Back to Journals » Orthopedic Research and Reviews » Volume 15
3D Printing of Individual Running Insoles – A Case Study
Authors Danko M ![]() , Sekac J, Dzivakova E, Zivcak J, Hudak R
, Sekac J, Dzivakova E, Zivcak J, Hudak R
Received 10 December 2022
Accepted for publication 3 May 2023
Published 29 May 2023 Volume 2023:15 Pages 105—118
DOI https://doi.org/10.2147/ORR.S399624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Maria Danko, Jan Sekac, Eva Dzivakova, Jozef Zivcak, Radovan Hudak
Department of Biomedical Engineering and Measurement, Technical University of Kosice, Kosice, Slovak Republic
Correspondence: Maria Danko, Technical University of Kosice, Letna 9, Kosice, 040 01, Slovak Republic, Tel +421 55 602 2382, Email [email protected]
Purpose: The study’s starting point is to find a low-cost and best-fit solution for comfortable movement for a recreational runner with knee pain using an orthopedic device. It is a case study. The research aims to apply digitization, CAD/CAM tools, and 3D printing to create an individual 3D running insole. The objective is to incorporate flexible shape optimization would provide comfort reductions in foot plantar pressures in one subject with knee pain while running. The test hypothesis was if it is possible to make it from one material. For this purpose, we created a new digital workflow based on the Decision Tree method and analyzed pain and comfort scores during user testing of prototypes.
Patient and Methods: The input data were obtained during a professional examination by a specialist doctor in the orthopedic outpatient clinic in the motion laboratory (DIERS 4D Motion Lab, Germany) with the output of data on the proband’s complex movement stereotype. Surface and volumetric data were obtained in the biomedical laboratory with the 3D scanner. We modified the digital 3D foot models in 3D mesh software, developed the design in SW Gensole (Gyrobot, UK), and finally incorporated the internal structure and the surface layer of the insole data of the knowledge from the medical examination, comfort analyses, and scientific studies findings.
Results: Four complete 3D-printed prototypes (n=4) with differences in density and correction elements were designed. All of them were fabricated on a 3D printer (Prusa i3 MK3S, Czech Republic) with flexible TPU material suitable for skin contact. The Participant tested each of them five times in the field during a workout and final insoles three months on the routine training.
Conclusion: A novel workflow was created for designing, producing, and testing full 3D-printed insoles. The product is fit for immediate use.
Keywords: insole, orthotic, digitization, 3D printing, algorithm, foot
Introduction
Custom-made Orthopedic Insoles (CMIs) are an ordinary conservative solution to the complications associated with pes planus (flatfoot).1–28 Only orthopedic physicians and podiatrists can prescribe CMIs.2 They are responsible for diagnosis establishing,2 and defining the correction elements on the insoles.2,3,27,28
The production of a CMI that meets the biomechanical requirements for damping and support is demanding from material and mechanical points of view, knowledge, and skills.1,3–5,7,15,21,27,28 It follows from the above that a fundamental assumption for the successful designing CMIs is to understand the correlation of the foot to posture29 and other aspects of the musculoskeletal system,1,3–9 to perceive relationships to associated diseases and cognition of the biomechanics,1,4,5,12 weight-bearing activities1,3,5–7,9 of humans, and pathological forces1,3,5–7,13 which affect the foot. In general, the main principle in the design of CMI is the correction of deformities,1,3,7–9 reductions of painful symptoms,3–10and adequate load distribution.1,3,6,8,12
Pain in the lower limbs and muscle fatigue are characteristic symptoms of flat feet.1–10 These severe accompanying phenomena make ordinary life miserable and are why a person seeks professional help.3 An insole must bear the often-extreme loads3,8,9 in athletes.1,12,15–18 Therefore, comfort evaluation is essential8 because the perception of poor comfort6 may lead to poor user compliance.30,31
Other crucial things are the correct shoe size, adequate space19 for the exact insole inside, which is in contact5,8,18 with the foot during all dynamic and postural movements,9 such as standing, walking, and running.5, It is precisely for this purpose that digitizing dimensions is of great importance.1,12
Several studies1,3,6,15,18–20 have investigated whether 3D-printed CMIs can reduce metatarsal pressure by distributing it over the midfoot.3,12 They reported a reduction in damage to symptomatic flat feet.3,6 Current research3 shows CMIs do not significantly affect foot re-aligning.4 However, they significantly affect comfort perception3,6 and reduce painful symptoms.3 Initial studies also report that properly designed and manufactured 3D-printed CMIs effectively manage heel pain3,4 and influence altering lower limb biomechanics.4,19,20 A detailed analysis of the results3 showed that the evidence is insufficient and that extensive research is needed.2,11 At the same time, this analytical study recognized 3D printed insoles as successful in alleviating pain with an increase in the feeling of comfort (comfort score3,6,20,21,28) and a possible effect on foot biomechanics.1,4,6,18,20
The research results show that the insole should be flexible in the most stressed areas1,9 and provide optimal support9 in the longitudinal arch,1,6 which can also be achieved with the porous structure inside the insole.5 Previous studies mainly focus on insoles composed from different materials and components;3,8,15,28 only a few are made from one material.10,19,20 This was one of the main points of our research.
Next, contemporary research is oriented toward testing the effect of already manufactured3,11 CMIs. However, only a few studies experiment with fabrication without mentioning the printing parameters.18,20 Therefore, the study aims to create a procedural algorithm for additive manufacturing, CMI prototype testing, and a cost-effective solution to produce functional custom-made orthopedic insoles for running. The goal was to develop the digital workflow9,32,33 for the production and testing procedure of CMIs. The tested hypothesis was whether a comfortable insole for a recreational runner could be made from only one material using different densities of the inside structure to achieve the required comfort and biomechanical properties. It is a pilot study in which one proband participated.
Patients, Materials, and Methods
Patient
General information about the patient (woman): body weight (90 kg), height: 168cm; age: 22 years old; pathology: Bilateral flat feet transversely and longitudinally, painless when walking and palpation. Heel valgus. An individual without skin issues on the feet, neuropathy, or deformity was recruited for this study. Activity level: recreational runner; the participant’s routine is running about one km thrice a week.
The study was approved by the Ethics Committee of the Technical University in Košice (file number: 26272/2023/R-OLP). The participant was informed in advance about the purpose of the research and signed the patient’s written informed consent regarding the study.
