Back to Journals » Journal of Pain Research » Volume 13
10 kHz Spinal Cord Stimulation for Combined Alleviation of Post-Laminectomy Syndrome and Chronic Abdominal Pain: A Case Report
Authors Berger AA ![]() , Hasoon J
, Hasoon J ![]() , Urits I
, Urits I ![]() , Viswanath O, Gill J
, Viswanath O, Gill J
Received 29 December 2019
Accepted for publication 9 April 2020
Published 30 April 2020 Volume 2020:13 Pages 873—875
DOI https://doi.org/10.2147/JPR.S244084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Robert B. Raffa
Amnon A Berger,1 Jamal Hasoon,1 Ivan Urits,1 Omar Viswanath,2– 4 Jatinder Gill1
1Beth Israel Deaconess Medical Center and Harvard Medical School, Department of Anesthesia, Critical Care and Pain Medicine, Boston, MA, USA; 2Valley Anesthesiology and Pain Consultants – Envision Physician Services, Phoenix, AZ, USA; 3University of Arizona College of Medicine-Phoenix, Department of Anesthesiology, Phoenix, AZ, USA; 4Creighton University School of Medicine, Department of Anesthesiology, Omaha, NE, USA
Correspondence: Jamal Hasoon
Beth Israel Deaconess Medical Center and Harvard Medical School, Department of Anesthesia, Critical Care and Pain Medicine, Boston, MA, USA
Email [email protected]
Abstract: Chronic pain affects roughly 50 million Americans, or 20.4% of the national population, and is a huge economic burden on society. Spinal cord stimulation (SCS) is a cost-effective interventional treatment modality for patients with chronic neuropathic and radicular pain. It is traditionally reserved for patients suffering from post-laminectomy syndrome, complex regional pain syndrome, or chronic back pain that is refractory to other less invasive techniques. There have been a few cases describing the use of SCS at higher levels to successfully obtain coverage of visceral abdominal pain. Here we describe an interesting case of a patient who suffered from chronic back pain and radiculopathy with post-laminectomy syndrome as well as chronic abdominal pain. We describe the use of high-frequency SCS to alleviate the patient’s post-laminectomy pain as well as his abdominal pain. Our case describes SCS use with multi-level lead placement targeting both post-laminectomy pain and abdominal pain. We describe a strategy that can be useful to patients with concurrent pain from more than one source. Our case also adds to the growing evidence supporting the use of SCS for treating chronic visceral pain syndromes.
Keywords: abdominal pain, chronic pain, neuromodulation, spinal cord stimulation
Introduction
According to CDC data from the 2016 National Health Interview Survey, chronic pain affects roughly 50 million Americans, or 20.4% of the national population. Chronic low back and neck pain carries an estimated healthcare spending cost of $67.5 billion-$94.1 billion annually, the third highest in the US after ischemic heart disease and diabetes.1 The costs are even higher when societal costs are also included.2 Spinal cord stimulation (SCS) is a cost-effective interventional treatment modality for patients with chronic neuraxial and radicular pain. It is traditionally reserved for radiculopathy or chronic back pain that is refractory to other less invasive techniques.3 However, there is some evidence that SCS may be useful for a variety of visceral pain syndromes as well.4–7
There have been a few case reports of using SCS at higher levels than traditional levels to successfully obtain coverage of visceral abdominal pain such as pancreatitis.4,5 Leads are placed higher around T5-T6 for visceral coverage.6 Here we present an interesting case of a patient who suffered from chronic back pain and radiculopathy with post-laminectomy syndrome as well as chronic abdominal pain. We describe the use of high-frequency SCS to alleviate the patient’s post-laminectomy pain as well as his abdominal pain.
Case Description
We describe the case of a 56-year-old male suffering from post-laminectomy syndrome with long-standing right-sided back pain and lumbar radiculopathy. He also was suffering from severe chronic lower abdominal pain despite an extensive evaluation and diagnostic work-up by Gastroenterology. His previous medical history also included hypertension, asthma, GERD, hyperlipidemia, obesity, PVD, and sleep apnea. He presented for evaluation of a potential SCS implantation after a long history of failed treatment for his chronic back pain. His previous treatments included medication management with combinations of non-opioid analgesics, neuropathic medications, NSAID, muscle relaxants and opioids. He also underwent numerous procedures including interlaminar lumbar epidural steroid injections, caudal epidural steroid injections, medial branch blocks and radiofrequency ablations with minimal success. He participated in pain-targeted psychotherapy, including cognitive behavioral therapy, with no improvement in his pain. He was referred to our practice for SCS consideration.
The patient ultimately had a successful trial and subsequently underwent permanent implantation with 10 kHz high-frequency spinal cord stimulation. To properly address his multiple pain complaints that included abdominal, axial, and radicular pain, one lead was advanced to the middle of T8 to address his chronic back pain and radiculopathy, while a second lead was advanced to the top of T6 to provide lower abdominal coverage (Figure 1). The patient tolerated the procedure well and went home the same day. During the patient’s follow up appointments he has endorsed 70% improvement in back pain and radiculopathy along with 100% relief of his abdominal pain.
