Back to Journals » Journal of Pain Research » Volume 13
Women’s Perspectives On Provider Education Regarding Opioid Use
Authors Kalinowski J, Wallace BC ![]() , Williams NJ, Spruill TM
, Williams NJ, Spruill TM
Received 16 May 2019
Accepted for publication 1 November 2019
Published 9 January 2020 Volume 2020:13 Pages 39—47
DOI https://doi.org/10.2147/JPR.S215943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Jolaade Kalinowski,1 Barbara C Wallace,2 Natasha J Williams,1 Tanya M Spruill1
1Department of Population Health, NYU School of Medicine, New York, NY, USA; 2Department of Health Education, Teachers College, Columbia University, New York, NY, USA
Correspondence: Jolaade Kalinowski
NYU School of Medicine, 180 Madison Avenue, 7-21A, New York, NY 10016, USA
Tel +1 646 501-3437
Email [email protected]
Objective: To elucidate women’s experiences with opioid medications and their perspectives on provider education regarding opioid use, risks and safety.
Methods: Women with a self-reported history of pain who had been prescribed opioids were recruited in 2016 using a convenience sampling approach that included an online social media campaign. Participants (N=154) completed online surveys and open-ended questions regarding their experiences with pain and opioids, and their perspectives on the quality of education they received from their providers.
Results: Participants reported receiving insufficient education about opioid-related side effects, as reflected in both ratings for the quantity and quality of education they received from their providers. Non-white participants reported lower quantity and poorer quality of provider education (p<0.05). Themes identified from the qualitative data included frustrations with pain management options, fear of opioids, stigma associated with opioid use, and the need for improved provider education and patient-provider communication.
Conclusion: Findings suggest that from a patient’s perspective, there is a need for enhanced patient-provider communication and education regarding pain management and potential opioid-related side effects. Improved physician communication and education could promote shared decision-making and result in enhanced satisfaction with care and health outcomes.
Keywords: opioids, pain management, patient-provider communication, women’s health
Introduction
The US is facing an opioid epidemic. The Centers for Disease Control and Prevention (CDC) estimated that 42,000 deaths were attributable to opioids in 2016.1 The rise of the opioid epidemic coincided with increases in opioid prescribing in recent years.2,3 From 2000 to 2010, opioid prescriptions reached 89.2 million, which was a 104% increase from 1990 to 2000.4 The 2015 National Survey on Drug Use and Health estimated that 3.8 million Americans were misusing prescribed pain relievers, and since 1999, there has been a fourfold increase in opioid overdose deaths.5 Among women, deaths from opioid pain relievers increased 415% between 1999 and 2010, in comparison to 265% in men.6
Based on national survey data, more than half of US adults reported experiencing some level of pain, and the prevalence of chronic pain (pain lasting more than 3 months) was 10–15%.7,8 Women have a higher prevalence of pain and report greater pain severity compared to men.9 They are also at increased risk for opioid addiction, given that they are more likely than men to be given prescriptions for opioid medications for pain management10,11 and are more likely to engage in regular opioid use.12 The risk of adverse outcomes is affected by factors disproportionately experienced by women, particularly psychological comorbidity (e.g. depression, anxiety),13 which can also exacerbate pain.14
In response to the growing opioid epidemic, a significant amount of attention has been placed on providers’ opioid prescribing practices15 and informed patient consent and shared decision-making in regards to opioid use.16 In 2016, the CDC released guidelines for opioid prescribing in the context of chronic pain.17 Providers are urged to provide education to patients on the adverse side effects of opioid use and strategies to mitigate these effects. The guidelines stress the importance of providing this education to not only patients, but also to their caregivers, family, and others in patients’ networks.17 Opioid Treatment Agreements (OTAs), contracts between patients and providers that often include informed consent prior to the initiation of opioid therapy, are especially critical given the benefits and potential risks associated with opioid use,18 though some question how such contracts can be enforced as well as the legal ramifications associated with written agreements.19
Despite the growing opioid epidemic and risks that face women, little research has been focused on women and how patient-provider education regarding opioid use. The purpose of this study was to ascertain the experiences and opinions of women who had been prescribed opioids for pain. The focus of this research was on how women evaluated the education they received from their providers on the risks and side effects of opioid prescribed for pain management.
Methods
The data from this study were obtained from an online survey of women over the age of 18 with a self-reported history of pain who indicated they were ever prescribed pain medication by a medical provider. A convenience and snowball sampling approach was used to recruit participants. The recruiting message was circulated via emails, text messages, and postings on websites such as and Facebook, Instagram, Twitter, Reddit, and Craigslist.
Study advertisements were sent to advocacy organizations, including Our Young Addicts, BoneSmart (an arthritis online discussion forum), AfterTheBite (a Lyme disease online discussion forum), and Courage to Speak (a foundation targeted towards preventing and addressing drug use). These organizations were targeted given the prevalence of chronic pain among individuals with lupus, Lyme disease, and arthritis.20–22 Flyers were also posted in the New York City community. Participants recruited via any of these approaches followed a link to the online survey. All participants provided informed consent.
Participation was limited to individuals who did not appear to have taken the survey more than once, ascertained by reviewing the database for duplicate computer IP addresses. Study participants were entered into a drawing to receive one of three $100 Amazon gift cards. Institutional Review Board (IRB) approval was obtained from Teachers College, Columbia University.
