Back to Journals » Patient Preference and Adherence » Volume 10
What should be the patient's preference regarding the choice of hospital in the case of radical cystectomy? Evaluation of early complications after open radical cystectomy in a medium and high volume setting in one hospital
Authors Mani J, Vallo S, Brandt MP, Gust KM, Bartsch C, Daechert J, Tsaur I, Bartsch G, Haferkamp A
Received 27 December 2015
Accepted for publication 11 April 2016
Published 28 October 2016 Volume 2016:10 Pages 2181—2187
DOI https://doi.org/10.2147/PPA.S103217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Jens Mani,1 Stefan Vallo,1 Maximilian P Brandt,1 Kilian M Gust,1 Claudia Bartsch,1 Johannes Daechert,1 Igor Tsaur,1 Georg Bartsch,2,* Axel Haferkamp1,*
1Department of Urology, Goethe University Hospital, Frankfurt am Main, 2Department of Urology, Johannes Gutenberg University Hospital Mainz, Mainz, Germany
*These authors contributed equally to this work
Purpose: This study compares early complications after cystectomy and urinary diversion (UD) stratified by the surgical focus and case load of two different department chairpersons in a single institution in two time periods. Creating clear data about complications that can affect the quality of life is an important tool for patients to decide whether and where to perform this extensive surgery.
Hypothesis: A team of surgeons with a clear focus on pelvic surgery leads to lower complication rates in radical cystectomy.
Materials and methods: Radical cystectomy was performed in two separate time periods under the patronage of two different chairmen in the same university hospital. The patient data were analyzed retrospectively and the complications 30 days after surgery were assessed using the Clavien–Dindo classification.
Results: Statistical analysis showed a significant difference in the severity of complications between the two time periods, A and B, in total (P<0.001). When placing patients into subgroups, significantly more complications in period A were also seen concerning sex (male, P<0.001; female, P=0.003), age (<70 years, P<0.001; >70 years, P≤0.001) tumor grade (low grade, P<0.001; high grade, P≤0.001), and UD (ileal conduit, P<0.001; neobladder, P<0.001). In a multivariable analysis, age (P=0.031) and type of UD (P=0.028) were determined as independent predictors for complications in period A. When joining the two periods together, the type of UD (P=0.0417), age (P=0.041), and the time periods (A/B) (P<0.001) show a significant association with the presence of complications.
Conclusion: This study compares for the first time surgical complications in two time periods with different case load and surgical focus in one department. Categorization shows that patients should prefer radical cystectomy in centers of excellence or a high-volume hospital in order to keep complications at the lowest possible level and thus have the highest benefit for oncologic outcome and quality of life.
Keywords: Clavien–Dindo classification, early complications, high-volume period, low-volume period, radical cystectomy, urinary diversion, UD
Introduction
Bladder cancer is the second most common malignant urogenital tumor.1 Open radical cystectomy is the gold standard of treatment for patients with muscle-invasive bladder cancer. Radical cystectomy includes radical surgery on the urinary tract and lymph nodes. For creation of urinary diversion for the conduit, the surgeon takes about 20 cm of intestine/bowel; for neobladder the surgeon needs to take 60 cm of bowel/intestine on order to create the new bladder. So for each surgery a different amount of intestine is needed to create the new urinary diversion. Even though radical cystectomy and UD represent well-established open surgical approaches, they are still associated with significant perioperative morbidity (49%–68%) and notable perioperative mortality rates (1.5%–6.9%).2–6
Numerous studies have demonstrated an inverse relationship between surgeon volume and postoperative mortality for radical cystectomy.7–11 Currently, limited data exists showing the impact of hospital volume on the morbidity of radical cystectomy,10 even though postoperative complications are potentially responsible for a substantially large portion of the burden of bladder cancer patients.
Information about key performance markers like complications are also important factors for patients for treatment decision making and selection of the proper institution, especially for an extensive surgery like cystectomy.12
However, surgical expertise and focus, and thus the quality of surgery in a department, are prone to changes, especially through transition of leading authority.
For the first time, this study directly and objectively compares and analyses all early (30 days or less) complications after open radical cystectomy and UD in a university hospital before and after transition from medium-to high-volume centers because of a change of surgical focus. Our hypothesis is that this change of surgical focus leads to higher quality and thus lower complication rates.
