Back to Journals » Clinical Interventions in Aging » Volume 12
Why do seniors leave resistance training programs?
Authors Burton E ![]() , Hill AM
, Hill AM ![]() , Pettigrew S, Lewin G
, Pettigrew S, Lewin G ![]() , Bainbridge L
, Bainbridge L ![]() , Farrier K, Airey P, Hill KD
, Farrier K, Airey P, Hill KD ![]()
Received 21 November 2016
Accepted for publication 9 February 2017
Published 27 March 2017 Volume 2017:12 Pages 585—592
DOI https://doi.org/10.2147/CIA.S128324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Elissa Burton,1 Anne-Marie Hill,1 Simone Pettigrew,2 Gill Lewin,3 Liz Bainbridge,1 Kaela Farrier,1 Phil Airey,4 Keith D Hill1
1School of Physiotherapy and Exercise Science, 2School of Psychology and Speech Pathology, 3School of Nursing, Midwifery and Paramedicine, Curtin University, 4Council on the Ageing, Perth, WA, Australia
Purpose: The proportion of the population, that is older, is growing at a faster rate than other age groups. Physical activity is important for older people because it assists in living independently. Participating in resistance training on a regular basis (twice weekly) is recommended for older people; yet, fewer than 15% of people over 60 years achieve this level. The aim of this article was to investigate the factors contributing to older people’s decisions to stop participation in a resistance training program.
Participants and methods: Participants were older people who had chosen to participate in a structured resistance training program specifically designed for seniors and then after a period of time discontinued. This population received a questionnaire in the mail focused on factors contributing to their cessation of resistance training exercise. Qualitative results were analyzed using inductive content analysis.
Results: Fifty-six survey responses were received (average age 71.5 years, SD =9.0; 79% females). Injury, illness, and holidaying were the main reasons for ceasing participation. A small but important number of responses (11%) reported that they considered they were not provided with sufficient support during the resistance training programs.
Conclusions: To attract and retain their senior clients, the results indicate that program organizers need to provide tailored support to return to resistance training after injury and offer flexible and individualized services that accommodate older people’s life choices in retirement.
Keywords: older people, strength training, gymnasium, retention, aging
Introduction
It is well established that resistance training is good for adults’ health, regardless of age.1–3 Increased strength and bone density, improved ability to complete activities of daily living, improvement in health-related quality of life, reduced signs and symptoms of chronic illness, and a reduction in sarcopenia are all benefits of regular participation in resistance (strength) training.4 The World Health Organization (WHO) and multiple national guidelines specifically include resistance training in their recommended physical activity guidelines, particularly the guidelines for those aged ≥60 years (older people).5,6 Nevertheless, the proportions of older people participating are low.7–9
Older populations across the world are growing, and it is expected that by 2050, there will be two billion people aged ≥60 years living worldwide, which is more than double the number in 2013.10 With this increase, it is important that older people stay as healthy as possible for as long as they can to avoid needing ongoing health and care services, hospitalization, or a move into residential aged care. Physical activity plays an essential role in staying healthy, maintaining independence, reducing the risk of falling, and allowing older people to live their later life well.11,12 The physical activity of choice for older people, particularly in Australia is walking, with the majority of the older population participating only in this mode of exercise.13
Studies have shown that fewer than 15% of older people participate in resistance training twice a week (the minimum guideline recommended frequency).14,15 A number of studies have explored motivators and barriers to older people participating (or commencing participation) in resistance training in an attempt to increase participation rates.16–19 The main motivators specific to older people participating in resistance training were preventing deterioration or disability, building muscle, falls prevention, and feeling more alert or having better concentration.16 Barriers are usually identified by asking participants who are not or have not participated in a given activity to provide their reasons for not taking part. For older people, barriers to participating in resistance training include the following: health issues, pain, tiredness or fatigue, lack of social support, and a lack of available exercise facilities.16
Given the low uptake of resistance training by older people, it is important that strategies are implemented to support ongoing participation for those who commence such programs, so that they maintain long-term participation, which can assist to optimize health and well-being. Evidence from two systematic reviews that examined the effects of resistance training for improving physical function4 and exercise for improving balance20 found withdrawals after 12 months participating ranged between 20% and 48%, respectively. This highlights the importance not only for research to guide improved uptake or commencement of resistance training programs but also for retaining those who commence programs for the longer term. This study differs from other studies described as investigating barriers or reasons for ceasing participation because participants in these previous studies were still engaged in a resistance training program or had never participated.19,21,22 However, this study explores reasons why older people stop participating in a structured resistance exercise program by asking people who have recently made this choice. Exploring why this particular cohort ceases resistance training could benefit older people by assisting them to understand how to maintain their participation in resistance training. It is also important for gymnasium and fitness center owners, managers, and staff who provide such programs to better understand the reasons why older participants withdraw from attending resistance training programs after having commenced the program. Therefore, the aim of this study was to identify the reasons why older people who had been participating in a resistance training program chose to discontinue participation.
