Back to Journals » Open Access Journal of Contraception » Volume 15
Women’s Experiences on Injectable Contraceptive Preference Among Jimma Town Public Health Facilities, Southwest Ethiopia 2023. A Phenomenological Study Design
Authors Lemu YK ![]() , Terfa YB
, Terfa YB ![]() , Inkosa LT, Mohammed AA
, Inkosa LT, Mohammed AA ![]() , Yadeta GB, Tulu YT
, Yadeta GB, Tulu YT ![]() , Negari DH, Mamo Y, Mamo A
, Negari DH, Mamo Y, Mamo A ![]()
Received 26 October 2023
Accepted for publication 10 February 2024
Published 19 February 2024 Volume 2024:15 Pages 1—12
DOI https://doi.org/10.2147/OAJC.S443453
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Yohannes Kebede Lemu,1 Yonas Biratu Terfa,2 Lensa Terefe Inkosa,3 Ahmed Andiye Mohammed,1 Geremu Bayissa Yadeta,1 Yidnekachew Tafesse Tulu,1 Desalegn Hundera Negari,1 Yiftusira Mamo,1 Abebe Mamo1
1Department of Health, Behaviour and Society, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia; 2School of Nursing, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia; 3Jimma Medical Center, Jimma, Oromia, Ethiopia
Correspondence: Yonas Biratu Terfa, School of Nursing, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia, Tel +251913826248, Email [email protected]; [email protected]
Background: Contraception is the information, devices, and medications that enable individuals to decide whether and when to have children. It is a cost-effective method of limiting and spacing childbirth. In Ethiopia, the prevalence of modern contraceptives is increasing, and injection contraceptives represent a high prevalence. However, it is unclear why the women preferred injection contraception.
Objective: To explore Women’s experiences on contraceptive preference among Jimma town public health facilities, southwest Ethiopia, 2023.
Methods: An interpretative phenomenological study design was employed. Women aged between 18 and 49 who have been using injectable contraceptives for more than one year were our study population. Data were collected through in-depth interviews using an open-ended, structured interview guide. The purposive sampling technique was used to select 12 participants from three randomly selected public health facilities in Jimma town. Audio data were transcribed verbatim into word files, and finally, Atlas.ti 7.0 software was used to facilitate coding and categorizing.
Results: Twelve women who have been using injectable contraceptives for the last year were involved in this study. Religious beliefs, fear of side effects, visiting Arab countries, and previous contraceptive experiences were the main reasons for respondents to prefer injectable contraceptive methods. This study revealed that women were experiencing positive and negative effects while using injection contraceptives. The majority of the respondents felt comfortable and pleased and had not encountered any health-related issues since beginning to use injection contraceptives.
Conclusion: The key factors influencing respondents’ preference for injection methods of contraception included fear of side effects, religious convictions, travel to Arab nations, and prior contraceptive experiences. The majority of respondents felt at ease and pleased and reported no substantial health difficulties associated with injection contraception, despite a few women reporting minor adverse effects. Therefore, switching to long-acting methods of contraception necessitates increased women’s understanding of contraceptives.
Keywords: contraception, women experiences, contraceptive preference, Ethiopia
Introduction
Family planning is the ability of individuals or couples to anticipate and attain their desired number of children and the spacing and timing of their births. It is accomplished by using contraceptive methods and treating unintentional infertility.1,2 Contraception is the information, devices or medications, and methods that enable individuals to decide whether and when to have children. Modern contraceptive method product or medical procedure that interferes with reproduction from acts of sexual intercourse.1,3
The proportion of women in the reproductive age range who use contraception has consistently risen from 42% in 1990 to 49% in 2019. The prevalence of contraceptive methods varies greatly from country to country; it is extremely high in developed countries, while it is lowest in undeveloped countries particularly in Africa. Among contraceptive users, the vast majority are using modern contraceptive methods. Globally, in 2019, 45% of women of reproductive age were using a modern method of contraception, which represents 91% of all contraceptive users.4–6
The most widely used form of contraception worldwide is female sterilisation, followed by male condoms. In sub-Saharan Africa, however, injectable contraceptives predominate, with a prevalence of 10% among women of reproductive age.6,7 In Ethiopia, over the past 15 years, use of modern contraceptives has rapidly increased, rising from 8% in 2000 to 41% in 2019. The most often used contraceptive methods, according to the Mini EDHS 2019, are injectable (27%), and the largest proportion of contraceptive methods used is short acting contraceptive methods.8
Many women prefer injectable contraceptives since they are highly effective and do not need to be used every day like oral contraceptives or during sexual activity like barrier methods. Additionally, an injection is preferred over other methods since it may be used secretly from family and friends and can be utilized by lactating women.9,10
Counseling should consider women’s expectations and tolerance for side effects to ensure satisfaction with contraceptive methods. Promoting contraception and providing access to preferred methods is crucial to protect women’s autonomy and well-being, as their preferences are influenced by sociocultural norms and personal experiences.9,11,12
Contraceptive use is often discouraged due to geographic, financial, health, cultural, and religious factors, as well as a lack of contraceptive services and scientific limitations, leading to unintended pregnancies.13,14 Modern contraceptive use is increasing globally, but only 18% of women in sub-Saharan Africa use them, with injectable contraceptives being the most popular. Ethiopia’s prevalence is relatively good, but injectable contraceptives are highly prevalent due to factors influencing preferences.6,8,15
Worldwide, women’s choice of contraceptive method is a sensitive decision that is influenced by many factors such as contraceptive characteristics, women’s reproductive history and previous experiences of using contraception. Furthermore, social aspects and norms such as partner’s support, family member’s expectations, reported experiences among friends and in social media affect women’s contraceptive preferences.16–19
