")
Back to Journals » Nature and Science of Sleep » Volume 16
Parents’ Sleep Multi-Trajectory Modelling from 3 to 36 Months Postpartum in the SEPAGES Cohort
Authors Kim M , Lyon-Caen S, Bayat S , Philippat C, Plancoulaine S
Received 26 July 2023
Accepted for publication 14 November 2023
Published 6 March 2024 Volume 2024:16 Pages 247—261
DOI https://doi.org/10.2147/NSS.S430024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Valentina Alfonsi
Mihyeon Kim,1 Sarah Lyon-Caen,2 Sam Bayat,3 Claire Philippat,2 Sabine Plancoulaine1,4
1Université Paris Cité and Université Sorbonne Paris Nord, Inserm, INRAE, Center for Research in Epidemiology and StatisticS (CRESS), Paris, F-75004, France; 2University Grenoble Alpes, Inserm U1209, CNRS UMR 5309, Team of Environmental Epidemiology applied to Development and Respiratory Health, Institute for Advanced Biosciences, Grenoble, France; 3STROBE Inserm UA7 Laboratory & Grenoble University Hospital, Sept. of Pulmonology, Grenoble, France; 4Université Claude Bernard Lyon 1, CNRS, INSERM, Centre de Recherche en Neurosciences de Lyon CRNL U1028 UMR5292, WAKING, Bron, F-69500, France
Correspondence: Sabine Plancoulaine, INSERM U1153, Team 6 EAROH, 16 Avenue Paul Vaillant Couturier, Villejuif Cedex, 94807, France, Email [email protected]
Objective: We investigated maternal and paternal sleep evolution from 3 to 36 months postpartum, their interrelations and predictors in the SEPAGES cohort.
Methods: Sleep information (night sleep duration [NSD], weekend daytime sleep duration [DSD] and subjective sleep loss [SSL]) was collected by self-administered questionnaires at 3, 18, 24 and 36 months postpartum in the SEPAGES French cohort that included 484 mothers and 410 fathers. Group-based multi-trajectory modelling was used to identify maternal, paternal and couple sleep multi-trajectory groups among 188 couples reporting sleep data for at least 2 time points. Multinomial logistic regression was used to assess associations between parental sleep multi-trajectories and early characteristics such as sociodemographic, chronotypes, child sex, birth seasonality or breastfeeding duration.
Results: We identified three maternal (M1-M3), paternal (F1-F3) and couple (C1-C3) sleep multi-trajectory groups with similar characteristics: a group with short NSD and high SSL prevalence (M1, F2, C2), a group with long NSD but medium SSL prevalence (M2, F3, C3) and a group with long NSD and low SSL prevalence (M3, F1, C1). Mothers with the shortest NSD (M1) were less likely to have a partner with long NSD (F2). As compared with long NSD and low SSL prevalence (C1), couples with short NSD and high SSL prevalence (C2) were less likely to have had a first child born in the autumn and fathers in C2 had a later chronotype.
Conclusion: We identified distinct sleep multi-trajectory groups for mothers, fathers and couples from 3- to 36-month postpartum. Sleep patterns within couples were homogeneous.
Keywords: multi group-based-trajectory modelling, parental sleep, sleep epidemiology, sleep interrelation
Introduction
Healthy sleep, characterized as adequate duration, appropriate timing and good quality without disturbances, is a key element for a healthy life.1,2 Appropriate night sleep duration (NSD) for healthy adults is from 7 to 9 hr per night on a regular basis.2 Several factors have been reported to be cross-sectionally and longitudinally associated with sleep quantity and quality. In the general population, odds of self-reported short sleep less than 6 or 7 hr/night was found associated with high BMI and low socioeconomic position (ie, low education level, unemployment and poor living condition)3,4 as was poor sleep quality.5 Additionally, cross-sectional studies suggested that late chronotype3,6 (ie, preference for eveningness or later mid-sleep) is associated with short sleep duration in the general population. Sex differences in sleep duration have been reported. Men are more likely to report shorter sleep than women in the general population7 and among couples.8–11 Despite longer sleep duration than men, women reported higher prevalence of poor sleep quality in the general young adult population12 and more frequent nocturnal disturbances when in a couple relationship.13
Couples’ sleep is additionally altered by the arrival of a newborn. Mothers and fathers from the third to eighth postpartum weeks experienced greater sleep disturbances, lower sleep efficiency and sleepiness than childless couples.9,11,14 US and German prospective cohort studies found that first-time mothers and fathers lost an average of about 40 min and 15 min of mean NSD as compared with pre-pregnancy NSD during the first14 and first 3 postpartum months,15 respectively. The German study additionally reported that women experienced a 1-hr reduction in NSD as compared with pre-pregnancy during the first 3 months postpartum and then slowly recovered until 4 to 6 years postpartum.15
Parental sleep patterns can also vary according to child-specific factors such as child age, breastfeeding and the number of children they have. As example, parents with children up to age 2 years had lower sleep quantity16 and quality17 than those with older children. Also, breastfeeding has been associated with longer sleep duration of mothers or both parents up to 1 year postpartum as compared with bottle feeding.18 Although those factors are associated with both maternal and paternal sleep, first-time mothers reported longer consecutive nocturnal sleep duration, fewer nocturnal awakenings and better sleep quality but with no difference in total NSD as compared with experienced mothers at 6 months postpartum.19,20 Paternal sleep patterns did not differ according to parental experience.19,20
However, previous studies have limitations. First, they included relatively small sample sizes between 50 and 100 couples.9,10,14,19 Second, they were performed cross-sectionally14,17,19 or longitudinally but only in early postpartum (ie, up to 6 months),9,10,21 which may not fully reflect the parental sleep transition considering that parental sleep duration may not fully recover until 4 years after the birth of a first child.15 Thus, a longitudinal study overviewing sleep transition from early postpartum and over few years would provide a better understanding of sleep in couples with a newborn. Third, they considered the global mean of parental sleep durations, which may not reflect the variety of sleep patterns across the population. The diversity of sleep evolutions over time could be better characterized by trajectory modelling, as has been reported in adults from general population.22
Thus, our aims in this study were to identify 1) parents’ sleep evolution from 3 to 36 months postpartum (as individuals and within couples) by using group-based multi-trajectory modelling, which analyses multiple outcomes simultaneously and longitudinally, and 2) sleep interrelations between maternal and paternal sleep multi-trajectory groups from 3 to 36 months postpartum.
