Back to Journals » Orthopedic Research and Reviews » Volume 8
3D-printed patient-specific applications in orthopedics
Authors Wong KC ![]()
Received 1 August 2016
Accepted for publication 9 September 2016
Published 14 October 2016 Volume 2016:8 Pages 57—66
DOI https://doi.org/10.2147/ORR.S99614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Video abstract presented by Kwok Chuen Wong
Views: 8961
Kwok Chuen Wong
Department of Orthopedics and Traumatology, Prince of Wales Hospital, The Chinese University of Hong Kong, Shatin, Hong Kong
Abstract: With advances in both medical imaging and computer programming, two-dimensional axial images can be processed into other reformatted views (sagittal and coronal) and three-dimensional (3D) virtual models that represent a patients’ own anatomy. This processed digital information can be analyzed in detail by orthopedic surgeons to perform patient-specific orthopedic procedures. The use of 3D printing is rising and has become more prevalent in medical applications over the last decade as surgeons and researchers are increasingly utilizing the technology’s flexibility in manufacturing objects. 3D printing is a type of manufacturing process in which materials such as plastic or metal are deposited in layers to create a 3D object from a digital model. This additive manufacturing method has the advantage of fabricating objects with complex freeform geometry, which is impossible using traditional subtractive manufacturing methods. Specifically in surgical applications, the 3D printing techniques can not only generate models that give a better understanding of the complex anatomy and pathology of the patients and aid in education and surgical training, but can also produce patient-specific surgical guides or even custom implants that are tailor-made to the surgical requirements. As the clinical workflow of the 3D printing technology continues to evolve, orthopedic surgeons should embrace the latest knowledge of the technology and incorporate it into their clinical practice for patient-specific orthopedic applications. This paper is written to help orthopedic surgeons stay up-to-date on the emerging 3D technology, starting from the acquisition of clinical imaging to 3D printing for patient-specific applications in orthopedics. It 1) presents the necessary steps to prepare the medical images that are required for 3D printing, 2) reviews the current applications of 3D printing in patient-specific orthopedic procedures, 3) discusses the potential advantages and limitations of 3D-printed custom orthopedic implants, and 4) suggests the directions for future development. The 3D printing technology has been reported to be beneficial in patient-specific orthopedics, such as in the creation of anatomic models for surgical planning, education and surgical training, patient-specific instruments, and 3D-printed custom implants. Besides being anatomically conformed to a patient’s surgical requirement, 3D-printed implants can be fabricated with scaffold lattices that may facilitate osteointegration and reduce implant stiffness. However, limitations including high cost of the implants, the lead time in manufacturing, and lack of intraoperative flexibility need to be addressed. New biomimetic materials have been investigated for use in 3D printing. To increase utilization of 3D printing technology in orthopedics, an all-in-one computer platform should be developed for easy planning and seamless communications among different care providers. Further studies are needed to investigate the real clinical efficacy of 3D printings in orthopedic applications.
Keywords: 3D printing, patient-specific orthopedics, custom implants, patient-specific instrument, image processing
Introduction
Orthopedics is a surgical discipline that is commonly tied to biomedical engineering, which has been applied to various orthopedic disciplines, ranging from trauma surgery, joint arthroplasty, and tumor surgery to deformity correction. One of the reasons for the success of these applications is the contemporary medical imaging technologies that have allowed for detailed analysis of the individual’s musculoskeletal system. With advances in both medical imaging and computing programming, virtual models that are representative of patients’ own anatomy can be generated for planning patient-specific orthopedic procedures.
From preoperative planning to training and education to implant designing, the use of three-dimensional (3D) printing is rising and has become more prevalent in medical applications over last decade as surgeons and researchers are increasingly utilizing the technology’s flexibility in manufacturing objects. 3D printing is a type of manufacturing process in which materials such as plastic or metal are deposited in layers to create a 3D object from a digital model.1 The process is distinct from traditional manufacturing methods in that it is an additive rather than a subtractive process. Specifically in surgical applications, the 3D printing techniques can not only generate models that give a better understanding of the complex anatomy and pathology of the patients,2 but can also produce patient-specific instruments (PSIs)3–11 or even custom implants12,13 that are tailor-made to the surgical requirements.
Only a few papers have recently reviewed the 3D printing technology and its medical applications.2,14–16 However, they were reported mainly from the perspectives of radiologists, surgeons, and engineers. Although relevant studies and clinical data on 3D printing in orthopedics are limited, its potential in personalized treatment in orthopedics is huge. As the clinical applications of 3D printing continue to evolve, orthopedic surgeons should embrace the latest knowledge of the technology and incorporate it into their clinical practice for possible benefits to patients. This paper is written to help orthopedic surgeons stay up-to-date on the emerging 3D technology, starting from the acquisition of clinical imaging to 3D printing for patient-specific applications in orthopedics. The paper 1) presents the necessary steps to prepare the medical images that are required for 3D printing, 2) reviews the current applications of 3D printing in patient-specific orthopedic procedures, 3) discusses the potential advantages and limitations of 3D-printed custom orthopedic implants, and 4) suggests the directions for future development.