Participants completed questionnaires assessing sociodemographic information, reports of pain, and opioid use history. Those who reported that they had ever been prescribed an opioid (n=154), completed the Quality of Education/Rating of Provider Scale, which was developed for this study and had excellent internal consistency (Cronbach’s alpha=0.961). To ascertain side effects, participants were asked to indicate whether or not they experienced any of the following 29 opioid side effects, reported in five categories: 1) upon initial use (e.g. constipation, drowsiness and tiredness, etc.); 2) when the dose was too high (e.g. feeling very drowsy, confused, dizzy or faint, etc.); 3) when experiencing tolerance (i.e. need for a higher dose to experience relief from pain); 4) when experiencing withdrawal (e.g. yawning, sweating, nausea, vomiting, diarrhea, insomnia, etc.); and 5) when experiencing strong craving as a sign of addiction (e.g. uncontrollable desire). To ascertain whether or not participants were provided education on side effects, participants were asked if their provider delivered education regarding each of these five categories of side effects, and on what they should do if they experienced side effects (10 items). To measure participants’ rating of the quality of education received, participants were asked to rate the quality of education they received regarding each of the five categories of side effects, as well as an overall rating of the quality of education their provider delivered to them on opioid side effects (6 items). Each of the six items was rated on a 6-point Likert scale (very poor to excellent); total scores range from 6 to 36, with higher total scores indicating higher quality education.
In the qualitative aspect of the study, participants were asked the following three questions: 1) are there any thoughts or feelings that came up while you were taking this survey – specifically about your own experiences with taking narcotics/opioids/painkillers?; 2) do you have any thoughts or feelings about your experiences with medical providers who prescribed narcotics/opioids/painkillers to you?; and 3) do you have any recommendations with regard to these medical providers? The rationale for this approach stems from prior research demonstrating the benefit of utilizing open-ended questions in addition to close-ended questions, particularly with regard to provider satisfaction and care.23,24 Given the sensitive nature of the topic, a web-based survey was ideal for providing confidentiality.
Analysis
Quantitative data were analyzed in SPSS, 24.0. Associations between the quantity and quality of provider education received with participants’ age, race/ethnicity (white vs non-white) were assessed using Pearson’s correlations and independent samples t-test for continuous and dichotomous variables, respectively. Qualitative data were analyzed using thematic analysis,25 a method of analyzing qualitative data which emphasizes the identification of themes and patterns in qualitative data that has been previously utilized and discussed in the fields of health and psychology.26,27 For this particular study, qualitative data were collected and stored in SPSS. The responses were then reviewed and coded into themes based on patterns and prevalence of the responses submitted by participants. Using the principles of thematic analysis, two researchers reviewed the data and coded and identified emerging themes. A third researcher reviewed the data and themes for additional themes and patterns and to identify possible discrepancies.
