Back to Journals » Risk Management and Healthcare Policy » Volume 16
A Bibliometric Analysis of Diagnosis Related Groups from 2013 to 2022
Authors Lang X ![]() , Guo J
, Guo J ![]() , Li Y, Yang F, Feng X
, Li Y, Yang F, Feng X
Received 4 May 2023
Accepted for publication 24 June 2023
Published 2 July 2023 Volume 2023:16 Pages 1215—1228
DOI https://doi.org/10.2147/RMHP.S417672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Xiaona Lang,1 Jinming Guo,1 Yuntao Li,2 Fan Yang,1 Xin Feng1
1Pharmacy Department, Tianjin Hospital, Tianjin, People’s Republic of China; 2Integrative Chinese and Western Medicine Department, Tianjin Hospital, Tianjin, People’s Republic of China
Correspondence: Xin Feng, Pharmacy Department, Tianjin Hospital, Tianjin, People’s Republic of China, Tel +86 13652001152, Email [email protected]
Purpose: As an important management method of the global healthcare system, diagnosis related groups (DRGs) classify patients into different cost groups and pay more attention to the equitable distribution of medical resources and the quality of medical services. At present, most countries have used DRGs to help medical institutions and doctors to treat patients more accurately, avoid the waste of medical resources, and improve treatment efficiency.
Methods: The Web of Science database was searched to collect all relevant literature on DRGs from 2013 to 2022. The literature information was imported into CiteSpace, Vosviewer, and Histcite for data analysis and visualization of the results. Analyze the cooperative relationship among the countries, institutions, journals, and authors. The usage trend of keywords; Highlight the content of the cited articles.
Results: The number of articles published in this decade was stable, and the number of citations in 2014 was the highest. The United States and Germany, as the first countries to use the DRGs system, are ahead of other countries in terms of the number and quality of articles. We have carried out content research on the articles with high citations, and summarized the application range of DRGs; classification method; advantages and disadvantages of the application. In general, the development trend of DRGs in foreign countries is to continuously optimize the classification method, expand the scope of application, and improve the application effect. These provide support and reference for the improvement of medical services and the perfection of the medical insurance system.
Conclusion: The application of DRGs can improve the quality and efficiency of medical services, and reduce the waste of medical expenses. It can also promote the rational allocation of medical resources and the equity of medical services. In the future, DRGs will pay more attention to the personalized diagnosis and treatment and fine management of patients, and the sharing and standardization of medical data, to promote the development of medical informatization.
Keywords: DRGs, healthcare, costs, surgery, bibliometrics
Introduction
With the continuous development of medical technology and the continuous expansion of medical services, countries around the world are facing the problem of the growth of medical costs. To control the growth of medical costs and improve the quality of medical services, countries have adopted a series of medical payment systems and management measures.1,2 The diagnosis related groups (DRGs) system is designed based on the patient’s primary diagnosis and treatment process to group patients and determine their payments, as well as the allocation of hospital resources.3–5 At present, DRGs have become an important classification system in the global healthcare system, including in Europe, Asia, Australia, and other places.1,6–8 DRGs achieve the management and control of medical costs and quality by dividing patients into different cost groups based on similar characteristics in disease diagnosis, treatment, and rehabilitation.9–12 In the process of DRGs application, medical institutions and doctors need to pay more attention to the details of disease diagnosis, treatment, and rehabilitation, to improve the quality and effect of medical services. At the same time, more attention should be paid to the utilization efficiency of medical resources to reduce the waste of medical expenses.13–16
Citespace and Vosviewer are literature visualization analysis software. After understanding and studying certain literature materials by metrological analysis method, visual maps are made, hot spots are analyzed around the current situation of research content, and development trends are explored.17–19 HistCite is a citation analysis tool that can quickly map the development trend of the same field, organize the number of citations of articles, and find key studies and researchers.20
This paper is based on the literature analysis of the past ten years, and the literature information is organized and visualized by software. This paper expounds on the theoretical basis, application effects, development, and shortcomings of DRGs at home and abroad, to provide a reference for global medical service management and medical insurance system reform. At the same time, it also provides comprehensive data and analysis of DRGs for researchers and institutions in related fields.
Materials and Methods
Data Sources
Using the core collection of the Web of Science database, “diagnosis related groups” was used as the subject term, and synonyms included: “diagnosis-related group”; “DRG”; “DRGs”; “diagnostic-related group”; “diagnosis related group”; “diagnostic related group”; “diagnostic-related groups”; “diagnosis-related groups”; “diagnostic related groups” were searched. The period was set as January 1, 2013, to December 31, 2022, and the length of the period was ten years. The search began on March 4, 2023, and a total of 7702 pieces of literature were retrieved. Types such as conferences, newspapers, abstracts, and books were excluded by manual screening. After reading the title and abstract of the article, the articles that were not related to the content of the topic words were removed, and 1769 articles met the requirements.
Analytical Tools
HistCite software was used to visualize and analyze the data of countries/regions, institutions, and journals after statistics. Journal Impact Factor (IF) was obtained from Journal Citation Reports (2022). CiteSpace could be used to parse keywords and article clustering information. Vosviewer could visually analyze the information of publishing institutions and authors. By analyzing the DRGs’ information and constructing a co-occurrence network, the hotspots and development trends of related research in recent years can be obtained. CiteSpace 6.1.R6 was set to “Slice=1” and “g-index k=25”, when constructing the cluster analysis map of keywords and articles in this study to ensure that the amount of node information obtained from each time slice was as same as possible. Set Pruning to “Pathfinder” and “Purning sliced networks”; “Pruning the merged network”.
Results
Literature Statistics
As shown in Figure 1, a total of 1769 articles were included after the screening, from 64 countries and regions, 8381 authors, 728 journals, and 3522 keywords. They were written in 12 languages, mainly English (N=1437) and German (N=261). By calculating the Total Global Citation Score (TGCS), 60 research articles were cited more than 50 times, and 15 of them were cited more than 100 times.
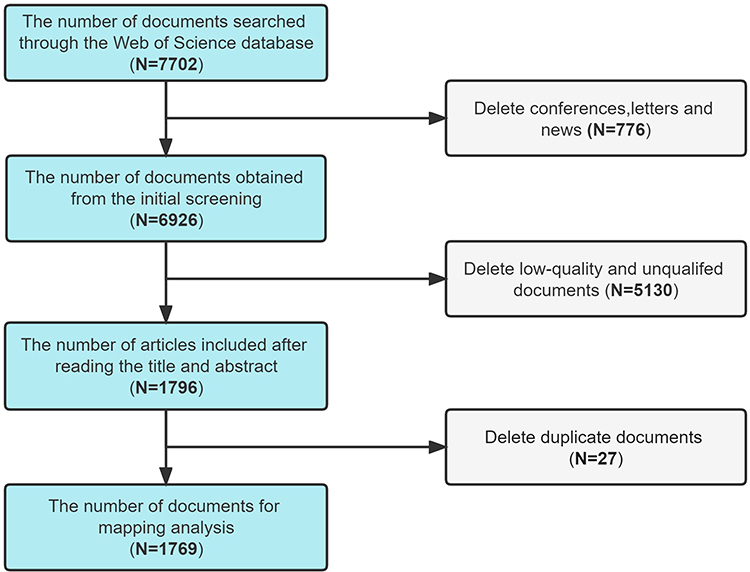 |
Figure 1 The process of literature screening. |
As shown in Figure 2A, the number of articles published in 2013 was 133, and the number of articles published in the following years increased slightly. Although the number curve was up and down, the overall number was very stable, maintained at more than 160. Most articles were published in 2018, with 207 articles. This indicates that DRGs related research has been concerned for researchers and has maintained good popularity in recent years. Although the number of articles published in 2014 was only 177, their TGCS values were high, indicating that the research content of this year was of good quality, and the content was of great help to subsequent research. After 2019, the number of articles was stable, but the TGCS value was not high, this decline may be due to a lack of content innovation or due to the new age and no citations.