Patient-specific orthopedics
In traditional orthopedic procedures, surgeons have to mentally integrate all preoperative two-dimensional (2D) images and formulate a 3D surgical plan. This preoperative planning is particularly difficult in areas that have complex anatomy and severe deformity or in cases of bone tumor surgery. With the advent of volumetric medical imaging and computing technology, 2D axial images can be processed into other reformatted views (sagittal and coronal), and 3D virtual models with patient-specific anatomy can be created. With improved visualization, surgeons can then analyze this processed information to make more detailed diagnosis, planning, and surgical intervention on a patient-specific basis.
Although frequently used, the term “patient-specific” has not been clearly defined. An orthopedic surgeon may intuitively refer to it as the unique bone geometry or density that is assessed using the patient’s medical images. Other factors like material properties, design of orthopedic implants, or force acting on an individual patient may be incorporated qualitatively in the decision of “patient-specific” orthopedic treatment. On the other hand, the outcome for a particular treatment is based on the results of clinical trials that are only average estimates of different patients within the trials. These average results might not apply directly to individual patients for whom surgeons care.17 In biomedical engineering, patient-specific modeling (PSM) is the development of computational models of human pathophysiology that are personalized to patient-specific data.18 PSM is gaining more attention because of its potential to optimize an individual’s treatment by predicting outcomes of surgical interventions. It has been utilized in optimizing the preoperative planning of periacetabular osteotomies in hip dysplasia19,20 and in predicting the outcome of corrective surgery in scoliosis21,22 and bony reconstruction with a custom implant after complex pelvic tumor resection.23 Although PSM is beyond the scope of discussion of this paper, the combination of PSM and 3D printing technology has been increasingly used in patient-specific orthopedic applications such as for the creation of anatomic models for surgical planning, education and training, PSIs, and custom implants (Figure 1).
 | Figure 1 This image summarizes the clinical workflow of patient-specific orthopedics from image acquisition to 3D-printed models and implants. Notes: The workflow requires close collaboration between surgeons and engineers to achieve the surgery that is customized to the patient’s anatomy and surgical requirement. Abbreviations: CT, computer tomography; MR, magnetic resonance; FEA, finite element analysis. |
Image acquisition to generation of 3D objects
For patient-specific analysis in orthopedic applications, accurate medical imaging data must be obtained to represent an individual patient. The modern multirow detector computer tomography (MDCT) and magnetic resonance imaging (MRI) provide fast and accurate 3D image data with high resolution. With image postprocessing tools, it is possible to produce multiplanar reformatted 2D images and 3D views of the patient’s anatomy. The technique of converting digital medical images into a 3D physical object has been described in detail in a previously published review article.14 The conversion consists of three steps: 1) image acquisition, 2) image postprocessing, and 3) 3D printing.
Image acquisition
High-quality medical images must be acquired first as the resolution of 3D objects generated from medical images is dependent on the resolution of the medical images themselves. The quality of the 3D object cannot outreach the quality of its raw 2D imaging data. Both MDCT and MRI are commonly used imaging modalities. Because of high contrast in CT, it is the imaging modality of choice in orthopedics when bones are the region of interest for an imaging study. MDCT can produce thin-section axial image with slice thickness of less than 1 mm and isotropic voxel. These high-resolution CT images are ideal to facilitate the image postprocessing for 3D applications.24 MRI has the advantage of no radiation exposure during image acquisition. It is superior to CT in delineating soft tissue anatomy, such as that of articular cartilage in joint disease and intramedullary or extraossoeus extension in orthopedic tumors. However, it is more difficult to obtain thin 1–2 mm thick MR slices for image postprocessing as the image quality of the MRI can be adversely affected by movement artifacts generated during the long scanning times.25 Therefore, image postprocessing in orthopedic applications is mainly based on CT images and supplemented with tissue information from MRI. All the acquired medical images are saved in digital imaging and communications in medicine (DICOM), which is a standard data format to store, exchange, and transmit medical images.
Image postprocessing
