Back to Journals » Drug Design, Development and Therapy » Volume 13
Pharmacokinetic comparison of a fixed-dose combination versus concomitant administration of amlodipine, olmesartan, and rosuvastatin in healthy adult subjects
Authors Oh M, Shin JG, Ahn S ![]() , Kim BH, Kim JY
, Kim BH, Kim JY ![]() , Shin HJ, Shin HJ, Ghim JL
, Shin HJ, Shin HJ, Ghim JL
Received 23 January 2019
Accepted for publication 6 March 2019
Published 3 April 2019 Volume 2019:13 Pages 991—997
DOI https://doi.org/10.2147/DDDT.S202730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Minkyung Oh,1 Jae-Gook Shin,1,2 Sangzin Ahn,1 Bo Hoon Kim,3 Ji Yeon Kim,3 Hyun Ju Shin,4 Hyun Ju Shin,4 Jong-Lyul Ghim1,2
1Department of Pharmacology and PharmacoGenomics Research Center, Inje University College of Medicine, Busan, Republic of Korea; 2Department of Clinical Pharmacology, Inje University Busan Paik Hospital, Busan, Republic of Korea; 3Formulation Research Team, Seoul, Daewoong Pharma, Republic of Korea; 4Clinical Research Team, Daewoong Pharma, Seoul, Republic of Korea
Objective: The aim of this study was to compare the pharmacokinetic (PK) and safety profiles of a fixed dose combination (FDC) formulation and co-administration of amlodipine, olmesartan, and rosuvastatin.
Materials and methods: This study was an open-label, randomized, cross-over design conducted in healthy male volunteers. All subjects received either a single FDC tablet containing amlodipine 10 mg/olmesartan 40 mg/rosuvastatin 20 mg, or were co-administered an FDC tablet containing amlodipine 10 mg/olmesartan 40 mg and a tablet containing rosuvastatin 20 mg, for each period, with 14-day washout periods. Plasma concentrations of amlodipine, olmesartan, and rosuvastatin were measured by liquid chromatography tandem mass spectrometry. Safety was evaluated by measuring vital signs, clinical laboratory parameters, physical examinations, and medical interviews.
Results: Sixty-four subjects were enrolled, and 54 completed the study. The geometric mean ratios and 90% CI for the maximum plasma concentration (Cmax) and area under the curve from time zero to the last sampling time (AUCt) were 1.0716 (1.0369,1.1074) and 1.0497 (1.0243,1.0757) for amlodipine, 1.0396 (0.9818,1.1009) and 1.0138 (0.9716,1.0578) for olmesartan, and 1.0257 (0.9433,1.1152) and 1.0043 (0.9453,1.0669) for rosuvastatin. Fourteen cases of adverse events occurred in 12 subjects. There was no statistically significant clinical difference between the formulation groups.
Conclusion: The 90% CI of the primary PK parameters were within the acceptance bioequivalence criteria, which is ln (0.8) and ln (1.25). These results indicate that the FDC formulation and co-administration of amlodipine, olmesartan and rosuvastatin are pharmacokinetically bioequivalent and have similar safety profiles.
