Back to Journals » Clinical Ophthalmology » Volume 16
24-Month Outcomes of Ahmed ClearPath® Glaucoma Drainage Device for Refractory Glaucoma
Authors Dorairaj S, Checo LA ![]() , Wagner IV
, Wagner IV ![]() , Ten Hulzen RD
, Ten Hulzen RD ![]() , Ahuja AS
, Ahuja AS ![]()
Received 30 March 2022
Accepted for publication 6 July 2022
Published 13 July 2022 Volume 2022:16 Pages 2255—2262
DOI https://doi.org/10.2147/OPTH.S368634
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Syril Dorairaj,1 Leticia A Checo,1 Isabella V Wagner,1 Richard D Ten Hulzen,1 Abhimanyu S Ahuja2
1Department of Ophthalmology, Mayo Clinic, Jacksonville, FL, USA; 2Charles E. Schmidt College of Medicine, Florida Atlantic University, Boca Raton, FL, USA
Correspondence: Syril Dorairaj, Department of Ophthalmology, Mayo Clinic, 4500 San Pablo Road, Jacksonville, FL, USA, Tel +1 904-953-2377, Fax +1 904-953-7040, Email [email protected]
Purpose: To describe the safety and efficacy of the Ahmed ClearPath® (ACP) 250 mm2 glaucoma drainage device (GDD) in the treatment of refractory primary open-angle glaucoma (POAG).
Patients and methods: This was a retrospective, noncomparative, single-surgeon, interventional case series of adult patients with medically ± surgically refractory POAG undergoing ACP implantation. Intraocular pressure (IOP), the number of glaucoma medications, and complications were recorded over 24 months of follow-up. Primary outcomes included mean reductions in both IOP and medication use through 24 months, and secondary outcomes included the proportion of eyes achieving an IOP between 6 and 19 mmHg, IOP reduction by ≥ 20%, and reduction by ≥ 1 medication at last mean follow-up.
Results: Twelve eyes of 11 patients (mean age 71.3 ± 14.1 years) fit inclusion criteria and were enrolled. Most patients were Caucasian (n = 8), female (n = 10), and all had severe POAG (n = 11). The mean last follow-up was 18 months, at which time the mean (standard deviation) baseline IOP of 29.0 (7.6) mmHg was reduced to 12.2 (4.0) mmHg (58% reduction). 91.7% of eyes achieved an IOP between 6 and 19 mmHg, and 100% of eyes met an IOP reduction of ≥ 20%. Mean baseline number of glaucoma medications was 3.0 (0.9) and was reduced to 0.5 (0.7) at last mean follow-up (83.3% reduction), with 91.7% of eyes using ≥ 1 fewer medications. No long-term complications were observed, and short-term complications (mild hyphema, inflammation, and pain) were resolved by month 3.
Conclusion: To our knowledge, this is the second long-term study evaluating the efficacy of the Ahmed ClearPath drainage device in adult patients, and the first study with 24-months follow-up. The ACP device is safe and effective at reducing both IOP and medication burdens in patients with severe POAG. Additionally, minimal short-term complications were noted with no long-term adverse effects, increasing comfort for both the surgeon and the patient.
Keywords: primary open angle glaucoma, intraocular pressure, IOP-lowering medications, valved drainage devices
Introduction
Eyes with glaucoma refractory to medical therapy, and particularly refractory to prior glaucoma surgery, pose a challenge for glaucoma surgeons. The options for next-step procedures for these eyes include trabeculectomy (or repeat trabeculectomy), glaucoma drainage device (GDD) implantation, or a host of novel glaucoma procedures. Data from the medical literature to guide decision-making for these patients are available for trabeculectomy versus GDD procedures1,2 and for valved versus valveless GDDs,3,4 but little data are available about the relative benefits of the new procedures in the absence of head-to-head trials.5–8 In some cases, the glaucoma surgical landscape is evolving so quickly that surgical options become available before any outcome data have emerged.