Image postprocessing software extracts DICOM images for data reconstruction. Thin-section axial images are used to create nonaxial 2D images by means of multiplanar reformation.24 The additional reformatted coronal or sagittal images can then be visualized for better clinical interpretation (Figure 2). This technique is particularly useful for examining skeletal structures as some information like fractures or joint alignment may not be readily apparent on axial sections. Other 3D visualization tools such as volume rendering generate 3D representations of the data set. Image segmentation is usually required to select regions of interest within the image data. Thresholding voxel intensity value is a technique that is commonly applied in segmenting regions that uniformly differ in intensity from their surrounding tissue, such as bone. 3D objects can be generated from the segmented regions of interest. Computer-aided design (CAD) software transforms the contour of a 3D model into a series of polygons, usually triangles, the number of which directly correlates with resolution.26 The CAD information is then converted into a common 3D file format, STereoLithography (STL). Further editing of the STL files like optimization of triangular meshes or modification of object geometries can be performed before the CAD data are sent to a 3D printing machine for object fabrication (Figure 3). Therefore, DICOM images are the key link between 3D printing technology and patient-specific medical imaging data in orthopedics.26
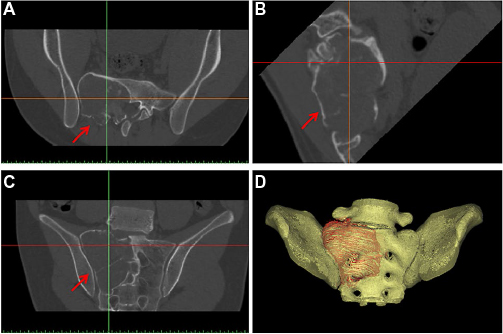 | Figure 2 Axial CT images were acquired in a patient with low-grade osteosarcoma involving the sacrum (red arrows). Notes: The CT images in DICOM format were imported into a CAD engineering program. As the sacrum was at a tilted position during CT scanning, the image data set could be resliced to allow better visualization of sacrum in its anatomical alignment. The extent of the tumor could also be segmented manually from the images. The reformatted axial (A), coronal (B), and sagittal (C) views, and the 3D bone-tumor model (D) enabled surgeons to analyze the patient’s anatomy and pathology accurately for customized surgical planning. Abbreviations: CT, computer tomography; CAD, computer-aided design; DICOM, digital imaging and communications in medicine. |
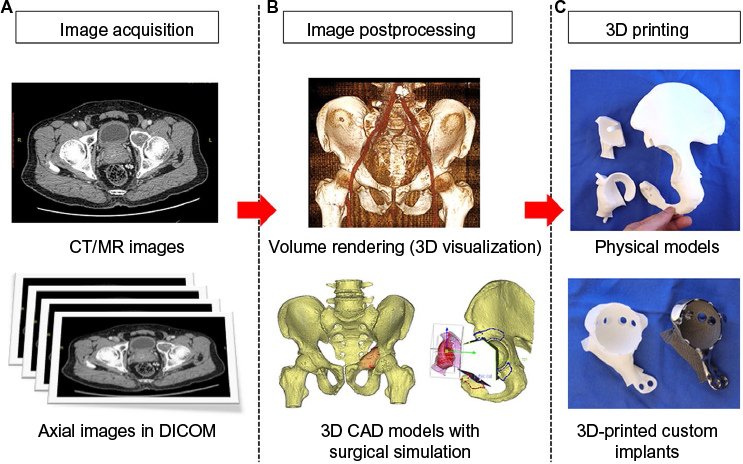 | Figure 3 Summary of the steps in patient-specific orthopedics in a patient with low-grade chondrosarcoma involving the anterior acetabulum of pelvis and a partial acetabular tumor resection and reconstruction with a 3D-printed custom implant was planned. Notes: The steps consist of image acquisition (A), image postprocessing (B), and 3D printing (C). Abbreviations: DICOM, digital imaging and communications in medicine; CAD, computer-aided design; CT, computer tomography; MR, magnetic resonance; 3D, three-dimensional. |
3D printing
CAD software analyzes the STL file that represents the 3D model to be fabricated and “slices” the model into a series of cross-sectional layers. A 3D printing machine then fabricates the 3D physical model by adding successive layers of material to recreate the virtual cross sections. The 3D printing technology used in medicine can be classified according to the technique of manufacturing. It mainly includes stereolithography apparatus (SLA), fused deposition modeling (FDM), selective laser sintering (SLS), or electron beam melting (EBM).14,15 The liquid-based 3D printing technology of SLA makes successive layers by using photosensitive resin that is cured by an ultraviolet laser. The solid-based 3D printing technology of FDM works by the extrusion of small beads of melted thermoplastic materials, from a small nozzle, that harden afterward to form layers. The powder-based 3D printing technology of SLS or EBM involves the use of a focused laser or electron beam to selectively fuse small particles of plastic or metal on the surface of a powder bed. The focused energy scans each layer according to the cross section generated from the STL file of the fabricated 3D object. The powder bed is reduced by one layer thickness after scanning of each cross section. A new layer of material is then applied on top, and the process is repeated until the fabrication is completed. In contrast with other 3D printing technology such as SLA and FDM, which requires special supporting structures to fabricate overhanging designs, SLS or EBM does not require supporters because the model being constructed is surrounded by unsintered powder at all times. This allows fabrication of objects with previously impossible complex geometries.
Applications of 3D printing in patient-specific orthopedics
In the last decades, 3D printing has undergone tremendous development and now has important applications in various fields of medicine. However, reports on orthopedic applications are limited and mainly consist of case reports or small series. They include anatomic models for surgical planning, education and training, PSI for assisting surgical procedures, and fabrication of complex custom metal implants.
Anatomic models for surgical planning
In traditional preoperative planning, orthopedic surgeons utilized 2D plain X-ray and CT images to assess the bony anatomy and pathology of the patient. As more advanced image postprocessing software can generate 3D nonaxial reformatted images and 3D images, patient-specific treatment choice(s) can be selected by studying all the digital images. Despite these advances in image processing technology, the 3D anatomy is still being viewed as a flat, 3D image. Patient-specific physical bone models can be recreated from patients’ CT image data by 3D printing. The models not only allow surgeons to have tactile and visual understanding of the patient-specific anatomy and pathology, but also anticipate the operative challenges that will aid in the planning of orthopedic procedures.