Results
In total, 327 women responded to the survey link. Of these, 209 women were eligible for the study and 171 participants completed the survey. Of these, 154 reported having ever been prescribed opioids for pain management, thereby comprising the sample for this study. The mean age was 39.7 years (SD±12.3) and the majority of participants (78.6%; n=121) identified as non-Hispanic White, while 6.5% (n=10) identified as non-Hispanic Black, 6.5% (n=10) Asian, 4.5% (n=7) Latina, and 3.6% (n=6) endorsed other or selected more than one race/ethnicity. With regard to socioeconomic status, 33.1% (n=51) of participants reported an annual household income of less than $50,000, 27.9% (n=43) completed less than a Bachelor’s degree, and 70.8% (n=109) were employed full-time or part-time, as shown in Table 1.
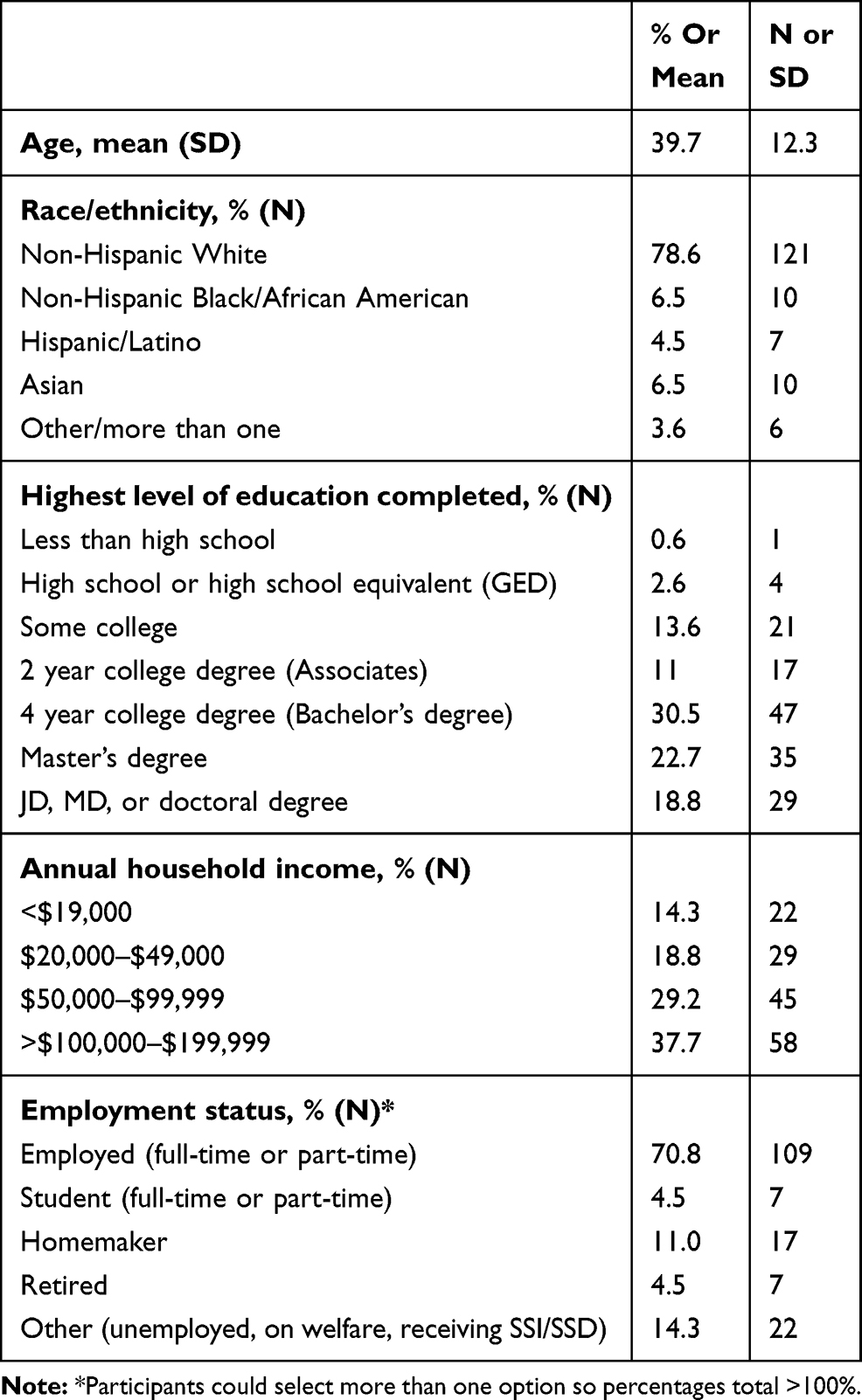 |
Table 1 Sample Characteristics (N=154) |
The most commonly reported types of pain (not mutually exclusive) were headache (82.5%), lower back pain (74.0%), dental pain (47.4%), knee pain (46.8%), joint pain (47.4%), migraine (42.2%), and muscle pain (42.2%). Chronic pain after acute health events or experiences was also common, including from surgery (48.1%), sports/exercise injuries (45.6%), dental procedures (32.5%), and labor/delivery (20.8%). Overall, chronic pain lasting for more than 6 months was reported by 60.4% of participants. Regarding opioids that had ever been taken, the top ranked were: Codeine at 57.1% (n=88), Oxycodone (OxyContin, Roxicodone, Oxecta) at 54.5% (n=84), Hydrocodone (Hysingla ER, Zohydro ER) at 46.1% (n=71), Tramadol (Ultram, ConZip) at 35.7% (n=55), and Morphine (Astramorph, Avinza, Kadian, MS Contin, Oramorph SR, Rescudose, Roxanol) at 27.3% (n=42).
Table 2 presents results regarding the frequency of each of the five categories of opioid-related side effects (Scale I), and the quantity (Scale II) and quality (Scale III) of provider education about each category of side effects. The majority of participants reported experiencing side effects related to initial opioid use (84.4%, n=130) and related to the dose being high (70.1%, n=108), while fewer reported side effects related to tolerance (32.5%, n=50), withdrawal (27.3%, n=42), or strong craving (10.4%, n=16). The mean provider education quantity (Scale II) was 4.5 on the 0–10 scale (SD=3.8). Rates of receiving provider education on individual side effects ranged from 31.8% (related to craving) to 70.8% (related to initial use). The mean overall education quality (Scale III) was 19.8 (SD=8.6), which corresponds to a rating between fair and poor. The quantity and quality of provider education were positively associated (r=0.79, p<0.001). White participants reported a higher quantity (5.0 vs 2.4, p<0.001) and quality (20.6 vs 17.1, p=0.038) of provider education received compared with non-white participants.