Participants and methods
Study design and sample
This was a cross-sectional descriptive study, in which participants were surveyed by mail. Inclusion criteria were people aged ≥60 years who had been attending a structured, gymnasium-based, resistance training program specifically designed for older people (ie, Living Longer Living Stronger)23 and who within the previous 15 months decided to no longer attend. During August and September 2015, questionnaires were sent to participants who had ceased participation in a resistance training program between May 2014 and April 2015. The managers from 15 gymnasiums advised the number of members who had ceased participation in their Living Longer Living Stronger resistance training programs (n=293) for the research team, to ensure an adequate number of surveys were provided to them for distribution. Due to confidentiality requirements, the managers could not provide actual contact details of these former participants to the research team. As a result, the researchers prepared 293 participant invitation letters, questionnaires, and reply paid envelopes into individual envelopes and posted them in bundles to each of the participating managers. The managers then added a name and address label to each individual envelope and posted them to past members meeting the study criteria. The participating gymnasiums were all delivering Living Longer Living Stronger resistance training programs specifically for seniors within their facility and agreed to be involved in the research.
Questionnaire
The questionnaire was developed by the researchers, research partners who came from a seniors’ advocacy organization, and a home care agency. Two consumer representatives (two older people, aged in their late 70s – one who participated regularly in resistance training and one who did not) also assisted to develop the wording and format of the questionnaire. This study was one section of a larger research project, and the consumer representatives were part of the project team for a period of 2 years. Both consumer representatives had worked extensively in education (Professorial level) and/or the sport industry in their previous working lives. Their role in this project was to provide feedback on the appropriateness of all research documents, methods, language, and so on to older people in the community.
The lack of research in this area prevented the use of validated scales in the data collection, but the questionnaire was based on eliciting responses, which would explain the reasons why participants no longer attended the resistance training program. The questionnaire included participant demographics (eg, age, sex, area lived in, self-reported physical and mental health, and number of prescribed medications taken daily), physical activity levels, why they joined resistance training and for how long (including sessions per week), type of program they had attended, why they withdrew, and whether they would consider participating again in the future and, if so, why. Other questions related to how challenging they found the resistance training program, whether they noticed any physical or psychological changes due to participating, their perspectives on whether the program represented value for money, their confidence in completing sessions, support received, and motivation to participate. A combination of open and closed questions (Likert scales) were utilized to avoid bias associated with checklists and to ensure opportunity for maximal responses. A copy of the survey is available from the corresponding author.
The physical activity level data in the questionnaire involved using the Physical Activity Scale for the Elderly (PASE), which is a valid and reliable tool for determining physical activity levels of older people.24,25 Scores on the PASE can range from 0 to 400, where 0 being not active at all to 400 being very active.