Materials
We selected a thermoplastic polyether-polyurethane elastomer with additives for additive manufacturing of CMI (TPU, Filaflex 82A Original; specification: 1.75 mm) — mechanical properties: Shore 82A hardness, Abrasion loss 25mm3, and stretching up to 650%. The filament complies with the EC 1272/2008/CE safety standard (CLP) regarding health and the environment.34 Filaflex® has hydrolysis resistance, high resistance to bacteria, is non-toxic, and can be in contact with the skin. It is an elastic fiber with low-temperature flexibility properties in printed parts. The most significant advantage is that it returns to its original shape without deformation or damage after stretching. Materials of this class are odorless and solvent resistant. Therefore, it has applications in medicine, prosthetics, the food industry, etc. The material data sheet from the manufacturer directly recommends manufacturing orthopedic insoles or shoes.
Methods
Podological Diagnostics
The entire examination was performed in an orthopedic outpatient clinic by a medical specialist, a board-certified podiatrist.2 The first step was to obtain a medical history from the proband, perform a physical examination and measure basic body proportions (height, weight, foot size).2, Subsequently, the proband underwent a series of tests on a DIERS pedogait (DIERS, Germany) with high-frequency measurements.32,35 Through instrumented quantitative foot diagnostics in statics and walking analysis in dynamics (Pedogait, DIERS, Germany), pressure distribution data during the dynamic test were obtained with a visual display of the contact map with the associated color resolution of data measurement. This includes stride length and width data, stride cycle, foot rotation, the body center of gravity trajectory,6 stride cadence, gait phases,32 foot-pad contact5 time, foot roll, average and maximum foot pressure, and information on the most loaded foot contact areas.32,35 As well as a representation of the compressive reaction forces of the foot during walking.
The subject was examined for bipedal standing, walking, and running (Figure 1). The static mentioned above and dynamic podiatric motion testing and diagnosis of the proband’s overall posture were similarly performed by an orthopedic specialist in the orthopedic outpatient clinic in the motion laboratory (DIERS 4D Motion Lab).
 |
Figure 1 Methodical diagram of the measurement procedure with Diers 4D Motion Lab. Subjects provided consent for a published photo. |
3D Foot Scan
Foot scan of neutral calcaneal position.3,7,22 3D scanning was performed with an Artec Eva handheld 3D scanner (Artec, USA) — used software algorithms:36 tracking Geometry+Texture, visualization of color distance, and Auto-align new scan. Feet capturing (Figure 2): (1) The standing-on-one-leg posture. The foot being captured kneels on a chair—Hip-width apart legs. The pelvis is neutral, hands are freely released, and the participant looks ahead.22 The measured ankle hangs over the edge of the chair. (Figure 2). (2) The Subtalar Joint Alignment7 (neutral position3,7). The participant keeps the captured foot neutral to make the transverse and longitudinal arches visible.
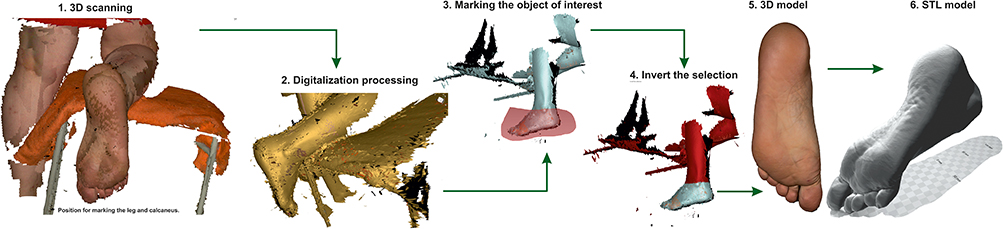 |
Figure 2 Scanning procedure with Artec Eva scanner (Artec, USA). |
(3) Whole-foot surface scanning. The capturing from the hindfoot alignment view to the sole and up to the distal ends of the phalanges and from the medial to the lateral aspect of the dorsal foot. Both legs (dexter/sinister) were digitized similarly (Figure 2).
Data Processing
Creating a 3D foot model (Figure 2)—data optimization in Artec Studio 14. (1) Used software algorithms: Model creation (scan quality), Auto-Alignment, Editor (Erasing all unnecessary parts), filling of holes, smoothing of surface shape, and reducing noise. Export to mesh (STL creation).
(2) Import of the STL foot model to Meshmixer® software for Modification (Figure 3). Both feet (dexter/sinister) are designed separately but similarly.8 Precise positioning of 3D foot model for the CAD coordinate system.8,10,19 Alignment primitives to the coordinate system according to CAD software for Insole design. We removed unnecessary parts of the foot. Smoothing of the model and removing the most noise.10 Alignment of Pternion10 to second distal phalange (X-axis). Identification of morphologically significant points8 (close to support points) on sole and creation of horizontal XY-plane.10
 |
Figure 3 Modification of STL foot model in Meshmixer software. |
CAD Designing the Running Insole
CMIs modeling in the parametric insole design by online Beta software Gensole EasyCAD, Gyrobot, UK10,37 (Figure 4): (1) determination of the CMI profile shape according to the inside curve of the shoe; (2) manual entry of input parameters affecting insole (individual’s weight, foot length, heel and forefoot width, inner and outer foot length); (3) uploading a 3D model of the foot (stl) and positioning the foot model on the insole blank; (4) A simple simulation to perform a foot impression on the insole design with visualization of data and colored mapping (Figure 4). 3D dimensional parameters captured by the Artec Eva® scanner were automatically translated into design parameters for insole customization10 (5) Solemorph, which means shaping the insole upper surface to foot scan model; (6) generating multiple density zones or importing pre-defined .dxf curves to increase the elastic properties of the material and relieve the foot; (7) creating an AMF file for the 3D printing slicing program.37
 |
Figure 4 Demonstration of the workflow in SW Gensole (Gyrobot, UK) for designing the internal structure of CMI. |
3D Printing Algorithm
3D Printing Pre-Processing (Figure 5). (1) Creating CAD design of the flexible parts for the heel and metatarsal bar.3, (2) Importing a foot scan stl file, flexible parts, and insole into the Ultimaker CURA software for slicing. (3) Positioning the foot on the insole. (4) Positioning of flexible parts according to morphological characteristics on the plantar side of the foot13,14 (sole). The metatarsal header and heel area relief were adjusted for each prototype and final product by layering and structurally patterning the material before printing in the free Ultimaker CURA software (Ultimaker, The Netherlands). These parts were independently adjusted to reduce the fill density by 50% compared to the rest of the print. (5) Checking the positioning of all components. (6) Deleting the foot model. (7) Setting of print parameters.
 |
Figure 5 Model preparation procedure in Ultimaker CURA software (Ultimaker, Netherlands). |
All novel Running CMIs we fabricated on a 3D printer (Prusa i3 MK3S, Czech Republic) with flexible material suitable for contact with skin (Filaflex 82A, Recreus, Spain).