3D physical models have been reported to be helpful in surgical treatment of complex acetabular27–29 and clavicle fractures.30 The models aided in better understanding of acetabular fractures and significantly reduced the degree of interobserver variation in the classification of these fractures.31 The metal plates could also be placed to the fracture bone model and bent to match the reduced bone fracture surface prior to the actual surgery.28,30 The precontoured plates could then be used to assess and assist in fracture reduction, and these have even facilitated minimally invasive plating in comminuted clavicle fractures.30 In a prospective observational study of the surgeons’ perceptions of 3D printed models to assist with complex surgical cases in pediatric spine and pelvis with anomalies, significant benefits were rated in designing a surgical plan, selecting implant type or external fixator, intraoperative reference of patients’ anatomy, precision of osteotomies, and communication with patients.32 The operative time may even be reduced in cases of congenital spinal deformity due to improvement in 3D understanding of the condition and surgical planning.32 In the author’s experience, patient-specific 3D-printed models can also be sterilized so that the surgeon can manipulate the model on the operative field while performing the procedure. It may help confirm surgical anatomy and guide resection in bone tumor surgery (Figure 4A).
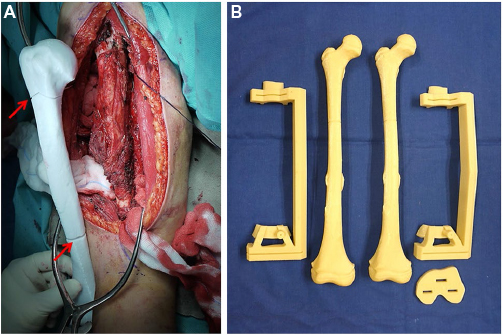 | Figure 4 (A) This image shows surgical exposure in a patient with humeral shaft bone sarcoma undergoing intercalary tumor resection. The 3D-printed PSM with planned resections (red arrows) could be used for easy intraoperative reference of the surgical plan. 3D-printed PSIs and bone models (B) were fabricated preoperatively for a joint-saving tumor resection in a 9-year-old patient with femur osteosarcoma. Abbreviations: 3D, three-dimensional; PSM, patient-specific model; PSI, patient-specific instrument. |
Education and surgical training
Patient-specific 3D-printed models can be used for education and preoperative discussions about surgical strategies and options among care providers across different disciplines. The use of the models has been reported in various pediatric orthopedic disorders, such as Perthe’s disease, Blount disease, physeal bars, or coalitions.33 These models could assist surgeons, therapists, and patients to understand better the patients’ musculoskeletal pathology. Patient-specific fracture models have also been used to improve the consent process in patients with complex acetabular fractures. It may increase the patient satisfaction as patients and their families can now easily understand their medical conditions with real physical models.29 Postoperatively, these physical models and their electronic CAD files could be kept to build a library of various types of fracture so that the models can be 3D-printed again when necessary. Such a collection of fracture models are useful educational tools for surgeons, other physicians, and medical students.29
Although the use of 3D-printed models has not been reported in surgical training in orthopedics, the potential benefits are obvious. Majority of the surgeons just train in the operating theater. This may place patients at risk when surgeons are trying to master certain surgical skills at the initial learning curve. With tangible solid models, senior surgeons can convey their surgical experience to residents much more easily. In addition, as complex or rare cases such as deformity correction, fracture fixation, or bone tumor resection may not be normally seen during resident training, 3D-printed models of the cases can provide residents or junior surgeons unique opportunities for authentic simulation-based surgical training. Besides enhancing surgeons’ understanding of the orthopedic conditions, surgical practice on prototypes created by 3D printing enables surgeons to be more familiar with the patient-specific scenarios before they actually perform similar procedures in real clinical setting. It may improve patients’ safety.
Patient-specific instruments
PSI is customized on the basis of the 3D surface model of bony anatomy, which is generated by image segmentation of a patient’s imaging data. The design is then fabricated by 3D printing technology for orthopedic applications (Figure 4B). This customized tool is used with an intention of easily replicating surgical plans that involve guiding a saw and/or drill in a specific planned direction. PSI has been reported in pedicle screw insertion for spinal surgery in the cervical4 or thoracic region,3 for performing difficult osteotomies in deformity correction of fracture malunion,6,10 and for guiding accurate implant placement in total knee and hip arthroplasty.5,7,9 The use of PSI has also recently been described in bone tumor surgery. It might help improve the bone resection accuracy for oncological clearance11 and the matching of a customized tumor implant to the bone defect after tumor resection.8,23
In contrast to computer navigation-assisted techniques that require bulky navigation facilities and a machine operator, PSI technique has the theoretical benefit of improving surgical accuracy by using simple personalized instruments with minimal operative setup and without distraction from the surgical field. However, two recent meta-analyses did not support the routine use of PSI in total knee arthroplasty as it was not shown to provide superior accuracy to using conventional manual instrumentation.31,34 One of the limitations in PSI technique is incorrect placement of a PSI on the bone surface determined during PSI design per the CAD software. The accurate fit between a PSI and its predetermined bone surface requires that the chosen bone contact surface or footprint should have sufficient registration features for stable positioning of PSI. A footprint with more contoured bone surface may improve the fit. In addition, accurate bone segmentation from the preoperative image data set (CT or MRI) is important to depict the real bony anatomy for PSI design. In patients with osteoarthritis undergoing PSI-assisted joint arthroplasty, the depiction of osteophytes in CT images can be unreliable and can possibly result in errors in determining PSI footprint, which should exactly match the bone surface with osteophytes.35 Unlike the navigation-assisted technique, the PSI technique does not have the intraoperative visual feedback of preoperative images that can reveal errors.36,37 Inaccurate placement of a PSI and the subsequent incorrect guided procedure may be undetected intraoperatively and may result in deviation error from the planned procedures. Currently, accurate intraoperative PSI placement relies mainly on the subjective feeling of the fit by surgeons. Studies are needed to investigate how much footprint at the bone contact is sufficient for consistent positioning of a PSI.8 In addition, possible intraoperative methods to quantitatively verify the correct positioning of the PSI should be determined as they might help minimize registration errors of the PSI.35