Statistical analysis and ethics
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) (version 22). Descriptive statistics were generated for all quantitative data using the total sample. The qualitative data derived from the open-ended responses were analyzed using inductive content analysis. Content analysis is a research method for making replicable and valid inferences from data in a way which can generate new insights and can inform practical actions.26 Inductive content analysis was used as it was felt that there was limited knowledge about barriers and enablers to resistance training in this specific cohort.27 These data were entered verbatim onto an Excel spreadsheet (Microsoft Corporation, Washington, DC, USA), and color highlights were used to code. Responses were prepared using open coding, category creation, and abstraction. A number of categories were generated from the headings copied onto coding sheets. Two researchers (EB and A-MH) coded the data independently, then compared and discussed the data until they reached a consensus. The results were then joined under higher order headings to reduce the number of categories through the collapse of like and unlike categories. Content-specific words were then added to each category. Categories with similarities were combined to make the main categories. Frequency counts were undertaken where data were grouped into subcategories. The final data were presented using participant quotes to illustrate each category. To assist in clarifying connections among the categories, these data were concept mapped using Visio (Microsoft Corporation). Concept maps are graphical tools that are used for confirming relationships among concepts and validating ideas.28 The concept map was constructed with reference to the research question “why do older people who had been participating in a resistance training program choose to discontinue?” To minimize bias, the analyses were verified at each stage by a second independent researcher (A-MH). Ethics approval was granted from the University Human Research Committee (HR38/2015). Informed consent was assumed by the completion and return of the questionnaire.
Results
Respondents
Of the 293 questionnaires posted by the 15 gymnasiums, 56 were returned, a response rate of 19%. The mean age of respondents was 71.5 years (SD: 9.0), with over three quarters (79%, n=44) being female and 21% male (n=12). Almost all (95%, n=53) respondents lived in the metropolitan area. Over three quarters (79%, n=44) said that they had good (39%, n=22), very good (30%, n=17), or excellent (9%, n=5) physical health. The majority (87%, n=49) also reported being in good to excellent mental health. Almost half were taking three or more prescribed medications (48%, n=27), with only 16% taking none (n=9). The mean PASE score for the group was 119.5 (SD: 68.4), males: 156.8 (SD: 78.0) and females: 113.5 (SD: 63.2). Given the PASE norms for 70–75 year olds are males: 102.4 (SD:53.7) and females: 89.1 (SD:55.5),29 these groups were more physically active than others of a similar age.
Attendance
Over half (57.1%, n=32) of the respondents had attended the resistance program for >4 months. Only 8.9% left in the first month (n=5), 12.5% during months 1 and 2 (n=7), 8.9% between months 2 and 3 (n=5), and 12.5% in months 3 and 4 (n=7). During the initial 4 months, most respondents attended class once (36.8%, n=21) or twice (47.4%, n=27) a week. Only eight respondents (14%) attended three classes a week and no one attended more than three.
Many respondents attended a group session (53.6%, n=30) or a combination of group and individual work (10.7%, n=6), whereas 19.6% worked individually (n=11) and 16.1% had a personalized assessment (n=9). Ninety-three percent of respondents (n=52) were confident or very confident that they could complete the exercises included in the sessions. Only 7.2% were not confident (n=2) or not confident at all (n=2) in completing the exercises. Almost 80% of respondents were motivated (41.1%, n=23) or very motivated (37.5%, n=21) to complete each session. Twelve percent described themselves as neither motivated nor not motivated (neutral) and 8.9% (n=5) as not or not at all motivated.
Program support
The majority of respondents felt that they were given more than adequate (26.8%, n=15) or adequate (46.4%, n=26) support during their sessions. However, 10% suggested that they were given inadequate (1.8%, n=1) or very inadequate (8.9%, n=5) support, and a further 16.1% (n=9) were neutral on this subject. Comments on where improvement could occur included:
the instructor was more interested in their own exercise regime than considering the needs of their clients (n=2), the attention you received from the physio during the session depended on whether you were a patient at the practice or not and the instructors tended to respond to your questions rather than initiating any step-up in exercise.
There were also a number of positive comments which included the following: staff being helpful and supportive (n=10), exercise individualized to my level and capabilities (n=4), and average group of 10 with an engaged and interested physio always present.