Methods
Study Design
The Suivi de l’Exposition à la Pollution Atmosphérique durant la Grossesse et Effet sur la Santé (SEPAGES; https://cohorte-sepages.fr/en) cohort is aimed at characterizing the exposure to environmental contaminants and their influence on the health of pregnant women, fetuses, and children. The cohort details have been previously published.23 Briefly, 2,321 pregnant mothers were eligible: they were at less than 19 gestational weeks, older than 18 years, had a singleton pregnancy, lived in the Grenoble area (France) and planned to give birth in one of the four maternity clinics involved in the study. Participation rate was 21%, and 484 mothers were included. Male partners (n = 410) were included when they were older than 18 years old and had social insurance. Data collection started in the first or the very beginning of the second trimester of pregnancy and regularly up to 36 months. Participation to the entire protocol was compensated at a rate of 50 euros.
Participating mothers and fathers signed consent for themselves and their child. The SEPAGES cohort obtained approval from the Comité de Protection des Personnes Sud-Est V (CPP) and the Commission Nationale de l’Informatique et des Libertés (CNIL), the French data privacy institution.23 This study complies with the Declaration of Helsinki.
Data Collection
Main Measures for Postpartum Sleep Trajectory Modelling
Maternal and paternal sleep information were collected by self-administered questionnaires at 3, 18, 24 and 36 months postpartum. Bedtime and wake-up times were collected for both weekdays and weekend days at each time point with the questions “What time do you go to bed?” and “What time do you wake up?”. Mean NSD for the total week was calculated in hours and minutes. Daytime sleep duration during weekdays and weekend days was collected by 2 questions: “Do you take nap? (Y/N)” and “How long do you take nap?”. Weekday naps were infrequent among mothers and fathers between 3 and 36 months postpartum (<10%) except for mothers at 3 months postpartum (14.6%) and were more common during weekend days (>45.0%), so we considered only weekend daytime sleep duration (weekend DSD) in the analysis. Subjective sleep loss (SSL) was collected by the question “Do you think you do not have enough sleep? (Y/N)”.
Because parental NSD might be affected by the frequency of child night wakings, especially in the early months postpartum, we performed a sensitivity analysis using the recalculated mean NSD accounting for child night waking frequency. Information on child night waking was collected with 2 questions: “How many nights does your child wake up during the night? (Never or almost; sometimes; one in two nights; and every night or almost)” and “How many times per night did your child wake up? (Once a night; and at least twice a night)”. We arbitrary subtracted 30 min per night waking from both maternal and paternal NSD at each age. Thus, we deducted 1 hr of NSD when child night waking occurred at least twice a night, every night or almost every night; 30 min of NSD when child night waking occurred once a night, every night or almost every night or one in two nights at least twice a night; and 15 min of NSD when child night waking occurred once in two nights. We performed no deduction for couples reporting that the child never or almost never woke up or only woke up sometimes.
Early Predictors of Sleep Patterns
Household socioeconomic, demographic and maternal or paternal factors were collected at inclusion for both the mother and father: education attainment (below bachelor, Y/N), working during pregnancy (Y/N), work qualification (labourer and employee, intermediate profession, and executive or higher intellectual profession), age at conception, and pre-pregnancy BMI. Nationality (European or not) was also collected but not accounted for because of low variability (only 2 individuals were of non-European origin). The Hospital Anxiety and Depression scale (HAD), validated in French general population,24 was used to estimate the presence of anxiety and depressive symptoms in the 2nd trimester of pregnancy for fathers and the 3rd trimester for mothers. A score ≥8 was considered presence of anxiety or depressive symptoms25 (Cronbach’s alpha = 0.79 for the whole questionnaire, 0.65 for anxiety and 0.66 for depression). Maternal and paternal chronotype were estimated by the Munich Chronotype Questionnaire26 at 1 year postpartum and corresponded to mid-sleep time on free days accounting for sleep debt. Tobacco smoking during pregnancy (Y/N) was collected for only mothers. Finally, the early child’s characteristics were collected at birth from parental-reported questionnaires and the medical record, including the delivery method (caesarean section or vaginal delivery), sex, birth term (weeks), birth weight (kg), and being a first child (Y/N). Childbirth seasonality was estimated based on the month of birth and classified as spring (Mar–May), summer (Jun–Aug), autumn (Sep–Nov), and winter (Dec–Feb). Information on breastfeeding was collected at age 2, 18, 24 and 48 weeks postpartum and dichotomised as breastfed for ≥26 weeks (Y/N). In a sensitivity analysis, we additionally included maternal weekday nap at 3 months postpartum (Y/N) as a covariate.
Statistical Methods
All statistical analysis was performed with SAS® v9.4 (SAS Institute Inc, Cary, NC, USA).
Multi-Trajectory Modelling
The group-based multi-trajectory modelling method (PROC TRAJ procedure) developed by Nagin et al27–31 was used to identify maternal, paternal and couple sleep multi-trajectory groups based on NSD, weekend DSD and SSL between 3 and 36 months postpartum. The method is based on the underlying assumption that the population consists of a mixture of distinct groups defined by individual differences in each trajectory, which is considered to approximate population distribution and their shape. The method identifies latent groups of individuals following similar trajectories across multiple outcomes of interest; thus, each multi-trajectory group is defined by a set of trajectories for multiple outcomes, modelled using polynomial functions of time.30 Each mother, father and couple were included in the multi-trajectory modelling if information on sleep characteristics was available for at least 2 of 4 time points collected for both parents, in order to characterize their interrelationships within the couple. Different models of 2 to 5 multi-trajectory groups were computed separately for mothers, fathers and couples. The best-fitting models were selected according to Bayesian information criteria (BIC) and were verified according to the recommended criteria: the average probability of belonging to each trajectory (≥0.7), the odds of correct classification (≥5) and the similarity between the model’s estimation of the trajectory prevalence and the actual prevalence.27,29 Each individual or couple was assigned to the sleep multi-trajectory group to which they had the highest probability of belonging. In sensitivity analyses, multi-trajectory modelling was re-run using the re-calculated mean NSD after accounting for child night waking frequency at each age.