(8) G-code. Slicing of the insole and generating G-code. G-code is a programming language for the 3D print setting. It comprises all information about the material, 3D dimensions, and layers density of 3D model files imported, printer head positioning, extruder, bed temperature, pauses, printer head speed, and more. (9) Inputting the G-code to the 3D -print.
Prototypes Testing
Measurement Aids: Participant Running Shoes (dimension, shape); A Visual Analogue Scale (VAS,3,38 Comfort Scale), Apple Watch Series 6 (application Workout: Outdoor Run), Running Log (Microsoft Excel).
Measurable Indicator: Pain, Comfort; Running Distance (Established Route).
First, the dimensional accuracy of the CMIs in the proband’s running shoes was tested. If they fit, the dynamic testing of comfort proceeded. The task of the proband was to run the set route recreationally. If the participant was exhausted or had pain, she walked. At the end of each workout, proband shared records with the study operator and rated the run with a mark on a pain scale.
Insole testing. (1) 1. Insole; CMIs without correction elements. The reason was to test the material’s properties during the user’s moving and obtain feedback2,3 regarding pain. We determined the dimensional accuracy and whether the insole fits in the proband’s running shoes (static test). We tested all other prototypes (2nd-4th inserts) similarly. (2) Dynamic testing; Five runs along a designated route (more than one kilometer) every four days (five workouts per month) (3) Instant sharing of running activity (route, time) and pain assessment according to VAS. (4) After a series of five outdoor runs, the comfort of the insole was evaluated. A new insole (2nd) was created based on a podiatry examination. (5) Dynamic Testing; Five runs along a designated route (more than one kilometer) every four days. (6) Instant sharing of running activity (route, time) and pain assessment according to VAS. (7) After a series of five outdoor workouts, the comfort of the insole was evaluated. Based on feedback from the proband, a new insole (3rd insole) was created. (8) Dynamic testing; Five runs along a designated route (more than one kilometer) every four days (five workouts per month). (9) Instant sharing of running activity (route, time) and pain assessment according to VAS. (10) After a series of five outdoor workouts, the comfort of the insole was evaluated. (11) Based on feedback from the proband and the results of the podiatry examination, a new insole (4th insole) was created. (12) Dynamic testing; Five runs along a designated route (more than one kilometer) every four days (five workouts per month). (13) Instant sharing of running activity (route, time) and pain assessment according to VAS. (14) After a series of five outdoor workouts, the comfort of the insole was evaluated.
(15) Based on the analysis, a new 4th insole was created, and a three-month comfort testing was started. Dynamic testing; running along a designated route (more than one kilometer), eight running workouts per month for three months. (16) Instant sharing of running activity (route, time) and pain assessment according to VAS. (17) Evaluation of the comfort of CMIs after three months of use).
Results
The multi-stage process7 was applied to design the customized novel insoles (Figures 1–8).2 (1) The expert podiatric examination resulted in a complete diagnosis established of the condition10 of the proband’s legs, posture, and movement,2 where no deformities of the limbs or limitations of mobility in individual joints were found. The spine is symmetrical, without motion reduction and palpation pain. Podoscopics: lowering of the transverse arch; PC podoscopy (static): tension in the area of metatarsals 1–5 bilaterally. PC posturometry: scoliotic deformity gr. Ia Dg. pedes transveroplani. Based on the digitized pressure point data and walking motion analysis,2 quantitative data and colored visual maps were obtained (Figure 6).
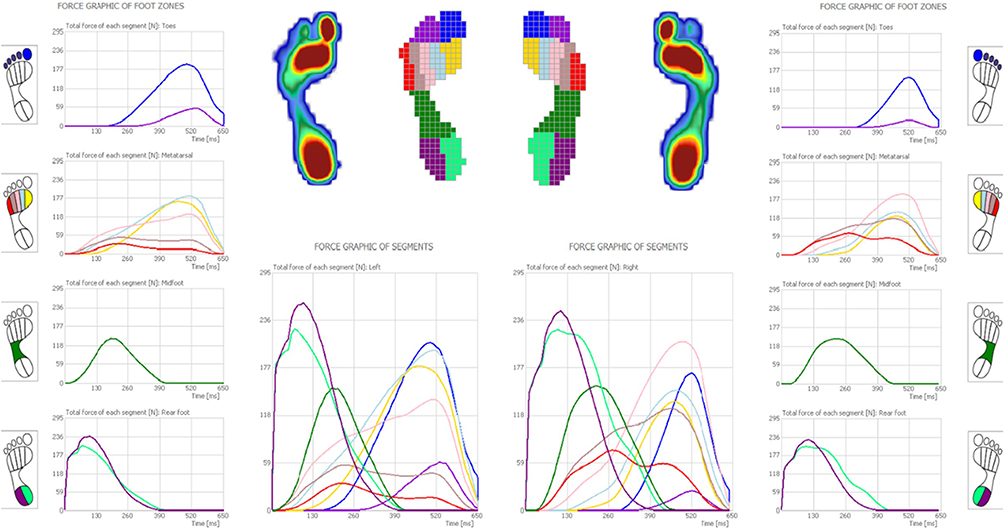 |
Figure 6 Output of the measurement. Distribution of pressures acting on the foot, Pedogait DIERS (Illustrative visual representation). |
 |
Figure 7 Prototyps of individual insoles. View of the top, bottom, and side of the insoles part; Graphical visualization of Pain Scale (VAS). |
 |
Figure 8 3D printing process of CMI. |
The developed 3D-printed CMIs are based on podology dynamic pressure measurement15,26 (DIERS 4D Motion Lab), adapted for the participant’s running shoes, and subjectively evaluated after each outdoor workout. The shape and internal structure modification depended on the medical findings when (2) designing the insoles in the free online software (Beta software Gensole EasyCAD (Gyrobot, UK). Insoles were solved separately for each foot (dexter/sinister). The inner and outer widths of the insole and the bare thickness were the same. (3) Four designs with different internal structure designs were created by editing an exemplary configuration of the required parameters and considering all the specified foot orthoses4 (FO) requirements (Table 1). The used material of CMIs is suited for sports4 such as walking and running activities.25 The difference between prototypes is based on the use of predominant elements.