3D-printed custom implants
Off-the-shelf, standard-sized bone implants are mainly fabricated using traditional subtractive manufacturing method. They are readily available to meet the surgical requirement for most patients. In contrast to an off-the-shelf implant in that the patient’s anatomy may need to be modified for a proper fit, a custom implant is a perfect match for the unique anatomy of that patient as it is based on the patient’s own medical images. Custom implants may be indicated when 1) patients’ bony geometries fall outside the range of standard implants with respect to implant size- or disease-specific requirements, and 2) improved surgical results are anticipated due to a better fit between implants and patients’ anatomical needs.14
Potential advantages and limitations of 3D-printed custom implants
The nature of additive layer manufacturing in 3D printing allows fabrication of custom implants with any complex shape or geometric feature; this is impossible using traditional subtractive manufacturing techniques. In addition to the advantage of being anatomically conformed to an individual patient, a 3D-printed implant can be generated with a complex free-form surface such as scaffold lattice in a metal monoblock (Figure 5). This interconnected pore surface structure has the potential to facilitate osteointegration and therefore the possibility to reduce the stiffness mismatch at bone–implant junctions.38,39 The stress-shielding problem may be further minimized as the porosity and pore size in the implants can be modified40 and the elastic modulus of porous titanium can be tailored to be comparable to that of the patient’s bone with the use of modern 3D printing techniques.41 Therefore, the modern design of a 3D-printed custom implant not only has the structural geometry that can match the surgical requirements of an individual patient, but also allows biomechanical evaluation under patient-specific loading conditions for design modification prior to the actual implant fabrication.23,42
 | Figure 5 (A) and (B) The figures show a 3D-printed custom implant for acetabular reconstruction in the patient with low-grade chondrosarcoma. The implant has a solid plate, flanges, and an acetabular cup with screw holes for fixation. The scaffold lattice (C) contains an interconnected network of pores with an average porosity of 70%. Notes: The pores have an average size of 720 µm and the thickness of the solid struts is about 350 µm. The porous construct can facilitate the bone ingrowth at the bone–implant interface for better implant longevity. In addition, it is highly resistant to mechanical compression, while its elastic modulus is similar to that of bone to minimize the stress-shielding problem around the implant. Abbreviation: 3D, three-dimensional. |
The use of 3D-printed custom implants has recently been reported in difficult revision hip arthroplasty with severe acetabular bone loss.12 Sixteen patients with large acetabular defects underwent revision hip arthroplasty using 3D-printed custom trabecular titanium implants. The implants were designed from a detailed analysis of patients’ CT images with special reference to the bone quality and the bone geometry of deficient acetabulum. The implant consisted of a porous augment and cage that recreated the artificial acetabulum. Flanges were added to the design for optimum screw fixation to the remaining pelvic bone. Patient-specific aids and instruments such as 3D-printed physical models of the hemipelvis, trial implants, and drill guides were provided for preoperative rehearsal and intraoperative reference and guidance. However, difficulty was reported in placing the custom implants accurately as planned in 7 out of 16 implants, which were found to be malpositioned in one or more parameters of measurement. This was the only study that addressed the accuracy of placement of custom acetabular implants by comparing the preoperative CT planning with CT data on the postoperative position. Further follow-up is needed to evaluate the clinical outcome of this new 3D-printed custom implant.
Bone tumor resection creates a bone defect that needs reconstruction to restore skeletal stability and function. 3D-printed tumor implants may be the ideal reconstructive solutions as they can be customized to match various shapes of the bone defects after tumor resection. Early reports have suggested that the custom implants were useful for reconstruction in clavicular, scapular, or pelvic bone tumors, which have unique bony geometry and no available off-the-shelf prosthesis.13,23 In addition, prefabricated custom implants and 3D models allowed surgeons to evaluate and better understand the surgical procedures prior to the actual surgery. To achieve a good fit of the custom implants, surgeons may require guiding tools such as PSI23 or computer navigation43 to replicate the same resection planes as planned per the design software. This patient-specific tumor implants may gain more attention and popularity in bone tumor surgery when the digital and manufacturing technology further advances.
A custom patient-specific knee implant (ConforMIS, Bedford, MA, USA) is commercially available for knee arthroplasty in patients with osteoarthritis. On the basis of the patient’s CT images, the implant is customized to match to each patient’s knee with unique shape and contour, thus optimizing bone preservation. A disposable set of personalized instrumentation is also provided with each implant to replicate the planned bone cuts. It may reduce implant inventory for the hospital when compared with the traditional off-the-shelf knee implants. However, it remains to be seen whether the potential benefit of this patient-specific implants can actually translate into a better clinical outcome.
