Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
White Hair–Induced Increased Scalp Visibility: Clinical Implications for Hair Loss Evaluation and Hair Transplantation
Authors Park JH ![]()
Received 8 February 2026
Accepted for publication 4 May 2026
Published 21 May 2026 Volume 2026:19 602144
DOI https://doi.org/10.2147/CCID.S602144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Michela Starace
Jae Hyun Park
Department of Plastic Surgery, Dana Plastic Surgery Clinic, Seoul, South Korea
Correspondence: Jae Hyun Park, Department of plastic surgery, Dana Plastic Surgery Clinic, Seoul, South Korea, Tel +82-2-512-0922, Fax +82-2-512-0942, Email [email protected]
Abstract: White hair is a common physiological change with aging; however, in clinical practice, increased scalp visibility associated with white hair is frequently misinterpreted as progression of hair loss. Because white or non-pigmented hair lacks melanin, hair–scalp contrast is markedly reduced, and some shafts may appear poorly demarcated or even translucent under magnification. Consequently, the scalp may appear more exposed despite preserved hair density and shaft diameter, leading to a clinically meaningful visual illusion. This article highlights white hair–induced increased scalp visibility as a distinct and highly prevalent clinical phenomenon that can confound hair loss evaluation and hair transplantation planning. We discuss the optical basis of scalp show-through, the non-linear relationship between white hair proportion and perceived scalp visibility, and diagnostic pitfalls that may lead to overtreatment. We further analyze procedure-specific technical implications for hair transplantation, including follicular unit dissection in strip surgery (FUT) and harvesting/placement challenges in follicular unit excision (FUE). Finally, based on clinical experience, we present five core principles for dyeing strategy in patients with white hair. The observations presented herein are derived from clinical experience and representative cases; quantitative validation through standardized imaging and blinded assessments remains an area for future investigation.
Keywords: white hair, scalp visibility, scalp show-through, trichoscopy, folliscope, hair transplantation, FUT, FUE, East Asian hair
Introduction
Hair loss evaluation and treatment decisions have traditionally been based on objective parameters such as hair density, hair shaft diameter, and follicular unit composition.1,2 While this approach is pathophysiologically sound and effective for many patients, a substantial discrepancy is frequently observed between objective findings and patients’ subjective perception of hair loss in daily clinical practice.
A common presentation involves patients who complain that their hair appears thinner, their part line has widened, or their scalp has become increasingly visible, despite trichoscopic or folliscopic examinations demonstrating hair density and shaft diameter within normal age-related ranges.3 In such cases, patient anxiety is often significant, yet conventional frameworks for hair loss assessment fail to adequately explain the perceived change.
One important and underrecognized contributor to this discrepancy is the presence of white or non-pigmented hair. Hair graying results from the progressive loss of melanocyte function within the hair follicle, primarily driven by depletion of melanocyte stem cells in the bulge region and cumulative oxidative stress.4 Although white hair is a natural consequence of aging, its visual impact extends beyond a simple change in color. Because white hair lacks melanin, the contrast between the hair shaft and the scalp is reduced or lost, and in some cases the hair appears partially translucent. Consequently, even with an unchanged number of hair shafts, scalp visibility may increase markedly, creating the impression of worsening hair loss. (Figure 1)
 |
Figure 1 White hair–induced increased scalp visibility. Clinical photographs illustrating increased scalp visibility associated with a high proportion of white hair despite preserved hair density. |
This visual effect is particularly pronounced in areas such as the part line, vertex, and frontal hairline, where light incidence and hair orientation accentuate scalp show-through.5 As a result, patients may interpret increased scalp visibility as progression of alopecia, and clinicians may be inclined to recommend treatment or surgery based on appearance rather than structural change.
The purpose of this review is to define white hair–induced increased scalp visibility as a clinical phenomenon distinct from true alopecia and to systematically examine how this phenomenon influences hair loss assessment and hair transplantation planning, including diagnostic pitfalls, procedure-specific technical constraints, and practical dyeing strategies.