Keywords: fixed-dose combination, pharmacokinetics, amlodipine, olmesartan, rosuvastatin
Introduction
Cardiovascular disease (CVD) accounts for about 34.3% of all deaths, and the total cost of CVD is 503.2 billion USD, causing serious social and economic impact on individuals and governments.1 According to the annual report on causes of death, released by the National Statistical Office of Korea, the Korean CVD mortality rate decreased by 0.4 (−0.4%) to 113.1 per 100,000, in 2013. In Korea, CVD was ranked second leading cause of death in 2013, after cancer (149.0 per 100,000).2
Amlodipine and olmesartan are antihypertensive agents with different mechanisms. Amlodipine is a dihydropyridine calcium channel blocker that blocks Ca2+ from entering the cell membrane of the heart and vascular smooth muscle, which directly relaxes the smooth muscle to lower blood pressure. Olmesartan, is an angiotensin II receptor blocker that blocks the binding of angiotensin II to the receptor that contracts the blood vessels. Together, they are often used as a combination therapy for the treatment of hypertensive patients who are unresponsive to single therapy.3,4
Hyperlipidemia is a CVD that is characterized by an increase in serum concentrations of cholesterol, triglycerides, or both, resulting from a metabolic lipoprotein abnormality. It is a major risk factor for arteriosclerosis and increases the risk of coronary artery disease. Rosuvastatin is widely used to treat hyperlipidemia. It lowers the concentration of total cholesterol and LDL-cholesterol in serum by inhibiting 3-hydroxy-3-methyl-glutaryl coenzyme A (HMG-CoA) reductase which inhibits the synthesis of mevalonate. Compared to other hyperlipidemic agents, rosuvastatin, in particular, has a high affinity for HMG-CoA reductase and a high inhibitory effect, which effectively reduces LDL cholesterol and increases HDL cholesterol.5
Hypertension is often associated with increased blood lipids that cause arteriosclerosis. Hypertension and hyperlipidemia are synergistic at the onset and exacerbation of CVD, so treatment should address both morbidities.6 In addition, hypertension and dyslipidemia are more likely to occur in patients with chronic illnesses. As the combined use of therapeutic agents increases, so too does the number of separate medications the patient is required to take, which can reduce medication compliance, leading to poor treatment outcomes. Therefore, reducing the number of separate medications taken by the patient can importantly contribute to good therapeutic results.7,8 The aim of this study was to compare the PK profile and safety of an FDC formulation and co-administration of amlodipine, olmesartan and rosuvastatin in healthy male subjects.
Materials and methods
The study protocol was approved by the Institutional Review Board of Inje University Busan Paik Hospital and the Korean Ministry of Food and Drug Safety (KMFDS) (ClinicalTrials.gov: NCT03753477). All procedures were conducted in compliance with the Declaration of Helsinki, the International Conference on Harmonization of Good Clinical Practice, and the current guidelines of the KMFDS.
Subjects
All subjects signed an informed consent before participating in this study. Healthy male subjects, aged 19–50 years old, with a body mass index between 18 and 27 (kg/m2) were enrolled in this study. All subjects were evaluated as healthy based on their medical history and results of a physical examination which included electrocardiograph (ECG), vital sign measurements, and clinical laboratory tests. The exclusion criteria were as follows: medical history that may affect the absorption, distribution, metabolism and excretion of a drug; sitting position systolic blood pressure (SBP) >140 or <100 mmHg, diastolic blood pressure (DBP) >90 or <65 mmHg, or pulse rate >100 beats/min; history of allergy or hypersensitivity to amlodipine, olmesartan or rosuvastatin; history of drug and/or alcohol abuse; taking any medication that induces or inhibits drug-metabolizing enzymes; blood donation within 30 days of the first day of study drug administration or whole blood donation within 60 days; and participation in other clinical trials within three months.
Study design
This study was a randomized, open-label, 2×2 cross over study with 14-day wash-out periods. The sample size was calculated at 64 subjects for the 90% confidence interval of the geometric mean ratio of the Cmax for rosuvastatin to fall within 0.8–1.25, assuming a significance level of 5%, a power of 90%, and a true geometric mean ratio of 0.95, based on the literature.9–11
All subjects were administered a single FDC tablet containing amlodipine 10 mg/olmesartan 40 mg/rosuvastatin 20 mg (Daewoong Co., Ltd., Seoul, Korea) or co-administered an FDC tablet containing amlodipine 10 mg/olmesartan 40 mg (Daiichi Sankyo Korea Co., Ltd., Seoul, Korea) and a tablet containing rosuvastatin 20 mg (AstraZeneca Korea, Seoul, Korea) for each period, in the fasting state. A 14-day wash out period was determined to be sufficient because it is over five times the elimination half-life of amlodipine (38~45 hrs12), which has the longest elimination time of the three study drugs. Blood samples for pharmacokinetic (PK) analysis of amlodipine and rosuvastatin were collected at baseline and 1, 2, 3, 4, 5, 6, 8, 10, 12, 24, 48, 72 hrs post administration. Blood samples for PK analysis of olmesartan were collected at baseline and 0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 10, 12, 24, 48 hrs post administration. Blood was collected in EDTA K2 tubes and centrifuged at 2,000 g for 10 mins. Plasma samples were removed and transferred to tubes and stored at −70 °C until bioanalysis.