Association Analysis
Confounding factors in the analysis of the association between maternal and paternal sleep multi-trajectory groups were identified from the literature and by using a directed acyclic graph.32 Potential factors associated with couples’ sleep multi-trajectory groups were identified from the literature only. Multiple imputation with fully conditional specification (SAS 9.4: MI procedure, FCS option) was used to impute missing covariate data (4.9%) on a variable-by-variable basis; nominal and ordinal variables were imputed by multinomial logistic regression and continuous variables by linear regression. Twenty datasets were established and analyzed. Pooled effect estimates were calculated (SAS 9.4: MIANALYSE procedure) according to Rubin’s rules.33 Associations between maternal and paternal sleep multi-trajectory groups and then between couples’ sleep multi-trajectory groups and potentially associated covariates were assessed with multinomial regression analysis. Additional multinomial logistic regression was used to determine how mothers’ or fathers’ sleep characteristics were modified with the presence of their partners within couples and thus assessed the relations between maternal or paternal sleep multi-trajectory groups and couples’ sleep multi-trajectory groups. In all analyses, the chosen reference group was the one closest to the recommended sleep duration in adulthood and lowest prevalence of SSL (ie, M3, F1 and C1 for mothers, fathers and couples, respectively). The level of significance was defined by p < 0.05.
Results
Population Characteristics
As our main aim was to characterize sleep interrelationships within couples, the included individuals had to be in couples and have available sleep data for trajectory modelling. Of the 484 women and 410 men registered in the cohort, sleep data were available for 339 women and 212 men, making in 188 couples eligible for the study (Figure 1). Their characteristics are presented in Table 1. Maternal NSD, weekend DSD and SSL did not significantly differ at any time-point by their partners’ inclusion (data not shown). As compared with excluded mothers (n = 296), included mothers were more frequently in an executive or higher intellectual profession (57.3% vs 46.1%, p = 0.01) (Table 2). As compared with excluded fathers (n = 222), included fathers had lower BMI (23.8 vs 24.8 kg/m², p = 0.004), less frequently had anxiety symptoms during their partner’s pregnancy (20.7% vs 31.1%, p = 0.05) and more frequently had an earlier chronotype (3h12 vs 3h30, p = 0.04). Other maternal, paternal and child characteristics did not differ between included and excluded individuals.
 |
Table 1 Population Characteristics |
 |
Table 2 Maternal and Paternal Sleep Characteristics at Each Time Point Postpartum (N = 188) |
 |
Figure 1 Flowchart of the population. |
Overall, from 3 to and 36 months postpartum, mean NSD and weekend DSD were longer for mothers than fathers, but the prevalence of SSL was lower and more stable over time for fathers compared to mothers (Table 2).
Identification of Multi-Trajectory Groups of Sleep Patterns
The best maternal sleep multi-trajectory model was a 3-group model illustrated in Figure 2A. All trajectories were best explained by a linear or constant relationship except for the NSD trajectory of group 1, which was best explained by a cubic shape. Mothers belonging to group M1 (19.7% of mothers, n = 37) had the shortest mean NSD, at 7h48, between 3 and 18 months, decreasing to a plateau at 7h36 from 24 months postpartum. This group also had a short mean weekend DSD, decreasing from 13 to 2 min between 3 and 18 months and then remaining stable. This DSD corresponded to a stable mean DSD of 60 min in a decreasing proportion of napping mothers (18.9% to 2.7%). In addition, this group showed a high prevalence of SSL (about 80%) between 3 and 36 months with a peak of 86% at 24 months postpartum. Mothers belonging to group M2 (33.0% of mothers, n = 62) had a mean NSD decreasing from 8h30 to 8h between 3 and 18 months and then remaining stable; a long mean weekend DSD varying from 61 to 50 min, corresponding to 65 and 57 min for those who napped (range 90.3% to 66.1%); and very high SSL prevalence, fluctuating from 89% to 95% between 3 and 36 months postpartum. Mothers belonging to group M3 (47.3%, n = 89) had the longest mean NSD, decreasing from 9h18 to 8h42 between 3 and 18 months and then remaining stable; a moderate and decreasing weekend DSD from 33 to 21 min between 3 and 36 months, corresponding to 61 and 49 min for 46.1% to 37.1% of napping mothers; and a decreasing SSL from 62% to 32.8% between 3 and 24 months, then remaining stable. The latter group, with the most optimal sleep patterns, was chosen as the reference group for association analyses.
 |
Figure 2 Sleep multi-trajectories from 3 to 36 months postpartum in the SEPAGES cohort. (A) Maternal sleep multi-trajectories (M1-M3). 1: M1 (N=37, 19.7%), 2: M2 (N=62, 33.0%), 3: M3 (N=89, 47.3%). Lines represent mean night and weekend daytime sleep duration and subjective sleep loss trajectories. (B) Paternal sleep multi-trajectories (F1-F3). 1: F1 (N=70, 37.2%), 2: F2 (N=35, 18.6%), 3: F3 (N=83, 44.1%). Lines represent mean night and weekend daytime sleep duration and subjective sleep loss trajectories. (C) Couple sleep multi-trajectories (C1-C3). M: maternal, F: paternal, C1 (N=55, 29.2%), C2 (N=52, 27.6%) and C3 (N=81, 43.1%). Lines represent mean night and weekend daytime sleep duration and subjective sleep loss trajectories. |
The best paternal sleep multi-trajectory model was also a 3-group model illustrated in Figure 2B. Similar to maternal trajectories, all trajectories were best explained by a linear or constant shape. Fathers belonging to group F1 (37.2% of fathers, n = 70) had a stable mean NSD of about 8 hr; a short and stable mean weekend DSD (≈1 min), corresponding to a DSD of 37 to 21 min in 4.3% and 2.9% of napping fathers; and a relatively low stable prevalence of SSL (≈33%) between 3 and 36 months postpartum. Fathers belonging to group F2 (18.6%, n = 35) had a stable but relatively short mean NSD of about 7 hr from 3 to 36 months postpartum; a stable mean weekend DSD of about 9 min, corresponding to about 33 min among fathers taking naps (25.7% at 3 months and 17.1% at 36 months postpartum) but with a small peak at 24 months postpartum (up to 14 min for the whole population and 52 min for 22.3% of napping fathers); and very high decreasing prevalence of SSL of 95.4% to 80.4% between 3 and 36 months postpartum. Fathers belonging to group F3 (44.7%, n = 83) had a stable mean NSD of about 8h20; a relatively long and increasing weekend DSD from 33 to 42 min, corresponding to 45 and 49 min for napping fathers (65.1% at 3 months and 75.9% at 36 months); and a stable prevalence of SSL of about 50% from 3 to 36 months postpartum. The group F1, showing the most optimal mean NSD and the lowest prevalence of SSL between 3 and 36 months postpartum, was chosen as the reference group for association analyses.