Respondents were asked to rate the adequacy of the information provided about safety while they were participating in the resistance training program. In total, 88% said that the information was either adequate (n=25) or very adequate (n=20). Twelve percent rated safety information as inadequate (n=3) or very inadequate (n=3).
Reasons for withdrawing from the program
There were initially 70 reasons given by respondents as to why they withdrew. These were coded into three subcategories, such as health, program/facility, and other. Injury (32.1%, n=18) was the most common reason to emerge for the respondents ceasing participation in a resistance training program. Table 1 shows the main categories, subcategories, and some example quotes from respondents. There were many reasons for discontinuing, and 22 of the 56 questionnaire respondents (39.3%) reported two or more reasons for withdrawing. The three most commonly reported reasons within the subcategories for withdrawing included illness, holidays, and the program not being suitable. Cost was only reported by two participants. Over three quarters of the respondents thought that the resistance training program was good (40.4%, n=23) or very good (36.8%, n=21) value for money. Ten percent found the cost barely acceptable (n=6), 1.8% poor (n=1), and 5.3% very poor (n=3).
 | Table 1 Reasons for withdrawing |
Negative aspects of the resistance training program
Only 36 respondents (64.3%) answered this question, the other 20 either left it blank (n=10) or reported none (n=10). Class time and places available within preferred classes were the most commonly identified negative aspects of the resistance training programs. Waiting for machines and equipment issues were also highlighted as well as poor staff support and the program not satisfying the participants. Table 2 shows the main categories, subcategories, and participant quotes of the most commonly reported negative aspects of participating in a resistance program. Although the blank responses cannot be interpreted, it is likely that those reporting “none” had ceased participation for reasons other than those relating to the program.
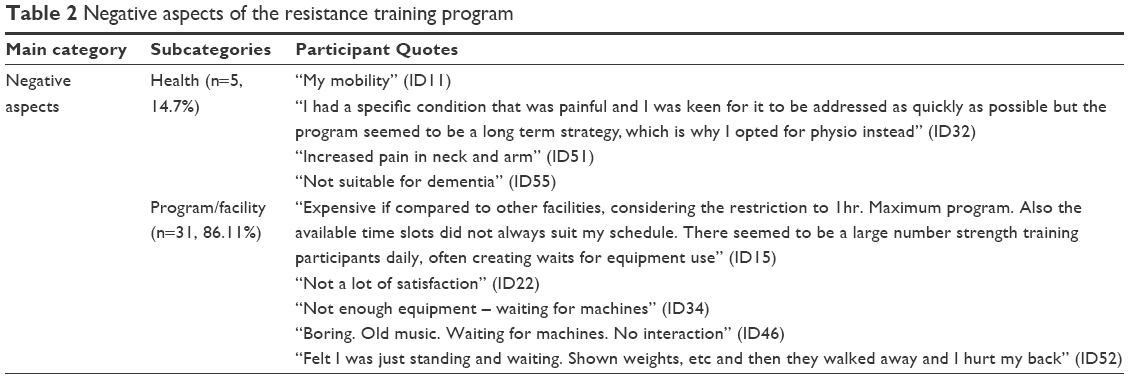 | Table 2 Negative aspects of the resistance training program |
The data were concept mapped to understand the flow of participation and withdrawal from the respondents (Figure 1). This showed that there were several reasons why withdrawal occurred and there are opportunities to have older people participate again in the future. The map demonstrates the importance of the staff and facility in maintaining participation for this age group.