Optical Characteristics of White Hair and Mechanisms of Increased Scalp Visibility
White hair is not merely pigmented hair that has “lost color”; it exhibits fundamentally different optical properties. Pigmented hair absorbs light through melanin, creating strong contrast against the scalp and contributing to the perception of coverage and density. In contrast, white hair reflects or transmits light and tends to visually blend with the scalp.
Under trichoscopic and folliscopic examination, white hair often appears faint, poorly demarcated, or partially translucent—even at high magnification.3 (Figure 2) This limitation persists despite the use of magnifying loupes or optical enhancement, indicating that the phenomenon reflects a contrast-dependent visual constraint rather than insufficient resolution. In practical terms, white hair on a light-toned scalp may be near-invisible, and “transparent-appearing” white hairs may be functionally invisible in situ.
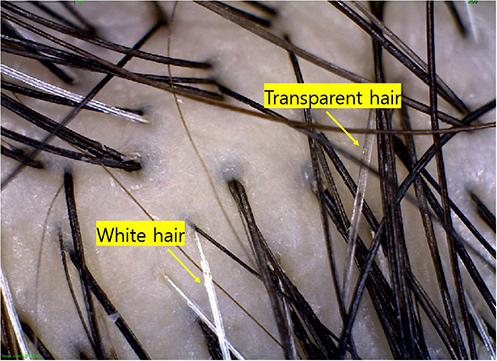 |
Figure 2 Trichoscopic and folliscopic appearance of white and transparent hair. High-magnification images demonstrating reduced contrast of white hair against the scalp and the presence of transparent-appearing hair shafts that are difficult to identify even under magnification. |
As a result, scalp show-through may become exaggerated despite preservation of hair density and shaft diameter. Therefore, increased scalp visibility in this setting should be understood primarily as an optical/perceptual phenomenon rather than a direct indicator of follicular miniaturization or reduced density.
Non-Linear Relationship Between White Hair Proportion and Perceived Scalp Visibility
Clinical observation suggests that the relationship between white hair proportion and perceived scalp visibility is non-linear. When white hair constitutes a small fraction of total hair (often below approximately 10%), scalp visibility rarely becomes a prominent concern.
As the proportion of white hair increases to approximately 15–20%, white hairs begin to intermix with pigmented hairs, disrupting the visual shielding effect of darker shafts. At this stage, scalp visibility is often perceived abruptly, and many patients interpret this change as sudden progression of hair loss. In this range, white hairs between pigmented hairs may be perceived as “empty spaces” or areas of hair loss.6
When white hair becomes the dominant component (approximately 60–70% or more), a different visual pattern emerges. Pigmented hairs become the minority and may be perceived as scattered dark strands within a predominantly light background. In some patients, this configuration results in reduced perception of scalp show-through compared with the intermediate stage. These observations suggest that perceived scalp visibility depends not only on the quantity of white hair but also on its distribution and contrast relationships.7
Diagnostic Pitfalls in Hair Loss Evaluation
White hair–induced increased scalp visibility represents a frequent source of diagnostic confusion. In daily practice, patients may present with complaints of severe hair loss despite objective assessments demonstrating preserved follicular density and normal shaft diameter.8 (Figure 3)
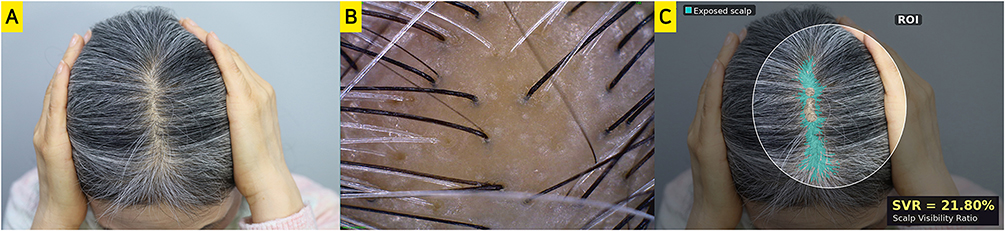 |
Figure 3 Representative case illustrating the assessment of scalp visibility using digital image analysis. A 60-year-old female patient presented with prominent scalp visibility along the part line despite preserved follicular density (~130 hairs/cm2) and shaft diameter (>90 μm) on folliscopic examination. (A) Original vertex photograph showing diffuse white hair with increased scalp show-through. (B) Folliscopic image (×14 magnification) confirming preserved follicular density and shaft diameter. (C) Semi-automated digital image analysis using HSV color segmentation. An elliptical region of interest (ROI, white outline) was defined over the vertex region. Exposed scalp pixels (cyan overlay) were identified based on empirically calibrated thresholds. The Scalp Visibility Ratio (SVR) was 21.80%. |
Digital Image-Based Analysis of Scalp Visibility
To provide an illustrative quantitative representation of scalp visibility, a digital image–based analysis was performed on standardized vertex photographs from a representative 60‑year‑old female patient who presented with prominent scalp show‑through along the part line despite preserved follicular density and shaft diameter (Figure 3A and B). A standardized elliptical Region of Interest (ROI) was defined along the mid-sagittal parting line to capture the area where scalp exposure is most prominent while minimizing peripheral distortion.