Women of reproductive age go through personal, familial, and social experiences that can either positively or negatively affect their needs and preferences for contraception. Positive experiences include the relative cost of injectable forms, the perception that implants do not have any adverse effects, and proven efficacy and duration of action of the modern method used. Negative experiences included weight gain, pill compliance, infertility worry, irregular bleeding patterns, headaches, and negative effects on mood and sexual desire.20–22
Women’s expectations and side effects can impact their satisfaction with contraceptive methods. Adverse effects are linked to unmet contraceptive needs in developing countries. In Ethiopia, injectable contraceptives dominate preferences. Counselors must understand clients’ expectations and tolerance for adverse effects to ensure regular contraceptive use.23–25 Women’s misconceptions about long-acting contraceptives, based on safety concerns, intolerance of menstrual side effects, and social or moral objections, often lead to a lack of use, such as implant contraception not suitable for daily labor, and discomfort during sex.26,27
Variables like health services, insurance coverage, patient knowledge, and communication influence contraceptive use. Patient preferences vary, with some preferring self-determination and others seeking professional help. Counseling is crucial for couples to use suitable contraceptive methods and prevent unintended pregnancies.28,29
Despite the fact that contraception is inexpensive, readily accessible, and simple to use for all sexually active women.6,30 Contraception is not as often used by couples in Ethiopia as one may have thought, even though a variety of long- and short-term techniques are readily available. The use of injectable contraceptives, which accounts for a sizeable share of contraceptive techniques in the nation’s health care system, is one noteworthy exception, though. This pattern emphasizes how critical it is to comprehend the variables influencing adoption and preferences for contraception in Ethiopia. The low use of contraceptives may be caused by a number of circumstances. Nonetheless, the use of injectable contraceptives can point to certain benefits that suit Ethiopian couples’ requirements and preferences. In our context, however, it is unclear why women favored injectable contraception. Thus, the aim of this study is to explore the women experiences about contraceptive preferences.
Methods and Materials
Study Area and Period
The study was conducted in Jimma town, Oromia regional state, south-west Ethiopia. Jimma town is located 352 km southwest of Addis Ababa. It had a total population of 241,372 in 2015 E.C. currently, the town is administered by a municipality with three sub-cities, 13 town kebeles, and 4 rural kebeles. The town has a total of 128 health institutions (one referral hospital, one governmental and one private hospital, 4 governmental health centers, 55 private clinics, 25 pharmacies, 36 drug stores, and 5 drug distributors) that provide health services in Jimma City. The study was conducted at Shenen Gibe Hospital, Bachobore Health Center, and Mandara Health Center, which were selected purposefully from August 21–September 8, 2023.
Study Design
A phenomenological study design was employed to explore the women’s lived experiences and reasons regarding contraceptive preference. The study focuses on the contraceptive preference use and on the factors that influence their choices. It was used to elaborate the reasons why women choose injectable contraceptives, to explore the lived experience of women who utilized injectable contraceptive methods for more than one year.
Population
All women of reproductive age group who visited the selected health facilities during data collection period for contraceptive services. Women who have been on injectable contraceptive methods for a minimum of one year, permanent residence of Jimma town for minimum of six months, and educational status (different educational status) were interviewed for their lived experience to get inclusive information.
Sample Size Determination and Sampling Procedure
A purposive sampling technique was employed to select participants for in-depth interview. A total of 12 women of reproductive age group, who have been using the injectable contraceptive for minimum of one year, were selected for in-depth interview. Four reproductive age group women were selected purposively from each three health centers based on their educational, religious, age and year of contraceptive use background. A semi-structured interview guide was developed for the interview, and the participants were encouraged to speak up about their experiences. This deepened discussions and reflection on the life experiences of the women.
Data Collection Methods
Data were gathered through In-Depth Interviews (IDI), which employed an interview guide that was written in English and translated into the local languages of Amharic and Afaan Oromo. The research team conducted interviews with a total of 12 women at health facilities. In order to continue the interview and record it on paper and audio tape, a consent form was read, and consents were received. Each interviewee was encouraged to share her life story in detail without any hesitation.
Data Management and Analysis
The interview was recorded, and note takers noticed key information. Audio data was transcribed verbatim into word files and translated to English. Before the analysis, the team members were read each document several times to be familiar with the data, then imported into Atlas.ti 7.0 software to facilitate coding and categorizing. Then, the various codes were compared based on differences and similarities and sorted into categories. Finally, based on content analysis, the underlying meaning that which is the latent content of the text was formulated under each of the categories. The findings encompass direct quotes of women and were narrated without editing the grammar to avoid loss of its meaning. A quote that best described the categories and frequently mentioned ideas was chosen from several groups. Summarized reports were presented to the study participants about the conclusions derived from their shared experiences. Discussions were held with participants about the study guide questions and core concepts of the study. Participant feedback was then considered alongside the experiences of the researcher.
Results
Respondents Back Ground Information
Twelve women who have used injectable contraceptives participated in an in-depth interview for this study. Interviews were approximately 20–45 minutes in duration. The participants were between the ages of 19 and 22. The majority of the study participants had completed secondary school or higher in terms of their educational status. All of the participants were married, and six of the participants were Muslims. Fifty percent of women were housewives in terms of occupation. Injectable contraceptives have been used by more than half of the participants for longer than three years (Table 1).