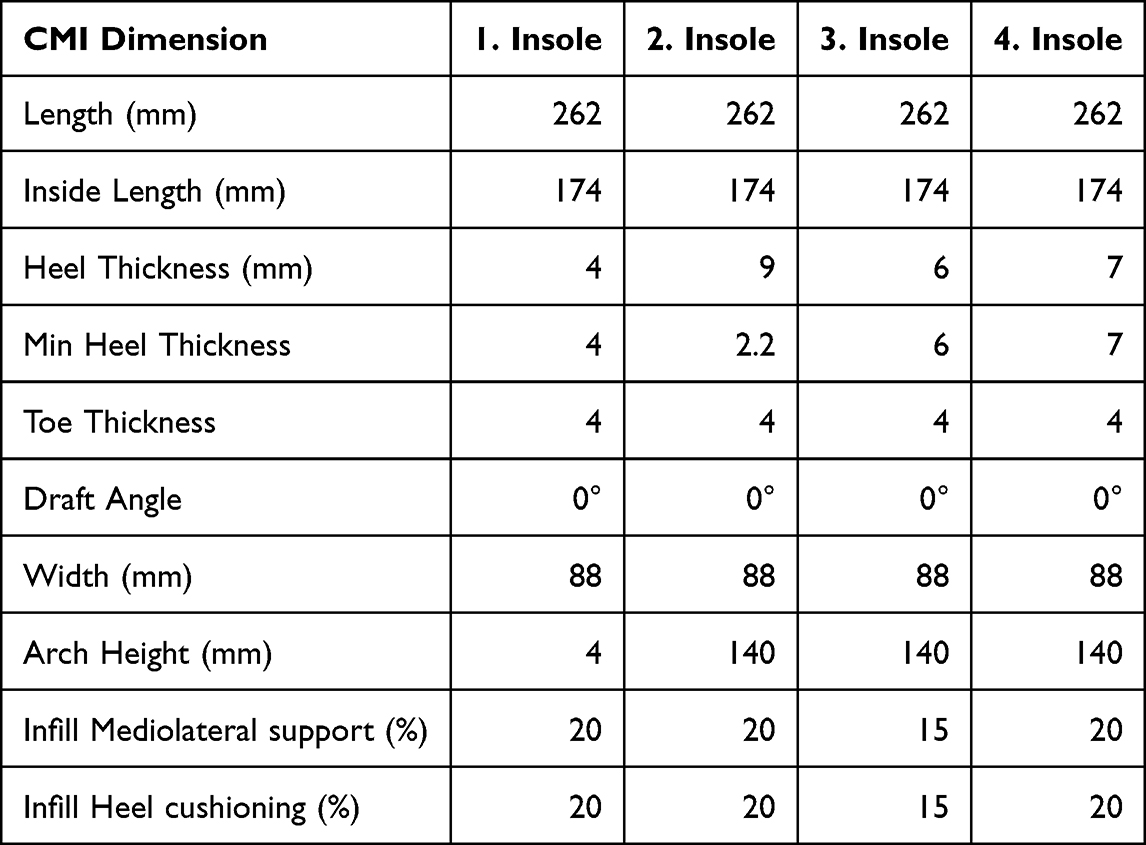 |
Table 1 Dimensional Comparison of 3D-Printed Prototypes |
1. Insole: without correction elements; The first surface did not show aspects of raised corrections, only places of partial springing.
2. Insole: The second suggestion insisted on adherence to the medical examination and the results from the motion analysis with a recommendation for pronounced heel support (heel cup), supported foot arch, and support in the metatarsal area.3,4,9,14,16,17
3. Insole: The third proposal resulted from a search of scientific articles on forming lightweight elastic structures7,10,19,23,24 and their definition of FO.1,2,27 It was a composition inspired by commercial over-The-counter insoles designed to run25 with slight modifications of preset parameters in specialist insoles creation software (Gensole EasyCAD, Gyrobot, UK).35
This way, three insoles’ prototypes with different material layering were made additively, which served as a prototype to test the dimensional shapes and comfort.
4. Insole: Based on the statistical analyses of the comfort and visual assessment by the physician, and the technician, a compromise solution was chosen, combining the last two designs (Figure 7).
3D Printing Parameters of Final Insole
Profile: Draft −0.2mm; Infill Density: 20%, Infill Line Distance: 2.0 mm; Infill Pattern: Zig Zag; Infill Overlap Percentage: 10.0%; Infill Overlap: 0.04 mm; Infill Wipe Distance: 0.1 mm; Infill Layer Thickness: 0.2 mm; print speed 15 mm/s, print temperature 240∘C, wire diameter23 1.75 mm; filament flow: 112%.
The “zig-zag” pattern10,11,29 was used for the fill because it can form the filling of the printout in one stroke without interruption, which avoids sliding along the Z-axis and therefore avoids stringing. When printing flexible materials, the recommended printing speed is 20 mm/s. However, our 3D printer has above-average vibrations during printing, so the rate was set to 15 mm/s due to poor-quality bearings. The number of layers on the top and bottom24 of the insole was appointed to three for optimum integrity24 and strength. Since in a print that is made up of different percentage densities of fill (Figure 8), the fillings are not connected in any way. This means that the filler of the print only adheres to the top and bottom layers.
The printing temperature of the flexible material was set to 240 °C based on the filament manufacturer’s recommendations and the experiment. The filament flow was set to 112% to achieve optimum flow. It was found experimentally that setting the increased filament flow from 105–120% for direct extruder printers when printing with flexible filament is common. When pushing the filament through the nozzle, unwanted shrinkage occurs, which is solved by setting a higher filament flow rate, thus also avoiding problems with a lack of material coming out of the nozzle when the flow is interrupted when the nozzle is moved to a new initial position or when changing the layer.
As with flexible materials, to achieve the highest quality printout, retraction is disabled in the settings to ensure a stable supply of filament volume from the nozzle. Therefore, it is necessary to specify in the settings to move the hotend (end nozzle) only within the print to prevent stringing (ie, wetting, whiskers, or “hair patterns” when plastic threads remain on the 3D printed model). The flexible filaments of the Filaflex range have excellent adhesion (Figure 8) to the printing pad, so a heated bed is not necessary, nor are additional aids for better adhesion. Nevertheless, commercial hairspray was used as an adhesive layer on the place. The layer height is set to double when creating the first layer on the pad. The modification creates a better quality first layer and adhesion to the bed.