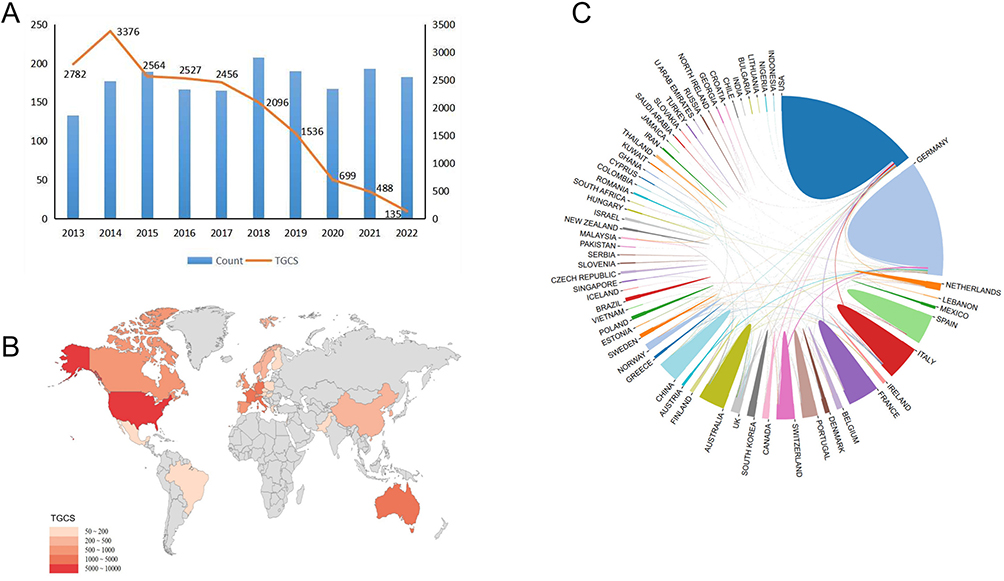 |
Figure 2 (A) Yearly output and score; (B) Distribution of global publications in the field of DRGs; (C) Academic cooperation networks between countries/regions. |
Geographical Distribution of the Literature
As could be seen from the display of Figure 2B, in terms of TGCS, the quality of publications in this field from Europe and America was high, and the content of the articles was worthy of citation and had great value for the research field. Next was Asia, dominated by China. Figure 2C showed that the United States and Germany had the largest number of articles. It could be seen from the line that many countries and regions cooperate. Table 1 listed the top ten countries with the number of publications involved in the study, showing that Europe and America had a large number of publications. There were 6 European countries, with a total number of 923 articles, accounting for 52.18% of the total. The top three countries in terms of Average Citation Index (ACI) values were the United States, France, and Australia, which indicates that these three countries had more mature research results and more valuable research content than other countries in this field.
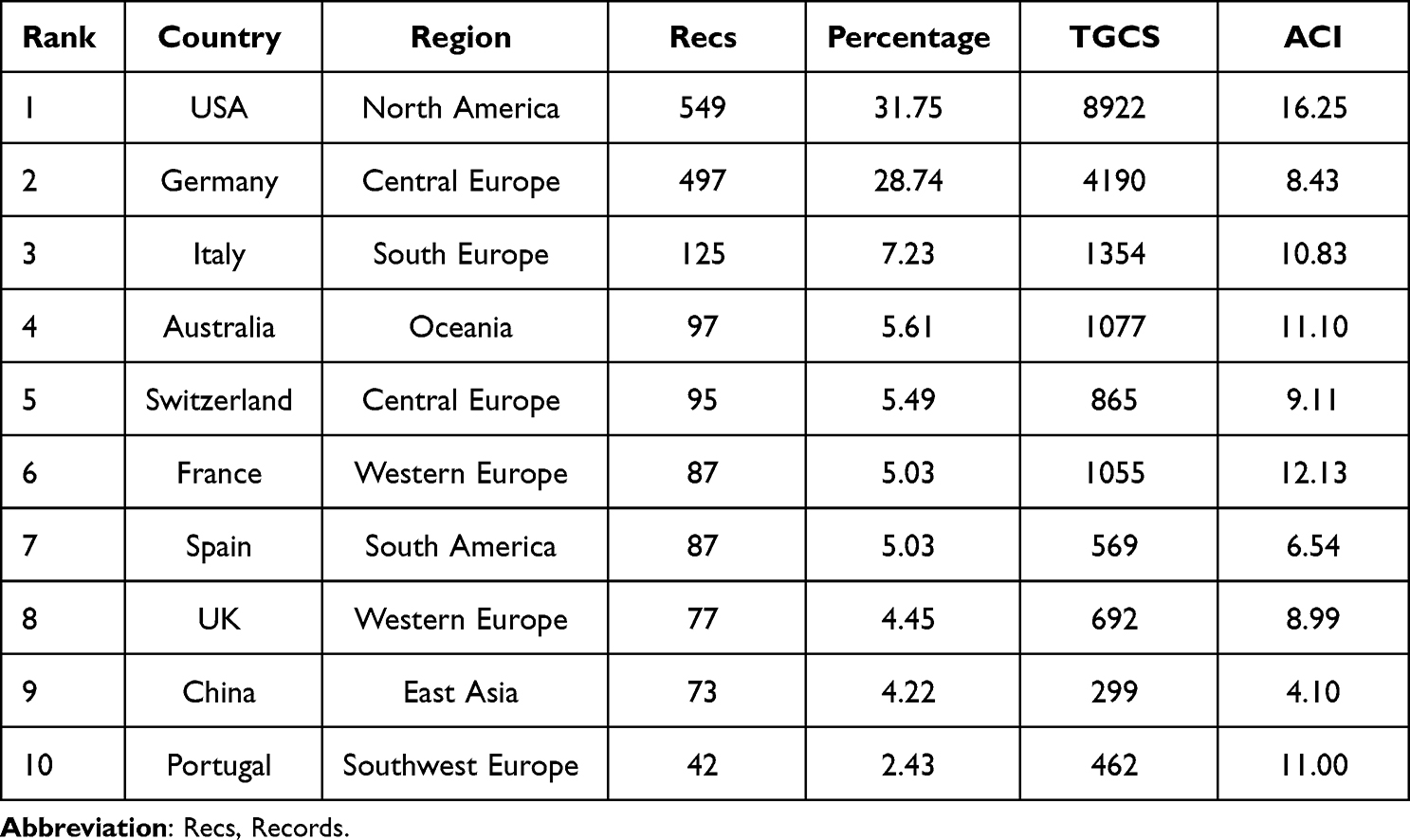 |
Table 1 The Top 10 Productive Countries in the Studies |
As shown in Table 2, the top ten TGCS institutions were all in the United States and Germany. The top institution was New York University, which had the highest TGCS score. This was followed by Hannover Medical School in Germany and the University of Michigan in the United States. The ACI value of Jena University Hospital was 39.70, which was higher than that of other institutions, indicating that the content of the article was good and the overall evaluation was high. The ACI value of The University of Iowa was 34.09, and the ACI value of New York University was 31.53. Through this data, we found that in the field of DRGs research, the United States and Germany were significantly ahead of other countries.