Within this ROI, the Scalp Visibility Ratio (SVR) was calculated using a Python-based image analysis pipeline (OpenCV). Images were converted to the HSV color space to separate chromatic information from luminance, enabling more stable identification of scalp regions under variable lighting conditions. Exposed scalp areas were identified using empirically defined thresholds and highlighted with a cyan overlay for visual clarity (Figure 3C).
The SVR was calculated as:
SVR (%) = (Pixel count of exposed scalp / Total pixel count within ROI) × 100
In the representative case, the SVR was 21.80%, demonstrating a substantial degree of visually apparent scalp exposure. This analysis is intended to provide a conceptual illustration of perceived scalp visibility rather than a validated diagnostic metric. Absolute SVR values may be influenced by individual variations in scalp pigmentation, hair curvature, and lighting conditions; therefore, this metric is best suited for within-patient comparative assessments rather than cross-patient diagnostic thresholds.
In such cases, reliance on visual impression alone may lead to misdiagnosis and unnecessary medical or surgical intervention. The discrepancy between subjective perception and objective findings can also strain the physician–patient relationship, particularly when the patient strongly believes that hair loss has progressed.
Accordingly, assessment of hair pigmentation and white hair distribution should be considered an integral component of hair loss evaluation, alongside density and caliber measurements. In selected cases, conservative management (including counseling and dyeing recommendations) may adequately address the patient’s primary concern.
Technical Implications of White Hair in Hair Transplantation
Strip Surgery (FUT)
In strip-based hair transplantation, accurate follicular unit dissection under stereomicroscopic magnification is essential for graft survival and consistent outcomes.9 When follicular units consist predominantly or exclusively of white hair, their boundaries may be extremely difficult to identify due to poor contrast with surrounding dermal tissue.
In practice, dyed hair shafts often serve as visual references for estimating follicular unit location, orientation, and size during dissection. Without dyeing, reliable dissection may be impractical. Furthermore, when patients desire preferential transplantation of pigmented hair, selective exclusion of white-hair grafts becomes technically unfeasible without preoperative dyeing. (Figure 4)
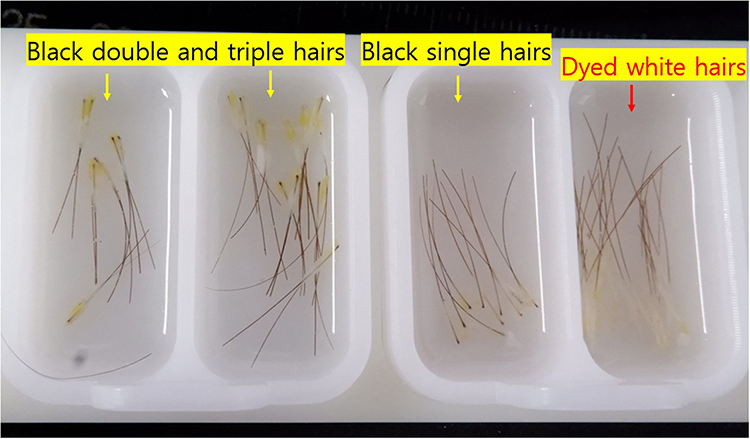 |
Figure 4 Follicular units dissected during strip surgery in a patient with a high proportion of white hair. When hair shafts are not dyed, follicular unit boundaries are extremely difficult to identify, making dissection highly challenging. In contrast, dyed hairs serve as visual references, allowing approximate identification of follicular unit borders and safer dissection. |
For these reasons, in FUT, dyeing should be regarded not as a cosmetic option but as a technical prerequisite in patients with a meaningful proportion of white hair.