Testing Prototypes and Statistical Analyses
To unambiguously interpret the workflow and decision-making process during insoles testing,2 we applied the machine learning technique and created a decision tree.12,32,33,36 Feedback information can improve the performance of classification12 and manufacturing.32 The produce of the first CMIs undertook a deeper examination of parameter optimization,12 morphology shape10 selection and inside density.1 Every prototype was created and tested using a novel procedural algorithm (Figure 9). Different densities and geometry shapes on prototypes have been applied to investigate19 and analyze the comfort of CMIs. The Pain Score of each CMI (routine of five-day workouts per month for CMI). The mean, SD, and range were calculated for all investigated measures (Table 2). The Shapiro–Wilk tests did not show a significant departure from the normality, W (20) = 0.928, p = 0.140. The data does not contain any extreme values. The selections have noted the same variance. A one-way analysis of variance (ANOVA) was performed24 to investigate the differences between each CMI (Table 2). A significance level set a p<0.05. The results showed significant differences between the samples (p<0.05, F>F crit). The podiatry examination identified four problematic aspects (Knees, Heel Cushioning, Arch support, and Heel Cup Fit). We paid particular attention to them during testing and had them rated on a five-point comfort scale, indexing from −4 very uncomfortable, −2 uncomfortable, 0 neutral, +2 comfortable, +4 very comfortable (Table 3). Based on testing results, we found a practical solution to the problem and examined the comfort of corrective elements.
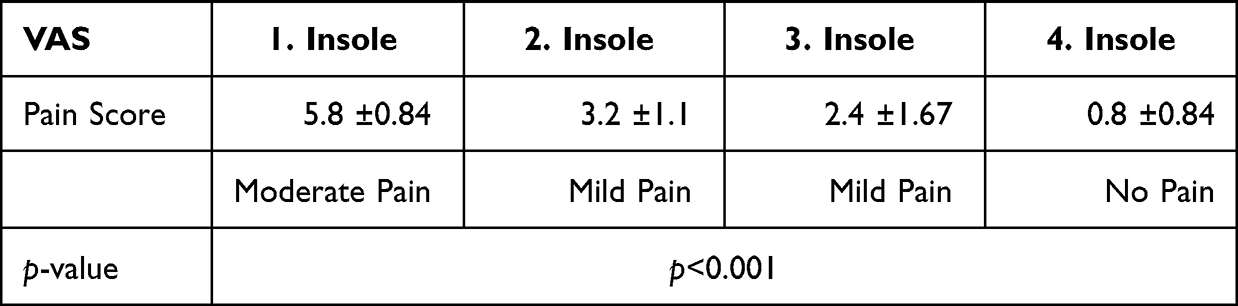 |
Table 2 Pain Score Evaluation (VAS)36 After Five Running Workouts |
 |
Table 3 Comfort Score Evaluation (VAS)36 After Five Running Workouts |
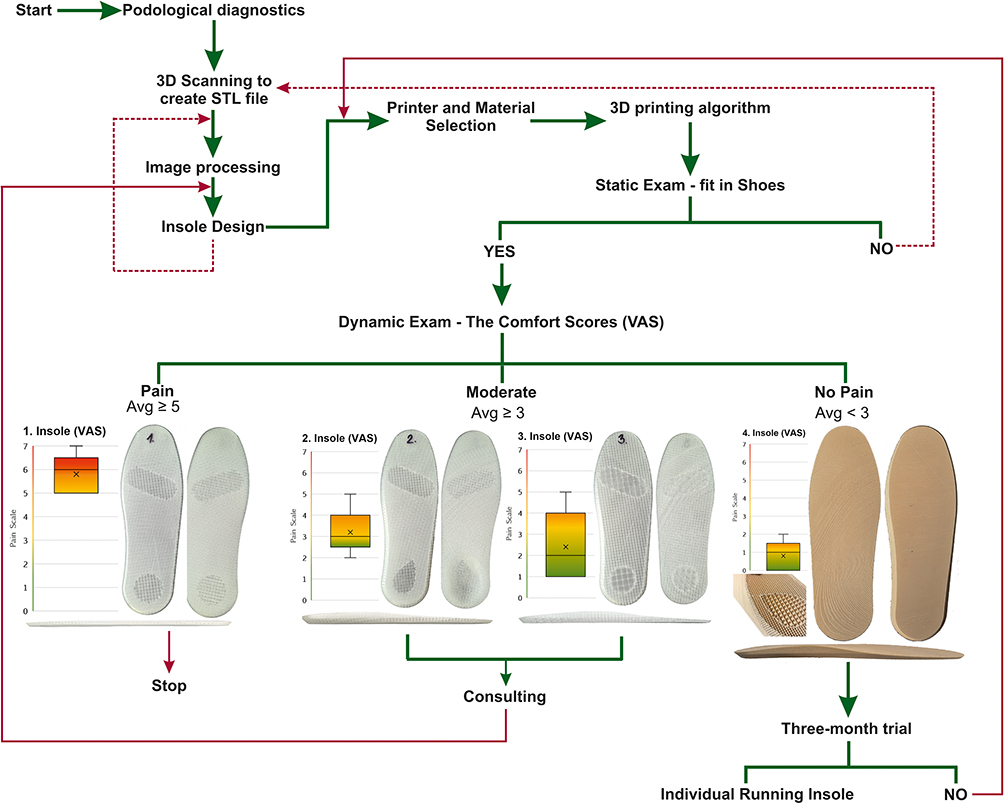 |
Figure 9 Flowchart of Workflow (the Decision Tree Method). |
The Comfort Test of each CMI (five workouts per month for each CMI): The mean, standard deviation (SD), and range were calculated for all the measures investigated (Table 3). The smaller the p-value, the more it supports H1. Anova: Two-Factor Without Replication confirms significant differences between problematic aspects and prototypes (p <0.001). The cushioning of the heel, solved by the porous internal structure and the support of the arch, significantly affects shock absorption and the perception of comfort.
The Comfort Test of the final CMI (eight running workouts per month for three months; twenty-four workouts for three months) was evaluated on a five-point comfort scale (−4 very uncomfortable, −2 uncomfortable, 0 neutral, +2 comfortable, +4 very comfortable): The mean and SD were calculated for all the measures investigated (Table 4). The Shapiro–Wilk tests did not show a significant departure from the normality (W (24) = 0.937, p = 0.138). The results found are more than satisfactory. After three months of training, the overall perception of comfort was comfortable (2.8 ±1.5) but neutral for the knees (1.3±2.3).