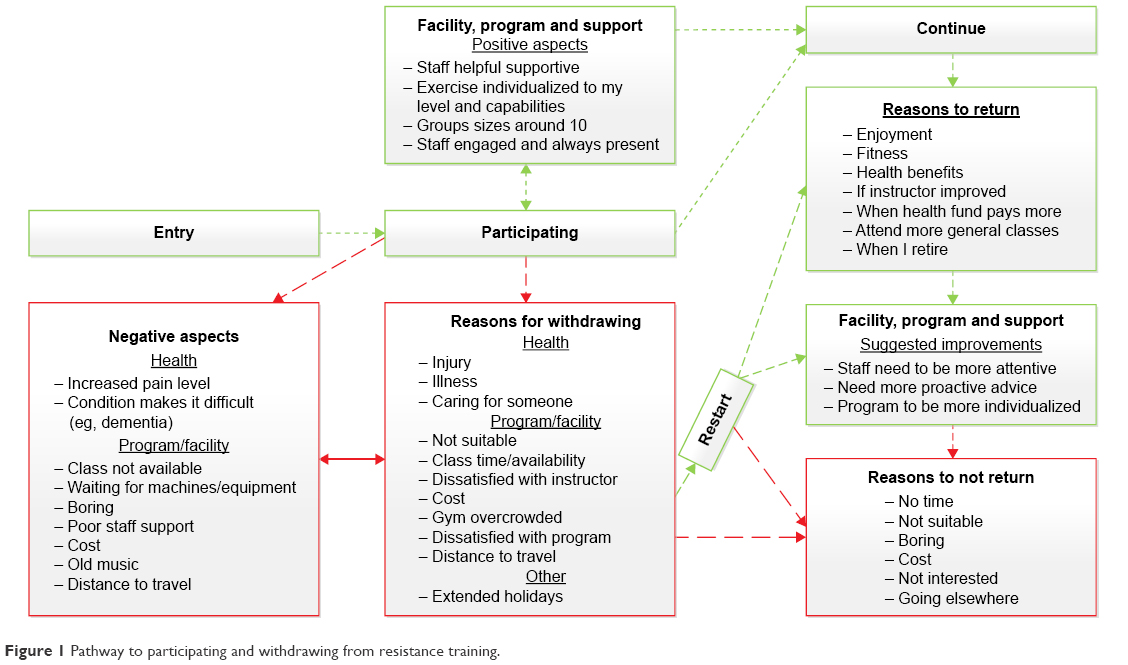 | Figure 1 Pathway to participating and withdrawing from resistance training. |
Returning to program in the future
When asked if they would “like” to return to the program in the future, 68.4% of the respondents (n=39) said that they would, 19.3% reported being unsure (n=11), and 12.3% were not interested (n=7) in participating again. The reasons given by those not interested in returning were time, not suitable, boring (waiting for machine and no interaction), cost, attending gym elsewhere, and not interested. The most common reasons why past participants said that they would “like” to return to a resistance training program in the future were enjoyment (26.3%, n=10), fitness (18.4%, n=7), gaining health benefits and exercises (13.2%, n=5 each), and if the instructor improved (7.9%, n=3). Other reasons provided by individual respondents included the following:
in the New Year when my Health Fund will pay more, I would like to join more general classes, possibly when I’m not working and I intend to.
Respondents were also asked if they would “be able” to return to the program at some point and around two thirds (67.3%, n=37) reported “yes” they would be able to, 21.8% were unsure (n=12), and 10.9% stated no (n=6). The reasons why respondents would return were similar to those described above, with additional reasons including: because I can or I am able to and if a class is available. Reasons given for not being able to return were the following: don’t want to, I’m active in other areas, not with this set up at the center, and time and cost factors.
Discussion
The respondents in this study stopped attending resistance training programs for a number of reasons. Most commonly reported reasons were the result of injury or illness, going away on holidays, and issues at the facility (eg, class not available including type, age range, and times; waiting for machines; and poor staff support). Previous research that explored the barriers preventing older people participating in resistance training and exercise, in general, also found injury and pain to be common reasons for nonparticipation, together with feeling too old and not being interested.16,17,30
It is unknown how many of the injuries occurred due to taking part in resistance training or for some other reason, such as falling downstairs on holiday. However, regardless of the reason and depending on the injury and also illness (which was the second most common response), it may be possible for the older person to still attend (either immediately following the injury or illness or after a period of time) but be given a modified program to accommodate any new exercise constraints associated with their injury or recovery. Illness for an older person can often make it difficult to bounce back and for some continuing with activities of daily living and living independently becomes challenging. Fitness center and other health professionals should be aware that this may occur and provide regular advice, support, and referral to the appropriate health professional. It is also recommended that facilities provide screening for past injuries to reduce the likelihood of previous injuries reoccurring.