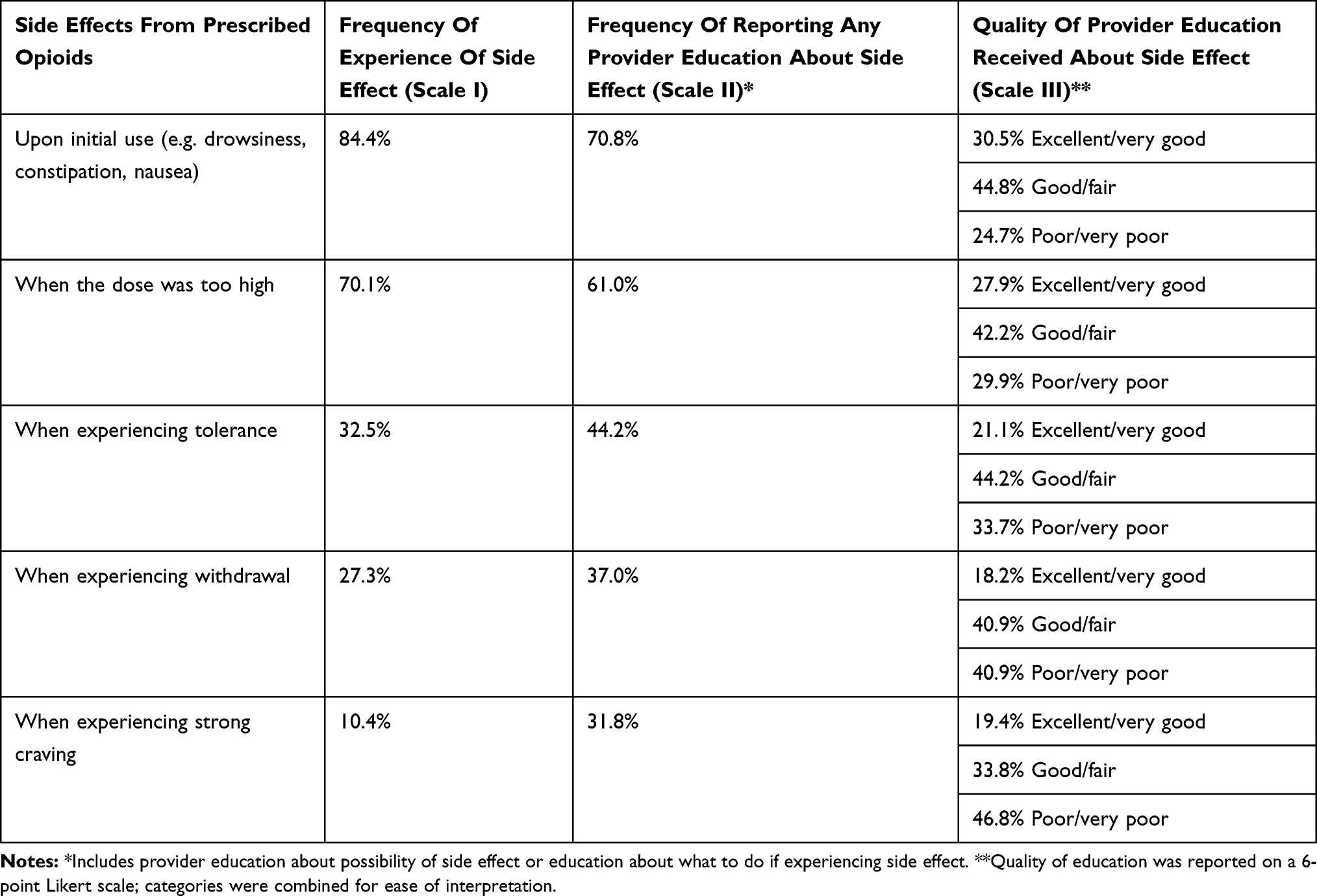 |
Table 2 Frequency Of Side Effects Of Prescribed Opioids And Receipt And Quality Of Provider Education About Side Effects Of Prescribed Opioids (N=154) |
With regard to the qualitative data, the thematic analysis of responses to the three open-ended questions resulted in the identification of the following themes: 1) frustrations with chronic pain; 2) fear of opioid medications; 3) acknowledgement of the stigma associated with taking opioids; 4) lack of provider emphasis on the root causes of pain; 5) improvements needed in patient/provider relationship communication; 6) desire for increased provider education on opioids and their risks; and 7) positive experiences with providers. Selected quotes from the 206 responses that illustrate these themes are presented below.
Theme 1: Frustrations With Chronic Pain
Many participants described frustrations and challenges associated with living with chronic pain. Others expressed frustration specifically related to needing opioids to manage their pain. For example, one woman explained,
I am addicted, but the problems of addiction aren’t as severe as the problems of my back injury. I wish I didn’t need opiates and I wish I understood better that I would become addicted when I first took them, but they let me live an almost normal life with my injury. I wish there was a non-addictive option, but the pros outweigh the cons.
Participants also expressed frustration with the lack of alternative options to manage their pain. Examples include, “Wish something was effective for pain management for chronic pain,” and, “Pain sucks and most days I just suffer through it not wanting to take drugs.”
Theme 2: Fear Of Opioid Medications
Participants expressed fear and anxiety about using opioid medications and how they feel when taking these medications. One participant expressed,
I personally don’t like taking pain medicine and only do so when I can no longer handle the level of pain I am at and all other forms of relief no longer work. I don’t enjoy feeling out of control so I take as little as possible but that still helps with the pain.
For others, a fear of addiction and side effects from opioid use was apparent. For example, one participant noted,
I was always nervous about taking the prescribed painkillers b/c [sic] I heard that addiction is easy to develop. I took less than the prescribed dose b/c [sic] they made me drowsy. I also felt nervous about the pain returning after I finished the prescription.
Another participant expressed, “Opioids are very dangerous, they scare me so I try to limit my exposure to them.” For some, these fears prevented them from taking opioids – even to manage pain concerns. One participant noted,
I need a stronger pain killer than tramadol to help with my chronic back pain, but I will never accept a prescription for harder narcotics or opioids because I don’t want to risk getting addicted.
Theme 3: Acknowledgement Of The Stigma Associated With Taking Opioids
A persistent theme throughout the open-ended responses was an acknowledgement of the stigma associated with opioid use.
I’ve used pain medicine as one of MANY management tools. This survey highlights real concerns, but also stigma. There are patients who take their medications appropriately and responsibly, and our story in the context of our current opioid crisis is usually not shared.
Some participants elaborated on their own experience of feeling stigma for taking opioids and expressed frustration with people who suffer from addiction. One participant explained,
I feel vilified for needing pain killers. But I genuinely do not take to get high, I never have (except back in high school for fun). It’s unfortunate that people with chronic, severe pain have a hard time getting access to medicine just because addicts can’t control themselves.