Safety assessment
Vital signs, physical examination results, diagnostic tests, adverse reaction confirmations, combined drug identification, and ECGs of each subject who received at least one does of study drug were evaluated. The occurrence, severity, and frequency of adverse events (AE) and/or adverse drug reactions were compared between treatment groups.
Bioanalysis
Concentrations of amlodipine, olmesartan, and rosuvastatin in plasma samples were measured using LC-MS/MS by BioInfra (Suwon, Republic of Korea). Calibration curves were established in the concentration range of 0.05–50 ng/mL for amlodipine, and 10–2,000 ng/mL for olmesartan, and 0.4–100 ng/mL for rosuvastatin; these had coefficients of determination (R2) greater than 0.9992, 0.9990 and 0.9989, respectively. The CVs for assay precision were less than 15%, 15% and 8.5%, respectively and the accuracy values were greater than 95.5%, 97.1% and 95.9%, respectively. There was no relevant cross-talk or matrix effect.
Pharmacokinetic analysis
Pharmacokinetic analysis was performed with a non-compartmental method using the Pheonix WinNonlin software package version 8.0 (Pharsight, CA, USA). Actual blood sampling time of each subject was used for analysis. The Cmax and Tmax were obtained directly from the time-concentration curves, and the elimination rate constant (k) was obtained by using the least squares method of regression for the log concentration value of the terminal disappearance part of the plasma concentration. The terminal elimination half-life (t1/2β) was calculated by using the equation t1/2β=0.693/k. Linear up/linear down trapezoidal method was used for AUC calculation.
Statistical analysis
Means and standard deviations are presented for continuous variables and the counts and percentages are shown for categorical variables. For PK parameters, Cmax and AUCt, the point estimator of the geometric mean ratio (GMR) (test drug/reference drug) between treatment groups after natural logarithm transformation was estimated and the 90% of confidence interval of this was yield. Statistical analysis was conducted using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Subjects characteristics
Sixty-four healthy male subjects participated in this study. The mean age was 25.63±5.07 years, weight was 71.61±8.10 kg, and height was 174.22±5.98 cm. Two subjects did not complete the study because of investigator judgment and eight subjects withdrew consent. Pharmacokinetic analysis was conducted on all 54 subjects who completed the entire study schedule, and safety analysis was performed on the 62 subjects who were administered at least one dose of study drug.
Pharmacokinetics
The mean plasma concentration of amlodipine, olmesartan, and rosuvastatin over time are presented in Figures 1–3, respectively. Descriptive statistics of the PK parameters for amlodipine, olmesartan, and rosuvastatin in the FDC and co-administration groups are summarized in Table 1. Pharmacokinetic parameters were similar between treatment groups. ANOVA analysis showed no statistically significant difference in treatment, period, or sequence.