The Ahmed ClearPath (ACP; New World Medical) is a novel valveless GDD cleared by the US Food and Drug Administration in 2019. It was designed in collaboration with glaucoma surgeons and features several design elements intended to improve the ease and safety of implantation.9 ACP is available in 350 mm2 or 250 mm2 sizes, both of which are designed to limit muscle manipulation. The 350 mm2 model contains a winged design and a posteriorly positioned plate to avoid rectus muscle insertions, while the 250 mm2 model is designed to fit between muscles and eliminates the need for muscle isolation.7 The device is packaged with a prethreaded 4–0 polypropylene rip cord and 23-gauge needle to facilitate creation of a sclerostomy and minimize the risk of early hypotony associated with other GDD procedures.7 In contrast to the widely used nonvalved Baerveldt implants and valved Ahmed implants, ACP includes a lower-lying plate with more anteriorly positioned scleral fixation points, limiting further posterior dissection and increasing the ease of access for implantation.7 Despite being available for more than 3 years, there is only a single outcome study available in the PubMed-indexed literature (as of this writing) that is limited to short-term six-month follow-up.
Herein, we report our early experience with the ACP through up to 24 months of follow-up.
Methods
This was a retrospective, noncomparative, single-surgeon (SD), interventional case series. The study protocol was reviewed and approved by the Mayo Clinic Institutional Review Board (IRB) in 2021 (certificate approval number: 08/16/2021). The study was conducted in accordance with the tenets of the Declaration of Helsinki.10
Patients were eligible to participate if they were adults aged 18 years or older with POAG that was uncontrolled with medical therapy with or without prior glaucoma surgery and were scheduled to undergo elective implantation of the 250 mm2 ACP between January 1, 2019 and December 31, 2020. Eligible eyes had mobile conjunctiva within the quadrant suitable for ACP implantation and a best corrected visual acuity of hand motions or better. Patients with secondary forms of open-angle glaucoma (pseudoexfoliative, pigmentary, steroid-induced, uveitic, and traumatic glaucoma) were excluded. Patients with other glaucoma diagnoses (angle closure glaucoma, normal tension glaucoma) and those deemed unlikely to attend all follow-up visits were additionally excluded. All consecutive eligible patients were enrolled.
In all cases, the ACP implantation procedure was performed as described in the manufacturer’s directions for use.11 The use of ligation, fenestration, and the 4–0 polypropylene ripcord occurred in all eyes. In each case, the ACP implant was ligated with 8–0 Vicryl near the plate and sutured to the episclera with 8–0 nylon sutures 8 millimeters posterior to the surgical limbus. The drainage tube was trimmed 2 to 3 mm and bevel cut to an anterior chamber angle of 30 degrees to permit insertion. A paracentesis was performed, and the anterior chamber was entered <2 mm back from the limbus with a 23-gauge cannula, to which the ACP device was then inserted 2 to 3 mm through the needle track. Three horizontal slits were made in the tube below the 8–0 Vicryl ligature, and the scleral flap was sutured over the silicone tube with 8–0 nylon sutures. The tube was allowed to rest against the sclera in an S configuration, to account for plate movement without affecting the anterior chamber positioning of the tube. The device was then sutured to the sclera with three 9–0 nylon sutures and covered with a Tutoplast graft 5 to 6 millimeters posteriorly. Following this, the conjunctiva was closed at the limbus using a purse string suture and running 8–0 Vicryl suture.
In 2 cases, a pre-existing gel stent (Xen; Allergan, and AbbVie Company) was simultaneously revised by removing Tenon tissue obstructing the distal end of the stent. In all eyes, a postoperative regimen of topical moxifloxacin 0.5% and prednisolone acetate 1% ophthalmic solutions administered 4 times per day was prescribed and tapered down over a 2-month period, depending on patient information. The polypropylene ripcord suture was not removed in any case, due to the absence of tube exposure, vision threatening complications, and choroidal effusions throughout the follow-up period.
Participants were evaluated preoperatively, intraoperatively, and 1 day, 1 week, and 1, 3, 6, 12, 18, and 24 months postoperatively. Intraoperative data included surgical details and complications. Pre- and postoperative data included IOP, medication use, and complications. On post-operative day (POD) 1, IOP was measured using rebound tonometry (iCare ic100; iCare) according to its instructions for use.12 The iCare device was used in favor of Goldmann applanation tonometry (GAT) due to the increased sensitivity of the eye following ACP implantation. GAT was used to measure IOP during all remaining post-operative visits. Visual acuity was assessed using a Snellen eye chart at 20 feet. Slit lamp and fundus examinations were used to visualize the anterior and posterior segments of each eye. Anterior chamber inflammation at each postoperative visit was graded using the Standardization of Uveitis Nomenclature schema.13
Standard descriptive statistics were used to report demographics and baseline characteristics, with means and standard deviations (SD) used for continuous variables, and percentages used for categorical variables. The primary outcome measures of the study were the changes from baseline in both IOP and the number of IOP-lowering medications at each postoperative time point, each assessed using 2-tailed paired t-tests with p < 0.05 as the level of significance. Primary outcomes were reported as means with SD and were calculated from the total of available eyes at each follow-up visit. Sample size was determined by the number of available cases, and no formal power analysis was conducted as no hypotheses were being tested. The data were analyzed using the SPSS program 22.0 (SPSS Inc., Chicago, IL). Secondary outcome measures included the proportion of eyes achieving an IOP between 6 and 19 mmHg, an IOP reduction of ≥20%, and reduction by ≥1 medications at last follow-up. All secondary outcomes were evaluated at the last follow-up of each eye (mean 18 months) using descriptive statistics. ACP implantation was considered successful if IOP was reduced by 20% or remained between 6 and 19 mmHg through at least 6 months of follow-up. Eyes that did not reach the desired IOP criteria or required a surgical reintervention were considered a failure.
