steinmetz P, Weerdenburg K, et al. The Canadian medical student ultrasound curriculum: a needs assessment and review. BMC Med Educ. 2014;14:207. doi:10.1186/1472-6920-14-207
11. Thistlethwaite JE, Davies D, Ekeocha S, et al. The effectiveness of case-based learning in health professional education. Med Teach. 2012;34(6):e421–e444. doi:10.3109/0142159X.2012.680939
12. Bi M, Zhao Z, Yang J, Wang Y. Comparison of case-based learning and traditional method in teaching postgraduate students of medical oncology. Med Teach. 2019;41(10):1124–1128. doi:10.1080/0142159X.2019.1617414
13. Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/MD.0000000000038813
14. Al-Elq AH. Simulation-based medical teaching and learning. Family Community Med. 2010;17(1):35–40. doi:10.4103/1319-1683.68787
15. Jiang Z, Wang J, Chen X, et al. Competency-based ultrasound curriculum for standardized training resident: a pre- and post-training evaluation. BMC Med Educ. 2024;24(1):1516. doi:10.1186/s12909-024-06560-2
16. Pedersen MRV, Østergaard ML, Nayahangan LJ, et al. Simulation-based education in ultrasound - diagnostic and interventional abdominal focus. Ultraschall Med. 2024;45(4):348–366. doi:10.1055/a-2277-8183
17. Recker F, Neubauer R, Dong Y, et al. Exploring the dynamics of ultrasound training in medical education: current trends, debates, and approaches to didactics and hands-on learning. BMC Med Educ. 2024;24(1):1311. doi:10.1186/s12909-024-06092-9
18. Barth G, Prosch H, Blaivas M, et al. Student ultrasound education, current views and controversies; who should be teaching? Z Gastroenterol. 2024;62(10):1718–1723. doi:10.1055/a-2356-7906
19. McLean SF. Case-Based learning and its application in medical and health-care fields: a review of worldwide literature. J Med Educ Curric Dev. 2016;3:
20. Kuang M, Hu HT, Li W, et al. Articles that use artificial intelligence for ultrasound: a reader’s guide. Front Oncol. 2021;11:631813. doi:10.3389/fonc.2021.631813
21. Provenzano SM, Mageto I, González Frontera A, et al. Ultrasound as a foundational tool in medical education: a literature review. Adv Med Educ Pract. 2025;16:2167–2179. doi:10.2147/AMEP.S552069
22. Ali M, Wahab IA, Huri HZ, et al. Personalised learning in higher education for health sciences: a scoping review. BMC Med Educ. 2025;25(1):969. doi:10.1186/s12909-025-07565-1
23. Boerboom TB, Jaarsma D, Dolmans DH, et al. Peer group reflection helps clinical teachers to critically reflect on their teaching. Med Teach. 2011;33(11):e615–e623. doi:10.3109/0142159X.2011.610840
24. White J, Stavros K, Lynch K, et al. Peer observation and feedback for small group facilitators in medical education. Med Sci Educ. 2025;35(2):639–645. doi:10.1007/s40670-024-02252-0
25. Natesan S, Bailitz J, King A, et al. Clinical teaching: an evidence-based guide to best practices from the council of emergency medicine residency directors. West J Emerg Med. 2020;21(4):985–998. doi:10.5811/westjem.2020.4.46060
26. Penn L, Golden ED, Tomblinson C, et al. Training the new radiologists: approaches for education. Semin Ultrasound CT MR. 2024;45(2):139–151. doi:10.1053/j.sult.2024.02.003
27. Ertl S, Wadowski PP, Löffler-Stastka H. Improving students’ performance via case-based e-learning. Front Med. 2025;11:1401124. doi:10.3389/fmed.2024.1401124
28. Teichgräber U, Ingwersen M, Bürckenmeyer F, et al. Structured work-based learning in undergraduate clinical radiology immersion experience. BMC Med Educ. 2021;21(1):167. doi:10.1186/s12909-021-02592-0
29. He R, Xie Y, Liu F, et al. Implementing case-based collaborative learning curriculum via webinar in internal medicine residency training: a single-center experience. Medicine. 2023;102(16):e33601. doi:10.1097/MD.0000000000033601
30. Höhne E, Recker F, Dietrich CF, et al. Assessment methods in medical ultrasound education. Front Med. 2022;9:871957. doi:10.3389/fmed.2022.871957
31. Signor E, Gerstenberger J, Cotton J, et al. Integrating a self-directed ultrasound curriculum for the internal medicine clerkship. Ultrasound J. 2024;16(1):19. doi:10.1186/s13089-024-00367-4
32. Noerholk LM, Morcke AM, Kulasegaram K, et al. Does group size matter during collaborative skills learning? A randomised study. Med Educ. 2022;56(6):680–689. doi:10.1111/medu.14791
33. Cavaleiro I, de Carvalho Filho MA. Harnessing student feedback to transform teachers: role of emotions and relationships. Med Educ. 2024;58(6):750–760. doi:10.1111/medu.15264
34. Li J, Xue E. Dynamic interaction between student learning behaviour and learning environment: meta-analysis of student engagement and its influencing factors. Behav Sci. 2023;13(1):59. doi:10.3390/bs13010059
35. Evans DJ, Zeun P, Stanier RA. Motivating student learning using a formative assessment journey. J Anat. 2014;224(3):296–303. doi:10.1111/joa.12117
36. Christensen L, Karle H, Nystrup J. Process-outcome interrelationship and standard setting in medical education: the need for a comprehensive approach. Med Teach. 2007;29(7):672–677. doi:10.1080/01421590701370537
37. Al Ansari A, Strachan K, Al Balooshi S, Al-Qallaf A, Otoom S. Influence of student feedback on the quality of teaching among clinical teachers in Bahrain. Med Sci Educ. 2019;30(1):253–262. doi:10.1007/s40670-019-00892-1
38. Gunther PG, Bingham RL. A continuous quality improvement cycle for teaching the identification of psychosocial problems to general internal medicine residents. Acad Med. 1993;68(4):308–310. doi:10.1097/00001888-199304000-00022
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.