 |
Table 4 Comfort Score Evaluation (VAS)36 After Three Months Running Workouts |
Discussion
Methods
Previous studies deal with (1.) the comparison of the production method3–5,7,15,21,27,28 and, therefore, the calculation of the difference between traditional plaster-molden and additive insole production. Based on this criterion, especially from an ecological point3 of view and repeatability,7 3D printing is more universal. In this case, aspects such as time-consuming processes,3,7 material waste3,7 minimizations, and dependence on the skills level3,7 of the orthopedic technician in input measurements and production are essential.2,3,15,38–41 This makes the procedures challenging to standardize3,7 and replicate3,7 and increases costs.2,7,27 On the other hand, thanks to artificial intelligence33,36 and machine learning,12,32 development in the technical field is constantly progressing, making it possible to automate individual procedures,2 speed up the work process, and reduce costs.3,7,27 Through 3D and 4D scanning,37 we can obtain the virtual9 geometry of the scanned object, which can be archived and, if necessary, compared4 over time.2,37
Nowadays, more and more emphasis is being placed on the environment and saving and recycling materials. One way to achieve this in the field of individual medical device manufacturing is through the introduction of digitization and the use of zero-waste technology like additive manufacturing.7 The minimal waste generated during 3D printing can be recycled and reused.19 Fabricating insoles in the traditional way3,4,7,15 of obtaining input data or gluing individual components from different types of material3,38 produces a significantly higher carbon footprint. From this point of view, the topic of the present study concerning the 3D printing of running insoles is eminently topical.
Moving to 3D-printed shoe insoles, individual parts, and the whole shoe gives designers and manufacturers more creative freedom.1 The overall workflow12 would be short, and the number of tools and aids currently necessary for production would be reduced. Simplifying the production cycle would streamline production and increase productivity, which would positively reflect the economics of the provider in question and the time saved.2
Digitization makes it possible to consider biomechanical4 aspects of movement and posture.1,4,24,36,38,39 Different scanning equipment,3,7,23 aids, and capture positions3,7,23 were described and used in individual studies.2 Some authors have used a scanner designed directly to capture legs with a predefined sitting position with a reference location and alignment of the feet.3,23 Others captured the foot in a prone position,7 etc. One study compared individual positions with the traditional plaster-based4,7 position. The authors found that body location did not matter. Correct foot alignment and a neutral angle in the TC3 are limiting.7 Our proband stood on one leg while the sensed limb kneeled on a chair.
We chose a capture position that we did not find among the reviewed studies, but we can recommend it considering the result. It reduces the requirement for space for measuring compared to capturing in a horizontal position on the bed.
The artificial intelligence26,37 (AI) in current 3D scanners allows scanning of the entire foot and can also cope with possible micro-movements during active positioning in the TC. Of course, data processing algorithms,15 3D point accuracy, 3D resolution, and others play an essential role in quality.1 Outside of this study, we also tried scanning using a mobile application, and the result was a usable 3D model; it just required more adjustments.
The 3D model of the foot can be edited in freely available CAD software,1,8 and thanks to parametric modeling,8 it is user-friendly to design7 CMIs. Simulation9 tools allow applying and visualizing the pressure data1,7,9,37 obtained by the podological scan and setting of the correction elements3 on the CMIs accordingly. However, the market lacks a comprehensive workflow for customizing the liner design.1,12 This situation calls for extensive research and logistical procedures.2
Progress7 in digitalization, additive manufacturing, materials science,20 and CAD/CAM software1–3,7,37 have allowed us to create new 3D-printed running CMIs whose mechanical properties are derived from the TPU material and printing parameters7 of Infill (such as Density, Line Distance, Pattern, Overlap, Layer Thickness, etc.) print speed7 and temperature and filament flow.
Materials
Recent studies (2) were limited to easily printable materials7 such as ABS (acrylonitrile butadiene styrene) or more used PLA40 (polylactic acid).7,19 However, neither PLA nor ABS meets the mechanical properties for a fully loaded3 insole for regular use.7,19 These thermoplastic filaments are suitable for creating reinforced insole components or shaped prototypes. They are cheap,19 recyclable materials that are easy to print7 and intended for basic shape testing.19
In contrast, using new TPU materials appears highly effective, cheap, and highly resistant to mechanical stress. Our study is based on such findings. For this purpose, we decided to use a low-cost printer and flexible TPU material suitable for contact with skin and fit for immediate use without post-processing. Each 3D printer prints differently, so before introducing a new material, it is necessary to tune the settings to achieve the desired product quality. The final production parameters were determined by the experimental printing of the sample (a cube with a volume of 8cm3) to assess the mechanical properties and print quality.
Individuality
Previous studies worked with several participants.3,6,7,15 Unlike them, we decided to aim to solve the needs of one individual with higher weight and knee pain. We focused on the painful symptoms of one proband. For this reason, we tried 3D printing different infill and correction components.
Efficiency
Studies comparing additive and traditional manufacturing methods3–5,7,11,15,21,27,28 have focused on dimensional evaluation,28 analysis of perceived comfort3,6,7 during a certain period of use, and practical solutions for bilateral3 and unilateral heel3,28 pain and walking pain.1,4–6 They reported no significant or greater differences in biomechanical4,6 and comfort parameters.6,7 Studies dedicated to the research of the 3D printed insole declare its big potential in physiotherapeutic intervention1 at different degrees of FPI (Foot Posture Index3) and during ordinary use.28 They highlight the precision, quality, repeatability of production, and the effect of reducing plantar pressure3,9 and painful symptoms.28 They point out the positive effects of medial pressure3 distribution on 3D printed insoles and suggest a beneficial effect on human gait biomechanics4 with a diagnosis of pes planus.5,21,28
However, the analytical study11 found variances between the evaluation for plantar pressures and the biomechanical gait analysis4,6,9,21 while using the 3D-printed insole, etc.6 The analysis concluded that further research was needed because of insufficient evidence.6,21
Current research is rather oriented towards testing the effect of an already manufactured3,38 individual shoe insole. Only a few articles are devoted to the production without mentioning the printing parameters.18 Our contribution is using a low-cost printer and material suitable for contact with skin. We present a completely new and complete digital workflow with 3D printing parameters.
Based on the above, we feature a new digital workflow12 with 3D-printing algorithms for 3d-printed insoles. The decision tree method makes it possible to facilitate the decision-making procedure for further research and its possible optimization. It increases the repeatability and reproducibility of the workflow.32
We tested the participant’s perception of shock absorption around the heel and metatarsals. We aim not to create a universal insole. We wanted to develop a procedural algorithm for manufacturing and testing for the subsequent expansion of the participant database. The benefits of our research are the mentioned 3D printing algorithms and workflow for prototype testing.
Limits
The very demanding thing was to create a long-term sustainable training program. We need to count on a series of repetitions and effort to keep the motivation of the proband. Developing a monitoring application that would allow monitoring and communication with the subject would be interesting.33 In the future, we need to expand communication channels and make information sharing between the proband and the research team more efficient.