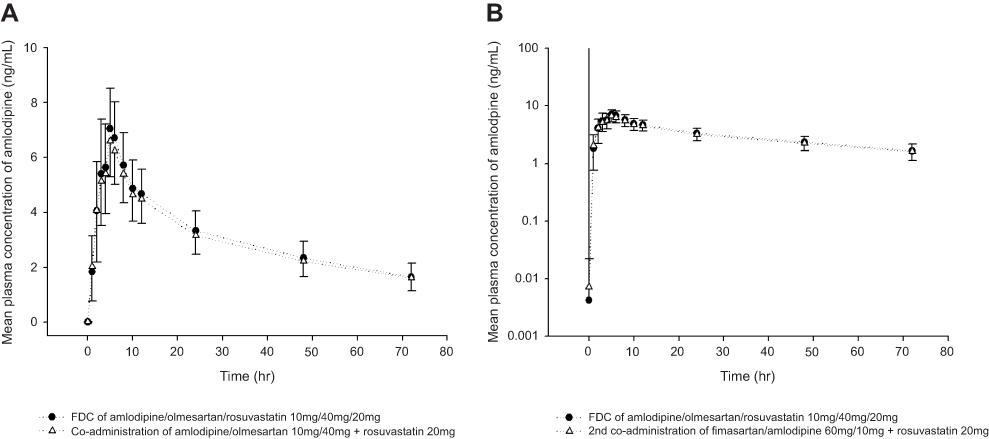 | Figure 1 Mean (SD) plasma concentration profiles of amlodipine following administration of a single oral administration of a fixed-dose combination (FDC) tablet formulation or separate formulations of amlodipine/olmesartan 10/40 mg FDC tablet and rosuvastatin 20 mg tablet in healthy male subjects. Linear scale (A), log scale (B). |
 | Figure 2 Mean (SD) plasma concentration profiles of olmesartan following a single oral administration of a fixed-dose combination (FDC) tablet formulation or co-administration of amlodipine/olmesartan 10/40 mg FDC tablet and rosuvastatin 20 mg tablet in healthy male subjects. Linear scale (A), log scale (B). |
 | Figure 3 Mean (SD) plasma concentration profiles of rosuvastatin following a single oral administration of a fixed-dose combination (FDC) tablet formulation or separate formulations of amlodipine/olmesartan 10/40 mg FDC tablet and rosuvastatin 20 mg tablet in healthy male subjects. Linear scale (A), log scale (B). |
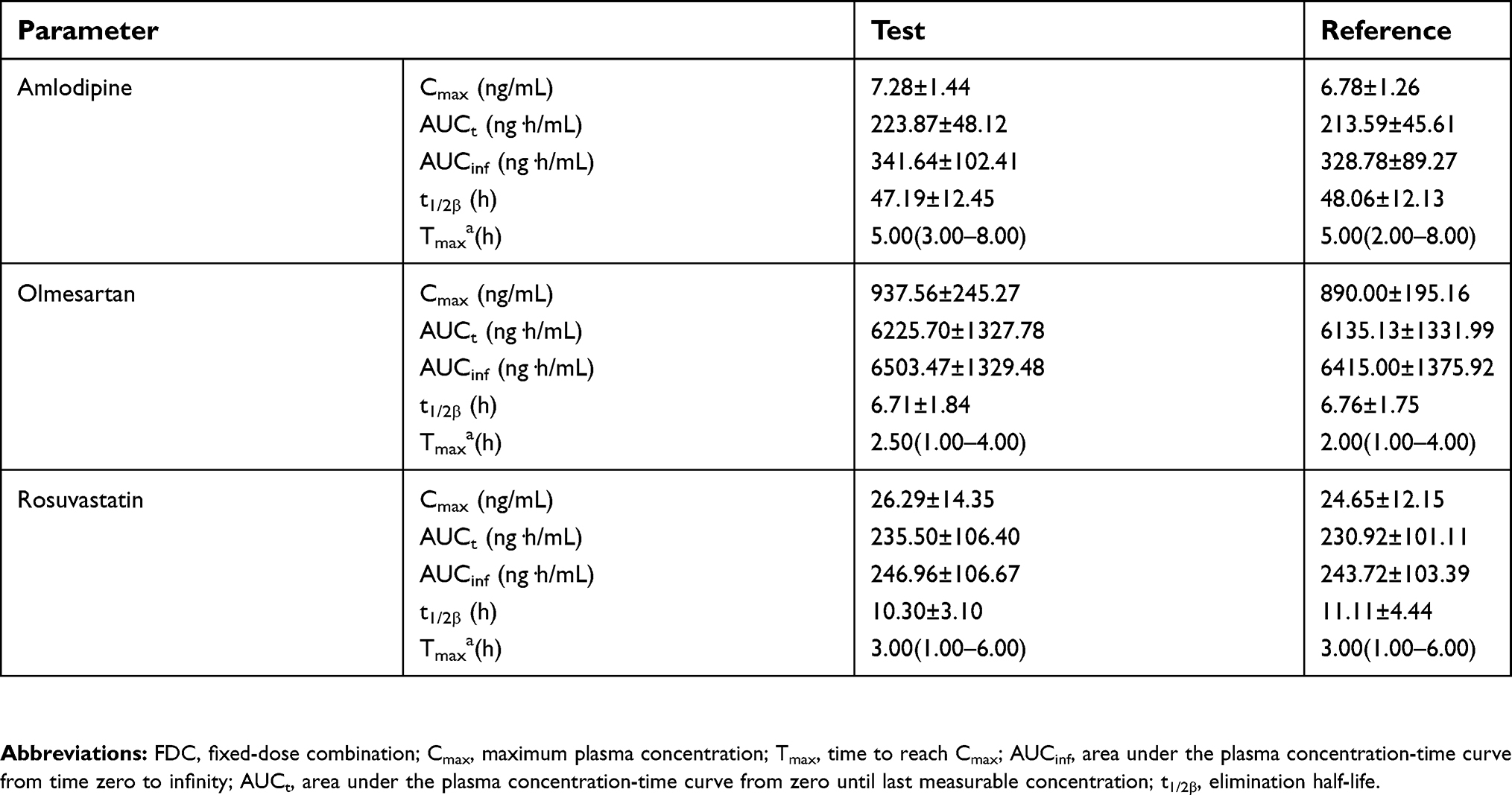 | Table 1 Pharmacokinetic properties of amlodipine, olmesartan, and rosuvastatin following single oral administration of FDC tablet or co-administration, in healthy male subjects (n=54) |
The GMRs (90% CI) of Cmax and AUCt were 1.0716 (1.0369, 1.1074) and 1.0497 (1.0243, 1.0757) for amlodipine, 1.0396 (0.9818, 1.1009) and 1.0138 (0.9716, 1.0578) for olmesartan, and 1.0257 (0.9433, 1.1152) and 1.0043 (0.9453, 1.0669) for rosuvastatin, respectively (Table 2). The 90% CI of the primary PK parameters such as Cmax and AUCt fell within the equivalence criteria of 0.80–1.25.
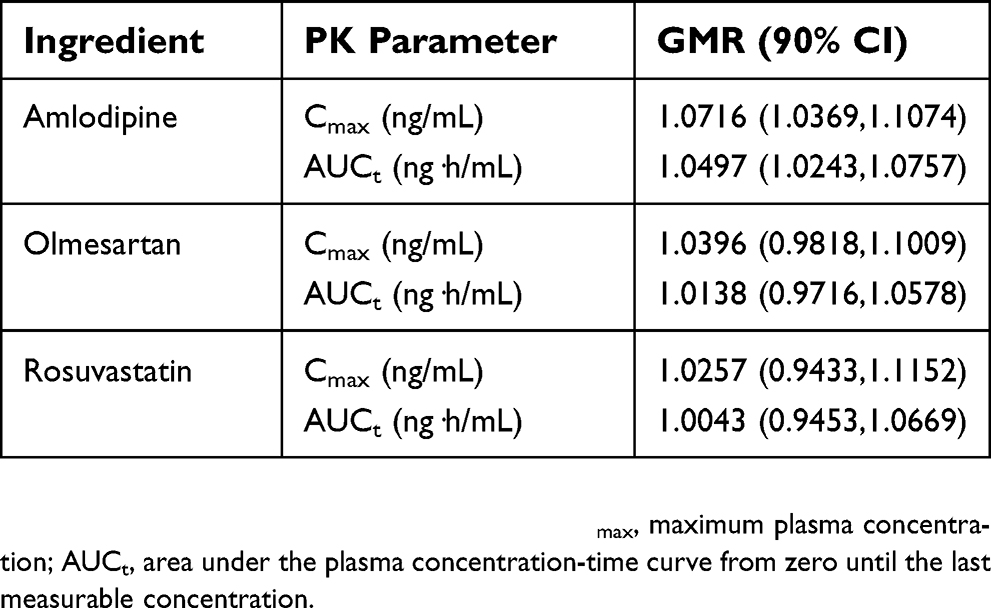 | Table 2 Geometric mean ratios (90% CI) of the pharmacokinetic properties of amlodipine, olmesartan, and rosuvastatin following single oral administration of FDC formulation tablet or co-administration in healthy male subjects (n=54) |
Safety