Regular physical activity and resistance training for improving strength, if appropriately moderated, can assist the older person to return to better health and fitness at a faster rate.4,31 Indeed, national physical activity guidelines for older Australians recommend
older people who have stopped physical activity, or who are starting a new physical activity, should start at a level that is easily manageable and gradually build up the amount, type, and frequency of activity.32
This study did not explore whether it is already common practice for fitness centers/others running resistance programs to follow-up those who cease participation and encourage them back with a program designed to help them regain fitness after injury or illness. This warrants further research, especially the costs and benefits for both the centers and participants.
Holidays were the third most commonly reported reason for withdrawing from the resistance training program. Unlike people working full-time who receive 4 weeks annual leave a year (in Australia and less elsewhere), some older people have the option of holidaying for much longer periods of time. A proportion of older people in Australia are well known for taking “driving holidays” to the northern parts of Australia for up to 3–4 months each year to avoid the cold winters.33 Older people in the USA do something similar in moving to the southern states of the USA,33 and many British seniors have spent prolonged periods of time in Spain.34 It may be that the lengths of these long breaks make it difficult to recommence resistance training when settling back home; especially, if it was necessary for the older person to withdraw rather than suspend their program membership when they were away. If this is the case, one strategy to help would be for gymnasiums and fitness centers to consider flexibility with their memberships, allow long suspensions, and make a personalized phone call to the older person on their return to encourage them back to the program. Of note, over 65% of the people were keen to return to the program so a personalized phone call or written invitation may well be a means of easily getting these people to return.
Some of the participants also identified issues with the gymnasium or fitness center programs as being the reason(s) they stopped participating. These issues included distance to travel to the program, class times and availability not suitable, dissatisfaction with the instructor, the facility being overcrowded, and the program provided not being suitable. The majority of these issues can be addressed relatively easily. Older instructors are often more able to relate to this target group, and research has shown that using peer leaders (older instructors) can be beneficial.35–38 Using peer leaders could also provide a competitive point of difference for their business. There are obvious requirements for training and support for peer exercise trainers that would need to be considered. Session times are also important. Fitness facilities staff often put sessions for older people in off-peak times (late morning, middle of the day, and early afternoon) thinking older people can attend at any time. Yet, many older people have multiple commitments and interests such as looking after grandchildren, doing volunteer or paid work, and attending classes, and as a result, prefer sessions to be held earlier in the mornings or later in the afternoon.21,39 With the projected increase in the proportion of people aged >60 years in the forthcoming decades, businesses need to be flexible and consider the needs and preferences of this important and growing target group.
Limitations
This study had several limitations that need to be considered. The low-response rate to the questionnaire may limit the generalizability of the findings. Because of privacy reasons, we were not able to contact the participants directly to follow-up on their completion of the survey, to interview them as a form of member checking, or to explore their responses in more depth. Also, sections of the tool were nonvalidated because of this type of study not having been undertaken with this population previously; therefore, it was not possible to use a validated tool. The authors also had no knowledge about participants’ health and injury status prior to them commencing participation resistance training. Despite these limitations, this is the first study to actually look at a population of seniors who recently stopped attending a structured resistance training program of their own accord after having participated for a period, and we believe that it provides useful information for resistance training providers running programs for older people. The number of older people participating in the recommended minimum two resistance training sessions a week is currently fewer than one in six.7–9 This needs to increase so more older people can experience some of the many benefits that have been shown to be associated with resistance training. Providing those working in this area with as much information as possible about older people’s needs, preferences, and motivations is, therefore, essential if this needs to be achieved.