Although the potential clinical performance of 3D printed custom implants can be outstanding owing to their ability to address reconstructive challenges that are beyond the scope of off-the-shelf implants, limitations of this emerging technology should be noted. The concerns include the high cost of the implants, the lead time required in designing and manufacturing to meet the surgical deadlines, the lack of intraoperative flexibility, and the difficulty of achieving accurate implant placement.16 The initial cost of custom implants may be higher than off-the-shelf implants. However, 3D printing can generate custom implants with structural geometry that would be impossible using traditional subtractive technique irrespective of costs. Therefore, it is better to evaluate with reference to the total procedural costs from the preoperative planning, the implant design and manufacturing, the implementation of surgical procedures, and the long-term clinical outcomes. The potential excellent long-term performance of the custom implants may reduce the costly revision surgeries due to implant-related failures and result in lower overall lifetime costs.16 With the advances in computer design software and 3D printing technology, biomedical engineers and implant manufacturers can integrate the whole planning process from 3D image data processing to complex custom implant fabrication via the close collaboration with surgeons. Therefore, the turnaround time of the implant fabrication may be further reduced and the 3D-printed custom implants can be a suitable adjunct for most patients in the future. In addition, post 3D printing steps, such as surface finishing and cleaning of metal powders in scaffold lattice, are essential to provide suitable and flawless 3D-printed objects to surgeons. Sterilization of physical models with materials not resistant to high temperature may raise a critical issue for intraoperative use. Implant-related infection may be a concern as the lattice structure may increase the hospitable surface for microbial adherence that is difficult to eradicate. Finally, some regulatory considerations in the design and manufacturing of 3D-printed custom implants remain challenging for hospitals as there are currently limited regulatory standards that monitor the safety of these 3D-printed custom products.26 Overall, although the clinical data to support the routine use of the 3D-printed custom implants are currently limited, the integration of advanced 3D design and 3D printing technology with PSI or computer navigation-assisted implant placement is very promising as it may further enhance the performance of custom implants in patient-specific orthopedics.
Directions for potential future developments
A few years ago, only plastics could be 3D-printed into anatomic models and PSIs. Then, metal powders, such as titanium or cobalt-chrome, were used to fabricate custom implants by 3D printing. The advances in biomimetic materials for 3D printing will be one major direction for future development in 3D printing technology in patient-specific orthopedics. The material should be biocompatible and sterilizable for intraoperative use. 3D-printed artificial bone should consist of materials with mechanical properties similar to the native bone, which might help restore bony anatomical structures and biomechanical function. One example is polyether ether ketone (PEEK), which has been used as an effective biomaterial for implantable medical devices. This high-performance thermoplastic can now be 3D printed to make durable, lightweight, and geometrically complex objects. Besides offering exceptional strength along with superior heat and chemical resistance, PEEK has a modulus of elasticity closer to that of cortical bone, which might help minimize stress-shielding effects in orthopedic implants.44,45 PEEK has been used as reconstructive cages in cervical spine surgery.46 It is yet to be demonstrated if 3D-printed PEEK artificial bones or implants are beneficial in patient-specific orthopedics.
Drug delivery is the method of administering a pharmaceutical compound to achieve a therapeutic effect in cells and humans. 3D printing technology has been successfully incorporated into drug delivery systems to fabricate 3D scaffolds with biomolecules or pharmaceutical compounds.47 The combination of 3D printing technology and drug delivery systems has been suggested for surgery in tuberculous spinal infection. Poly-DL-lactide and nanohydroxyapatite, two promising drug delivery systems and materials for bone repair, were mixed with antituberculosis drugs to fabricate a 3D porous scaffold via 3D printing technology.48 The construct may provide sufficient mechanical properties for spinal stabilization, encourage bone growth, and function as drug delivery platforms for treating tuberculosis.
The current workflow from clinical imaging to 3D printing of physical models requires multiple separate software that are designed for use mainly by biomedical engineers. Surgeons might not easily master the steps in the working process such as image postprocessing, creating 3D images that highlight of regions of interest, planning the surgery with various reconstructive options, and even preoperative biomechanical evaluation of the implant design or a reconstructive method. To increase the popularity of 3D printing technology among orthopedic surgeons, an integrated all-in-one computer platform should be developed to allow for easy planning and seamless communication among different care providers like radiologists, orthopedic surgeons, engineers, and implant companies. All the digital orthopedic data can be integrated to facilitate customized patient treatments. Surgeons may then choose which 3D-printed products are most appropriate for their patients.
Conclusion
The advent of image processing and 3D printing technology is opening up many opportunities in patient-specific applications in orthopedics. The modern high-resolution medical imaging data can further be processed to create 3D images that are essential for 3D printing of physical objects. The 3D printing technology has been reported to be beneficial in patient-specific orthopedics, such as for the creation of anatomic models for surgical planning, education and surgical training, PSIs, and 3D-printed custom implants. Besides being anatomically conformed to a patient’s surgical requirement, 3D-printed implants can be fabricated with scaffold lattices that may facilitate osteointegration and reduce implant stiffness. Early results in revision hip arthroplasty and bone tumor surgery have been promising. However, limitations including high cost of the implants, the lead time in manufacturing, and lack of intraoperative flexibility need to be addressed. Materials like PEEK, which are biocompatible and have superior strength and heat resistance, have been investigated for use in 3D printing. In addition, 3D printing has been incorporated into drug delivery systems that may restore bony anatomy and deliver therapeutic compound to the target tissue. To increase utilization of 3D printing technology in orthopedics, an all-in-one computer platform should be developed for easy planning and seamless communication among different care providers. Further objective investigation into the clinical efficacy of the technology is needed before one can put the technology into routine clinical practice in orthopedics.