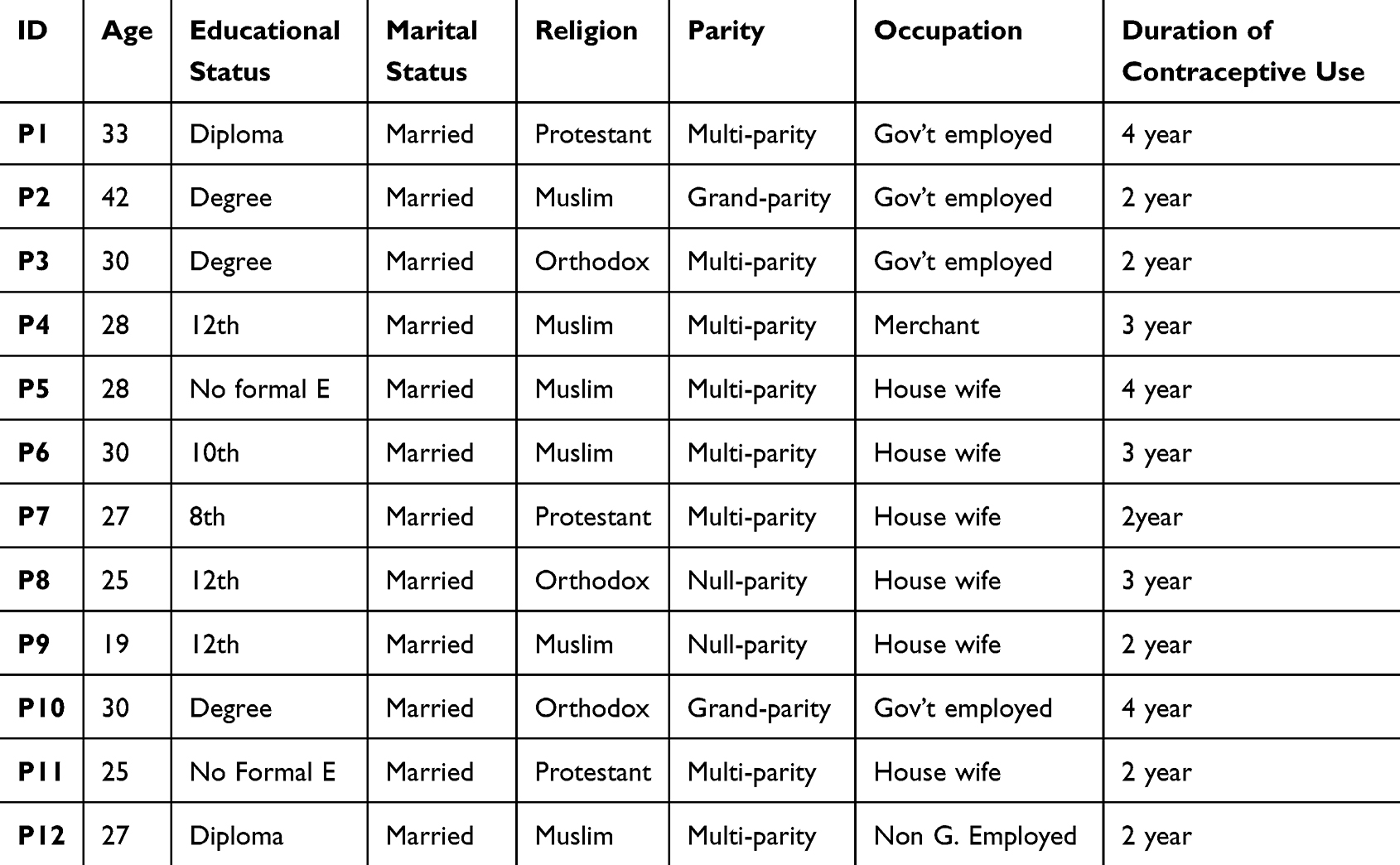 |
Table 1 Background Characteristics of the Study Participants, Jimma Town, Southwest Ethiopia, 2023 (n = 12) |
In this current study, we have identified six themes and 20 subthemes or categories regarding women’s lived experiences regarding injectable contraceptives and their overall contraceptive knowledge. The themes extracted were women’s contraceptive knowledge, contraceptive provision, participants’ contraceptive preference, contraceptive experience, and barriers to using contraceptives. The themes and subthemes are shown as follows (Table 2).