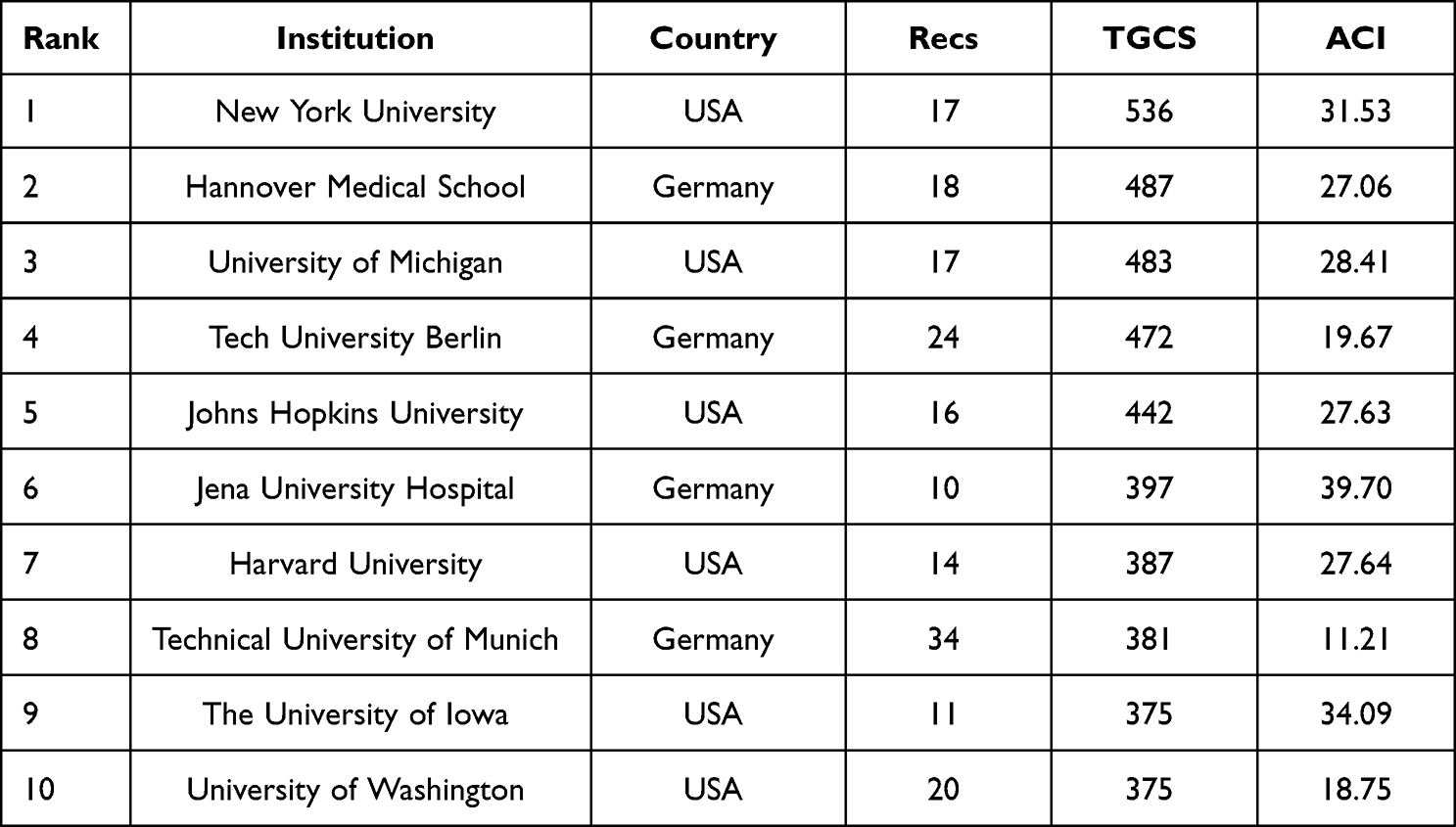 |
Table 2 The Top 10 Institutions (Based on Records and TGCS Respectively) |
Analysis of Journals
Table 3 listed the top 15 journals with TGCS scores on DRGs research. BMC HEALTH SERVICES RESEARCH published the most articles (N=55, 3.11%), followed by the JOURNAL OF ARTHROPLASTY (N=34, 1.92%). The top three TGCS were: JOURNAL OF TRAUMA AND ACUTE CARE SURGERY; JOURNAL OF ARTHROPLASTY and JAMA-JOURNAL OF THE AMERICAN MEDICAL ASSOCIATION. Interestingly, JAMA-JOURNAL OF THE AMERICAN MEDICAL ASSOCIATION published only five articles, it had a very high TGCS and a high ACI value of 119.40. This indicates that as a journal with a very high influence, its article collection requirements were strict, and the content of its published articles was also worthy of research and citation, which was easier to be used by researchers to learn and explore. The journal with high ACI value also had PHARMACOEPIDEMIOLOGY AND DRUG SAFETY (105.67), RESPIRATORY CARE (94.50) and JAMA SURGERY (72.75). The number of articles published in these journals was not large, but the ACI value was very high. Their articles were cited by many scholars, and their content was worthy of attention.
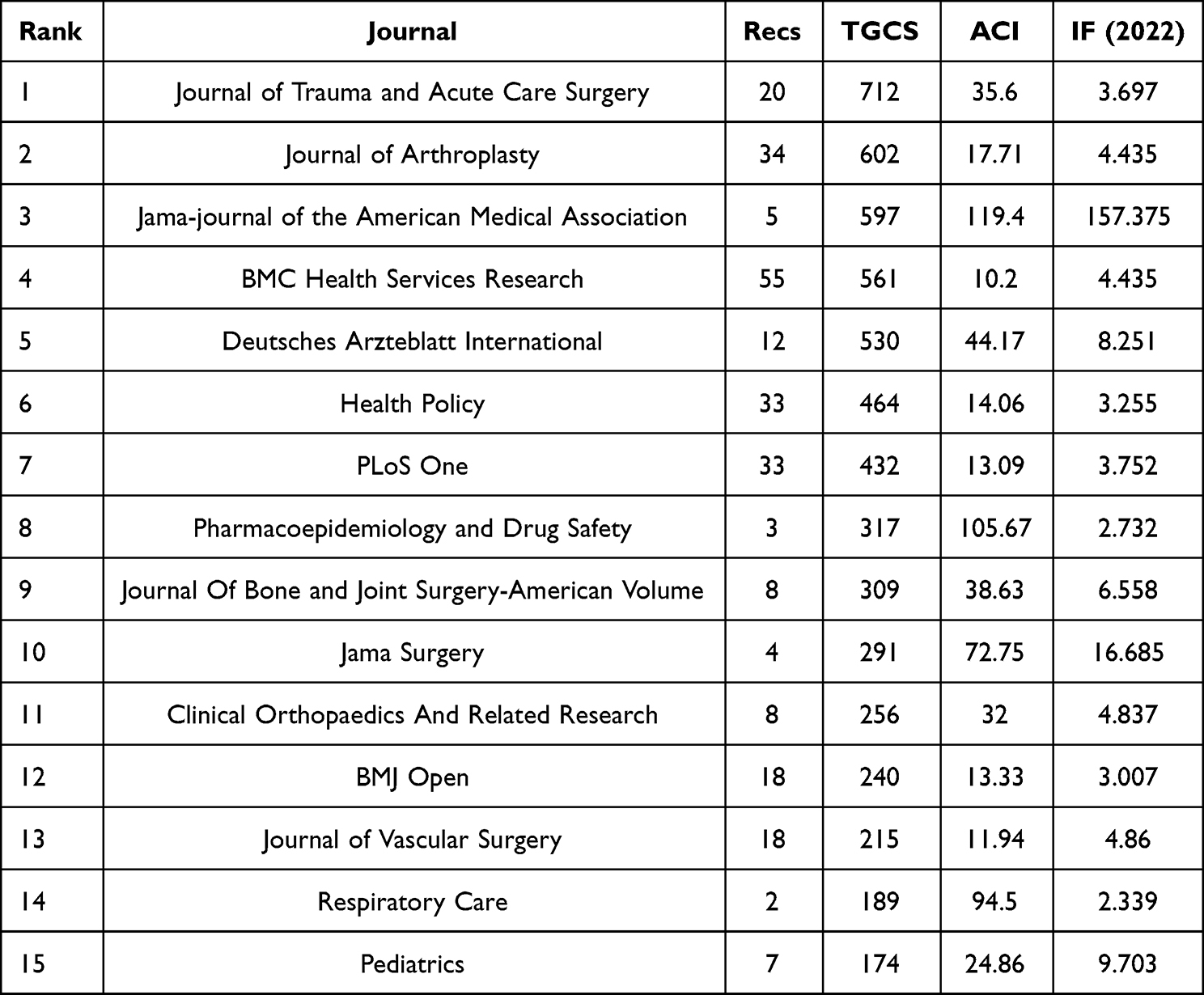 |
Table 3 The Top 15 Journals (Based on TGCS) |
Analysis of the Cooperative Relationship Between Authors and Institutions
Figure 3A illustrated the collaboration between institutions, and Figure 3B represent the collaboration of authors. Each node on the map was an institution, and the node size was proportional to the publication volume of the institution. The line was proportional to the cooperation relationship of different institutions, and the line thickness was proportional to the strength of the cooperation relationship. Most of the top institutions were universities or research institutes, with few hospitals. This indicates that DRGs research was still biased toward basic research. Due to a large number of authors and institutions, only the main cooperative noded in the cooperative network were selected in this paper, and the nodes were selected according to the number of papers published by the authors and the closeness of cooperation.