The best couple sleep multi-trajectory model was a 3-group model illustrated in Figure 2C. All trajectories were best explained by linear or constant shapes except for the NSD maternal trajectory in group C1, which was best explained by a cubic shape. Couples belonging to group C1 (29.2% of couples, n = 55) had a mean maternal NSD decreasing from 9h20 to 8h20 between 3 and 24 months postpartum and a stable paternal NSD at 8h20 and a stable and short mean maternal and paternal weekend DSD of ≈10 min and ≈5 min, respectively. The weekend DSD corresponded to about 45 min for napping mothers (20% of mothers) and 35 to 25 min for napping fathers (20% of fathers at 3 and 36 months, 11% and 16% at 18 and 24 months). In this group of couples, the maternal prevalence of SSL was 58% at 3 months, decreasing to 31% from 18 to 36 months postpartum, and the paternal SSL rate was stable (≈30%). Couples belonging to group C2 (27.6%, n = 52) had a stable mean NSD of 7 to 8 hr for both parents; a decreasing maternal mean weekend DSD from 41 to 23 min between 3 and 18 months, corresponding to 65 and 50 min for napping mothers (53.8% at 3 months and 32.7% at 18 months), then remaining stable (≈55 min for 43% of napping mothers); a stable paternal mean weekend DSD of about 10 min for all fathers and about 40 min for napping fathers (≈25% up to 24 months and 17.3% at 36 months postpartum); and a very high prevalence of SSL for both parents (90% to 86% for mothers and 76% to 61% for fathers). Couples belonging to C3 (43.1%, n = 81) had a mean maternal and paternal NSD of 8 to 9 hr, a mean weekend DSD decreasing from 54 to 41 min between 3 and 36 months postpartum for all mothers from 65 to 57 min in napping mothers (79.0% and 59.3%, respectively) but increasing from 28 to 39 min for all fathers (50 to 53 min for 51.9% to 65.4% of napping fathers), and a stable but relatively high SSL (≈70% for mothers and ≈55% for fathers) between 3 and 36 months postpartum. The group C1, with the most optimal sleep patterns for both mothers and fathers, was chosen as the reference group for association analyses.
Sensitivity analysis using the recalculated NSD according to frequency of child night waking identified similar sleep multi-trajectory groups (number, shape and proportion of individuals per groups) but with lower NSD at 3 and 18 months, especially in the groups with already the shortest NSD (Appendix 1 and 2).
Interrelations Between Maternal, Paternal and Couples’ Sleep Multi-Trajectory Groups
Results from unadjusted and adjusted multinomial regression analyses between maternal and paternal sleep multi-trajectory groups are presented in Table 3. The odds of the father belonging to F3 (long NSD, longest weekend DSD and moderate level of SSL) were decreased with maternal membership in M1 (shortest NSD and weekend DSD, relatively high SSL). No other association was observed between the maternal and paternal sleep multi-trajectory groups.
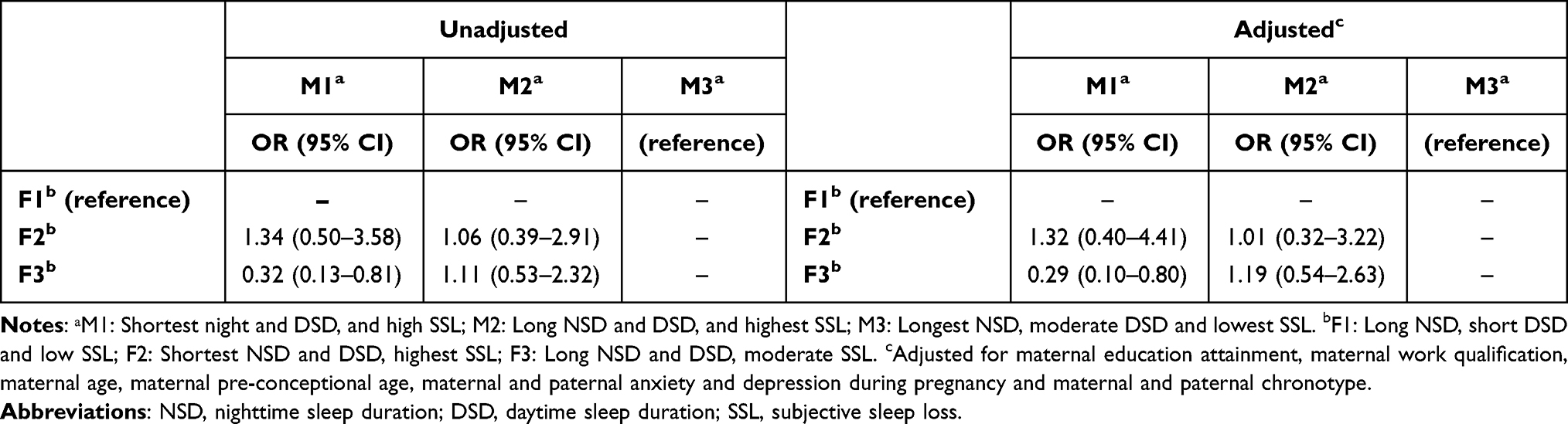 |
Table 3 Interrelations Between Maternal (M1-M3) and Paternal (F1-F3) Sleep Multi-Trajectories (N = 188 Pairs) |
The distribution of each maternal and paternal sleep multi-trajectory groups within couples’ sleep multi-trajectory groups is presented in Table 4. Briefly, fathers in each individual sleep group were more frequently distributed within the corresponding couples’ sleep multi-trajectory groups: 52.9% of fathers belonging to F1, 82.9% to F2 and 75.9% to F3 were distributed within the couples’ multi-trajectory groups C1, C2 and C3, respectively. The distribution of individual mothers’ sleep multi-trajectory groups within couples’ sleep multi-trajectory groups was more diverse. More than half of the mothers belonging to groups M1 (53.7%) and M2 (64%) belonged to groups C2 and C3, respectively, whereas the mothers belonging to group M3 were almost equally distributed between groups C1 (47.0%) and C3 (44.6%).
 |
Table 4 Distribution of Maternal (M1-M3) and Paternal (F1-F3) Sleep Multi-Trajectory Groups According to Couples (C1-C3) Sleep Multi-Trajectory Groups (N = 188) |
Covariates Associated with Couples’ Sleep Multi-Trajectory
Results from unadjusted and adjusted multinomial regression analyses are in Table 5.
 |
Table 5 Unadjusted and Adjusted Multinomial Logistic Regression for Couples Sleep Multi-Trajectory Groups (N = 188; C1 Was the Reference) |
In the adjusted model, the odds of the couple belonging to C2 versus C1 were associated with later paternal chronotype, whereas the odds of belonging to C2 versus C1 were decreased when the child was the first child and was born in autumn. No studied factors differentiated the odds of belonging to C3 versus C1.