Follicular Unit Excision (FUE)
In FUE, individual follicular units are selected and extracted directly by the surgeon.10 However, white hair often exhibits poor visibility on the scalp surface, increasing the risk of graft injury during punching and extraction (Supplementary Figure S1).
When selective transplantation of pigmented hair is intended, discrimination between pigmented and non-pigmented hairs must occur prior to or during extraction. Without dyeing, this distinction cannot be made reliably. Thus, even in FUE, dyeing may play a strategic role depending on surgical objectives.
Representative Case
A 62-year-old male patient underwent non-shaven FUE with transplantation of 1900 follicular units. There was almost no white hair in the frontal area, while approximately 15% white hair was present in the occipital donor area. The patient preferred preferential transplantation of pigmented hair; therefore, he was instructed not to dye his hair preoperatively. (Figure 5)
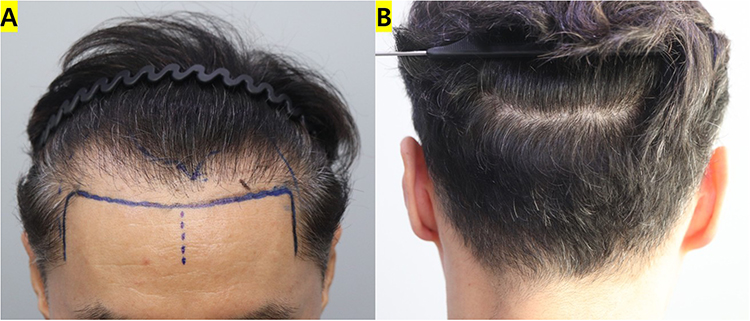 |
Figure 5 Representative case of selective transplantation of pigmented hair using non-shaven follicular unit excision (FUE). A 62-year-old male patient underwent non-shaven FUE (1900 follicular units). Approximately 15% white hair was present in the occipital donor area. The patient preferred preferential transplantation of pigmented hair; therefore, surgery was performed without dyeing. (A) Hairline design on the day of surgery. (B) Donor area on the day of surgery. |
Recipient-Site Considerations
At recipient sites, white hair may be difficult to distinguish from the scalp even under high-magnification loupes. This limitation may compromise graft handling and contribute to underestimation of surgical results during postoperative assessment. In addition, poor visibility may increase the risk of graft injury during placement. Therefore, if there is white hair at the recipient area, it is generally recommended to dye it beforehand.
Representative Case
A 43-year-old female patient presented for hairline correction combined with density enhancement in the part-line area. A very high proportion of white hair (approximately 70–80%) was present in both the recipient and donor areas. Surgery was performed using FUE after thorough preoperative dyeing 1–2 days before surgery. (Figure 6)
 |
Figure 6 Representative case of preoperative dyeing for surgery in a patient with a very high proportion of white hair. A 43-year-old female patient presented for hairline correction combined with part-line density enhancement. Approximately 70–80% white hair was present in both the recipient and donor areas. Surgery was performed using FUE after thorough preoperative dyeing 1–2 days before surgery. (A) Part-line area during consultation showing abundant white hair. (B) Occipital donor area during consultation. (C) Part-line area on the day of surgery after dyeing. (D) Hairline design area on the day of surgery after dyeing. |
Five Core Principles for Dyeing Strategy in Patients with White Hair
Dyeing strategies in patients with white hair cannot be reduced to a single algorithm because decisions depend on multiple interacting factors, including white hair proportion, distribution, surgical technique, recipient-site location, and patient preferences. Therefore, dyeing strategy should be planned in advance after systematically confirming the following items during consultation:
General Considerations in White Hair Dyeing Strategy
- How much white hair is present in the recipient area and donor area, respectively
- Whether the patient regularly dyes hair, and if so, how often
- Whether the patient desires preferential transplantation of pigmented hair only versus acceptance of white hair transplantation
- The proportion of white hair is also an important consideration when deciding on the surgical method: FUT versus FUE
- In FUE, dyeing strategy may vary according to graft number, white hair proportion, and shaved area
- In FUE, the harvesting field differs by non-shaven FUE, partial-shaven FUE, and full-shaven FUE, and should be considered accordingly
- Allergic contact dermatitis to hair dye must be checked in advance
Recipient Area
In the recipient area, dyeing is recommended in nearly all cases when white hair is present. Dyeing may be omitted when white hair is minimal (eg, <~5%); however, in most patients, white hair at the recipient site is difficult to identify even with magnification loupes and can increase the risk of graft injury during placement. Therefore, recipient-site dyeing should be understood as a measure to reduce technical error and graft damage rather than a purely cosmetic choice (Supplementary Figure S2).