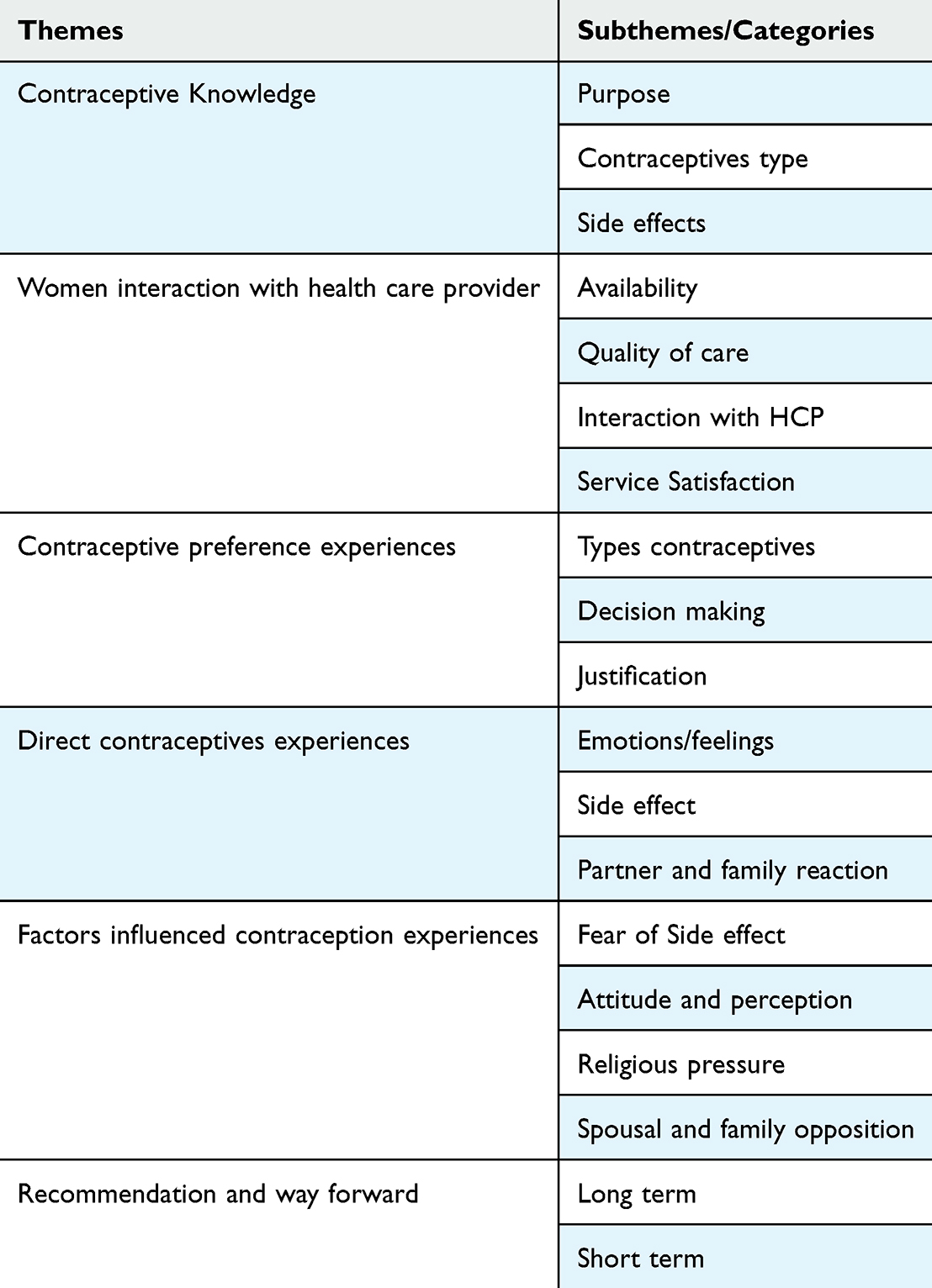 |
Table 2 The Themes and Categories Emerged for Women Use Injectable Contraceptives at Jimma Town Public Health Facilities, South West, Ethiopia, 2023 |
Respondents Contraceptive Knowledge
The ability of individuals to determine their family size and the timing and spacing of their children has resulted in significant improvements in health and social and economic well-being. This study revealed that the majority of interviewed participants explained that family planning is intended to determine the number and spacing of one’s children by using effective methods of birth control.
For example, one IDI participant among family planning users said:
Family planning benefits Women to profit economically and have better wellbeing and health when they space out their children. (P10, 30 years old women)
There was no discernible knowledge gap between the interviewees regardless of general concepts of contraceptives and most of them are relatively aware of the methods they are using.
…I prefer and using injection b/c it has low side effects, I used for many times but only faced absence of menus’ and I don’t know the rest one. (P8, 25 years old women)
Regarding side effects, majority of respondents reported the following side effects; changes in bleeding patterns, including lighter bleeding and fewer days of bleeding, infrequent bleeding, irregular bleeding, no monthly bleeding, prolonged bleeding, back pain and headache.
…As my experience many women has been reported me that as they developed excessive bleeding, back pain and headache after they used implanon. (P10, 30 years old women)
…which one who inserted to arm causes menstruation irregularity, and they advise me as I take Iron, foods rich in vitamin but no change. Thus way I used or prefer injectable one by removing it. (P7, 27 years old women)
Women Interaction with Health Care Provider
Based on the findings, the most important categories under the contraceptive service provision theme are availability of contraceptives, quality of care, interaction with health care providers, and service satisfaction.
Availability of Contraception
Majority of the respondents were reported the availability of all contraceptive methods in the health facility except sometimes there were the shortage of depo-provera.
The respondents were mentioned their feelings as follows:
…It’s good so far, but sometimes there is a chance that the Depo, I’m using now, disappears, and when such cases occur, there are situations where I use it outside of this health center. (P5, 28 years old women)
I follow at this Health facility, so the medications are available and the health workers are given for us with a good condition so I’m agree with their service.̎ (P11, 25 years women)
Regarding interaction with health care provider, in this study, we tried to identify the interaction of health care provider with their injectable contraceptive users, in which most of the users witness that the health professionals treat them respectfully.
Their welcoming and approach is good therefore I can use the injection at any time…they serve us in a respectful manner. (P11, 25 years women)
However, some of the women’s who participate in this study have complain on the health care provider interaction with the clients, in relation to informed choice and improper handling.
For example, one respondent were expressed her feeling according to this
Health center refused me to remove an implanon after I have explained her why I wanted to remove however she was not interested to remove it and sent me to hospital and when I arrived hospital, the hospital staffs were also not accepted me. (P4, 28 years old women)
They treat us well overall, however some of them arrive from home angry and cause trouble when they meet with you. Otherwise, they are quite lovely. (P5, 28 years old women)
Contraceptive Preference
Women’s are preferred different types of contraceptives based on their educational background, experience and awareness. In this study, all of the participants were expressed their contraceptive preferences; therefore, based on their preferences, we have identified three major categories which are types of contraceptives (long and short acting contraceptive methods), decision-making power and justifications for their preferences.