Fourteen AEs were observed in 12 subjects who were administered at least one dose of study drug (n=62). There were 11 mild AE cases and three moderate cases. In the co-administration group (n=58), there were six cases of AEs in six patients, one of which (bronchitis) was evaluated as not related to the study drug. There were eight cases of AEs in seven of the subjects who received the FDC formulation (n=59), three of them were evaluated as unrelated to the study drug (tendonitis, gastroenteritis, and urinary tract infection). There were no deaths during the study. One serious adverse event (bronchitis) occurred, and one subject dropped out due to AE (urinary tract infection). In both cases, the cause of the AEs was evaluated as unrelated to the study drug. There were no statistically significant differences in the number of subjects with AE or adverse drug reaction between the treatment groups (p=0.7630).
Discussion
The purpose of this study was to evaluate the PK and safety profiles of FDC and co-administration of amlodipine, olmesartan, and rosuvastatin. The results of statistical analysis for PK parameters demonstrated that the 90% CIs for GMRs of Cmax and AUCt were within the acceptance equivalence limit (0.8–1.25). This indicates that the FDC formulation was bioequivalent to co-administration, and that there was no statistically significant clinical difference between the formulations.
Essential hypertension is a condition in which arterial blood pressure is consistently high. High blood pressure is defined by the WHO (World Health Organization) as resting SBP equal to or anove 140 mmHg and./or DBP equal to or above 90 mmHg.13,14 A new 2017 AHA/ACC (American Heart Association/American College of Cardiology) guideline defines high blood pressure to be SBP ≥130 mmHg or DBP ≥80 mm Hg.15 According to the 2012 Korean National Health and Nutrition Examination Survey (KNHANES V-S), one in three men and one in four women over 30 years old are suffering from hypertension.16,17