Disclosure
The Materialise, Mobelife company did not fund or sponsor this research in any way. The author reports no conflicts of interest in this work.
References
Schubert C, Van Langeveld MC, Donoso LA. Innovations in 3D printing: a 3D overview from optics to organs. Br J Ophthalmol. 2014;98:159–161. | ||
Martelli N, Serrano C, van den Brink H, et al. Advantages and disadvantages of 3-dimensional printing in surgery: a systematic review. Surgery. 2016;159(6):1485–1500. | ||
Mac-Thiong JM, Labelle H, Rooze M, Feipel V, Aubin CE. Evaluation of a transpedicular drill guide for pedicle screw placement in the thoracic spine. Eur Spine J. 2003;12:542–547. | ||
Lu S, Xu YQ, Lu WW, et al. A novel patient-specific navigational template for cervical pedicle screw placement. Spine. 2009; 34(26):E959–E966. | ||
Hananouchi T, Saito M, Koyama T, Sugano N, Yoshikawa H. Tailor-based surgical guide reduces incidence of outliers of cup placement. Clin Orthop Relat Res. 2010;468:1088–1095. | ||
Miyake J, Murase T, Moritomo H, Sugamoto K, Yoshikawa H. Distal radius osteotomy with volar locking plates based on computer simulation. Clin Orthop Relat Res. 2011;469(6):1766–1773. | ||
Ng VY, DeClaire JH, Berend KR, Gulick BC, Lombardi AV Jr. Improved accuracy of alignment with patient-specific positioning guides compared with manual instrumentation in TKA. Clin Orthop Relat Res. 2012; 470(1):99–107. | ||
Wong KC, Kumta SM, Sze KY, Wong CM. Use of a patient-specific CAD/CAM surgical jig in extremity bone tumor resection and custom prosthetic reconstruction. Comput Aided Surg. 2012;17(6):284–293. | ||
Buller L, Smith T, Bryan J, Klika A, Barsoum W, Innotti JP. The use of patient-specific instrumentation improves the accuracy of acetabular component placement. J Arthroplasty. 2013;28:631–636. | ||
Takeyasu Y, Oka K, Miyake J, Kataoka T, Moritomo H, Murase T. Preoperative, computer simulation-based, three-dimensional corrective osteotomy for cubitus varus deformity with use of a custom-designed surgical device. J Bone Joint Surg Am. 2013 20;95(22):e173. | ||
Gouin F, Paul L, Odri GA, Cartiaux O. Computer-assisted planning and patient-specific instruments for bone tumor resection within the pelvis: a series of 11 patients. Sarcoma. 2014;Article ID 842709:9. | ||
Baauw M, van Hellemondt GG, van Hooff ML, Spruit M. The accuracy of positioning of a custom-made implant within a large acetabular defect at revision arthroplasty of the hip. Bone Joint J. 2015;97-B(6):780–785. | ||
Fan H, Fu J, Li X, et al. Implantation of customized 3-D printed titanium prosthesis in limb salvage surgery: a case series and review of the literature. World J Surg Oncol. 2015;13:308. | ||
Rengier F, Mehndiratta A, von Tengg-Kobligk H, et al. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg. 2010;5:335–341. | ||
Kim GB, Lee S, Kim H, et al. Three-dimensional printing: basic principles and applications in medicine and radiology. Korean J Radiol. 2016;17(2):182–197. | ||
Unwin PS, Eshraghi A. Custom implants. In: Ritacco LE, Milano FE, Chao E, editors. Computer-Assisted Musculoskeletal Surgery: Thinking and Executing in 3D. Switzerland: Springer; 2016;181–198. | ||
Kent DM, Hayward RA. Limitations of applying summary results of clinical trials to individual patients: the need for risk stratification. JAMA. 2007;298:1209–1212. | ||
Neal ML, Kerckhoffs R. Current progress in patient-specific modeling. Brief Bioinform. 2010; 11(1):111–126. | ||
Lepisto J, Armand M, Armiger RS. Periacetabular osteotomy in adult hip dysplasia – developing a computer aided real-time biomechanical guiding system (BGS). Suom Ortoped Traumatol. 2008;31:186–190. | ||
Armiger RS, Armand M, Tallroth K, Lepisto J, Mears SC. Three-dimensional mechanical evaluation of joint contact pressure in 12 periacetabular osteotomy patients with 10-year follow-up. Acta Orthop. 2009;80:155–161. | ||
Lafon Y, Lafage V, Dubousset J, Skalli W. Intraoperative three-dimensional correction during rod rotation technique. Spine. 2009;34:512–519. | ||
Wang X, Aubin CE, Labelle H, Crandall D. Biomechanical modelling of a direct vertebral translation instrumentation system: preliminary results. Stud Health Technol Inform. 2008;140:128–132. | ||
Wong KC, Kumta SM, Geel NV, Demol J. One-step reconstruction with a 3D-printed, biomechanically evaluated custom implant after complex pelvic tumor resection. Comput Aided Surg. 2015;20(1):14–23. | ||
Dalrymple NC, Prasad SR, Freckleton MW, Chintapalli KN. Informatics in radiology (info-RAD): introduction to the language of three-dimensional imaging with multidetector CT. Radio-Graphics. 2005;25:1409–1428. | ||