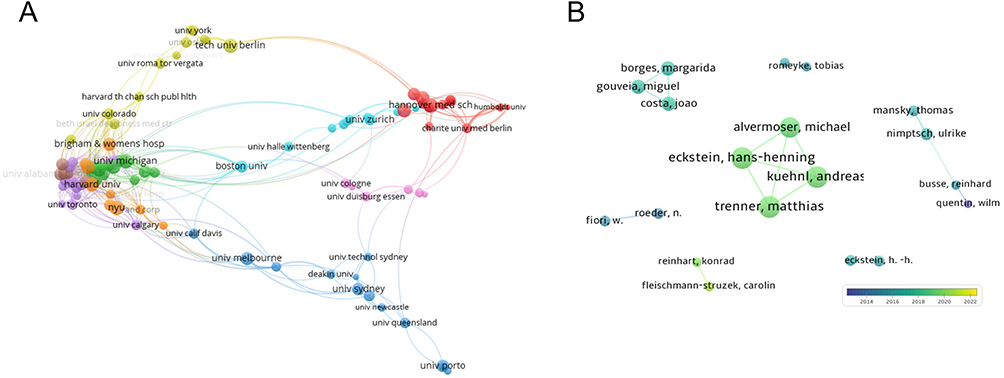 |
Figure 3 (A) Academic cooperation networks between institutions; (B) Academic cooperation networks between authors. |
Analysis of Keywords
The top five keywords in frequency were diagnosis related groups, care, outcome, mortality, and impact. From the above words, we could not only see the main content of this research direction but also the main noded of other important research directions. Figure 4A shows the top 20 most quotation-bursting words, the longer the red area, the longer the word had been cited. These included trial, acute myocardial infarction; discharge; medicare, etc. The breakout words in the last three years were repair, clinical coding, burden, time, and cesarean section. These words were the breakout words in DRGs research in recent years. We found that clinical indicators, hospitalization operation, and time were the hot topics. This also gave us a hint of future research directions. The map of high-frequency co-occurrence words was shown in Figure 4B, in which the circular nodes wrapped by purple circles represent the centrality of this keyword greater than 0.1, indicating that they were closely related to other keywords and had a large proportion of discussion in the article. The nodes with red dots were the top-ranked breakout words, which were also the trend and development in this field. The relevant information on the top 20 high-frequency keywords was summarized in Table 4, which reflected the main keywords discussed in the relevant literature in recent years.
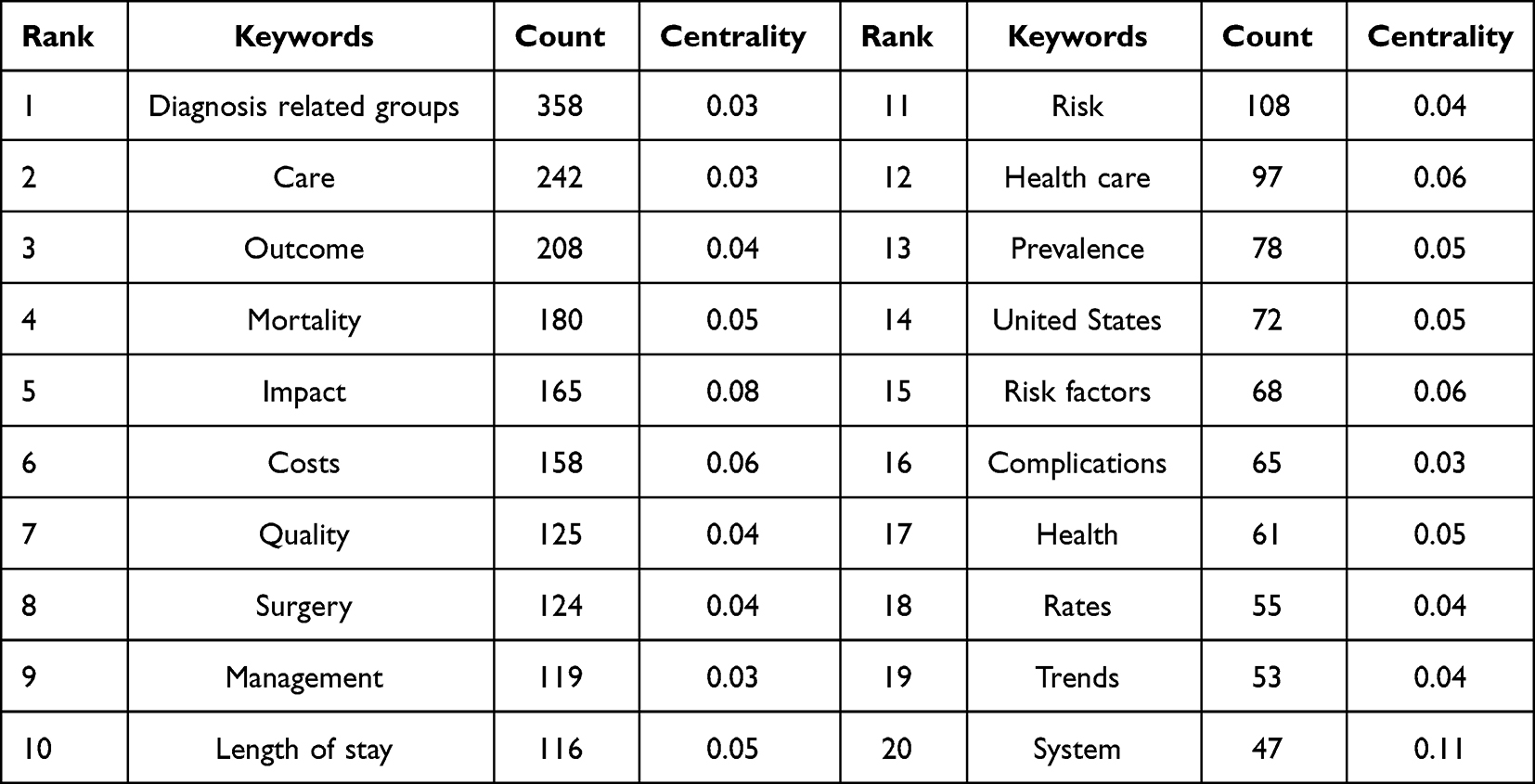 |
Table 4 The Top 20 Keywords |
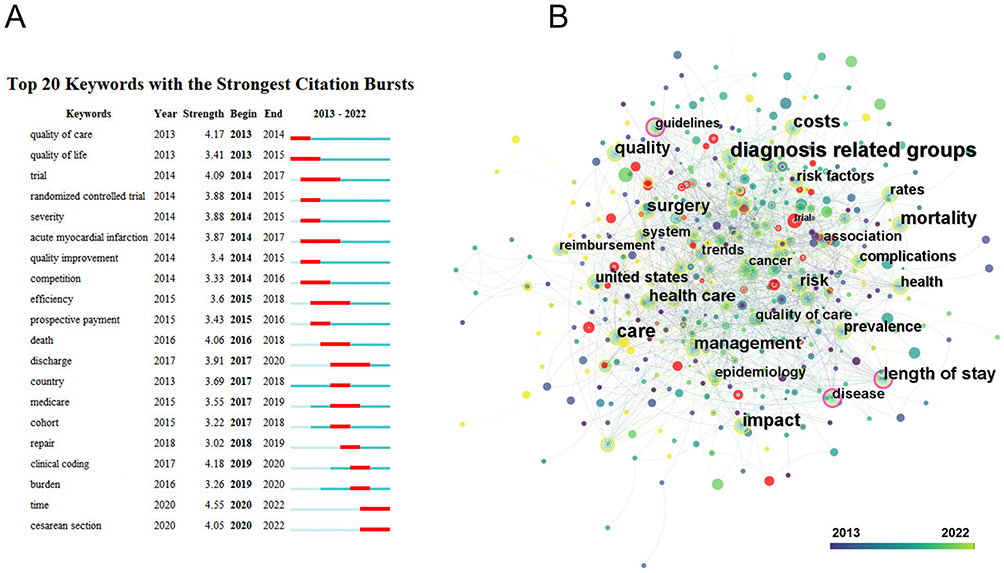 |
Figure 4 (A) The top 20 strongest strength citation burst; (B) Networks of keywords in the studies. |
Literature Co-Citation Analysis
Co-citation analysis was performed on the included literature and co-citation network to obtain and cluster to obtain Figure 5. Different colors represent the different cluster blocks. After clustering, the top 11 clusters were selected, including: #0 changing incentive structure; #1 hospital-initiated episode; #2 DRG system; #3 veterans health administration, and so on. Table 5 shows representative articles in each cluster block with high citations or high TGCS scores. It also illustrates the importance of these articles for researchers.