The results obtained in the sensitivity analysis, additionally adjusting for maternal weekday nap at 3 months postpartum, were similar. In the sensitivity analysis, the odds of belonging to C2 versus C1 were decreased with having first child. The associations between C2 membership and both later paternal chronotype and having a child born in autumn became borderline significant but with stable effect sizes (Appendix 3).
Discussion
To the best of our knowledge, this is the first study to describe longitudinal patterns of sleep duration identified by multi-trajectories in mothers and fathers during 36 months postpartum and to assess their early correlates. Overall, we identified 3 sleep multi-trajectories among mothers and fathers as individual and in couple, and both maternal and paternal NSD were longer as compared with other populations even among the shortest sleeping groups (M3 and F3). We also identified that paternal chronotype, having their first child and giving birth in autumn are associated with couples’ sleep.
In this study, maternal mean NSD ranged from 8 to 9 hr between 3 and 36 months postpartum, with a decrease between 3 and 18 months postpartum. For instance, US mothers reported a mean NSD from 6h30 to 7h00 between 7 weeks9 and 5 months postpartum.34,35 Canadian mothers reported less than 7h00 of NSD at 2 and 6 months postpartum;19,36,37 while NSD was objectively measured by accelerometry at 7h28 at the same period.37 Breastfeeding Chinese mothers also reported about 7h00 of NSD from 2 to 7 months postpartum, and about 7h30 at 12 to 17 months.38 Mean paternal NSD was stable, about 8 hr, from 3 to 36 months postpartum. It was also longer in our study than in other studies: the mean NSD was 6h11 at 7 weeks postpartum among US fathers9 and about 7h20 by subjective and objective measures among Canadian fathers at 6 months postpartum.39 Both maternal and paternal NSD in our study were also longer than the mean NSD reported in a French general population survey in 2010, reporting 7h30 to 7h15 NSD for women and 7h00 to 6h50 NSD for men between ages 26 and 44 years.40
The long sleep duration of the study population may be due to the subjective sleep measurement based on self-reports that better reflect time in bed than sleep duration. Although most parental sleep studies measured maternal or paternal sleep by sleep diaries19,36 or validated questionnaires,9,10 self-reported sleep based on bedtime and wake-up time is widely used in epidemiological studies of sleep in general populations.37,38 We did not collect data on the frequency and duration of parental night waking, but we considered the frequency of the child’s night waking in a sensitivity analysis showing that parental NSD was low from 3 to 18 months postpartum but remained longer than the parental sleep duration reported in other populations.9,19,38,39 Another explanation for the observed long sleep durations may be the specificity of the study population. The included fathers and mothers had high socioeconomic status, low BMI and long breastfeeding duration, which may reflect families that are more likely to follow healthy lifestyle recommendations,41 including sleep recommendations.
Despite a long NSD, we observed a prevalence of SSL > 50% for mothers and fathers in all groups up to 36 months postpartum, with a higher prevalence of SSL (up to 70%) in mothers from 3 to 18 months postpartum. Although SSL is a measure of subjective lack of sleep quantity, our high prevalence of SSL may be an indicator of poor sleep quality, given the high level of reported NSD in this population. In particular, mean NSD and weekend DSD were longer for mothers than fathers, which is consistent with previous findings,8–11 but maternal SSL was still higher than paternal SSL, which suggests that mothers would experience more sleep disturbances in the postpartum period up to 24 months after birth and is consistent with previous publications.10,11,17,37,42 Thus, higher maternal prevalence of SSL could reflect lighter sleep, modified arousal thresholds or greater maternal involvement in global and night-time care, at least in the early postpartum period.19,43
All maternal, paternal and couple sleep characteristics were classified into 3 distinct multi-trajectory groups with different sleep patterns. Mothers and fathers in the same couple multi-trajectory group exhibited similar sleep patterns. A cross-sectional laboratory study showed that couples sleeping together had more synchronized sleep stages than those sleeping individually,44 which suggests similar sleep characteristics. However, the distribution between individual and couple multi-trajectory groups exhibited larger differences for maternal than paternal sleep multi-trajectory groups, so mothers might be more likely to adapt their sleep to their partner’s sleep or synchronize their sleep with their partner’s. This finding is consistent with the hypothesis reported by a systematic review of 14 studies on co-sleeping couples in general populations.13
We assessed early correlates regarding couples’ sleep evolution. Firstly, fathers with the later chronotype frequently belonged to the couples’ group with the shortest mean NSD and highest SSL for both mothers and fathers. In childless couples, chronotypes (morning–evening preference) have been found correlated within couples,45 and couples with both members of the morning type have better sleep quality and less insomnia symptoms than couples with both members of evening types.46 However, men are known to have later chronotypes than women,13 and the later chronotype is associated with short sleep duration47 as was observed for fathers in C2 (constantly lower NSD between 1h00 and 1h30 than in other couples groups). In addition, couples less frequently belonged to the couples’ group with the shortest mean NSD and highest SSL for both mothers and fathers when their child was a first child and born in autumn. Having multiple children would increase the burden of child care, as previously suggested,19,20 which may lead to a short sleep duration. People tend to sleep longer during the winter season than other seasons48 and infants and toddlers sleep more deeply during the darker seasons.49 Thus, this seasonal effect may translate into better sleep quantity/quality at age 3 months (ie, our first time point in winter) in children born in autumn, which could result in better sleep consolidation and quality up to 36 months of age and thus less disturb parental sleep. This hypothesis should be confirmed by other studies.