Conclusion
In conclusion, we can conclude that we managed to create a working algorithm for the entire production process of a 3D-printed insert and establish decision criteria for assessing quality and comfort. Four prototypes were made according to the selected parameters and recommendations. The final product was designed and printed based on evaluations of these four prototypes. Final CMIs were tested for three months. Then, their influence on the perception of comfort and pain was analyzed. The study concludes that 3D-printed shoe inserts made of TPU material and a customized internal structure with corrective elements in the form of springing around the metatarsals bar and heel, with the support of the longitudinal arch, can redistribute pressure and increase the feeling of comfort. In pursuance of feedback from the proband, we found that the inserts increased his movement activities and reduced pain in the knee joints. During the long-term use, some suggestions for improvement and the design of a new prototype were discussed.
However, it is necessary to continue the development of the 3D-printed running insole. We plan to synchronize and evaluate subjective feelings compared to the material’s mechanical wear and with objective data from gait analyses.
Ethics Statement
The presented paper’s study is entirely original, and none of it has been previously published. Written Informed Consent and Patient Consent for Publication were obtained from the participant in this study before her participation. The study has been reviewed and approved by the ethics committee of the Technical University of Kosice File no. 26272/2023/R-OLP.
Acknowledgments
This publication is the result of the project implementation: Open scientific community for modern interdisciplinary research in medicine (Acronym: OPENMED), ITMS2014+: 313011V455 supported by the Operational Programme Integrated Infrastructure funded by the European Regional Development Fund.
This work was supported by the Slovak Research and Development Agency under contract No. APVV-19-0290 (Research and development of lower limb prosthetic sockets manufactured by additive technologies).
This work was supported by the Slovak Research and Development Agency under contract No. APVV-20-0068 (Development of new bioresorbable alloys for invasive implants).
This work was supported by the Slovak Research and Development Agency under contract No. APVV-17-0278 (Research of additive manufacturing of biodegradable magnesium alloys and their applications in implantology and regenerative medicine).
This research was supported by project KEGA 050TUKE-4/2022 Additive manufacturing in medicine - creation of multimedia material and tools to support teaching in biomedical engineering.
This publication is the result of the project implementation CEMBAM - Center for Medical Bioadditive Research and Production, ITMS2014+: 313011V358 supported by the Operational Programme Integrated Infrastructure funded by the European Regional Development Fund.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhao Y, Zhong J, Wang Y, et al. Photocurable and elastic polyurethane based on polyether glycol with adjustable hardness for 3D printing customized flatfoot orthosis. Biomater Sci. 2023;11(5):1692–1703. doi:10.1039/d2bm01538b
2. Mandolini M, Brunzini A, Germani M. A collaborative web-based platform for the prescription of custom-made insoles. Adv Eng Inf. 2017a;33:360–373. doi:10.1016/j.aei.2016.10.004
3. Xu R, Wang Z, Ren Z, et al. Comparative study of the effects of customized 3D printed insole and prefabricated insole on plantar pressure and comfort in patients with symptomatic flatfoot. Med Sci Monit. 2019;25:3510–3519. doi:10.12659/MSM.916975
4. Ho M, Nguyen J, Heales L, Stanton R, Kong PW, Kean C. The biomechanical effects of 3D printed and traditionally made foot orthoses in individuals with unilateral plantar fasciopathy and flat feet. Gait Posture. 2022;96:257–264. doi:10.1016/j.gaitpost.2022.06.006
5. Lucas-Cuevas AG, Camacho-García A, Llinares R, Priego Quesada JI, Llana-Belloch S, Pérez-Soriano P. Influence of custom-made and prefabricated insoles before and after an intense run. PLoS One. 2017;12(2):e0173179. doi:10.1371/journal.pone.0173179
6. Daryabor A, Kobayashi T, Saeedi H, Lyons SM, Maeda N, Naimi SS. Effect of 3D printed insoles for people with flatfeet: a systematic review. Assist Technol. 2023;35(2):169–179. doi:10.1080/10400435.2022.2105438
7. Brognara L, Fantini M, Morellato K, Graziani G, Baldini N, Cauli O. Foot orthosis and sensorized house slipper by 3D printing. Materials. 2022;15(12):4064. doi:10.3390/ma15124064
8. Fantini M, De Crescenzio F, Brognara L, Baldini N. Design and rapid manufacturing of a customized foot orthosis: a first methodological study. In: Eynard B, Nigrelli V, Oliveri S, Peris-Fajarnes G, Rizzuti S, editors. Advances on Mechanics, Design Engineering and Manufacturing: Lecture Notes in Mechanical Engineering. Cham, Switzerland: Springer; 2017.
9. Telfer S, Woodburn J, Collier A, Cavanagh PR. Virtually optimized insoles for offloading the diabetic foot: a randomized crossover study. J Biomech. 2017;60:157–161. doi:10.1016/j.jbiomech.2017.06.028
10. Hu CW, Nguyen CT, Holbling D. A novel 3D printed personalised insole for improvement of flat foot arch compression and recoil - preliminary study. Proc Inst Mech Eng Part L. 2023;237(2):329–342.