Results
Twelve eyes of 11 patients underwent Ahmed ClearPath implantation and were followed for up to 24 months. Demographic and baseline glaucoma status data are described in Table 1. Their mean (SD) age was 71.3 (14.1) years, most were Caucasian (72.7%) and female (90.9%). All eyes had severe POAG as classified by the International Classification of Diseases 10 definition.14 Follow-up was incomplete due to the COVID-19 pandemic.
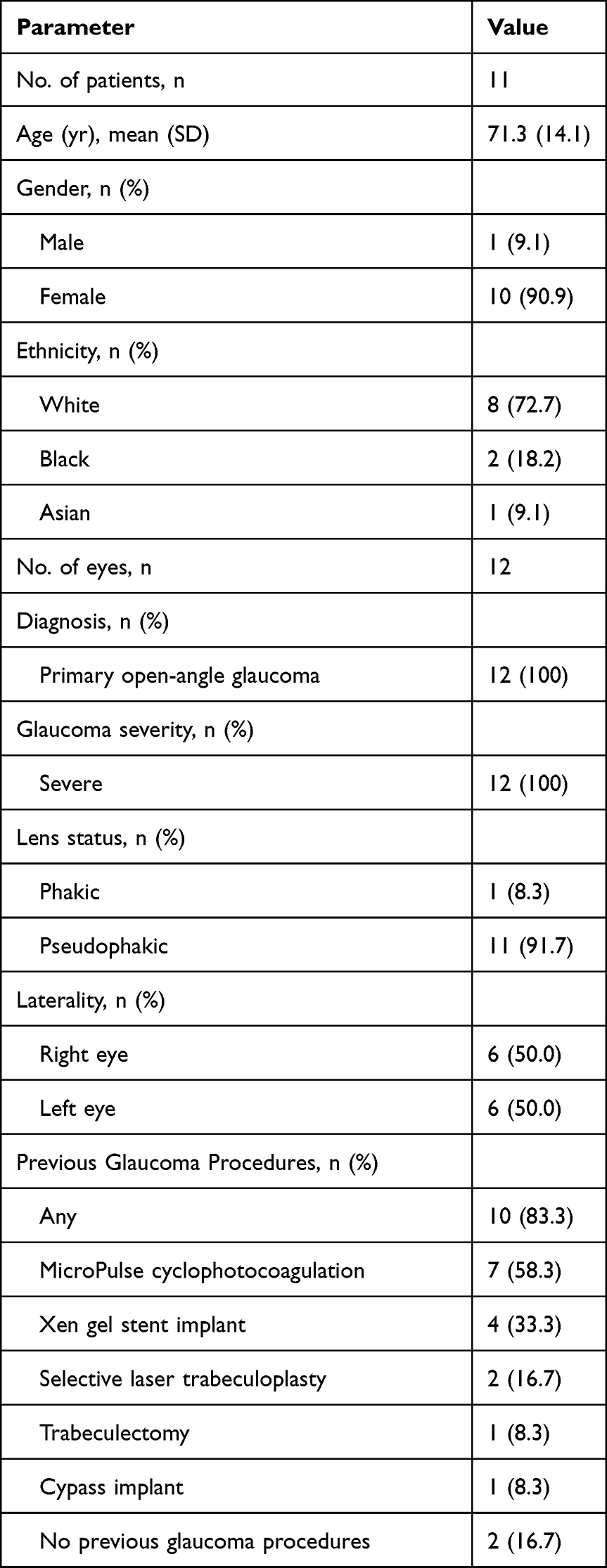 |
Table 1 Demographic and Baseline Glaucoma Status of Study Participants |
Mean IOP at baseline and each postoperative visit is given in Table 2. The mean (SD) baseline IOP was 29.0 (7.6) mmHg and through up to 24 months of follow-up ranged from 5.9 (2.6) mmHg to 11.2 (4.7) mmHg (p < 0.05 at every time point versus baseline) with a trend for rising IOP over time (Figure 1). Mean IOP reductions across time points ranged from 58% to 80%. Among the 5 eyes seen at month 24, mean IOP was 11.2 (4.7) mmHg, a 61.4% reduction from baseline. Among all 12 eyes, the mean IOP at the last follow-up (mean 18 months) was 12.2 (4.0) mmHg (a 58% reduction from baseline); 91.7% achieved IOP between 6 and 19 mmHg, and 100% achieved an IOP reduction of ≥20% from baseline at the last follow-up. The success rate was 100%.