This study has several strengths and some limitations. First, the prospective cohort design with repeated follow-up from 3 to 36 months postpartum provided longitudinal data with high accuracy and low memory bias. Second, the cohort included paternal information, thus allowing the study of both individuals and couples sleep changes over time, whereas most previous studies focused on only maternal sleep.50–52 Third, the use of the group-based multi-trajectory modelling29,30 method allowed for longitudinal analysis of maternal, paternal, and couple sleep patterns from 3 to 36 months postpartum by simultaneously accounting for multiple measures of sleep (nighttime, daytime, and perceived sleep deprivation), which allowed for a better characterization of parents’ overall sleep patterns over time. Most previous studies investigating longitudinal analysis of sleep in adults using trajectory modelling reported only one sleep characteristic, mainly total sleep duration.53 Fourth, the group-based multi-trajectory modelling method allowed for including missing data, and we included individuals and their partners with sleep data available for at least 2 of 4 time-point measurements to maximize the study sample size. Nevertheless, this led to the exclusion of approximately 60% of the cohort population. It could have led to population selection bias, but individual sleep characteristics did not differ by study inclusion, which suggests that the impact of the exclusion may be small. Therefore, although the sample size of 188 couples is larger than previous studies of couples’ sleep at a new birth,10,15,19,21 the population size may not be sufficient to capture associations between couples’ sleep and the factors we considered. Nonetheless, we were able to control for several potential factors influencing couples’ sleep multi-trajectory groups, including parental chronotypes, child rank and birth seasonality. Fifth, sleep was subjectively assessed through self-questionnaires. However, to minimize recall bias, questions were asked at each time point on current bedtime and wake-up time during both weekdays and weekend days, as commonly used in epidemiological studies37,38 as well as questions on naps and subjective sleep loss reflecting their own perception of their sleep. Lastly, we only included heterosexual couples. Our results may not be generalizable, especially to same-sex couples and single parents.
Conclusion
Using an original modelling method, this study sheds new light on changes in maternal, paternal and couple sleep between 3 and 36 months postpartum. For each category, we identified 3 different groups of sleep characteristics, including nighttime and daytime sleep duration and subjective sleep loss. Women were more likely to adopt their male partners’ sleep patterns, and so the couples tended to have similar sleep characteristics. Further studies are needed to investigate the longitudinal relations between parental and child sleep patterns in the postpartum period up to toddlerhood to better characterize interrelationship of sleep within families and to develop potential prevention strategies.
Abbreviations
BIC, Bayesian Information Criteria; BMI, Body mass index; CNIL, Commission nationale de l’informatique et des libertés; CPP, Comité de Protection des Personnes Sud-Est V; DSD, Daytime sleep duration; FCS, Fully Conditional Specification; FG, Paternal sleep multi-trajectory group; G, Couple sleep multi-trajectory group; MCTQ, Munich Chronotype Questionnaire; MG, Maternal sleep multi-trajectory group; NSD, Nighttime sleep duration; SEPAGES, Suivi de l’Exposition à la Pollution Atmosphérique durant la Grossesse et Effet sur la Santé; SD, Standard deviation; SSL, Subjective sleep loss; OR: Odds ratio, 95% CI: 95% confidence interval.
Acknowledgments
We thank the SEPAGES study group: E. Eyriey, A. Licinia, A. Vellement (Groupe Hospitalier Mutualiste, Grenoble), S. Bayat, P. Hoffmann, E. Hullo, C. Llerena (Grenoble Alpes University Hospital, La Tronche), X. Morin (Clinique des Cèdres, Echirolles), A. Morlot (Clinique Belledonne, Saint-Martin d’Hères), J. Lepeule, S. Lyon-Caen, C. Philippat, I. Pin, J. Quentin, V. Siroux, R. Slama (Grenoble Alpes University, Inserm, CNRS, IAB).
Many thanks to Dr I. Pin who was the Sepages PI from 2012 until 2022. We thank also Mrs. A. Benlakhryfa, Mrs. L. Borges, Mr. Y. Gioria, clinical research assistants; Mrs. J. Giraud, Mrs. M. Marceau, Mrs. M-P. Martin, nurses; Mrs. E. Charvet, Mrs A. Putod, midwives; Mrs. M. Graca, Mrs. K. Gridel, Mrs. C. Pelini, Mrs M. Barbagallo fieldworkers; Mrs. A. Bossant, K. Guichardet, J-T Iltis A. Levanic, C. Martel, E. Quinteiro, S. Raffin neuropsychologists; the staff from Grenoble Center for Clinical Investigation (CIC): Prof. J.-L. Cracowski, Dr. C. Cracowski, Dr. E. Hodaj, Mrs. D. Abry, Mr. N. Gonnet and Mrs. A. Tournier. A warm thank you also Dr. M. Althuser, Mr. S. Althuser, Dr. F. Camus-Chauvet, Mr. P. Dusonchet, Mrs. S. Dusonchet, Dr. L. Emery, Mrs. P. Fabbrizio, Prof. P. Hoffmann, Dr. D. Marchal André, Dr. X. Morin, Dr. E. Opoix, Dr. L. Pacteau, Dr. P. Rivoire, Mrs. A. Royannais, Dr. C. Tomasella, Dr. T. Tomasella, Dr. D. Tournadre, Mr. P. Viossat, Mrs. E. Volpi, Mrs. S. Rey, Dr. E. Warembourg and clinicians from Grenoble University Hospital for their support in the recruitment of the study volunteers. We also thank Mrs. A. Buchet, Mrs. SF. Caraby, Dr. J-N. Canonica, Mrs. J. Dujourdil, Dr. E. Eyriey, Prof. P. Hoffmann, Mrs. M. Jeannin, Mrs. A. Licina, Dr. X. Morin, Mrs. A. Nicolas, and all midwives from the four maternity wards of Grenoble urban areas. SEPAGES data storage was possible with an Inserm RE-CO-NAI platform funded by Commissariat Général à l’Investissement, with the implication of Sophiede Visme (Inserm DSI). Many thanks to Dr. M.A. Charles, RE-CO-NAI coordinator, for her support. Finally, and importantly, we express our sincere thanks to participants of the SEPAGES study.