11. Farhan M, Wang JZ, Bray P, Burns J, Cheng TL. Comparison of 3D scanning versus traditional methods of capturing foot and ankle morphology for the fabrication of orthoses: a systematic review. J Foot Ankle Res. 2021;14(1):2. doi:10.1186/s13047-020-00442-8
12. Chhikara K, Sidhu SS, Gupta S, Saharawat S, Kataria C, Chanda A. Development and effectiveness testing of a novel 3D-printed multi-material orthosis in nurses with plantar foot pain. Prosthesis. 2023;5(1):73–87. doi:10.3390/prosthesis5010006
13. Riddick R, Farris DJ, Kelly LA. The foot is more than a spring: human foot muscles perform work to adapt to the energetic requirements of locomotion. J R Soc Interface. 2019;16(150):20180680. doi:10.1098/rsif.2018.0680
14. Bus SA, van Deursen RW, Armstrong DG, et al. Footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in patients with diabetes: a systematic review. Diabetes Metab Res Rev. 2016;32(Suppl 1):99–118. doi:10.1002/dmrr.2702
15. Lee KKW, Ling SKK, Yung PSH. Controlled trial to compare the achilles tendon load during running in flatfeet participants using a customized arch support orthoses vs an orthotic heel lift. BMC Musculoskelet Disord. 2019;20(1):535. doi:10.1186/s12891-019-2898-0
16. Jafarnezhadgero A, Alavi-Mehr SM, Granacher U, Boullosa D. Effects of anti-pronation shoes on lower limb kinematics and kinetics in female runners with pronated feet: the role of physical fatigue. PLoS One. 2019;14(5):e0216818. doi:10.1371/journal.pone.0216818
17. Zhang X, Delabastita T, Lissens J, De Beenhouwer F, Vanwanseele B. The morphology of foot soft tissues is associated with running shoe type in healthy recreational runners. J Sci Med Sport. 2018;21(7):686–690. doi:10.1016/j.jsams.2017.11.008
18. Jandova S, Mendricky R. Benefits of 3D printed and customized anatomical footwear insoles for plantar pressure distribution. 3D Print Addit Manuf. 2022;9(6):547–556. doi:10.1089/3dp.2021.0002
19. Hudak YF, Li JS, Cullum S, et al. A novel workflow to fabricate a patient-specific 3D printed accommodative foot orthosis with personalized latticed metamaterial. Med Eng Phys. 2022;104:103802. doi:10.1016/j.medengphy.2022.103802
20. Muir BC, Li JS, Hudak YF, Kaufman GE, Cullum S, Aubin PM. Evaluation of novel plantar pressure-based 3-dimensional printed accommodative insoles - a feasibility study. Clin Biomech. 2022;98:105739. doi:10.1016/j.clinbiomech.2022.105739
21. Lucas-Cuevas AG, Pérez-Soriano P, Priego-Quesada JI, Llana-Belloch S. Influence of foot orthosis customisation on perceived comfort during running. Ergonomics. 2014;57(10):1590–1596. doi:10.1080/00140139.2014.938129
22. Wang K, Lu C, Ye R, et al. Research and development of 3D printing orthotic insoles and preliminary treatment of leg length discrepancy patients. Technol Health Care. 2020;28(6):615–624. doi:10.3233/THC-202170
23. Anderson J, Williams AE, Nester C. Development and evaluation of a dual density insole for people standing for long periods of time at work. J Foot Ankle Res. 2020;13(1):42. doi:10.1186/s13047-020-00402-2L
24. Kharazi M, Bohm S, Theodorakis C, Mersmann F, Arampatzis A. Quantifying mechanical loading and elastic strain energy of the human achilles tendon during walking and running. Sci Rep. 2021;11(1):5830. doi:10.1038/s41598-021-84847-wK
25. Phits Orthotics Custom 3D-printed orthotic insoles. Available from:© Copyright Materialise 2023. https://www.materialise.com/it/healthcare/phits-suite/phits-3d-printed-orthotics.
26. Desmyttere G, Leteneur S, Hajizadeh M, Bleau J, Begon M. Effect of 3D printed foot orthoses stiffness and design on foot kinematics and plantar pressures in healthy people. Gait Posture. 2020;81:247–253. doi:10.1016/j.gaitpost.2020.07.146
27. Roberts A, Wales J, Smith H, Sampson CJ, Jones P, James M. A randomised controlled trial of laser scanning and casting for the construction of ankle-foot orthoses. Prosthet Orthot Int. 2016;40(2):253–261. doi:10.1177/0309364614550263
28. Ho M, Nguyen J, Talbot K, et al. Immediate comfort perception of 3D-printed foot orthoses in individuals with unilateral heel pain. Prosthet Orthot Int. 2022;46(1):31–36. doi:10.1097/PXR.0000000000000068
29. Trebunova M, Danko M, Bednarcikova L, et al. The effect of footwear to the posture. Lek Tech. 2020;50:58–64. doi:10.14311/ctj.2020.2.03
30. Thurzo A, Šufliarsky B, Urbanová W, Čverha M, Strunga M, Varga I. Pierre Robin sequence and 3D printed personalized composite appliances in interdisciplinary approach. Polymers. 2022;14(18):3858. doi:10.3390/polym14183858
31. Danko M, Michalikova M, Bednarcikova L, Trebunova M, Nalevankova M, Hudak R. Design of thermoplastic immobilization forearm splints. Acta Tecnol. 2020;6(3):69–72. doi:10.22306/atec.v6i3.84
32. Trentzsch K, Schumann P, Śliwiński G, et al. Using machine learning algorithms for identifying gait parameters suitable to evaluate subtle changes in gait in people with multiple sclerosis. Brain Sci. 2021;11(8):1049. doi:10.3390/brainsci11081049
33. Thurzo A, Kurilová V, Varga I. Artificial intelligence in orthodontic smart application for treatment coaching and its impact on clinical performance of patients monitored with AI-TeleHealth system. Healthcare. 2021;9(12):1695. doi:10.3390/healthcare9121695
34. Filaflex 82A (filament) [datasheet]. Available from: © 2022 RECREUS INDUSTRIES S.L.™. https://recreus.com/gb/filaments/9-filaflex-82a.html.
35. Liu X, Yang XS, Wang L, Yu M, Liu XG, Liu ZJ. Usefulness of a combined approach of DIERS formetric 4D® and QUINTIC gait analysis system to evaluate the clinical effects of different spinal diseases on spinal-pelvic-lower limb motor function. J Orthop Sci. 2020;25(4):576–581. doi:10.1016/j.jos.2019.09.015
36. Banga HK, Kumar R, Kalra P, Belokar RM. Book Additive Manufacturing with Medical Applications. CRC Press; 2022.
37. Scott C. Design Your Own 3D Printable Insoles with Gensole, a Free Browser-Based Tool from Gyrobot.2016; Available from:3DPrint.com. https://3dprint.com/140373/gensole-3d-printable-insoles/.
38. Delgado DA, Lambert BS, Boutris N, et al. Validation of digital visual analog scale pain scoring with a traditional paper-based visual analog scale in adults. J Am Acad Orthop Surg. 2018;2(3). doi:10.5435/JAAOSGlobal-D-17-00088
39. Costa BL, Magalhães FA, Araújo VL, et al. Is there a dose-response of medial wedge insoles on lower limb biomechanics in people with pronated feet during walking and running? Gait Posture. 2021;90:190–196. doi:10.1016/j.gaitpost.2021.09.163
40. Jin H, Xu R, Wang S, Wang J. Use of 3D-printed heel support insoles based on arch lift improves foot pressure distribution in healthy people. Med Sci Monit. 2019;25:7175–7181. doi:10.12659/MSM.918763
41. Telfer S, Abbott M, Steultjens MP, Woodburn J. Dose-response effects of customised foot orthoses on lower limb kinematics and kinetics in pronated foot type. J Biomech. 2013;46(9):1489–1495. doi:10.1016/j.jbiomech.2013.03.036
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.