Conclusion
This study identified reasons why older people who had been participating in resistance training for a period of time ceased taking part. Injury, illness, holidays, and issues with the resistance training program, center, or staff were the most commonly reported reasons for stopping. To reduce the number of older people leaving resistance training programs, it is suggested that gymnasiums and fitness centers provide ongoing advice for prevention and return to training after injury and flexible programs and services (membership types) that accommodate older people’s life choices in retirement.
Acknowledgments
The authors would like to thank the Living Longer Living Stronger centers that participated and all of the past members who completed the questionnaires. We would also like to thank Bob Ziegler and Shirley Barnes, the consumer representatives for their input and perspectives on the project. This work was supported by a Healthway Research Project Grant (grant number 24208).
Disclosure
The authors report no conflicts of interest in this work.
References
Lange AK, Vanwanseele B, Fiatarone Singh MA. Strength training for treatment of osteoarthritis of the knee: a systematic review. Arthritis Rheum. 2008;59(10):1488–1494. | ||
Lee MJ, Kilbreath SL, Singh MF, Zeman B, Davis GM. Effect of progressive resistance training on muscle performance after chronic stroke. Med Sci Sports Exerc. 2010;42(1):23–34. | ||
Mikesky AE, Mazzuca SA, Brandt KD, Perkins SM, Damush T, Lane KA. Effects of strength training on the incidence and progression of knee osteoarthritis. Arthritis Rheum. 2006;55(5):690–699. | ||
Liu C, Latham N. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst Rev. 2009;(3):CD002759. | ||
Australian Government Department of Health. Australia’s physical activity and sedentary behaviour guidelines: recommendations for older Australians; 2014. Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines#chba. Accessed April 30, 2015. | ||
World Health Organization. Physical activity and older adults: recommended levels of physical activity for adults aged 65 and above; 2015. Available from: http://www.who.int/dietphysicalactivity/factsheet_olderadults/en/. Accessed April 30, 2015. | ||
Humphries B, Duncan MJ, Mummery WK. Prevalence and correlates of resistance training in a regional Australian population. Br J Sports Med. 2011;44(9):653–656. | ||
Mayer F, Scharhag-Rosenberger F, Carlsohn A, Cassel M, Müller S, Scharhag J. The intensity and effects of strength training in the elderly. Dtsch Ärztebl Intl. 2011;108(21):359–364. | ||
National Center for Health Statistics. Health, United States, 2014: With Special Feature on Adults Aged 55–64. Hyattsville, MD: National Center for Health Statistics; 2015. | ||
United Nations. World Population Ageing 2013. New York, NY: Department of Economic and Social Affairs, Population Division; 2013. | ||
Taylor AH, Cable NT, Faulkner G, Hillsdon M, Narici M, Van De Bij AK. Physical activity and older adults: a review of health benefits and the effectiveness of interventions. J Sports Sci. 2004;22(8):703–725. | ||
Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. 2006;174(6):801–809. | ||
Australian Bureau of Statistics. 4364.0.55.004 – Australian health survey: physical activity, 2011–2012. 2013. Available from: http://www.abs.gov.au/ausstats/[email protected]/Lookup/D4495467B7F7EB01CA257BAC0015F593?opendocument. Accessed June 5, 2015. | ||
Bennie JA, Pedisic Z, van Uffelen JG, et al. Pumping iron in Australia: prevalence, trends and sociodemographic correlates of muscle strengthening activity participation from a national sample of 195,926 Adults. PloS One. 2016;11(4):e0153225. | ||
Merom D, Pye V, Macniven R, et al. Prevalence and correlates of participation in fall prevention exercise/physical activity by older adults. Prev Med. 2012;55(6):613–617. | ||
Burton E, Farrier K, Lewin G, et al. Motivators and barriers for older people participating in resistance training: a systematic review. J Aging Phys Act. 2016;1–41. Epub 2016 Sep 06. | ||