Funding
Mihyeon KIM was funded by a doctoral contract with Université de Paris-Cité. The SEPAGES cohort was supported by the European Research Council (N°311765-E-DOHaD), the European Community’s Seventh Framework Programme (FP7/2007-206, no.308333-892 HELIX), the European Union’s Horizon 2020 research and innovation programme (no. 874583 ATHLETE Project, N°825712 OBERON Project), the French Research Agency – ANR (PAPER project ANR-12-PDOC-0029-01, SHALCOH project ANR-14-CE21-0007, ANR-15-IDEX-02 and ANR-15-IDEX5, GUMME project ANR-18-CE36-005, ETAPE project ANR-18-CE36-0005 - EDeN project ANR-19-CE36-0003-01 – MEMORI project ANR 21-CE34-0022), the French Agency for Food, Environmental and Occupational Health & Safety – ANSES (CNAP project EST-2016-121, PENDORE project EST-2016-121, HyPAxE project EST-2019/1/039, PENDALIRE project EST-2022-169), the Plan Cancer (Canc’Air project), the French Cancer Research Foundation Association de Recherche sur le Cancer – ARC, the French Endowment Fund AGIR for chronic diseases – APMC (projects PRENAPAR, LCI-FOT, DysCard), the French Endowment Fund for Respiratory Health, the French Fund – Fondation de France (CLIMATHES – 00081169, SEPAGES 5 – 00099903, ELEMENTUM – 00124527).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chaput JP, Dutil C, Featherstone R, et al. Sleep duration and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S218–S231. doi:10.1139/apnm-2020-0034
2. Watson NF, Badr MS, Belenky G, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep. 2015;38(6):843–844. doi:10.5665/sleep.4716
3. Paine SJ, Gander PH. Explaining ethnic inequities in sleep duration: a cross-sectional survey of māori and non-māori adults in New Zealand. Sleep Health. 2016;2(2):109–115. doi:10.1016/j.sleh.2016.01.005
4. Stamatakis KA, Kaplan GA, Roberts RE. Short sleep duration across income, education, and race/ethnic groups: population prevalence and growing disparities during 34 years of follow-up. Ann Epidemiol. 2007;17(12):948–955. doi:10.1016/j.annepidem.2007.07.096
5. Lee SY, Ju YJ, Lee JE, et al. Factors associated with poor sleep quality in the Korean general population: providing information from the Korean version of the Pittsburgh Sleep Quality Index. J Affect Disord. 2020;271:49–58. doi:10.1016/j.jad.2020.03.069
6. Saalwirth C, Leipold B. Sleep and chronotype in relation to work-related stress and negative affect: the moderating role of a flexible start of work. Somnologie. 2021;25(2):119–125. doi:10.1007/s11818-021-00294-9
7. Coutrot A, Lazar AS, Richards M, et al. Reported sleep duration reveals segmentation of the adult life-course into three phases. Nat Commun. 2022;13(1):7697. doi:10.1038/s41467-022-34624-8
8. Natale V, Adan A, Fabbri M. Season of birth, gender, and social-cultural effects on sleep timing preferences in humans. Sleep. 2009;32(3):423–426. doi:10.1093/sleep/32.3.423
9. Insana SP, Montgomery-Downs HE. Sleep and sleepiness among first-time postpartum parents: a field- and laboratory-based multimethod assessment. Dev Psychobiol. 2013;55(4):361–372. doi:10.1002/dev.21040
10. Cattarius BG, Schlarb AA. How the Sleep of Couples Changes from Pregnancy to Three Months Postpartum. Nat Sci Sleep. 2021;13:251–261. doi:10.2147/NSS.S259072
11. E. Montgomery-Downs H, Stremler R, P. Insana S. Postpartum sleep in new mothers and fathers. Open Sleep J. 2013;6(1):87–97. doi:10.2174/1874620901306010087
12. Fatima Y, Doi SAR, Najman JM, Mamun AA. Exploring gender difference in sleep quality of young adults: findings from a large population study. Clin Med Res. 2016;14(3–4):138–144. doi:10.3121/cmr.2016.1338
13. Richter K, Adam S, Geiss L, Peter L, Niklewski G. Two in a bed: the influence of couple sleeping and chronotypes on relationship and sleep. An overview. Chronobiol Int. 2016;33(10):1464–1472. doi:10.1080/07420528.2016.1220388
14. Gay CL, Lee KA, Lee SY. Sleep patterns and fatigue in new mothers and fathers. Biol Res Nurs. 2004;5(4):311–318. doi:10.1177/1099800403262142
15. Richter D, Krämer MD, Tang NKY, Montgomery-Downs HE, Lemola S. Long-term effects of pregnancy and childbirth on sleep satisfaction and duration of first-time and experienced mothers and fathers. Sleep. 2019;42(4):zsz015. doi:10.1093/sleep/zsz015
16. Hagen EW, Mirer AG, Palta M, Peppard PE. The sleep-time cost of parenting: sleep duration and sleepiness among employed parents in the Wisconsin Sleep Cohort Study. Am J Epidemiol. 2013;177(5):394–401. doi:10.1093/aje/kws246
17. Lollies F, Schnatschmidt M, Schlarb AA, Genuneit J. Child sleep problems affect mothers and fathers differently: how infant and young child sleep affects paternal and maternal sleep quality, emotion regulation, and sleep-related cognitions. Nat Sci Sleep. 2022;14:137–152. doi:10.2147/NSS.S329503
18. Srimoragot M, Hershberger PE, Park C, Hernandez TL, Izci Balserak B. Infant feeding type and maternal sleep during the postpartum period: a systematic review and meta‐analysis. J Sleep Res. 2023;32(2). doi:10.1111/jsr.13625
19. Kenny S, Burdayron R, Lannes É EM, Dubois-Comtois K, Béliveau MJ, Pennestri MH. Mothers’ and fathers’ sleep: is there a difference between first-time and experienced parents of 6-month-olds? J Sleep Res. 2021;30(4):e13238. doi:10.1111/jsr.13238
20. Christian LM, Carroll JE, Porter K, Hall MH. Sleep quality across pregnancy and postpartum: effects of parity and race. Sleep Health. 2019;5(4):327–334. doi:10.1016/j.sleh.2019.03.005
21. Elek SM, Hudson DB, Fleck MO. Couples’ experiences with fatigue during the transition to parenthood. J Fam Nurs. 2002;8(3):221–240. doi:10.1177/107484070200800305
22. Fatima Y, Bucks RS, Mamun AA, et al. Sleep trajectories and mediators of poor sleep: findings from the longitudinal analysis of 41,094 participants of the UK Biobank cohort. Sleep Med. 2020;76:120–127. doi:10.1016/j.sleep.2020.10.020
23. Lyon-Caen S, Siroux V, Lepeule J, et al. Deciphering the impact of early-life exposures to highly variable environmental factors on foetal and child health: design of SEPAGES couple-child cohort. Int J Environ Res Public Health. 2019;16(20):3888. doi:10.3390/ijerph16203888
24. Bocéréan C, Dupret E. A validation study of the hospital anxiety and depression scale (Hads) in a large sample of French employees. BMC Psychiatry. 2014;14:354. doi:10.1186/s12888-014-0354-0
25. Stern AF. The Hospital Anxiety and Depression Scale. Occup Med. 2014;64(5):393–394. doi:10.1093/occmed/kqu024
26. Ghotbi N, Pilz LK, Winnebeck EC, et al. The µMCTQ: an ultra-short version of the Munich Chronotype Questionnaire. J Biol Rhythms. 2020;35(1):98–110. doi:10.1177/0748730419886986
27. Nagin D. Group-Based Modeling of Development. Harvard University Press; 2005. Available from: http://www.jstor.org/stable/j.ctvjf9z1f.