 |
Table 2 Mean IOP and Medication Use at Each Study Visit |
 |
Figure 1 Mean IOP over time in the study cohort. Error bars represent standard deviation. Reductions from baseline were significant (p<0.05) at every time point. |
Mean medication use at baseline and each postoperative visit is also given in Table 2. The mean (SD) number of medications was 3.0 (0.9) and through up to 24 months of follow-up ranged from 0.2 (0.6) to 0.9 (0.9) medications (p < 0.05 at every time point versus baseline) with a trend for increased medication use over time (Figure 2). Mean medication reductions across time points ranged from 70% to 92%. Among the 5 eyes seen at month 24, mean medication use was 0.6 (0.5) medications per eye, an 80% reduction from baseline. Among all 12 eyes, the mean medication use at the last follow-up (mean 18 months) was 0.5 (0.7) medications per eye (an 83.3% reduction from baseline), and 91.7% were using ≥1 fewer medications than at baseline. All secondary outcome measures can be found in Table 3.
 |
Table 3 Secondary Outcome Measures at Last Mean Follow-Up (n = 12 Eyes) |
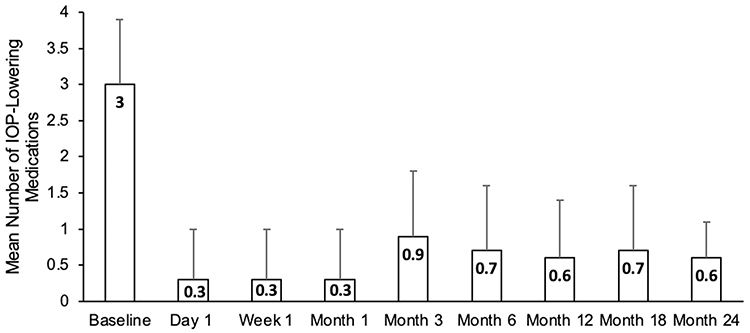 |
Figure 2 Mean medication use over time in the study cohort. Error bars represent standard deviation. Reductions from baseline were significant (p<0.05) at every time point. |
The procedure was performed without intraoperative complications in all eyes. All patients were treated with the ripcord and no removal or suture lysis occurred. The nature and frequency of the postoperative complications are given in Table 4. The most common complication was mild hyphema (33.3%), which failed to persist and was resolved by the 1-month follow-up in all affected eyes. No eyes experienced an IOP rise exceeding 21 mmHg at any postoperative visit. Only 2 eyes manifested in anterior chamber cell and flare (1+ in all cases) that resolved at month 1 and month 3. Bleb encapsulation did not occur during the early post-operative period, and a shallow, diffuse bleb was observed in all eyes at 24 months (Figure 3). No vision threatening complications or surgical reinterventions occurred throughout the entire follow-up period.
 |
Table 4 The Nature and Frequency of Postoperative Complications (n = 12 Eyes) |
 |
Figure 3 A shallow, diffuse bleb was observed in all eyes (n = 12) at the 24-month follow-up visits. |
Discussion
In this analysis of our early experience with the valveless Ahmed ClearPath device, clinically and statistically significant reductions in both IOP and the use of IOP-lowering medications were observed in all eyes through up to 24 months of follow-up. The procedure’s safety profile in this series was similar to that of other valveless GDDs.