Burton E, Lewin G, Pettigrew S, et al. Identifying motivators and barriers to older community-dwelling people participating in resistance training–a cross sectional study. J Sports Sci. 2016;1–10. Epub 2016 Aug 25. | ||
Henwood T, Tuckett A, Edelstein O, Bartlett H. Exercise in later life: the older adults’ perspective about resistance training. Ageing Soc. 2011;31(08):1330–1349. | ||
Keogh J, Rice J, Taylor D, Kilding A. Objective benefits, participant perceptions and retention rates of a New Zealand community-based, older-adult exercise programme. J Prim Health Care. 2014;6(2):114–122. | ||
Howe T, Rochester L, Neil F, Skelton D, Ballinger C. Exercise for improving balance in older people. Coch Database Syst Rev. 2001;(11):CD004963. | ||
Bopp M, Wilcox S, Oberrecht L, Kammermann S, McElmurray C. Correlates of strength training in older rural African American and Caucasian women. Women Health. 2004;40(1):1–20. | ||
Kleppinger A, Litt M, Kulldorff M, Unson C, Judge J. Health perceptions as predictors of exercise adherence in older women. Eur J Sport Sci.2003;3(4):1–15. | ||
Council on the Ageing. Living longer living stronger; 2016. Available from: http://www.lllswa.org.au/. Accessed November 17, 2016. | ||
Washburn R, McAuley E, Katula J, Mihalko S, Boileau R. The physical activity scale for the elderly (PASE): evidence for validity. J Clin Epidemiol. 1999;52(7):643–651. | ||
Washburn RA, Smith KW, Jette AM, Janney CA. The physical activity scale for the elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46(2):153–162. | ||
Krippendorff K. Content Analysis An Introduction to Its Methodology. 2nd ed. London, United Kingdom: Sage Publications; 2004. | ||
Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. | ||
Novak J, Canas A. Theoretical origins of concept maps, how to construct them, and uses in education. Reflect Educ. 2007;3(1):29–42. | ||
New England Research Institutes. PASE Physical Activity Scale for the Elderly .Administration and Scoring Instruction Manual. Watertown, MA: New England Research Institutes, Inc.; 1991. | ||
Hill AM, Hoffmann T, McPhail S, et al. Factors associated with older patients’ engagement in exercise after hospital discharge. Arch Phys Med Rehabil. 2011;92(9):1395–1403. | ||
Fiatarone MA, O’Neill EF, Ryan ND, et al. Exercise training and nutritional supplementation for physical frailty in very elderly people. N Engl J Med. 1994;330(25):1769–1775. | ||
Sims J, Hill K, Hunt S, Haralambous B. Physical activity recommendations for older Australians. Australas J Ageing. 2010;29(2):81–87. | ||
Onyx J, Leonard R. Australian grey nomads and American snowbirds: similarities and differences. J Tour Stud. 2005;16(1):61–68. | ||
Hardill I, Spradbery J, Arnold-Boakes A, Marrugat M. Severe health and social care issues among British migrants who retire to Spain. Ageing Soc. 2005;25:769–783. | ||
Dorgo S, King GA, Brickey GD. The application of peer mentoring to improve fitness in older adults. J Aging Phys Act. 2009;17(3):344–361. | ||
Dorgo S, Robinson KM, Bader J. The effectiveness of a peer-mentored older adult fitness program on perceived physical, mental, and social function. J Am Acad Nurse Pract. 2009;21(2):116–122. | ||
Iliffe S, Kendrick D, Morris R, et al. Multicentre cluster randomised trial comparing a community group exercise programme and home-based exercise with usual care for people aged 65 years and over in primary care. Health Technol Assess. 2014;18(49):1–105. | ||
Waters DL, Hale LA, Robertson L, Hale BA, Herbison P. Evaluation of a peer-led falls prevention program for older adults. Arch Phys Med Rehabil. 2011;92(10):1581–1586. | ||
Lin S-F, Lee J, Modeste N, Johnson E. Attitudes and beliefs predicting Taiwanese older adults’ intentions to attend strength and balance training programs. J Appl Gerontol. 2012;31(2):260–281. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.