Types of Contraceptives Preferred
Short acting contraceptives are the most preferred contraceptives; particularly, injectable contraceptives were preferred by ten respondents, and one respondent was preferred pills among twelve respondents. However, one respondent was implanon among long-acting family planning, though she has using injectable.
I preferred injection because I become torment if I have used other methods. Therefore, injectable is best and preferable for me because three months are very short to remember and it has minimal side effects. (P11, 25 years old women)
…I preferred short term contraceptive methods than long contraceptive methods. Because, long term family planning particularly implant dies with me if I die. (P10, 30 years old women)
I prefer the injectable (Depo); I have only used it so far and it has never caused me any Problems. (P06, 30 years old women)
I preferred injection because I have accepted as a good and also it is comfortable to my bodies. (P02, 42 years old women)
Though they have been using injectable contraceptives for the last one year, some women’s were expressed their preference as pills specially when they have plan to give birth and Implanon if they have no short-term plan to have children.
…I preferred a short term contraceptives particularly pills, therefore pills is most preferable for me and I have used Injectable if pills are not available because I have plan to have a pregnancy. (P12, 27 years old women)
I prefer implanon which used for 3 years, because when I need to get a child there is no delay however injectable can delay you giving birth. (P08, 25 years old women)
…I have preferred short term contraceptive methods particularly injection, but if there is no injection/dipo, I usually use the three-year/implanon contraceptives. (P10, 30 years old women)
Justification
The respondents gave a variety of reasoning for why they preferred injectable contraception over other short-term options and long-acting contraceptive methods, with the majority of the women citing their religious beliefs, fear about side effects and the challenges of visiting Arab countries.
Related to religious beliefs, the women raised the following issues.
… I believe that injection is a water and does not stay in my body for long period of time but implants are living with me for a long period of time so this is sin and It is seen as an abomination in the eyes of Rabbi. (P10, 30 years old women)
…For example if you inserted a contraceptives used for 3 or 5years in your arm, it is not allowable to pray for you if it is found in your body in case you die. (P09, 19 years old women)
…according to my religion (Muslims) view it is not recommended to use it, because it is considered as a sinful to place a foreign thing in one’s arms and then perish. (P02, 42 years old women)
Regarding fear of side effects, the respondents were preferred injectable contraceptives due to side effects related to long-acting contraceptives as below.
…because long term contraceptives are related with excessive bleeding and infertility. Thus is why I preferred injection. (P10, 30 years old women)
I preferred dipo/injection because, If you take a Depo, you can stay for three months without pregnancy fear and no need of daily taking of medicines and additionally some women have been used injection without knowledge of their husband because depo has not visible outside body, however if you choose pills you are worry always. (P03, 30 years old women)
Lastly, one respondent was mentioned that as it is impossible to go abroad particularly Arab countries with Implant due to medical check-up.
…I have a plan to go abroad if I will get a chance …Because a foreign countries/Arab country does not need a person who had Implant contraceptives…it is impossible to go abroad by having implant because it is seen during medical check-up. Therefore, if such like is found in your body, you are not allowed to go there. …additionally it is not suitable to work hard activities. (P11, 25 years old women)
Decision Making
Most of the respondents were decide their preferred contraceptives without husband and health care pressure; however, there are still HCP pressure and spousal opposition to use contraceptives as they need. However, the women may have been made with little knowledge.
Health care providers have given me a chance to decide the methods I want to use. (P12, 27 years old women)
I have decided by myself, so, it is my mandate to decide how many children are enough for me and how I can follow get it. (P9, 19 years old women)
Husband, he decide how many child is enough for us. (P8, 25 years old women)
…I decided by discuss with my husband, personally I recommend to leave the decision for women because the mother had a lot of responsibility and burdens. (P04, 28 years old women)
Health professionals advise me to take Implanon. But I didn’t try Implanon, because Depo is comfortable for me. (P06, 30 years old women)
Respondents Lived Experience of Injectable Contraceptive
Emotional Experiences/Perceives
Respondents/women have various experiences concerning the use of contraceptive methods, particularly Depo-Provera. Most women said that as they are comfortable and have no health related problems after starting to use Injection contraceptive. However, some women reported minimal side effects and one woman reported that she is not feeling good to use it.
Most of the respondents were feeling happy to use the injectable contraceptives, so they mentioned their feeling as follows.
I have been using injection contraceptive for a long time even when I was abroad I used injection because I worked hard. Therefore it is adapted with my body. (P11, 25 years old women)
I am enjoying it because I can’t see any menstrual bleed during the course of this injectable contraceptive. (P08, 25 years old women)
For the last two years I have using injectable contraceptives and it is fine for me, and I have been shifted to injectable from Jadele due to its side effects specifically excessive bleeding… even health center refused me to remove Jadele, however I removed at private clinic by money. (P07, 25 years old women)
Some of the respondents were expressed their experiences as stated below.
I have not been hurt, but sometimes once my period comes it doesn’t stop. I came to this health center and they gave me some pills, and when I took it, it gets better, unless, there is no other problem. (P05, 28 years old women)
I’m still using injectable contraceptives so that I’m comfortable with it…because I have adapted that my menstruation lasts long than usual, so I accept it as a normal behavior, but I don’t have any problems. There are things like: if I take the injection while on my period, the period will disappear, it will dry up. That’s how I feel and there are things like that but I don’t have health problems (P04, 28 years old women)
One respondent said explained that she was heard different negative rumors on the injection contraceptives; however, she reported that she had not faced any challenges.