Materials and methods
From January 1989 until December 2013, 404 patients underwent open radical cystectomy at the Department of Urology, Goethe-University Hospital Frankfurt am Main, Germany. Two time periods were defined based on a change of chairmanship in the department in April 2010. The type of UD performed in each period was determined by patient–surgeon consultation. Orthotopic diversion is always considered the gold standard and was applied when contraindications were ruled out.13
The patient data was retrospectively evaluated using the hospital information system Orbis (Agfa Healthcare, Bonn, Germany). Patient medical records, including inpatient notes, hospital discharge letters, outpatient notes and letters, hospital readmission records, and personal communications were extracted out of the Orbis database and all inpatient and post-discharge complications were recorded. All complications within 30 days of surgery were considered related to the radical cystectomy procedure and graded by three independent reviewers according to the 2004 Clavien–Dindo grading system (Table 1). The reviewers were blinded to all patient demographics, operative variables, and type of UD performed. Any discrepancies in grading caused reevaluation of the medical record until a consensus in grading was reached. The investigation was approved by the Human Research Ethics Committee, University of Frankfurt, Germany (Project 19/14). Information about the study purpose was conveyed to the patients by letter and written consent was obtained to use anonymous data for research purposes.
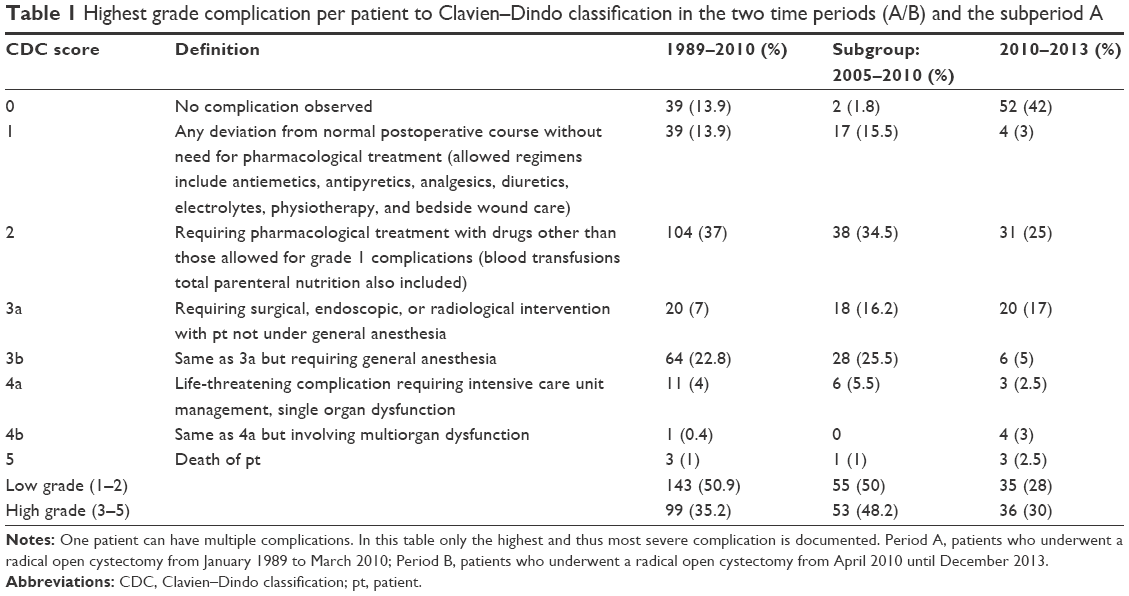 | Table 1 Highest grade complication per patient to Clavien–Dindo classification in the two time periods (A/B) and the subperiod A |
Statistical analysis was performed using the statistical program BiAS 10.04. (BiAS for Windows, EPSiLON-Verlag, Frankfurt am Main, Germany) Kruskal–Wallis test, chi-square contingency table, and chi-square test were used for statistical correlation analysis. Multivariable logistic regression analysis, including influencing factors like age, sex, type of UD, and tumor stage were performed to identify variables significantly associated with the presence and severity of complications. P-values of <0.05 were considered significant.