Another participant noted,
I am tired of people conflating my use of prescription painkillers with addiction and illegal behavior. There are lots of people that use these drugs and don’t end up addicted and living on the streets.
These fears of stigma also affected how they believed they were being perceived by doctors and medical providers. For example, a participant expressed, “Doctors treat pain patients like drug addicts which leads to low self-esteem, guilt and potentially poor choices for those patients.” Another noted, “There is a lot of distrust of patients who genuinely need these kinds of medication. I don’t think it stops a lot of addicts, I think it hurts people with chronic pain.”
Theme 4: Lack Of Emphasis On The Root Causes Of Pain
Participants expressed a desire for medical providers to focus on the root causes of pain, not necessarily the pain itself. For example, one participant recommended,
Be proactive and do tests to rule out what may be causing the pain instead of just treating the symptoms and hoping it will go away. Also don’t dismiss our pain and treat us like its psychological just because you don’t know the answer to what’s causing the pain.
Another participant stated, “They just prescribe pills instead of finding out and treating the cause of my pain.” Others experienced such issues even when they made attempts to investigate the cause of their pain further. For example, one participant noted, “She turned to prescribing painkillers as a first treatment response instead of considering alternative treatments, even though I proactively asked about other treatment options.” Others also expressed a desire for providers to receive more education and training about pain management. One participant argued, “They need to be educated to look for the source of the pain and stop telling people pain is ‘all in their head’ when it is physical pain.”
Theme 5: Improvements Needed In Patient/Provider Relationship And Communication
Participants described inadequate patient/provider relationships and identified areas for improvement. Some participants described their providers as dismissive, attributing such treatment to gender stereotypes. For example, one participant stated, “Do not dismiss women as dramatic.” Others expressed a desire for providers to understand their needs and desires regarding their pain. A recommendation that one participant expressed for providers was, “To listen, we know how we feel.” Some participants expressed that perhaps this could be achieved with increased training. For example, one recommendation for providers was to have, “Better training and more empathy. Focus more on why people are sick instead of giving them prescriptions.”
Theme 6: Desire For Increased Provider Education On Opioids And Their Risks And Alternatives
Many participants expressed a desire for increased provider education. For example, one participant stated,
I have been provided little to no information from any provider who has ever prescribed me a narcotic. I have also been prescribed a narcotic without realizing [until] I took the rx to be filled.
Others noted, “I wish they had better informed me of potential implications of using these medications,” and, “Although my medical provider mentioned the potential side effects, she did not provide much information about how to address any side effects I actually experienced.” One participant also expressed a desire for education from medical providers on alternative treatments, stating,
Listen to your patients and their concerns before prescribing painkillers. Some patients do not want to take them and may want more information about other forms of treatment, which you should have information available about.
Theme 7: Positive Experiences With Providers
While some participants expressed frustration with their experiences with their medical providers, others reported positive experiences. One participant noted,
I was fortunate to have an excellent physician, who informed me of what I needed to know and worked with me to address any side effects that came up, whether that involved adding sennokot for constipation or switching the opiate because it was not effectively addressing my pain or was causing too much fatigue.
Others stated,
I’ve had wonderful providers who set guidelines for proper pain medicine usage and took the time to understand the big picture–opiates are a tool that should be used in the right circumstances, but not the ONLY tool,
and, “I feel anyone who has prescribed to me has given me the proper warnings/education based on my propensity to use.”
Discussion
This study adds to the body of literature regarding women’s experiences with their providers in the context of pain and opioid use. Overall, both quantitative and qualitative findings indicate that participants felt they received insufficient education from providers regarding opioids. Almost one-quarter of women reported receiving no education about any of five categories of opioid-related side effects assessed. More than half the sample reported receiving no education about tolerance, withdrawal, and craving, which are possible indicators for opioid use disorder when they occur in individual taking opioids outside of medical supervision.28,29 The average rating of the quality of provider education received on opioid side effects fell between “fair” and “poor” on the 6-point response scale. The qualitative data reinforced the quantitative data, as participants expressed dissatisfaction with provider education about opioids and their associated risks in response to open-ended questions. Though some positive experiences with providers were described, many participants described poor patient-provider relationships, including a perceived lack of trust and harsh judgment from providers. The qualitative data also suggested that patients felt that their pain was not addressed by their provider and felt judgement and distrust from their providers, which was adversely affecting their health. This sentiment is consistent with other studies that have noted how lack of trust by providers is associated with poor health outcomes for patients.30 Several participants expressed that they felt their pain had been overlooked or ignored. This is consistent with other studies that have discussed the tendency for women’s pain to be overlooked and not taken seriously.31,32 Other emergent themes such as concerns about opioid side effects, fear of developing addiction, and perceived stigma were also reported which have been reported in other studies as well.33–35 It is noteworthy that some participants reported feeling stigmatized for using opioids appropriately for pain management, but also used stigmatizing language to describe their views of others they perceived as misusing opioids.