Donor Area
In the donor area, dyeing strategy should be planned independently from the recipient area. The decision should be made by integrating surgical technique, white hair proportion, the patient’s dyeing habits, and the patient’s goals. Donor-site dyeing should be discussed and planned in advance and explained clearly to the patient (Supplementary Figures S3 and S4).
Timing and Color
Dyeing should be performed 1–2 days before surgery, and patients should be instructed carefully to ensure that dyeing is thorough up to approximately 1 mm above the scalp surface. Any sufficiently dark color is acceptable; a specific shade is generally not critical.
Selective Harvesting / Selective Transplantation
When the primary goal is selective harvesting and selective transplantation that excludes white hair (ie, transplanting pigmented hair only), the appropriate approach is to proceed with FUE without dyeing, because selection is based on visible shaft color and selective harvesting is feasible. In such selective transplantation scenarios, FUT is not appropriate, because excluding white hair grafts would effectively require discarding grafts during dissection and is impractical in real clinical settings.
Discussion
White hair–induced increased scalp visibility is frequently encountered in outpatient practice, especially among middle-aged and older patients whose proportion of white hair is actively increasing. Many patients present with the chief complaint that hair loss has “suddenly worsened”, yet objective evaluation reveals preserved density and shaft diameter. This phenomenon has likely been underrecognized because white hair has traditionally been regarded as a cosmetic sign of aging rather than an independent variable in hair loss assessment. The present review emphasizes that white hair should be treated as a confounder that can meaningfully alter both patient perception and clinician interpretation.
Clinically, alopecia is defined by reduced density, reduced shaft diameter, or both. In contrast, the patient’s complaint is often “my scalp is showing”, which represents an outcome of visual perception. White hair can increase scalp visibility without structural changes, and therefore scalp show-through should not automatically be equated with alopecia progression.5 In real practice, evaluation often begins with visual impression, and even modest changes in contrast can be interpreted as major progression. As white hair increases into an intermediate range (approximately 15–20%), it intermixes with pigmented hair and can be perceived as empty spaces—an optical configuration that readily prompts the perception of worsening hair loss. Conversely, when white hair becomes dominant (approximately 60–70% or more), the “empty space” illusion may diminish, highlighting that perceived visibility is not linearly proportional to white hair percentage.
Beyond perception, white hair influences hair transplantation through technical feasibility. In FUT, dissection depends on identifying follicular unit boundaries, which are difficult to define when shafts are predominantly white. In FUE, visibility limitations affect harvesting accuracy and recipient-site placement. Dyeing strategy must reflect surgical goals—particularly when selective transplantation of pigmented hair is intended.
The clinical impact of white hair–induced increased scalp visibility may be particularly pronounced in East Asian patients. East Asian hair is generally characterized by a high proportion of dark, terminal hair shafts combined with relatively light scalp skin, resulting in strong baseline hair–scalp contrast.11 This contrast contributes to the perception of dense hair coverage in younger individuals but becomes abruptly diminished as white hair emerges. Even a modest increase in the proportion of white hair may lead to a disproportionate increase in perceived scalp visibility compared with populations with lighter baseline hair color. Cultural and aesthetic sensitivity to part-line width and scalp show-through may further amplify patient concern in this population.