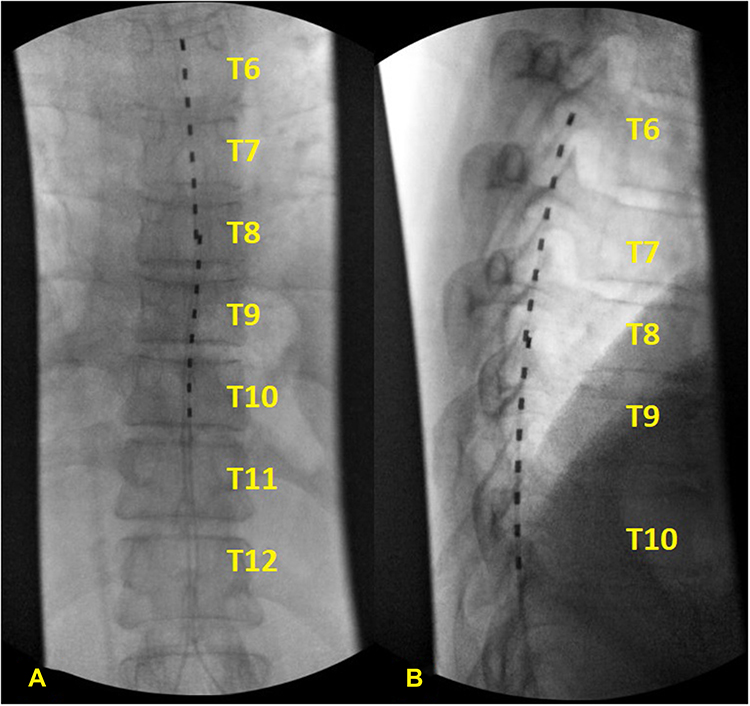 |
Figure 1 Lead placement, (A) anterior and (B) lateral views. Notes: Intra-operative fluoroscopy images demonstrate overlapping placement of the spinal cord stimulator leads from (A) anterior and (B) lateral views. The placement of the leads allows coverage from T6 down to T10 for optimal coverage of both back and leg as well as abdominal pain. |
The patient had two 8-contact leads placed utilizing high-frequency electrical stimulation pulses at 10 kHz. This method of stimulation does not rely on producing paresthesia, differing from traditional SCS. Traditional SCS therapy typically delivers electrical pulses at a frequency below 1200 Hz. Traditional SCS therapy replaces a patient’s pain with paresthesia, which are induced sensations that can be perceived as tingling or buzzing sensations. However, some patients may find the paresthesia created from traditional SCS therapy to be uncomfortable. High-frequency stimulation, specifically using 10 kHz therapy, is different from traditional SCS therapy in that it relieves pain without paresthesia which can be more desirable for some patients.
In regards to this patient, he utilizes 10 kHz therapy at an amplitude of 2mA with two programing options to alleviate his pain. He utilizes consistent high-frequency stimulation of his upper lead to optimize his abdominal pain coverage. Additionally, he utilizes a separate program for his axial back pain and radiculopathy. For these complaints, he utilizes pulse dosing over the T9-T10 discs with a two-minute off-time between pulses. During his follow up appointments, he continues to endorse good pain relief.
This case highlights the ability of SCS to achieve appropriate pain control of different types of chronic pain by varying the vertebral location of the SCS leads in the epidural space.
Conclusion
This case describes SCS insertion with multi-level lead placement targeting both post-laminectomy pain and abdominal pain. This strategy can be useful to patients with concurrent pain from more than one source. Additionally, this case adds to the growing evidence that SCS can be helpful in treating chronic visceral pain syndromes. We look forward to following this patient’s long-term results with our treatment and believe this case further demonstrates the usefulness of SCS in difficult to treat chronic pain conditions.
Patient Consent
Written informed consent has been provided by the patient to have the case details any accompanying images published.
Institutional Approval
Institutional approval was not required to publish the case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dieleman JL, Baral R, Birger M, et al. US spending on personal health care and public health, 1996–2013. JAMA. 2016;316(24):2627–2646. doi:10.1001/jama.2016.16885
2. Geurts JW, Willems PC, Kallewaard JW, van Kleef M, Dirksen C. The impact of chronic discogenic low back pain: costs and patients’ Burden. Pain Res Manag. 2018;2018:4696180. doi:10.1155/2018/4696180
3. Viswanath O, Urits I, Bouley E, Peck J, Thompson W, Kaye AD. Evolving spinal cord stimulation technologies and clinical implications in chronic pain management. Curr Pain Headache Rep. 2019;23(6):39. doi:10.1007/s11916-019-0778-9
4. Khan YN, Raza SS, Khan EA. Application of spinal cord stimulation for the treatment of abdominal visceral pain syndromes: case reports. Neuromodulation. 2005;8:14–27. doi:10.1111/j.1094-7159.2005.05216.x
5. Kapural L, Cywinski JB, Sparks DA. Spinal cord stimulation for visceral pain from chronic pancreatitis. Neuromodulation. 2011;14:
6. Kapural L, Nagem H, Tlucek H, et al. Spinal cord stimulation for chronic visceral abdominal pain. Pain Med. 2010;11(3):347–355. doi:10.1111/j.1526-4637.2009.00785.x
7. Hasoon J, Berger AA, Urits I, Orhurhu V, Viswanath O, Aner M. Spinal cord stimulation for the treatment of chronic pelvic pain after Tarlov cyst surgery in a 66-year-old woman: a case report. Case Rep Womens Health. 2020;11:e00171. doi:10.1016/j.crwh.2020.e00171
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.