A number of factors likely contribute to the insufficient education reported by patients who are prescribed opioids, including poor provider knowledge, poor communication, and implicit or explicit bias. In the current study, non-white participants reported receiving significantly lower quality education than white participants. This is consistent with a large body of data documenting racial and ethnic disparities in service delivery.36,37 This disparity is particularly concerning given that education quality was associated with opioid diversion, a growing concern within the opioid epidemic.38,39
Several limitations of the current study must be considered. First, this study was cross-sectional and retrospective, so possible changes in participants’ perceptions and opinions over time were not captured. Additionally, the retrospective study design is subject to recall bias. Second, the convenience sample was majority white (78.6% n=121) and of high socioeconomic status (i.e. 72.0% [n=111] college educated, 37.7% [n=58] with annual income >100,000), which limits the generalizability of the results. Third, the measures of quantity and quality of provider education were developed for this study and not previously validated.
Finally, it is important to note that the feedback we obtained concerned just one side of the patient-provider interaction. While it is noteworthy that the findings reflect insufficient education being delivered from providers about opioid use, it is also possible that education provided was not understood or retained by patients, as has occurred in previous studies.40 Regardless, the low level of patient satisfaction with provider education and care around pain management and opioids suggests the need for improved provider training and communication with patients.
Conclusion
Pain is one of the most common symptoms that patients present for resolve.41 Yet, training on non-pharmacological approaches for managing pain and best practices surrounding opioid prescribing could be improved.42,43 Many studies and interventions have focused on education of physicians and prescribers;44,45 yet, few have focused on education at the patient level. This study suggests that patient-provider education on opioids may be ineffective from the perspective of the patient. There are few research studies that have assessed patient education and opioids. A recent review suggested that perhaps nurses may be able to play an important role. Andrews-Cooper and Kozachik (2019) found that patient education was linked to the use of nonpharmacological modalities NPMs as well as improved pain management, thereby reducing risk for opioid use and their associated risks.46 One participant who was a nurse expressed, “I am a nurse and am very aware of this topic. I don’t see much discussion from doctors at work about this.” Because nurses are often on the front-lines of care, they have critical insight into patient care and education. Manworren and Gilson (2015) highlighted the helpful role nurses can have on patient education about opioid diversion, disposals, and general risks about opioid use.47 Previous studies have also highlighted the critical role nurses may play in the opioid epidemic and the clear gaps in knowledge and skills to meet these new demands.48,49 Researchers found that screening, brief intervention, and referral to treatment (SBIRT) education may facilitate increased understanding and reduced stigma among nurses caring of patients who use opioids and other substances.50 Costello et al (2016) also found that nurses’ knowledge of opioid safety was associated with patients’ knowledge about opioid use.51
The findings from this study also suggest the need for enhanced patient-provider communication that promotes shared decision-making by patients and providers and reduces stigma. Smith et al (2006) explored how patient-provider communication may affect pain and health outcomes and found that increased dialogues and exchanges between providers and patients led to more openness from patients regarding their concerns and symptoms of pain.52
While improved patient-provider communication is needed, it is important to acknowledge the realities facing both patients and providers. Patient-provider agreements (PPA) may be an effective tool for improving opioid education to patients, but barriers to their use include time, lack of evidence that they are effective, and lack of a standard agreement.53 Moreover, some data on the efficacy of PPAs demonstrate that they may be ineffective.54 Qualitative research has shown that pain management plans can be efficacious in helping both providers and patients set and manage their expectations of pain management, but such conversations are difficult, and being asked about possible substance use disorder may prompt some patients to seek care elsewhere.55 To overcome these barriers, it is imperative that providers receive education about how to best develop and use pain management plans and how to handle challenging conversations and dialogues regarding substance use disorder. Education programs that incorporate communication skills training may discourage physician bias15 and help providers become better equipped to handle sensitive conversations about opioids with patients.56
This research study helped to underscore the importance of patient education and how from a patient’s perspective, education from providers on opioids and the risks associated with their use is inadequate. Future research should explore whether interventions at the patient or provider level can increase patient satisfaction and knowledge regarding opioid education.
Acknowledgments
Sources of Funding This work was supported in part by the National Institutes of Health (T32HL129953 and KHL125939). The views expressed in this article are those of the authors and do not necessarily represent the views of the National Institutes of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control. Opioid overdose. Centers for Disease Control; 2017. Available from: https://www.cdc.gov/drugoverdose/index.html>.