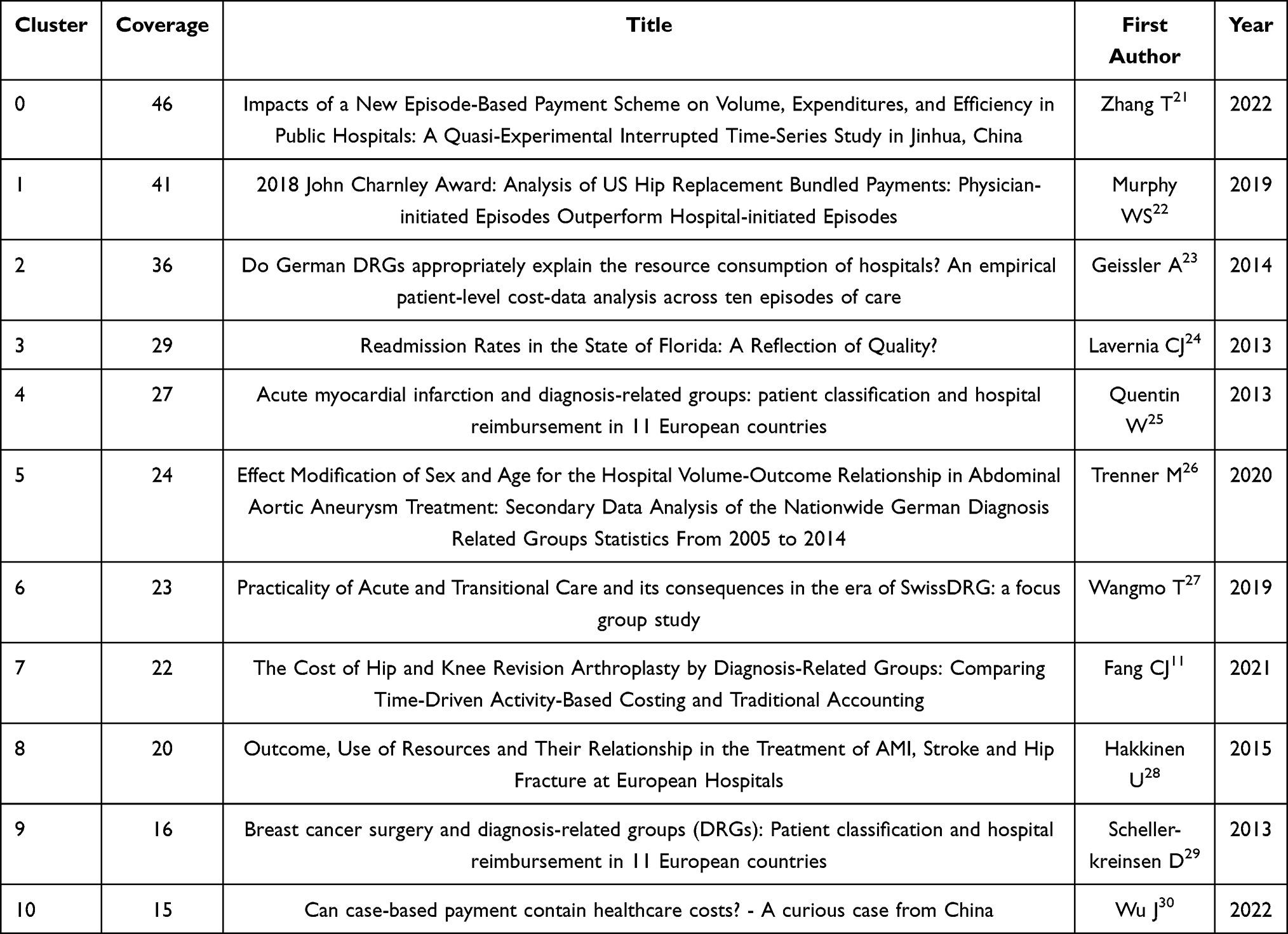 |
Table 5 Key Articles in Each Cluster |
 |
Figure 5 The cluster map of document co-citation. |
We summarized the representative articles of clustering and explored the research trends and hotspots of these articles. Zhang et al used a quasi-experimental interrupted time series study to analyze the volume, expenditure, and efficiency of medical services before and after the implementation of a new case-based payment system. The implementation of the new case-based payment system had led to a decline in the number and expenditure of medical services at public hospitals in Jinhua. At the same time, the operation efficiency of the hospital had been improved, that was, the hospital had better control of the treatment time and drug use of patients, and the quality and efficiency of medical services had been improved.21 Murphy et al found shorter operative time, less blood loss, and shorter hospital stays in physician-initiated behaviors. However, in the hospital-initiated behavior, the operation time was longer, the blood loss was greater, and the length of hospital stay was longer. In addition, physician-initiated behaviors were associated with higher patient satisfaction and lower complication rates.22 Geissler et al analyzed that the German DRG system has had only limited success in this regard. For any of the selected diseases, the G-DRG did not statistically reflect the actual resource needs of the hospital better than simple variables such as the number of diagnoses and procedures or selected ancillary diagnoses. Further development of the current classification of certain diseases was recommended. However, costs vary considerably among hospitals in some cases. The reason for these cost differences did not necessarily mean that higher price hospitals were less efficient. These differences may be related, on the one hand, to infrastructural conditions that were difficult for hospitals to influence and, on the other hand, to different types of organizations.23 Lavernia et al found relatively high 30-day readmission rates in Florida with significant regional variation. Meanwhile, readmission rates were related to factors such as hospital size, funding source, patient race, age, and gender. Readmission rates could be used as an indicator of hospital quality, but the effects of demographic and socioeconomic factors needed to be taken into account.24 Quentin et al suggested that the implementation of the DRG system differed in patient classification and hospital reimbursement for acute myocardial infarction (AMI). At the same time, the DRG system may have a certain impact on the hospital’s diagnosis and treatment decisions for AMI patients. Therefore, further research on the impact of DRG systems on hospitals and patients was needed to promote quality and equity of care.25 Trenner et al used DRG statistics from 2005 to 2014 for secondary data analysis. In the treatment of abdominal aortic aneurysm, there was an association between hospital operation volume and treatment outcome, the greater the operation volume, the better the treatment outcome. However, this association also required individualized treatment plans according to factors such as the gender and age of the patient to improve the treatment effect.26 Wangmo et al. Switzerland After the implementation of DRG, hospitals needed to pay more attention to the efficiency and economy of medical services. Acute and transitional care was considered to be the point of balance between hospital economics and quality of care. Further research on the impact of the implementation of care on hospitals and patients was needed to promote quality and equity of care.27 Fang et al found by comparison that Time-Driven Activity-Based Costing (TDABC) provides valuable bottom-up information about cost centers in the care pathway that, through targeted interventions, may lead to the valuable delivery of more desirable health care.11 Hakkinen et al used European health care outcomes from five countries: Finland, Hungary, Italy, Norway, and Sweden. The study found significant differences between hospitals and countries in the survival and use of resources. Some evidence would support increased horizontal integration: a higher concentration of regional aid is associated with lower resource use. In contrast, the resources of Finland and Sweden were more utilized.28 Scheller-kreinsen et al found differences in grouping rules and cost calculation methods for breast cancer surgery in the DRG system across 11 European countries. Some countries have higher hospital reimbursement than others. The implementation of the DRG system may lead to the hospital’s impact on the diagnosis and treatment decisions of patients with breast cancer surgery, for example, it may prompt the hospital to raise the admission threshold or reduce the admission time.29 Wu et al explored a case in China and found that a case-based payment system has been implemented in China and has been successful to some extent. The system can promote the cost control of hospitals, and encourage them to improve the quality of care and efficiency. However, the system also has some challenges and limitations, such as cost accounting and management problems in hospitals, and the preference of hospitals for high-profit cases.30
Most of these articles studied the comparison and status quo of hospitals or countries before and after the implementation of DRGs and discussed the advantages and disadvantages of current DRGs. In both developed and developing countries, the quality and efficiency of healthcare systems need to be improved, especially in terms of admission rates, surgical methods, and rehabilitation care. More approaches are needed to address the vulnerabilities posed by DRGs in the future.
We summarized the top 10 TGCS articles.31–40 Table 6 was the arrangement of the basic information of the articles. We believed that these representative articles had very valuable content and summarize the contents of the top 3 articles. According to the content, DRGs related articles could not be separated from the words of surgery, hospitalization, and complications. While saving medical costs, it was more important to ensure the quality and efficiency of medical services according to patients’ conditions. Improving the survival rate of patients and reducing the incidence of complications and mortality were the key points of the medical system.