One in ten Koreans over 30 years old have hyperlipidemia, and the prevalence is steadily increasing.16,17 Hyperlipidemia is characterized by elevated serum cholesterol or triglycerides caused by metabolic abnormalities of lipoprotein, and is a major risk factor for atherosclerosis and increases the risk of coronary artery disease. Hypertension and hyperlipidemia are significant risk factors for CVD. They increase the risk of coronary artery disease synergistically, and are commonly co-morbid. A retrospective study of 371,221 patients who visited six hospitals of the US Veterans Administration for three years from 1998 to 2001 found that 30.4% had both hyperlipidemia and hypertension.18
The guidelines from the 2018 European Society of Hypertension and European Society of Cardiology recommend hypertension treatment with two or more concomitant therapies rather than monotherapy. They also advise the use of FDC formulation rather than a co-administration.19
Amlodipine, olmesartan, and rosuvastatin are very likely to be used in combination long-term therapy for treatment of hyperlipidemia and hypertension. These increasingly prevalent chronic illnesses are often treated with multiple therapeutic agents which often decreases medication compliance. Changing from co-administration of amlodipine, olmesartan, and rosuvastatin to a single FDC formulation may be more convenient for the patient and result in greater medication compliance which may lead to better treatment outcomes.
Conclusion
This study demonstrated that the PK profile of an FDC formulation of amlodipine, olmesartan and rosuvastatin was bioequivalent to the co-administration of these drugs. The safety profiles were similar and there were no statistically significant clinical differences between the two formulations.
Acknowledgment
This was funded by Daewoong Pharma, Seoul, Republic of Korea.