2. Levy B, Paulozzi L, Mack K, Jones C. Trends in opioid analgesic–prescribing. Am J Prev Med. 2015;49(3):409–413. doi:10.1016/j.amepre.2015.02.020
3. Guy GP
4. Sites BD, Beach ML, Davis MA. Increases in the use of prescription opioid analgesics and the lack of improvement in disability metrics among users. Reg Anesth Pain Med. 2014;39(1):6–12. doi:10.1097/AAP.0000000000000022
5. Center for Behavioral Health Statistics and Quality; 2017. Key substance use and mental health indicators in the United States: Results from the 2015 National Survey on Drug Use and Health (HHS Publication No. SMA 16-4984, NSDUH Series H-51). Retrieved from http://www.samhsa.gov/data/
6. Centers for Disease Control and Prevention. Vital signs: overdoses of prescription opioid pain relievers and other drugs among women — United States, 1999–2010. MMWR Morb Mortal Wkly Rep. 2013;62(26):537–542. doi:mm6226a3 [pii]
7. Nahin RL. Estimates of pain prevalence and severity in adults: United States, 2012. J Pain. 2015;16:769–780. doi:10.1016/j.jpain.2015.05.002
8. Hardt J, Jacobsen C, Goldberg J, Nickel R, Buchwald D. Prevalence of chronic pain in a representative sample in the United States. Pain Med. 2008;9(7):803–812. doi:10.1111/j.1526-4637.2008.00425.x
9. Campbell CI, Weisner C, LeResche L, et al. Age and gender trends in long-term opioid analgesic use for noncancer pain. Am J Public Health. 2010;100:2541–2547. doi:10.2105/AJPH.2009.180646
10. Koons AL, Rayl Greenberg M, Cannon RD, Beauchamp GA. Women and the experience of pain and opioid use disorder: a literature-based commentary. Clin Ther. 2018;40(2):190–196. doi:doi:10.1016/j.clinthera.2017.12.016
11. Bawor M, Dennis BB, Varenbut M, et al. Sex differences in substance use, health, and social functioning among opioid users receiving methadone treatment: a multicenter cohort study. Biol Sex Differ. 2012;6. doi:10.1186/s13293-015-0038-6
12. Parsells Kelly J, Cook SF, Kaufman DW, Anderson T, Rosenberg L, Mitchell AA. Prevalence and characteristics of opioid use in the US adult population. Pain. 2008;138(3):507–513. doi:10.1016/j.pain.2008.01.027
13. Park TW, Saitz R, Ganoczy D, Ilgen MA, Bohnert ASB. Benzodiazepine prescribing patterns and deaths from drug overdose among US veterans receiving opioid analgesics: case-cohort study. BMJ. 2015;350:h2698–h2698. doi:10.1136/bmj.h2698
14. Conway A, Sheridan J, Maddicks-Law J, et al. Depression and pain in heart transplant recipients: an observational study. Biol Res Nurs. 2017;19:71–76. doi:10.1177/1099800416666717
15. Volkow ND, McLellan AT. Opioid abuse in chronic pain — misconceptions and mitigation strategies. N Engl J Med. 2016;374(13):1253–1263. doi:doi:10.1056/NEJMra1507771
16. Kinsman Hughes H, Korthuis P, Saha S, et al. Study of patient-provider communication about opioid analgesics. Patient Educ Couns. 2015;98(4):453–461. doi:10.1126/science.1249098.Sleep
17. Dowell D, Haegerich T, Chou R; Centers for Disease Control and Prevention. CDC guideline for prescribing opioids for chronic pain — United States, 2016. Morb Mortal Wkly Rep. 2016;65(1). doi:10.15585/mmwr.rr6501e1er
18. Cheatle MD, Savage SR. Informed consent in opioid therapy: a potential obligation and opportunity. J Pain Symptom Manage. 2012;44(1):105–116. doi:doi:10.1016/j.jpainsymman.2011.06.015
19. Arnold RM, Han PKJ, Seltzer D. Opioid contracts in chronic nonmalignant pain management: objectives and uncertainties. Am J Med. 2006;119(4):292–296. doi:10.1016/j.amjmed.2005.09.019
20. Bouhassira D, Lantéri-Minet M, Attal N, Laurent B, Touboul C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain. 2008;136(3):380–387. doi:10.1016/j.pain.2007.08.013
21. Greco CM, Rudy TE, Manzi S. Effects of a stress-reduction program on psychological function, pain, and physical function of systemic lupus erythematosus patients: a randomized controlled trial. Arthritis Care Res (Hoboken). 2004;51(4):625–634. doi:10.1002/art.20533
22. McDougall JJ. Arthritis and pain. Neurogenic origin of joint pain. Arthritis Res Ther. 2006;8(6):220. doi:10.1186/ar2069
23. Alemi F, Torii M, Clementz L, Aron DC. Feasibility of real-time satisfaction surveys through automated analysis of patientsʼ unstructured comments and sentiments. Qual Manag Health Care. 2012;21(1):9–19. doi:10.1097/QMH.0b013e3182417fc4
24. Locker D. Theoretical and methodological issues in sociological studies of consumer satisfaction with medical care. Soc Sci Med. 1978;12(283).
25. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1–13. doi:10.1177/1609406917733847
26. Braun V, Clarke V, Qualitative research in psychology using thematic analysis in psychology using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
27. Braun V, Clarke V. What can “thematic analysis” offer health and wellbeing researchers? Int J Qual Stud Health Well-Being. 2014;9:9–10. doi:doi:10.3402/qhw.v9.26152
28. Webster LR. Risk factors for opioid-use disorder and overdose. Anesth Analg. 2017;125(5):1741–1748. doi:doi:10.1213/ANE.0000000000002496
29. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). doi:10.1176/appi.books.9780890425596
30. Thom DH. Physician trust in the patient: development and validation of a new measure david. Ann Fam Med. 2001;9(2):148–154. doi:10.1370/afm.1224
31. Kuligowska E, Deeds L, Lu K. Pelvic pain: over- looked and underdiag- nosed gynecologic OBJECTIVES. Genetics. 2005;25:3–20.