I prefer injection. I have heard rumors that it has the ability to stay inside your body and causing infertility, but it hasn’t caused any harm to my health. I am happy and feel free and comfortable to use it. (P04, 28 years old women)
Side Effects Experience
Most of the women are not face heavy side effects; however, they have experiencing expected minimal side effects and they have seen that side effects as normal.
The respondents were express their Side effects experience as a below.
My menstrual cycle does not come monthly and it comes once in three to five months even sometimes it may come at seven months but other contraceptive users may see their menstruation monthly. (P11, 25 years old women)
Sometimes I have experienced headache but it disappear when I take diclofenac. So, it is impossible to say there is no headache. (P11, 25 years old women)
I have no any side effect but I can’t see any period or menses cycle during the course of this injectable family planning. (P9, 19 years old women)
…I don’t have anything to say about side effects, but I think it’s due to the nature of the Depo my menstruation lasts long than usual (P04, 28 years old women)
Partner, Family Reaction, and HCP Reaction Experiences
The women were experienced different reactions from their partner, family member and health care providers while using injectable contraceptives. Therefore, they expressed their feelings as follows;
One respondent reported as her husband support her.
Actually he knows as I have using contraceptives and also he support me to use it because he wants to avoid problems and unwanted pregnancies that may happen on me. So, I don’t use it in secret so my husband knows it. So, it is not a secret. (P11, 25 years old women)
Other respondents were raised an issues related to family and neighbors.
…the family doesn’t want you to take medication, but they do want you to have children every couple of years. (P11, 25 years old women)
…local communities and families don’t want you to use it, because they say you have grown up as much as God has given you, so they did not recommend you to go and use it. (P11, 25 years old women)
One participant was mentioned the pressure of health care providers to switch to long-acting contraceptive methods
Sometimes there is a pressure from the Health care provider side because they are enforce you to use long acting contraceptive methods. (P04, 28 years old women)
Factors Influenced Contraception Experiences
How Women Perceived the Community Perception
In this current study, the respondents were expressed the community's perception for being used the injectable contraceptives as it is not good because there are misconceptions in the mind of the community.
For example, one respondent said that.
…You will lose your ability to conceive if you use injectable contraceptives…and also it destroys the race. (P5, 28 years old women)
…It is not good to use it…because you have grew up as much as God has given you…therefore, the family don’t send anyone from their heart to use it, but they say go and use it and ask forgiveness from Allah (Rabbii kee toobbadhu (P11, 25 years old women)
Religious Pressure
The present study revealed that the presences of different religious related teaching which has directly or indirectly affecting the experiences of women.
Some of the Muslim follower women mentioned as the Muslim religion have not recommended the utilization of contraceptives. The below are some of their responses.
… It is not advisable; God orders all things by himself. (P7, IDI, 27 years old women)
In the other aspect, some participants replied that praying to their God also a key solution for managing family size and also used as a solution for contraception.
…it is not advisable, they believe praying to ‘Rabbi’ or God he orders children b/c he know every things (P9, 19 years old women)
However, the Orthodox and protestant religion followers strongly support the contraceptive utilization, and they have not faced any negative experiences related to their religious dogma.
… It is advantageous to your economy and wellness. It has no problem as my religion and I am not faced any challenges (P1, 33 years old women)
Participant Suggestion and Contraceptive Methods Recommendation
The women who participated in this study provide various recommendations and suggestions on the usage of contraception. Due to their lack of familiarity with other contraceptive methods and their concern over the potential side effects of long-term contraception, the majority of the respondents support the use of injectable contraceptives.
One participant has been recommended this:
I am using injectable contraceptives, so, as to me I recommend Injection …I fear of Implanon, thus why I recommend injection because I want to go and work hard activities. So, implanon is not suitable with hard work (P11, 25 years old women)
Some of the study participants feel that community awareness-building is necessary if long-term methods of contraception are to become prominent in the future.
The best course of action is to implement long-term family planning that is backed by education. They are in jeopardy because the majority of user lacks education…the relevant leadership and religious leaders should work on a long-term preventative strategy. (P1, 33 years old women)
Discussion
Family planning is the ability of individuals or couples to anticipate and attain their desired number of children and the spacing and timing of their births. It is a procedure that typically entails a conversation between a woman, a man, and a qualified service provider, and it is carried out with the aid of contraceptive methods. The current findings revealed that the majority of the respondents explained that family planning is the way to determine the number and spacing of one’s children by using effective methods of birth control, which is almost close to the WHO definition of family planning.31
This study found that there were relatively few misunderstandings regarding contraceptive types, side effects, and importance because some of the respondent’s concepts were not based on scientific merit and blind judgment, especially on long-acting contraceptive methods. This result is consistent with research from Arba Minch,32 Wolaita Sodo,33 and the South Gondar zone,34 which found that most respondents were unaware of all contraceptive methods, including their benefits and drawbacks. This similarity may occur due to similarities in socioeconomic background and cultural norms. This may reflect that Ethiopian women’s knowledge of contraception and health literacy is generally similar, suggesting the need for additional intervention.
The distribution of contraceptive preferences differs globally with respect to the use of contraception. The results of the current study indicated that among both short-acting and long-acting contraceptive methods, injectable contraception is the most popular. This result is comparable to studies done in Ghana10 that found that the majority of respondents preferred and were satisfied with the injection method, and it is also supported by a multilevel analysis study done in SSA,15 which revealed that the only preferred contraceptive in SSA is an injectable.