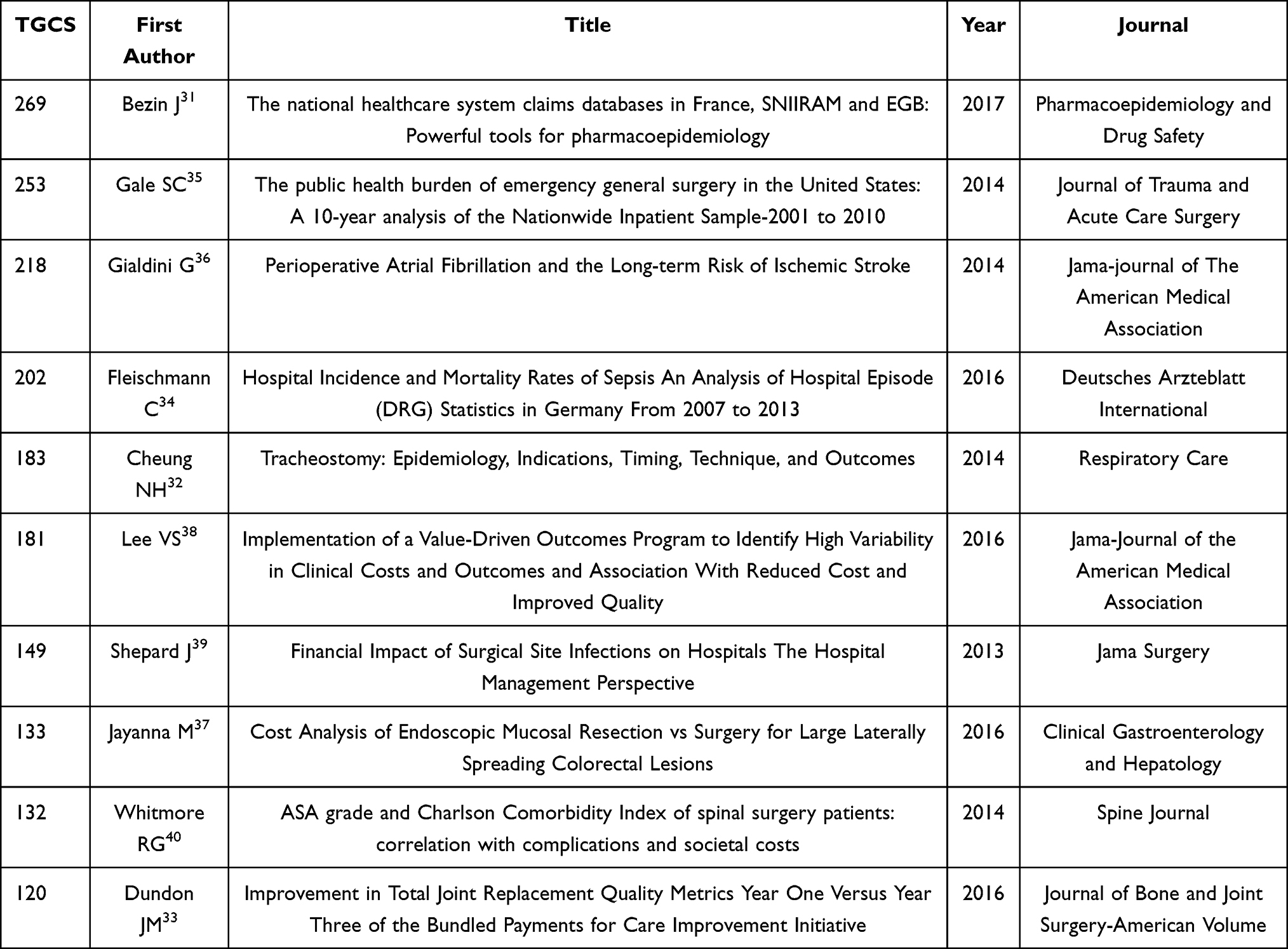 |
Table 6 Top 10 Articles (Based on TGCS) |
Bezin et al explored the role of two databases of the French national healthcare system, namely SNIIRAM and EGB, in pharmacoepidemiological studies.31 The SNIIRAM database contains healthcare data from all health insurance systems in France, including inpatient, outpatient, prescription, and other information. The EGB database is based on samples from the SNIIRAM database and is a continuous, repeatable, and representative sample database containing information on selected physicians and their patients. These two databases are powerful tools for conducting pharmacoepidemiological studies and can provide researchers with a wealth of information to better understand drug use and disease prevalence and to evaluate healthcare policies and disease management. However, when using these databases, attention needs to be paid to the quality and reliability of the data to ensure the accuracy and credibility of the findings.
Gale et al explored the public health burden of emergency general surgery in the United States by analyzing a national sample of hospitalized patients from 2001 to 2010.35 The incidence of emergency general surgery was increasing year by year, which was accompanied by high mortality and complication rates. These conditions resulted in longer medical costs and hospital stays for emergency general surgery, placing a heavy burden on the healthcare system and patients. Medical institutions needed to develop effective measures and recommendations to reduce this burden and improve the quality and efficiency of emergency general surgery.
Gialdini et al explored the relationship between perioperative AF and the long-term risk of ischemic stroke.36 Perioperative atrial fibrillation was one of the independent risk factors for ischemic stroke, and its incidence was several times higher than that of non-atrial fibrillation patients. In addition, perioperative AF increased the risk of cardiovascular events and death in patients. In addition, some factors such as hypertension and diabetes could further increase the risk of ischemic stroke in patients with perioperative atrial fibrillation. Minimizing surgical stimulation, maintaining electrolyte balance, actively controlling underlying diseases such as hypertension and diabetes, and timely diagnosis and treatment of atrial fibrillation were also needed. These measures would reduce the risk and burden for patients.
Discussion
According to the literature analysis, among the 1769 pieces of literature, the circulation of articles and TGCS in the United States and Germany ranked high, and many countries also cooperated. The cooperation between schools and research institutes was the main part of the article research institutions. Most of the coauthors come from the same country, and the cooperation between domestic and foreign scholars was not too much. The main contents of the literature were the length of hospital stay, mortality, medical insurance, income, etc., which were the research hotspots in the field. There were a lot of mutual citations among journals, especially the top several cited articles that had the characteristics of The Times, and the research was of great significance, which was worthy of researchers’ attention.
As a medical payment system based on disease classification, DRGs had been widely used and developed in the world. The application of DRGs in developed countries continues to expand. DRGs had been applied to medical services in more than 100 countries and regions. In addition to traditional application areas such as North America and Europe, DRGs had been gradually introduced and applied in Asia, Latin America, and Africa.41–45 The application scope of the DRGs system was very wide, including the following aspects: 1. Medical insurance payment: DRGs system was an important classification method of medical insurance payment. In the DRGs system, each patient was divided into a specific group that had a specific payment amount. This classification method could ensure the fairness and transparency of medical insurance payments.9,46,47 2. Hospital resource allocation: the DRGs system could help hospitals allocate resources reasonably to meet the needs of patients. Through the DRGs system, hospitals could understand the diagnosis and treatment process of patients so that they could better arrange medical resources.39,48 3. Medical quality assessment: the DRGs system could be used to assess medical quality. By comparing the treatment outcomes and costs of patients in different DRGs groups, the effectiveness and quality of care in hospitals could be assessed.5
The classification of DRGs had been continuously optimized. Initially, DRGs were classified according to disease diagnosis. With the development of DRGs, DRGS now included not only diagnostic information but also treatment, rehabilitation, surgery, and other information.26,49 In addition, the classification of DRGs also included the classification according to the patient’s age, gender, length of stay, hospital type, and other information, as shown in Figure 6.
 |
Figure 6 Different classifications of DRGs. |
The application effect of DRGs had been widely recognized. The application of DRGs could improve the quality and efficiency of medical services and reduce the waste of medical expenses. At the same time, DRGs could promote the rational allocation of medical resources and equity of medical services. In recent years, the application of DRGs in the field of medical services had been expanding, while some problems and controversies had also emerged. In health care reform, DRGs were regarded as an important means to reduce medical costs. However, the classification standard of DRGs was not accurate enough, which led to certain errors in hospital charges, which triggers dissatisfaction and protests from patients and health insurance institutions.23,50,51 This paper briefly summarized the advantages and disadvantages of DRGs, as shown in Table 7.