32. Werner A, Isaksen LW, Malterud K. “I am not the kind of woman who complains of everything”: illness stories on self and shame in women with chronic pain. Soc Sci Med. 2004;59(5):1035–1045. doi:doi:10.1016/j.socscimed.2003.12.001
33. Katelaris P, Krassas G. General practice the clinical challenge of opioid-induced constipation: insights from the opioid-induced constipation clinical audit. J Gen Pr. 2014;4:4. doi:doi:10.4172/2329-9126.1000221
34. van Dijk JFM, Kappen TH, Schuurmans MJ, van Wijck AJM. The relation between patients’ NRS pain scores and their desire for additional opioids after surgery. Pain Pract. 2015;15(7):604–609. doi:doi:10.1111/papr.12217
35. Kennedy-Hendricks A, Barry CL, Gollust SE, Ensminger ME, Chisolm MS, McGinty EE. Social stigma toward persons with prescription opioid use disorder: associations with public support for punitive and public health–oriented policies. Psychiatr Serv. 2017;68(5):462–469. doi:doi:10.1176/appi.ps.201600056
36. Zuvekas S, Taliaferro G. Pathways to access: health insurance, the health care delivery system, and racial/ethnic disparities, 1996–1999. Health Aff. 2003;22(2):139–153.
37. Fiscella K, Franks P, Gold MR, Clancy CM. Inequality in quality. Jama. 2000;283(19):2579. doi:doi:10.1001/jama.283.19.2579
38. Volkow N, Benveniste H, McLellan AT. Use and misuse of opioids in chronic pain. Annu Rev Med. 2018;69(1):
39. Hahn KL. Strategies to prevent opioid misuse, abuse, and diversion that may also reduce the associated costs. Am Health Drug Benefits. 2011;4(2):107–114.
40. Goldkamp J, Anderson S, Lifits-Podorozhansky Y, Gavard JAG. Women’s perceptions regarding obesity and comorbidities and provider interaction. J Obstet Gynecol Neonatal Nurs. 2015;44:784–792. doi:doi:10.1111/1552-6909.12751
41. Schnoll SH, Finch J. Medical education for pain and addiction: making progress toward answering a need. J Law Med Ethics. 1994;22(3):252–256. doi:10.1111/j.1748-720X.1994.tb01303.x
42. Waszak DL, Mitchell AM, Ren D, Fennimore LA. A quality improvement project to improve education provided by nurses to ED patients prescribed opioid analgesics at discharge. J Emerg Nurs. 2018;44(4):336–344. doi:doi:10.1016/j.jen.2017.09.010
43. Upshur CC, Luckmann RS, Savageau JA. Primary care provider concerns about management of chronic pain in community clinic populations. J Gen Intern Med. 2006;21(6):652–655. doi:doi:10.1111/j.1525-1497.2006.00412.x
44. Levi-Minzi MA, Surratt HL, Kurtz SP, Buttram ME. Under treatment of pain: a prescription for opioid misuse among the elderly? Pain Med. 2013;14(11):1719–1729. doi:10.1111/pme.12189
45. Kaye AD, Jones MR, Kaye AM, et al. Prescription opioid abuse in chronic pain an updated review of opioid abuse predictors and strategies to curb opioid abuse part 1. Pain Physician. 2017;20:93–110.
46. Andrews-Cooper IN, Kozachik SL. How patient education influences utilization of nonpharmacological modalities for persistent pain management: an integrative review. Pain Manag Nurs. 2019;(xxxx). doi:10.1016/j.pmn.2019.06.016
47. Manworren RCB, Gilson AM. CE: nurses’ role in preventing prescription opioid diversion. Am J Nurs. 2015;115(8):34–40. doi:doi:10.1097/01.NAJ.0000470398.43930.10
48. Costello M, Thompson S. Preventing opioid misuse and potential abuse: the nurse’s role in patient education. Pain Manag Nurs. 2015;16(4):515–519. doi:doi:10.1016/j.pmn.2014.09.008
49. Lewis LF, Jarvis L. Undergraduate nursing students’ experiences and attitudes towards working with patients with opioid use disorder in the clinical setting: a qualitative content analysis. Nurse Educ Today. 2019;73(July 2018):17–22. doi:doi:10.1016/j.nedt.2018.11.001
50. Mahmoud KF, Finnell D, Lindsay D, et al. Can screening, brief intervention, and referral to treatment education and clinical exposure affect nursing students’ stigma perception toward alcohol and opioid use? J Am Psychiatr Nurses Assoc. 2018. doi:doi:10.1177/1078390318811570
51. Costello M. Prescription opioid analgesics: promoting patient safety with better patient education. Am J Nurs. 2015;115(11):50–56. doi:doi:10.1097/01.NAJ.0000473315.02325.b4
52. Smith MY, Winkel G, Egert J, Diaz-Wionczek M, DuHamel KN. Patient-physician communication in the context of persistent pain: validation of a modified version of the patients’ perceived involvement in care scale. J Pain Symptom Manage. 2006;32(1):71–81. doi:doi:10.1016/j.jpainsymman.2006.01.007
53. Kraus CN, Baldwin AT, Curro FA, McAllister RG. Clinical implications of patient-provider agreements in opioid prescribing. 2015. http://www.ingentaconnect.com/content/ben/cds/2015/00000010/00000002/art00010?crawler=true.
54. Starrels JL, Becker WC, Alford DP, Kapoor A, Williams AR, Turner BJ. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152(11):712–720. doi:doi:10.7326/0003-4819-152-11-201006010-00004
55. Chang JS, Kushel M, Miaskowski C, et al. Provider experiences with the identification, management, and treatment of co-occurring chronic noncancer pain and substance use in the safety net. Subst Use Misuse. 2017;52(2):251–255. doi:10.1080/10826084.2016.1223138
56. Davis CS, Carr D. Legal changes to increase access to naloxone for opioid overdose reversal in the United States. Drug Alcohol Depend. 2015;157:112–120. doi:10.1016/j.drugalcdep.2015.10.013
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.