In the past decade, numerous clinical trials have clarified the role of GDDs in the surgical management of glaucoma. The Primary Tube Versus Trabeculectomy (PTVT) and Tube Versus Trabeculectomy (TVT) studies evaluated the relative roles of mitomycin-augmented trabeculectomy and (valveless) Baerveldt 350 mm2 GDD in eyes that were and were not surgically naïve, respectively. The PTVT demonstrated better IOP and medication reduction with trabeculectomy versus the GDD at 3 years in surgically naïve eyes,1 while the TVT demonstrated greater 5-year success with the GDD versus trabeculectomy in eyes previously operated for cataract or glaucoma.2 Among GDD designs (valved versus valveless), the pooled analysis of data from the Ahmed Baerveldt Comparison (ABC) and Ahmed Versus Baerveldt (AVB) studies demonstrated better IOP and medication reductions, lower failure rate, and lower rate of subsequent glaucoma surgery with the valveless Baerveldt 350 mm2 GDD compared to the valved Ahmed-PF7 GDD, albeit with higher risk of hypotony, at 5 years postoperatively.3 A meta-analysis comparing the valved Ahmed and valveless Baerveldt GDDs concluded that the Baerveldt implant provided better surgical success rates and medication reduction but comparable IOP reduction and safety when compared to the valved Ahmed GDD.4
The ACP is a novel valveless GDD cleared by the US Food and Drug Administration in 2019. Designed with input from glaucoma surgeons, the ACP features a curved, flexible plate to facilitate positioning and to conform to the shape of the globe. The plate height was reduced to produce low, diffuse blebs and reduce the risk of postoperative conjunctival erosion. The scleral fixation suture points were placed on anteriorly projected wings to make scleral fixation easier. The ACP is available in both 250 mm2 and 350 mm2 models. The smaller model fits between the rectus muscles for single-quadrant implantation, while the larger model has a posteriorly displaced plate to rest behind the rectus muscles and reduce the risk of postoperative diplopia. An optional pre-threaded 4–0 polypropylene rip cord suture is incorporated to minimize postoperative hypotony, and a 23-gauge needle is included to create an appropriately sized sclerotomy to pass through the tube. Among glaucoma surgeons participating in an early experience survey, the ACP reportedly better conformed to the curvature of the globe, was easier to suture to sclera, had shorter operating time, and had greater overall ease of use compared to their experience with Baerveldt GDDs.9
Our results compare favorably to a prior report of ACP efficacy and to outcomes with the valveless Baerveldt GDD. In the only other published report of ACP outcomes of which we are aware to date, mean IOP was reduced from 26.3 mmHg at baseline to 13.7 mmHg (a 43% reduction) and mean medication use was reduced from 3.9 to 1.9 (a 47% reduction) at 6 months.7 In comparison, our 6-month IOP and medication reductions with the ACP were 61.5% and 77.8%, respectively. In the ABC study, mean IOP in eyes receiving the Baerveldt 350 mm2 GDD decreased from 31.8 mmHg at baseline to 13.4 mmHg and 14.2 mmHg at 1 and 2 years, respectively,15 while in the AVB study, mean IOP was reduced from 31.7 mmHg at baseline to 13.6 mmHg and 14.4 mmHg in the Baerveldt group.16 In comparison, our 1- and 2-year mean IOP reductions from a 29.0 mmHg baseline were 7.8 mmHg and 11.2 mmHg, respectively.
Complication rates in our study compare favorably to the valved Ahmed GDD and other valveless GDDs. A five-year pooled data analysis of the ABC and AVB studies reported elevated IOP and severe vision loss as the most common complications resulting in failure, with incidence rates of 42% and 4.9% in the valved Ahmed GDD, and 23% and 7% in the valveless Baerveldt GDD.3 Interestingly, neither complication was observed within our study, and the failure rate was 0%. Our safety profile appears to compare similarly to a 6-month outcome report on ACP efficacy, in which anterior chamber inflammation and hyphema were the most common complications observed, with incidence rates of 16.3% and 15.4%, respectively.7 Unlike all previous GDD studies, hypotony was not observed throughout our follow-up period, likely due to use of the rip cord. No choroidal detachments were observed, which may be attributed to the rapid resolution of all post-operative complications, absence of hypotony, and relatively small sample size of our study. It is worth noting that our sample size is considerably smaller than that of the aforementioned studies, making direct comparison challenging.