However, the current findings are contrary to studies conducted in Guinea,25 Ghana,26 in which implants and injectables are the most preferred contraceptives, Turkey,35 and Nigeria,36 where it was found that withdrawal and condoms were the most preferred contraceptives by women. These differences can be attributed to differences in study participant backgrounds and the setting of the study, and contraceptives may not get equal attention across the country’s health care system.
Contraceptive preference is influenced by different factors. The present study revealed that contraceptive choices are affected by religious pressure, fear of side effects, cultural norms, partner opposition, previous experiences of using contraception, and family and social context. This finding is in line with studies conducted in Kenya,9 Nigeria,18 Ghana,19 and Southeast Nigeria.23 This similarity shows that African countries’ perceptions of the adverse effects of modern contraceptives have not improved and that there are still considerable religious restrictions and socio-cultural background effects.
Concerning women’s experiences with injectable contraceptives, women’s experiences can be positive or negative depending on their preferences for contraception and can involve a variety of factors, including side effects, partner and family pressure, emotional and physical adaptation, and side effects. The current study’s findings regarding positive experiences revealed that nearly all the women included in the study said that they felt comfortable, pleased and had not encountered any health-related issues since beginning to use injection contraceptives. This study is comparable to one done in Guinea.24 However, regarding negative experiences, the current study reveals that some women had their families in unstable situations as a result of their husbands’ disapproval, irregular menstruation, and lack of faith in their own religion. This study is comparable to studies done in Ghana37 and Guinea24 that show that sexual activity is interrupted and less effective.
Conclusion
Fear of side effects, religious beliefs, visiting Arab countries, and previous contraceptive experiences were the main reasons for respondents to prefer injectable contraceptive methods. Although some women reported minor side effects, the majority of the respondents felt comfortable and happy and had no significant health-related issues related to injection contraceptives. Therefore, it requires higher women’s awareness of contraceptives in order to shift to long-acting contraceptive methods.
Ethics Approval and Informed Consent
Ethical clearance or supportive letter was obtained from the Jimma University after review a proposal. It adhered to the basics of the Declaration of Helsinki. Informed consent was obtained from each study subject. To maintain the confidentiality and anonymity of the participants’ code, labels of participants were used. The study participants also agreed to publish their anonymized responses in scientific journals. Participants aged under 18 years were not included in this study.
Acknowledgments
We would like to express our great appreciation to Jimma University, department of health, Behavior and Society for giving this project. Secondly, our appreciation extends to the individuals and scholars for their backing us during this research and last but not least we thank the study participants for their cooperation in giving necessary information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding received.
Disclosure
The authors of the study confirmed that there is no conflict of interest in this paper.
References
1. Health WHOR. Medical Eligibility Criteria for Contraceptive Use. World Health Organization; 2010.
2. Kesetebirhan A. National Guideline for Family Planning Services in Ethiopia, e Federal Democratic Republic of Ethiopia. Addis Ababa: Ministry of Health; 2011.
3. Hubacher D, Trussell J. A definition of modern contraceptive methods. Contraception. 2015;92(5):420–421. doi:10.1016/j.contraception.2015.08.008
4. Ricci S. Essentials of Maternity, Newborn, and Women’s Health. Lippincott Williams & Wilkins; 2020.
5. Almalik M, Mosleh S, Almasarweh I. Are users of modern and traditional contraceptive methods in Jordan different. East Mediterr Health J. 2018;24(4):377–384. doi:10.26719/2018.24.4.377
6. Economic UNDo, PD SA. World Fertility and Family Planning 2020: Highlights (ST/ESA/SER. A/440). World Fertility and Family Planning 2020: Highlights; 2020.
7. Desa U. United Nations Department of Economic and Social Affairs. Population Division World Population Prospects; 2019.
8. EPHI I. Ethiopian Public Health Institute (EPHI)[Ethiopia] and ICF. Ethiopia Mini Demographic and Health Survey; 2019.
9. Ochako R, Mbondo M, Aloo S, et al. Barriers to modern contraceptive methods uptake among young women in Kenya: a qualitative study. BMC Public Health. 2015;15(1):1–9. doi:10.1186/s12889-015-1483-1
10. Laryea DO, Ankobeah F, Morhe ES, Amoako YA, Spangenberg K. Characteristics and contributory factors for injectable contraceptive usage among women in Kumasi, Ghana. Contracept Reprod Med. 2016;1(1):1–8. doi:10.1186/s40834-016-0019-0
11. Bradley SE, Schwandt H, Khan S. Levels, trends, and reasons for contraceptive discontinuation. DHS Anal Stud. 2009;20:1.
12. World Health Organization DoRHaR. Contraception, evidence brief; 2019.
13. Moreira LR, Ewerling F, Barros AJ, Silveira MF. Reasons for nonuse of contraceptive methods by women with demand for contraception not satisfied: an assessment of low and middle-income countries using demographic and health surveys. Reproductive Health. 2019;16(1):1–15. doi:10.1186/s12978-019-0805-7
14. Machiyama K, Casterline JB, Mumah JN, et al. Reasons for unmet need for family planning, with attention to the measurement of fertility preferences: protocol for a multi-site cohort study. Reproductive Health. 2017;14(1):1–11. doi:10.1186/s12978-016-0268-z
15. Tesema ZT, Tesema GA, Boke MM, Akalu TY. Determinants of modern contraceptive utilization among married women in sub-Saharan Africa: multilevel analysis using recent demographic and health survey. BMC Women's Health. 2022;22(1):181. doi:10.1186/s12905-022-01769-z
16. Sedgh G, Ashford LS, Hussain R. Unmet need for contraception in developing countries: examining women’s reasons for not using a method; 2016.