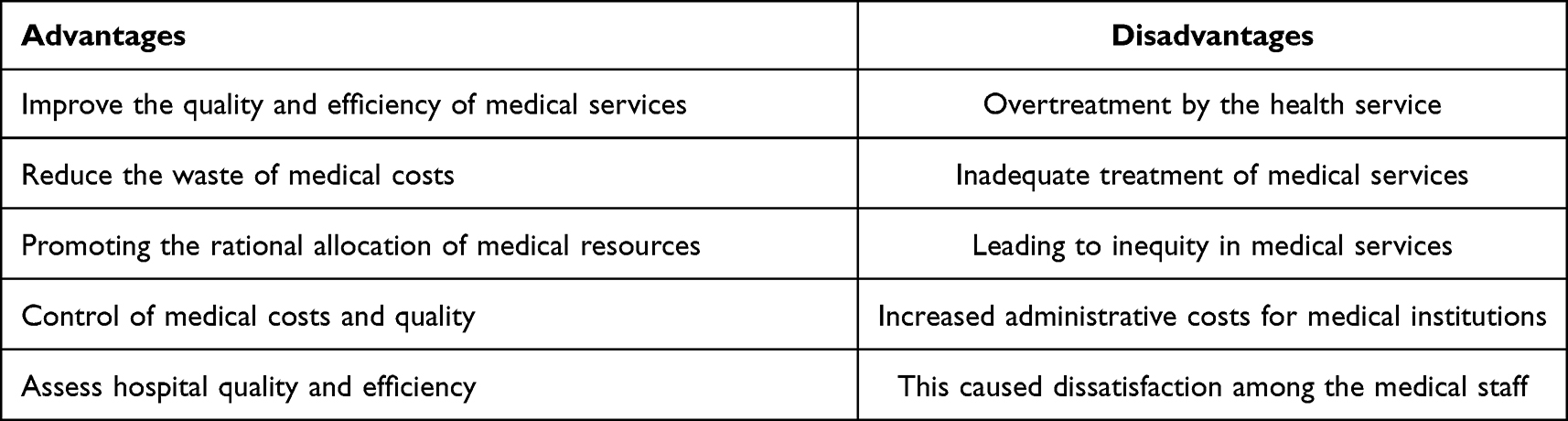 |
Table 7 Advantages and Disadvantages of DRGs |
In general, the development trend of DRGs in foreign countries is to continuously optimize the classification methods, expand the scope of application, and improve the application effect. These trends will continue to develop in the future, providing support and reference for the improvement of medical services and the perfection of the medical insurance system. DRGs will face many challenges and opportunities in the future. In the future, DRGs will pay more attention to personalized diagnosis and treatment and fine management of patients, to improve the efficiency and quality of medical services. In addition, DRGs will pay more and more attention to the sharing and standardization of medical data to promote the development of medical informatization.
In this study, we used bibliometrics to analyze the literature on DRGs in the Web of Science database and used Citespace, HistCite, and VOSviewer to quantitatively and qualitatively analyze the research contributions of different countries, institutions, journals, and authors in this field in recent years. The advantage of this paper is to sort out the development of this discipline through literature analysis in recent years and find out the characteristic publication period and key authors and their articles. Clarify the current research hotspots and development trends. The deficiency is that the literature search and collation were only conducted on the Web of Science, and no other databases were used. Some unpublished or ongoing publications have not been collected, which may also lead to incomplete statistics. Moreover, it has certain limitations and only analyzes the hot trend of the literature. In future research, we will learn more databases and software applications, improve our literature analysis content, and continue to pay attention to the development of DRGs in line with the requirements of the project.
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships construed as a potential conflict of interest.
References
1. Quentin W, Scheller-Kreinsen D, Blumel M, Geissler A, Busse R. Hospital payment based on diagnosis-related groups differs in Europe and holds lessons for the United States. Health Aff. 2013;32(4):713–723. doi:10.1377/hlthaff.2012.0876
2. Quinn K. After the revolution: dRGs at age 30. Ann Intern Med. 2014;160(6):426–429. doi:10.7326/m13-2115
3. Chin N, Perera P, Roberts A, Nagappan R. Review of medical discharge summaries and medical documentation in a metropolitan hospital: impact on diagnostic-related groups and Weighted Inlier Equivalent Separation. Intern Med J. 2013;43(7):767–771. doi:10.1111/imj.12084
4. Mathauer I, Wittenbecher F. Hospital payment systems based on diagnosis-related groups: experiences in low- and middle-income countries. Bull World Health Organ. 2013;91(10):746–756. doi:10.2471/blt.12.115931
5. Pongpirul K, Robinson C. Hospital manipulations in the DRG system: a systematic scoping review. Asian Biomed. 2013;7(3):301–310. doi:10.5372/1905-7415.0703.180
6. Peltola M, Quentin W; Euro DRGG. Diagnosis-Related Groups for Stroke in Europe: patient classification and hospital reimbursement in 11 countries. Cerebrovasc Dis. 2013;35(2):113–123. doi:10.1159/000346092
7. Liu R, Shi JW, Yang BL, et al. Charting a path forward: policy analysis of China’s evolved DRG-based hospital payment system. Int Health. 2017;9(5):317–324. doi:10.1093/inthealth/ihx030
8. Annear PL, Kwon S, Lorenzoni L, et al. Pathways to DRG-based hospital payment systems in Japan, Korea, and Thailand. Health Policy. 2018;122(7):707–713. doi:10.1016/j.healthpol.2018.04.013
9. Wright DJ, Mukamel DB, Greenfield S, Bederman SS. Cost variation within spinal fusion payment groups. Spine. 2016;41(22):1747–1753. doi:10.1097/brs.0000000000001649
10. Kifmann M, Siciliani L. Average-cost pricing and dynamic selection incentives in the hospital sector. Health Econ. 2017;26(12):1566–1582. doi:10.1002/hec.3451
11. Fang CJ, Shaker JM, Drew JM, Jawa A, Mattingly DA, Smith EL. The cost of hip and knee revision arthroplasty by diagnosis-related groups: comparing time-driven activity-based costing and traditional accounting. Article. J Arthroplasty. 2021;36(8):2674–2679. doi:10.1016/j.arth.2021.03.041
12. Hunger R, Mantke R. Outcome quality beyond the mean - an analysis of 43,231 pancreatic surgical procedures related to hospital volume. Ann Surg. 2022;276(1):159–166. doi:10.1097/sla.0000000000004315
13. Kim SJ, Han KT, Kim SJ, Park EC, Park HK. Impact of a diagnosis-related group payment system on cesarean section in Korea. Health Policy. 2016;120(6):596–603. doi:10.1016/j.healthpol.2016.04.018
14. Sorensen MLK, Burau V. Why we need to move beyond diagnosis-related groups and how we might do so. J Health Serv Res Policy. 2016;21(1):64–66. doi:10.1177/1355819615586444
15. Joya RM, Cottrell L, Kiefer A, Polak MJ. Diagnosis-related group weight and derived case mix index to assess the complexity among twins. Am J Perinatol. 2022;39(11):1223–1228. doi:10.1055/s-0040-1721847
16. Zhao SL, Gu YY, Huang ZJ. Building a performance management system for hospitals based on Diagnosis-Related Group (DRG) payment. J Sens. 2022;20227001423. doi:10.1155/2022/7001423
17. Chen C, Chou S-C, Chiu C-S; Assoc Comp M. Visualizing and exploring scientific literature with CiteSpace. J Food Drug Anal. 2018;26(1):369–370. doi:10.1016/j.jfda.2017.04.007
18. Chen CM. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inform Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
19. Li B, Hu K, Lysenko V, et al. A scientometric analysis of agricultural pollution by using bibliometric software VoSViewer and Histcite (TM). Article. Environ Sci Pollut Res. 2022;29(25):37882–37893. doi:10.1007/s11356-022-18491-w
20. Wu JF, Tsai HL. An explication of HistCite (TM): updates, modifications, and a variety of applications. Serials Rev. 2022;48(1–2):41–48. doi:10.1080/00987913.2022.2101821
21. Zhang T, Lu B, Yan Z, Huang X, Lu W. Impacts of a new episode-based payment scheme on volume, expenditures, and efficiency in public hospitals: a Quasi-experimental interrupted time-series study in Jinhua, China. Article. Risk Manag Healthc Policy. 2022;15:1659–1669. doi:10.2147/rmhp.S376516
22. Murphy WS, Siddiqi A, Cheng T, et al. 2018 John Charnley Award: analysis of US hip replacement bundled payments: physician-initiated episodes outperform hospital-initiated episodes. Article; Proceedings paper. Clin Orthop Relat Res. 2019;477(2):271–280. doi:10.1097/corr.0000000000000532
23. Geissler A, Quentin W, Busse R. Do German DRGs appropriately explain the resource consumption of hospitals? An empirical patient-level cost-data analysis across ten episodes of care. Article. Gesundheitswesen. 2014;76(5):284–296. doi:10.1055/s-0033-1351237
24. Lavernia CJ, Villa JM, Iacobelli DA. Readmission rates in the state of Florida: a reflection of quality? Article. Clin Orthop Relat Res. 2013;471(12):3856–3862. doi:10.1007/s11999-013-2849-2