Disclosure
BHK, JYK, HJS, and HJS are employed by Daewoong Pharma. The authors report no other conflicts of interest in this work.
References
1.
2. Yeon OK, Yun JHS. The Statics of Deaths in 2013. Daejeon, Republic of Korea: The Korean National Statistical Office(KNSO); 2013.
3. Frampton JE, Scott LJ. Amlodipine/valsartan single-pill combination. Am J Cardiovasc Drug. 2009;9(5):309–330. doi:10.2165/11201120-000000000-00000
4. Schwocho LR, Masonson HN. Pharmacokinetics of CS‐866, a new angiotensin II receptor blocker, in healthy subjects. J Clin Pharmacol. 2001;41(5):515–527.
5. Li Y, Jiang X, Lan K, Zhang R, Li X, Jiang Q. Pharmacokinetic properties of rosuvastatin after single-dose, oral administration in Chinese volunteers: a randomized, open-label, three-way crossover study. Clin Ther. 2007;29(10):2194–2203. doi:10.1016/j.clinthera.2007.10.005
6. Jackson R, Lawes CM, Bennett DA, Milne RJ, Rodgers A. Treatment with drugs to lower blood pressure and blood cholesterol based on an individual’s absolute cardiovascular risk. Lancet. 2005;365(9457):434–441. doi:10.1016/S0140-6736(05)70240-3
7. Dezii C. A retrospective study of persistence with single-pill combination therapy vs. concurrent two-pill therapy in patients with hypertension. Managed Care (Langhorne, Pa). 2000;9(9 Suppl):2–6.
8. Verma AA, Khuu W, Tadrous M, Gomes T, Mamdani MM. Fixed-dose combination antihypertensive medications, adherence, and clinical outcomes: A population-based retrospective cohort study. PLoS Med. 2018;15(6):e1002584. doi:10.1371/journal.pmed.1002593
9. Lee S-Y, Kim J-R, Jung JA, Huh W, Bahng MY, Ko J-W. Bioequivalence evaluation of two amlodipine salts, besylate and orotate, each in a fixed-dose combination with olmesartan in healthy subjects. Drug Des Devel Ther. 2015;9:2811. doi:10.2147/DDDT.S82820
10. Oh MJ, Hwang HH, Kim HG, et al. Bioequivalence study of a new fixed-dose combination tablet containing S-amlodipine nicotinate and olmesartan medoxomil in healthy Korean male subjects. Clin Ther. 2017;39(7):1371–1379. doi:10.1016/j.clinthera.2017.05.355
11. Park J-Y, Kim K-A, Lee G-S, et al. Randomized, open-label, two-period crossover comparison of the pharmacokinetic and pharmacodynamic properties of two amlodipine formulations in healthy adult male Korean subjects. Clin Ther. 2004;26(5):715–723.
12. Rohatagi S, Lee J, Shenouda M, et al. Pharmacokinetics of amlodipine and olmesartan after administration of amlodipine besylate and olmesartan medoxomil in separate dosage forms and as a fixed‐dose combination. J Clin Pharmacol. 2008;48(11):1309–1322. doi:10.1177/0091270008322176
13.
14. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. Jama. 2003;289(19):2560–2571. doi:10.1001/jama.289.19.2560
15. Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;70(2):252–289. doi:10.1016/j.jacc.2017.03.011
16. The Statistics of 5th Korea National Health and Nutrition Examination Survey (KNHANES V-S) in 2011. Korea Centers for Disease Control and Prevention; 2011.
17. Mokrini F, Waeyenberge L, Viaene N, Moens M The Statistics of the 8th Korea Youth Risk Behavior Web-based Survey(KYRBWS) in 2012. Korea Centers for Disease Control and Prevention; 2012. doi:10.1094/PDIS-11-11-0999-PDN
18. Johnson ML, Pietz K, Battleman DS, Beyth RJ. Prevalence of comorbid hypertension and dyslipidemia and associated cardiovascular disease. Heart Dis. 2004;2:3.
19. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. doi:10.1093/eurheartj/ehy339
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.