17. Islam AZ, Mondal MNI, Khatun ML, et al. Prevalence and determinants of contraceptive use among employed and unemployed women in Bangladesh. Int J MCH AIDS. 2016;5(2):92. doi:10.21106/ijma.83
18. Egede JO, Onoh RC, Umeora OUJ, Iyoke CA, Dimejesi IBO, Lawani LO. Contraceptive prevalence and preference in a cohort of south–east Nigerian women. Patient Preference Adherence. 2015;9:707–714. doi:10.2147/PPA.S72952
19. Achana FS, Bawah AA, Jackson EF, et al. Spatial and socio-demographic determinants of contraceptive use in the Upper East region of Ghana. Reprod Health. 2015;12(1):1–10. doi:10.1186/s12978-015-0017-8
20. World Health Organization. WHO Guidelines on Preventing Early Pregnancy and Poor Reproductive Health Outcomes Among Adolescents in Developing Countries. World Health Organization; 2011.
21. Michaels-Igbokwe C, Terris-Prestholt F, Lagarde M, Chipeta E, Initiative I, Cairns J. Young people’s preferences for family planning service providers in rural Malawi: a discrete choice experiment. PLoS One. 2015;10(12):e0143287. doi:10.1371/journal.pone.0143287
22. Biddlecom AE, Singh S, Munthali A. Adolescents’ views of and preferences for sexual and reproductive health services in Burkina Faso, Ghana, Malawi and Uganda. Afr J Reproduct Health. 2007;11(3):99–110. doi:10.2307/25549734
23. Ezenwaka U, Mbachu C, Ezumah N, et al. Exploring factors constraining utilization of contraceptive services among adolescents in Southeast Nigeria: an application of the socio-ecological model. BMC Public Health. 2020;20:1–11. doi:10.1186/s12889-020-09276-2
24. Bangoura C, Dioubaté N, Manet H, et al. Experiences, preferences, and needs of adolescents and urban youth in contraceptive use in Conakry, 2019, Guinea. Front Glob Women’s Health. 2021;2:655920. doi:10.3389/fgwh.2021.655920
25. Rominski SD, Morhe ES, Maya E, Manu A, Dalton VK. Comparing women’s contraceptive preferences with their choices in 5 urban family planning clinics in Ghana. Global Health. 2017;5(1):65–74. doi:10.9745/GHSP-D-16-00281
26. Oddsson K, Leifels-Fischer B, de Melo NR, et al. Efficacy and safety of a contraceptive vaginal ring (NuvaRing) compared with a combined oral contraceptive: a 1-year randomized trial. Contraception. 2005;71(3):176–182. doi:10.1016/j.contraception.2004.09.001
27. Lessard LN, Karasek D, Ma S, et al. Contraceptive features preferred by women at high risk of unintended pregnancy. Perspect Sex Reprod Health. 2012;44(3):194–200. doi:10.1363/4419412
28. Murray E, Pollack L, White M, Lo B. Clinical decision-making: patients’ preferences and experiences. Patient Educ Couns. 2007;65(2):189–196. doi:10.1016/j.pec.2006.07.007
29. Dehlendorf C, Levy K, Kelley A, Grumbach K, Steinauer J. Women’s preferences for contraceptive counseling and decision making. Contraception. 2013;88(2):250–256. doi:10.1016/j.contraception.2012.10.012
30. Hailu D, Gulte T. Determinants of short interbirth interval among reproductive age mothers in Arba Minch District, Ethiopia. Int J Reprod Med. 2016;2016:1–17. doi:10.1155/2016/6072437
31. World Health Organization, eHealth WHOGOf. Building Foundations for eHealth: Progress of Member States: Report of the WHO Global Observatory for eHealth. World Health Organization; 2006.
32. Utaile MM, Debere MK, Nida ET, Boneya DJ, Ergano AT. A qualitative study on reasons for early removal of Implanon among users in Arba Minch town, Gamo Goffa zone, South Ethiopia: a phenomenological approach. BMC Women’s Health. 2020;20(1):1–7. doi:10.1186/s12905-019-0876-1
33. Obsa MS, Takiso KT, Ayele TT, et al. Lived experience of women who underwent early removal of long-acting family planning methods in Bedesa Town, Wolaita Zone, Southern Ethiopia: a Phenomenological Study. Int J Women’s Health. 2021;Volume 13:645–652. doi:10.2147/IJWH.S307142
34. Weldegerima B, Denekew A. Women’s knowledge, preferences, and practices of modern contraceptive methods in Woreta, Ethiopia. Res Social Administrative Pharm. 2008;4(3):302–307. doi:10.1016/j.sapharm.2007.10.001
35. Zehra K, Şahin NH, Demirci FN. 18–49 yaş arası evli kadınların kontraseptif yöntem kullanma tercihleri ve bırnleri [Preference of contraceptives of married women between 18-49 and causes of discontinuation]. Ordu Üniversitesi Hemsirelik Çalismalari Dergisi. 2021;4(1):29–38. Turkish. doi:10.38108/ouhcd.851213
36. Claringbold L, Sanci L, Temple-Smith M. Factors influencing young women’s contraceptive choices. Aust J Gen Pract. 2019;18(20):21–22.
37. Agyei-Baffour P, Boahemaa MY, Addy EA. Contraceptive preferences and use among auto artisanal workers in the informal sector of Kumasi, Ghana: a discrete choice experiment. Reproductive Health. 2015;12(1):1–11. doi:10.1186/s12978-015-0022-y
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.