Wong KC, Kumta SM, Antonio GE, Tse LF. Image fusion for computer-assisted bone tumor surgery. Clin Orthop Relat Res. 2008;466(10):2533–2541. | ||
Trace AP, Ortiz D, Deal A, et al. Radiology’s emerging role in 3-D printing applications in health care. J Am Coll Radiol. 2016;13(7):856–862. | ||
Brown GA, Milner B, Firoozbakhsh K. Application of computer-generated stereolithography and interpositioning template in acetabular fractures: a report of eight cases. J Orthop Trauma. 2002;16(5): 347–352. | ||
Hurson C, Tansey A, O’Donnchadha B, Nicholson P, Rice J, McElwain J. Rapid prototyping in the assessment, classification and preoperative planning of acetabular fractures. Injury. 2007;38(10):1158–1162. | ||
Niikura T, Sugimoto M, Lee SY, et al. Tactile surgical navigation system for complex acetabular fracture surgery. Orthopaedics. 2014;37:237. | ||
Kim HN, Liu XN, Noh KC. Use of a real-size 3D-printed model as a preoperative and intraoperative tool for minimally invasive plating of comminuted midshaft clavicle fractures. J Orthop Surg Res. 2015;10:91. | ||
Voleti PB, Hamula MJ, Baldwin KD, Lee GC. Current data do not support routine use of patient-specific instrumentation in total knee arthroplasty. J Arthroplasty. 2014;29(9):1709–1712. | ||
Guarino J, Tennyson S, McCain G, Bond L, Shea K, King H. Rapid prototyping technology for surgeries of the pediatric spine and pelvis: benefits analysis. J Pediatr Orthop. 2007;27(8):955–960. | ||
Starosolski ZA, Kan JH, Rosenfeld SD, Krishnamurthy R, Annapragada A. Application of 3-D printing (rapid prototyping) for creating physical models of pediatric orthopedic disorders. Pediatr Radiol. 2014;44:216. | ||
Cavaignac E, Pailhé R, Laumond G, et al. Evaluation of the accuracy of patient-specific cutting blocks for total knee arthroplasty: a meta-analysis. Int Orthop. 2015;39(8):1541–1552. | ||
Kunz M, Balaketheeswaran S, Ellis RE, Rudan JF. The influence of osteophyte depiction in CT for patient-specific guided hip resurfacing procedures. Int J Comput Assist Radiol Surg. 2015;10(6):717–726. | ||
Leeuwen JA, Grøgaard B, Nordsletten L, Röhrl SM. Comparison of planned and achieved implant position in total knee arthroplasty with patient-specific positioning guides. Acta Orthop. 2014;11:1–6. | ||
Wong KC, Sze KY, Wong IO, Wong CM, Kumta SM. Patient-specific instrument can achieve same accuracy with less resection time than navigation assistance in periacetabular pelvic tumor surgery: a cadaveric study. Int J Comput Assist Radiol Surg. 2016;11(2):307–316. | ||
Ryan G, Pandit A, Apatsidis DP. Fabrication methods of porous metals for use in orthopaedic applications. Biomaterials. 2006;27:2651–2670. | ||
Lopez-Heredia MA, Goyenvalle E, Aguado E, et al. Bone growth in rapid prototyped porous titanium implants. J Biomed Mater Res A. 2008;85(3):664–673. | ||
Harrysson OLA, Cansizoglu O, Marcellin-Little DJ, Cormier DR, West HA II. Direct metal fabrication of titanium implants with tailored materials and mechanical properties using electron beam melting technology. Mater Sci Eng C. 2008;28:366–373. | ||
Hein P, Müller L, Körner C, Singer RF, Müller FA. Cellular Ti–6Al–4V structures with interconnected macro porosity for bone implants fabricated by selective electron beam melting, Acta Biomater. 2008;4:1536–1544. | ||
Harrysson O, Hosni Y, Nayfeh J. Custom-designed orthopedic implants evaluated using finite element analysis of patient-specific computed tomography data: femoral component case study. BMC Musculoskelet Disord. 2007;8:91. | ||
Wong KC, Kumta SM, Chiu KH, et al. Computer assisted pelvic tumor resection and reconstruction with a custom-made prosthesis using an innovative adaptation and its validation. Comput Aided Surg. 2007;12(4):225–232. | ||
Kostecki K. PEEK usage climbs for devices. Med Des. 2011. Available from: http://medicaldesign.com/materials/peek-usage-climbs-devices. Accessed on September 4, 2016. | ||
Li CS, Vannabouathong C, Sprague S, Bhandari M. The use of carbon-fiber-reinforced (CFR) PEEK material in orthopedic implants: a systematic review. Clin Med Insights Arthritis Musculoskelet Disord. 2015;8:33–45. | ||
Kersten RF, van Gaalen SM, de Gast A, Öner FC. Polyetheretherketone (PEEK) cages in cervical applications: a systematic review. Spine J. 2015;15(6):1446–1460. | ||
Lee JW, Cho DW. 3D Printing technology over a drug delivery for tissue engineering. Curr Pharm Des. 2015;21(12):1606–1617. | ||
Dong J, Zhang S, Liu H, Li X, Liu Y, Du Y. Novel alternative therapy for spinal tuberculosis during surgery: reconstructing with anti-tuberculosis bioactivity implants. Expert Opin Drug Deliv. 2014;11:299. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.