28. Jones BL, Nagin DS. Advances in group-based trajectory modeling and an sas procedure for estimating them. Sociol Methods Res. 2007;35(4):542–571. doi:10.1177/0049124106292364
29. Nagin DS. Group-based trajectory modeling: an overview. Ann Nutr Metab. 2014;65(2–3):205–210. doi:10.1159/000360229
30. Nagin DS, Jones BL, Passos VL, Tremblay RE. Group-based multi-trajectory modeling. Stat Methods Med Res. 2018;27(7):2015–2023. doi:10.1177/0962280216673085
31. Nagin DS, Odgers CL. Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol. 2010;6(1):109–138. doi:10.1146/annurev.clinpsy.121208.131413
32. Tennant PWG, Murray EJ, Arnold KF, et al. Use of directed acyclic graphs (DAGs) to identify confounders in applied health research: review and recommendations. Int J Epidemiol. 2021;50(2):620–632. doi:10.1093/ije/dyaa213
33. Rubin DB. Multiple imputation for nonresponse in surveys. In: Multiple Imputation for Nonresponse in Surveys. John Wiley & Sons, Ltd; 1987.i–xxix. doi:10.1002/9780470316696.fmatter
34. Ronzio CR, Huntley E, Monaghan M. Postpartum mothers’ napping and improved cognitive growth fostering of infants: results from a pilot study. Behav Sleep Med. 2013;11(2):120–132. doi:10.1080/15402002.2011.642487
35. Spaeth AM, Khetarpal R, Yu D, Pien GW, Herring SJ. Determinants of postpartum sleep duration and sleep efficiency in minority women. Sleep. 2020;44(4):zsaa246. doi:10.1093/sleep/zsaa246
36. Creti L, Libman E, Rizzo D, et al. Sleep in the postpartum: characteristics of first-time, healthy mothers. Sleep Disord. 2017;2017:e8520358. doi:10.1155/2017/8520358
37. Kalogeropoulos C, Burdayron R, Laganière C, Dubois-Comtois K, Béliveau MJ, Pennestri MH. Sleep patterns and intraindividual sleep variability in mothers and fathers at 6 months postpartum: a population-based, cross-sectional study. BMJ Open. 2022;12(8):e060558. doi:10.1136/bmjopen-2021-060558
38. Ruan H, Zhang Y, Tang Q, et al. Sleep duration of lactating mothers and its relationship with feeding pattern, milk macronutrients and related serum factors: a combined longitudinal cohort and cross-sectional study. Front Nutr. 2022;9:. doi:10.3389/fnut.2022.973291
39. Kalogeropoulos C, Burdayron R, Laganière C, Béliveau M-J, Dubois-Comtois K, Pennestri M-H. Investigating the link between sleep and postpartum depression in fathers utilizing subjective and objective sleep measures. Sleep Medicine: X. 2021;3:100036. doi:10.1016/j.sleepx.2021.100036
40. Beck F, Richard JB, Léger D. Prévalence et facteurs sociodémographiques associés à l’insomnie et au temps de sommeil en France (15–85 ans). Rev Neurol. 2013;169(12):956–964. doi:10.1016/j.neurol.2013.02.011
41. Logan C, Zittel T, Striebel S, et al. Changing societal and lifestyle factors and breastfeeding patterns over time. Pediatrics. 2016;137(5):e20154473. doi:10.1542/peds.2015-4473
42. Sinai D, Tikotzky L. Infant sleep, parental sleep and parenting stress in families of mothers on maternity leave and in families of working mothers. Infant Behav Dev. 2012;35(2):179–186. doi:10.1016/j.infbeh.2012.01.006
43. Ragni B, De Stasio S. Parental involvement in children’s sleep care and nocturnal awakenings in infants and toddlers. Int J Environ Res Public Health. 2020;17(16):E5808. doi:10.3390/ijerph17165808
44. Drews HJ, Wallot S, Brysch P, et al. Bed-sharing in couples is associated with increased and stabilized rem sleep and sleep-stage synchronization. Front Psychiatry. 2020;11:583. doi:10.3389/fpsyt.2020.00583
45. Randler C, Kretz S. Assortative mating in morningness–eveningness. Int J Psychol. 2011;46(2):91–96. doi:10.1080/00207594.2010.518237
46. Tanyi Z, Mészáros V, Smohai M, et al. Morningness-eveningness, relationship quality, and quality of life among couples living together. Chronobiol Int. 2020;37(12):1736–1747. doi:10.1080/07420528.2020.1802289
47. Allebrandt KV, Teder-Laving M, Kantermann T, et al. Chronotype and sleep duration: the influence of season of assessment. Chronobiol Int. 2014;31(5):731–740. doi:10.3109/07420528.2014.901347
48. Mattingly SM, Grover T, Martinez GJ, et al. The effects of seasons and weather on sleep patterns measured through longitudinal multimodal sensing. Npj Digit Med. 2021;4(1):1–15. doi:10.1038/s41746-021-00435-2
49. Kärki A, Satomaa AL, Huhtala H, et al. Season is related to the slow wave and sigma activity of infants and toddlers. Sleep Med. 2022;100:364–377. doi:10.1016/j.sleep.2022.09.006
50. Srimoragot M, Hershberger PE, Park C, Hernandez TL, Izci Balserak B. Infant feeding type and maternal sleep during the postpartum period: a systematic review and meta-analysis. J Sleep Res. 2024; n/a(n/a):e13625. doi:10.1111/jsr.13625
51. Sivertsen B, Hysing M, Dørheim SK, Eberhard-Gran M. Trajectories of maternal sleep problems before and after childbirth: a longitudinal population-based study. BMC Pregnancy Childbirth. 2015;15(1):129. doi:10.1186/s12884-015-0577-1
52. Mindell JA, Sadeh A, Kwon R, Goh DYT. Relationship Between Child and Maternal Sleep: A Developmental and Cross-Cultural Comparison. J Pediatr Psychol. 2015;40(7):689–696. doi:10.1093/jpepsy/jsv008
53. Wang Y, Hou W, Siddiqi SM, Sun C, Han T, Yang J. Association of sleep trajectory in adulthood with risk of hypertension and its related risk factors: the China health and nutrition survey. J Clin Sleep Med. 2020;16(4):515–521. doi:10.5664/jcsm.8254
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.