The main strength of our study is the inclusion of all consecutive qualifying patients. Further, this study’s results satisfy an unmet need for clinical outcome data with the ACP, as we are aware of only 1 other study in the PubMed-indexed literature, and it was only of 6-months duration. Limitations of our study include its small sample size, compounded by the incomplete follow-up resulting from reluctance to seek health care during the COVID-19 pandemic. The lack of a control group is not considered a limitation as interventional studies of new surgical procedures for refractory glaucoma typically do not have a control group.5–8
Conclusions
In summary, implantation of the valveless Ahmed ClearPath GDD produces significant reductions in IOP and the need for IOP-lowering medications through up to 24 months of follow-up. Advantages of ACP include its ease of use, good safety profile, and high efficacy concerning IOP and medication burden reduction. Disadvantages of ACP include its tendency to cause anterior chamber inflammation and hyphema. This procedure may be a useful therapeutic option in eyes with glaucoma refractory to medical ± surgical treatment.
Data Sharing Statement
The author’s institution does not permit data sharing. Other queries and requests should be directed to the corresponding author (SD).
Consent for Publication
This study was conducted in accordance with the tenets of Declaration of Helsinki. Due to the retrospective nature of the study, patient consent was waived by the Mayo Clinic IRB. All data and images have been deidentified, and no personal identifying information is contained within this report.
Acknowledgments
Manuscript preparation assistance was provided by Tony Realini, MD, MPH (Hypotony Holdings LLC) with support from New World Medical.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gedde SJ, Feuer WJ, Lim KS, et al. Treatment outcomes in the primary tube versus trabeculectomy study after 3 years of follow-up. Ophthalmology. 2020;127:333–345. doi:10.1016/j.ophtha.2019.10.002
2. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153:789–803. doi:10.1016/j.ajo.2011.10.026
3. Christakis PG, Zhang D, Budenz DL, et al. Five-year pooled data analysis of the ahmed baerveldt comparison study and the Ahmed versus baerveldt study. Am J Ophthalmol. 2017;176:118–126. doi:10.1016/j.ajo.2017.01.003
4. Wang S, Gao X, Qian N. The Ahmed shunt versus the Baerveldt shunt for refractory glaucoma: a meta-analysis. BMC Ophthalmol. 2016;16:83. doi:10.1186/s12886-016-0265-6
5. Batlle JF, Fantes F, Riss I, et al. Three-year follow-up of a novel aqueous humor microshunt. J Glaucoma. 2016;25:e58–65. doi:10.1097/IJG.0000000000000368
6. Grover DS, Godfrey DG, Smith O, Feuer WJ. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: technique report and preliminary results. Ophthalmology. 2014;121:855–861. doi:10.1016/j.ophtha.2013.11.001
7. Grover D, Kahook M, Seibold L, et al. Clinical outcomes of Ahmed ClearPath implantation in glaucomatous eyes: a novel valveless glaucoma drainage device. J Glaucoma. 2022;31(5):335–339. doi:10.1097/IJG.0000000000002013
8. Minckler DS, Baerveldt G, Alfaro MR, Francis BA. Clinical results with the Trabectome for treatment of open-angle glaucoma. Ophthalmology. 2005;112:962–967. doi:10.1016/j.ophtha.2004.12.043
9. Chang P. Early surgeon experience with a new valveless glaucoma drainage device.
10. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191–2194.
11. The AHMED ClearPath glaucoma drainage device. Available from: https://www.newworldmedical.com/wp-content/uploads/2020/10/50-0109-ClearPath_IFU-Full-Version.pdf.
12. iCare ic100 instruction manual. Available from: https://www.tpched.org/uploads/1/0/9/8/10988970/icare_ic100_instruction_manual_ta011-047_en-1-0.pdf.
13. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509–516.
14. American Academy of Ophthalmology. ICD-10-CM Quick Reference Guide for Glaucoma. San Francisco: American Academy of Ophthalmology; 2015.
15. Barton K, Feuer WJ, Budenz DL, et al. Three-year treatment outcomes in the Ahmed Baerveldt comparison study. Ophthalmology. 2014;121:1547–57 e1. doi:10.1016/j.ophtha.2014.01.036
16. Christakis PG, Tsai JC, Kalenak JW, et al. The Ahmed versus Baerveldt study: three-year treatment outcomes. Ophthalmology. 2013;120:2232–2240. doi:10.1016/j.ophtha.2013.04.018
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Efficacy of Successful Excisional Goniotomy with the Kahook Dual Blade
Wagner IV, Boopathiraj N, Lentz C, Dorairaj EA, Draper C, Kumar D, Checo L, Miller DD, Krambeer C, Dorairaj S
Clinical Ophthalmology 2024, 18:713-721
Published Date: 7 March 2024