Recognizing this phenomenon can prevent overtreatment, reduce unnecessary surgery, and improve counseling. In many cases, conservative management such as dyeing may adequately address the primary complaint. When surgery is pursued, planning based on the five principles described above helps maximize technical precision and patient satisfaction.
Limitations
This review is based on clinical observation and representative cases. The digital image–based scalp visibility analysis presented in this study was intended as an illustrative adjunct rather than a validated diagnostic tool. The calculated SVR was derived from representative clinical images and was not designed to define universal cutoff values or diagnostic thresholds. Inter-individual variations in hair color, shaft curvature, scalp pigmentation, lighting conditions, and photographic settings may influence absolute values. Future research using standardized imaging protocols, objective scalp visibility metrics, and blinded assessments would strengthen the generalizability of these observations.
Conclusion
White hair–induced increased scalp visibility is a common, clinically significant phenomenon that can lead to overestimation of hair loss severity and misdirected management decisions. The reduced contrast between non-pigmented hair shafts and the underlying scalp creates a visual illusion of decreased density, even when follicular density and shaft diameter are preserved. This phenomenon is especially relevant in East Asian patients, where high baseline hair–scalp contrast amplifies the perceptual impact of emerging white hair. Understanding the optical basis of this phenomenon, incorporating hair pigmentation assessment into routine evaluation, and applying strategic dyeing principles in surgical planning are essential for rational, patient-centered care. We recommend that hair color and white hair distribution be routinely documented as part of comprehensive hair loss evaluation.
AI Use Disclosure
Artificial intelligence tools were used solely to assist with language editing and manuscript organization. The scientific content, design concepts, and interpretations were developed and verified by the author.
Data Sharing Statement
The data supporting the findings of this study are available within the article and its figures. The Python/OpenCV-based image analysis pipeline used to compute the Scalp Visibility Ratio (SVR) and additional de-identified clinical data are available from the corresponding author (Jae Hyun Park) upon reasonable request. Original medical records and identifiable patient photographs cannot be shared publicly owing to patient privacy and confidentiality obligations.
Patient Consent for Publication
Written informed consent was obtained from all patients for the publication of clinical information and accompanying images.
Funding
No funding was received for this article.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Sinclair R. Diffuse hair loss. Int J Dermatol. 1999;38(Suppl 1):8–9. doi:10.1046/j.1365-4362.1999.00003.x
2. Olsen EA. Female pattern hair loss. J Am Acad Dermatol. 2001;45(3 Suppl):S70–S80. doi:10.1067/mjd.2001.117426
3. Rakowska A, Slowinska M, Kowalska-Oledzka E, Rudnicka L. Trichoscopy of the hair and scalp: practical tips. Dermatol Clin. 2013;31(4):617–630.
4. Tobin DJ. The aging hair follicle pigmentation system. Int J Trichol. 2009;1(2):83–93. doi:10.4103/0974-7753.58550
5. Park JH. See-through scalp appearance. Int J Dermatol. 2022;61(9):1165–1167. doi:10.1111/ijd.16118
6. Daulatabad D, Singal A, Grover C, Chhillar N. Clinical profile and epidemiology of premature canities. Indian J Dermatol Venereol Leprol. 2016;82(2):169–172. doi:10.4103/0378-6323.168911
7. Trüeb RM. Aging of hair. J Cosmet Dermatol. 2005;4(2):60–72. doi:10.1111/j.1473-2165.2005.40203.x
8. Shapiro J. Clinical practice. Hair loss in women. N Engl J Med. 2007;357(16):1620–1630. doi:10.1056/NEJMcp072110
9. Bernstein RM, Rassman WR. Follicular unit transplantation. Dermatol Surg. 1995;21(9):771–784. doi:10.1016/1076-0512(94)00060-4
10. Cole JP. The anatomy of the follicular unit and follicular unit transplantation. Facial Plast Surg Clin North Am. 2013;21(3):379–391.
11. Leerunyakul K, Suchonwanit P. Asian hair: a review of structures, properties, and distinctive disorders. Clin Cosmet Invest Dermatol. 2020;13:309–318. doi:10.2147/CCID.S247390
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.