25. Quentin W, Ratto H, Peltola M, Busse R, Hakkinen U; Euro DRGG. Acute myocardial infarction and diagnosis-related groups: patient classification and hospital reimbursement in 11 European countries. Article. Eur Heart J. 2013;34(26):1972–1981A. doi:10.1093/eurheartj/ehs482
26. Trenner M, Salvermoser M, Busch A, Reutersberg B, Eckstein -H-H, Kuehnl A. Effect modification of sex and age for the hospital volume-outcome relationship in abdominal aortic aneurysm treatment: secondary data analysis of the Nationwide German Diagnosis Related Groups Statistics from 2005 to 2014. Article. J Am Heart Assoc. 2020;9(6):e014534. doi:10.1161/jaha.119.014534
27. Wangmo T, Padrutt Y, Kone I, Gachter T, Elger BS, Leu A. Practicality of acute and transitional care and its consequences in the era of SwissDRG: a focus group study. Article. BMC Health Serv Res. 2019;19374. doi:10.1186/s12913-019-4220-0
28. Hakkinen U, Rosenqvist G, Iversen T, Rehnberg C, Seppala TT; Eurohope Study G. Outcome, use of resources and their relationship in the treatment of AMI, stroke and hip fracture at European hospitals. Article. Health Econ. 2015;24:116–139. doi:10.1002/hec.3270
29. Scheller-Kreinsen D, Quentin W, Geissler A, Busse R; Euro DRGG. Breast cancer surgery and diagnosis-related groups (DRGs): patient classification and hospital reimbursement in 11 European countries. Article. Breast. 2013;22(5):723–732. doi:10.1016/j.breast.2012.11.001
30. Wu J, He X, Feng XL. Can case-based payment contain healthcare costs? - A curious case from China. Article. Soc Sci Med. 2022;312115384. doi:10.1016/j.socscimed.2022.115384
31. Bezin J, Duong M, Lassalle R, et al. The national healthcare system claims databases in France, SNIIRAM and EGB: powerful tools for pharmacoepidemiology. Article. Pharmacoepidemiol Drug Saf. 2017;26(8):954–962. doi:10.1002/pds.4233
32. Cheung NH, Napolitano LM. Tracheostomy: epidemiology, indications, timing, technique, and outcomes. Article. Respir Care. 2014;59(6):895–915. doi:10.4187/respcare.02971
33. Dundon JM, Bosco J, Slover J, Yu S, Sayeed Y, Iorio R. Improvement in total joint replacement quality metrics year one versus year three of the bundled payments for care improvement initiative. Article. J Bone Joint Surg. 2016;98(23):1949–1953. doi:10.2106/jbjs.16.00523
34. Fleischmann C, Thomas-Rueddel DO, Hartmann M, et al. Hospital incidence and mortality rates of sepsis an analysis of hospital episode (DRG) statistics in Germany From 2007 to 2013. Article. Dtsch Arztebl Int. 2016;113(10):159–166. doi:10.3238/arztebl.2016.0159
35. Gale SC, Shafi S, Dombrovskiy VY, Arumugam D, Crystal JS. The public health burden of emergency general surgery in the United States: a 10-year analysis of the Nationwide Inpatient Sample-2001 to 2010. Article. J Trauma Acute Care Surg. 2014;77(2):202–208. doi:10.1097/ta.0000000000000362
36. Gialdini G, Nearing K, Bhave PD, et al. Perioperative atrial fibrillation and the long-term risk of ischemic stroke. Article. JAMA. 2014;312(6):616–622. doi:10.1001/jama.2014.9143
37. Jayanna M, Burgess NG, Singh R, et al. Cost analysis of endoscopic mucosal resection vs surgery for large laterally spreading colorectal lesions. Article. Clin Gastroenterol Hepatol. 2016;14(2):271–278. doi:10.1016/j.cgh.2015.08.037
38. Lee VS, Kawamoto K, Hess R, et al. Implementation of a value-driven outcomes program to identify high variability in clinical costs and outcomes and association with reduced cost and improved quality. Article. JAMA. 2016;316(10):1061–1072. doi:10.1001/jama.2016.12226
39. Shepard J, Ward W, Milstone A, et al. Financial impact of surgical site infections on hospitals the hospital management perspective. Article. JAMA Surg. 2013;148(10):907–914. doi:10.1001/jamasurg.2013.2246
40. Whitmore RG, Stephen JH, Vernick C, et al. ASA grade and Charlson Comorbidity Index of spinal surgery patients: correlation with complications and societal costs. Article. Spine J. 2014;14(1):31–38. doi:10.1016/j.spinee.2013.03.011
41. Bellanger MM, Quentin W, Tan SS; Euro DRGG. Childbirth and Diagnosis Related Groups (DRGs): patient classification and hospital reimbursement in 11 European countries. Eur J Obstetr Gynecol Reproduct Biol. 2013;168(1):12–19. doi:10.1016/j.ejogrb.2012.12.027
42. Chanturidze T, Esau M, Holzer S, Richardson E. Introducing Diagnosis-Related Groups in Kazakhstan: evolution, achievements, and challenges. Health Policy. 2016;120(9):987–991. doi:10.1016/j.healthpol.2016.07.007
43. Dimitropoulos V, Yeend T, Zhou QS, et al. A new clinical complexity model for the Australian Refined Diagnosis Related Groups. Health Policy. 2019;123(11):1049–1052. doi:10.1016/j.healthpol.2019.08.012
44. Kim S, Jung C, Yon J, et al. A review of the complexity adjustment in the Korean Diagnosis-Related Group (KDRG). Health Inform Manag J. 2020;49(1):62–68. doi:10.1177/1833358318795804
45. Kotherova Z, Caithamlova M, Nemec J, Dolejsova K. The Use of Diagnosis-Related Group-Based Reimbursement in the Czech Hospital Care System. Int J Environ Res Public Health. 2021;18(10):5463. doi:10.3390/ijerph18105463
46. Wu SW, Pan Q, Chen T. Research on diagnosis-related group grouping of inpatient medical expenditure in colorectal cancer patients based on a decision tree model. World J Clin Cases. 2020;8(12):2484–2493. doi:10.12998/wjcc.v8.i12.2484
47. Zhao CR, Wang C, Shen CW, Wang Q. Diagnosis-related group (DRG)-based case-mix funding system, a promising alternative for fee for service payment in China. Biosci Trends. 2018;12(2):109–115. doi:10.5582/bst.2017.01289
48. Tan SS, Chiarello P, Quentin W. Knee replacement and Diagnosis-Related Groups (DRGs): patient classification and hospital reimbursement in 11 European countries. Knee Surg Sports Traumatol Arthrosc. 2013;21(11):2548–2556. doi:10.1007/s00167-013-2374-6
49. Elgwairi E, Yang SP, Nugent K. Association of the All-Patient Refined Diagnosis-Related Groups severity of illness and risk of mortality classification with outcomes. South Med J. 2021;114(10):668–674. doi:10.14423/smj.0000000000001306
50. Fourie C, Biller-Andorno N, Wild V. Systematically evaluating the impact of diagnosis-related groups (DRGs) on health care delivery: a matrix of ethical implications. Health Policy. 2014;115(2–3):157–164. doi:10.1016/j.healthpol.2013.11.014
51. Zolbanin HM, Davazdahemami B, Delen D, Zadeh AH. Data analytics for the sustainable use of resources in hospitals: predicting the length of stay for patients with chronic diseases. Inform Manag. 2022;59(5):103282. doi:10.1016/j.im.2020.103282
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Trends of Low Back Pain Research in Older and Working-Age Adults from 1993 to 2023: A Bibliometric Analysis
Zheng DKY, Kawchuk GN, Bussières AE, Al Zoubi FM, Hartvigsen J, Fu SN, de Luca K, Weiner DK, Karppinen J, Samartzis D, Ferreira ML, Wu J, Dennett L, Wong AY
Journal of Pain Research 2023, 16:3325-3341
Published Date: 2 October 2023
Experiences of Healthcare Providers and Households Facing Healthcare Costs in Eastern Kasai/DR Congo: A Qualitative Analysis
Mutombo B, Mjumbe CK, Mpanya A, Cilumbayi DK, Lutumba P
ClinicoEconomics and Outcomes Research 2026, 18:573451
Published Date: 2 February 2026