Results
After statistical evaluation of the university hospital database, period A, which included 281 patients with radical open cystectomy from January 1989 to March 2010 (average 13.4/year), was identified as the medium-volume period. The time period B with 123 operated patients from April 2010 until December 2013 (average 35.1/year) was identified as the high-volume period.10 The total average number of cystectomies from 1989 to 2013 was 16.8 (high-volume per definition10). The two periods were comparable in terms of sex distribution (Table 2). According to epidemiological data of bladder carcinoma, the majority of patients were males in both periods (A vs B; 81% vs 75%). The mean age of the patients at the time of surgery was comparable with 66 years (range 34–86 years) in period A and 67.5 years (range 30–88 years) in period B. However, when defining a cutoff age of 70 years, a significantly larger proportion of younger patients (<70 years) was allocated in period A (P=0.010). The Eastern Cooperative Oncology Group (ECOG) score and the ratio between organ-confined and locally advanced disease demonstrated the higher complexity of cases in period B. Significantly more patients with ECOG score >2 underwent surgery in period B (37.7% vs 20.2% in period A) (P=0.001). Furthermore, a distinctly higher percentage of patients with locally advanced disease was evident in period B (50.5% vs 44% in period A) (P=0.301). A distinctly higher percentage of positive lymph node patients were noticeable in period B (34.3% vs 27.9% in period A) (P=0.168) (Table 2).
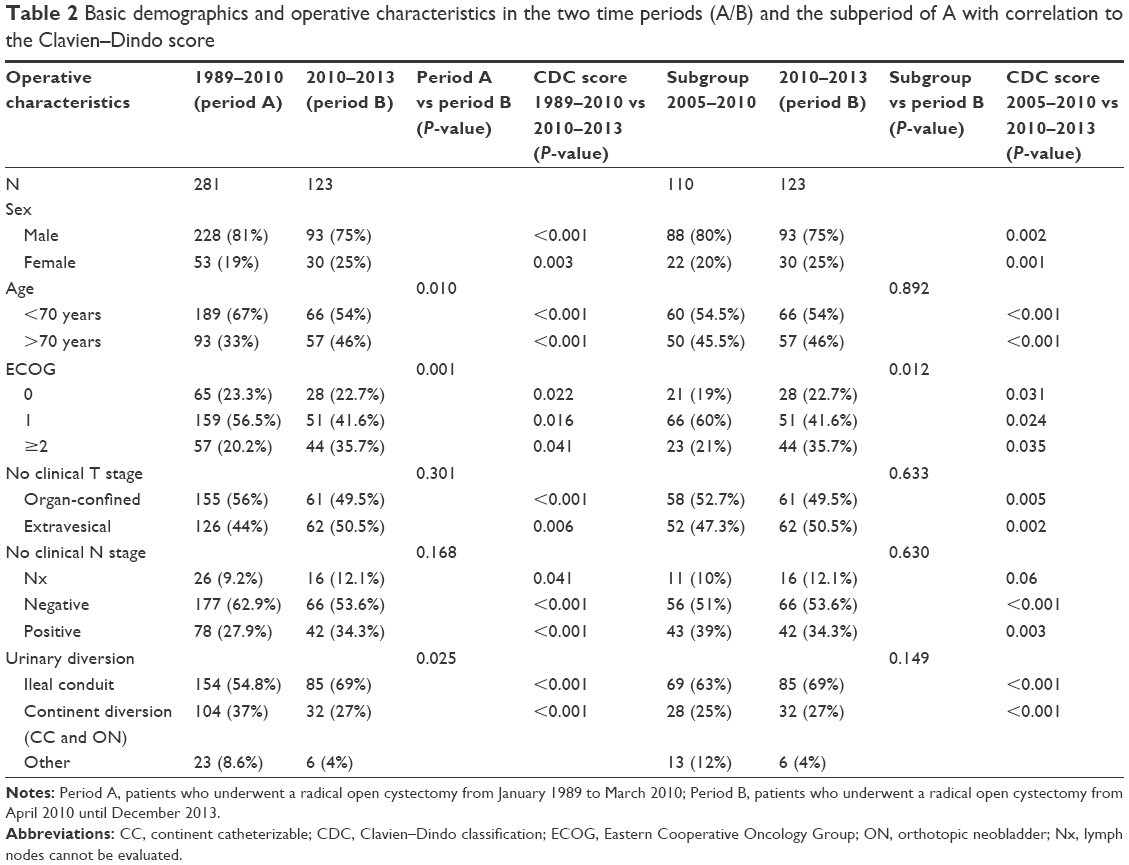 | Table 2 Basic demographics and operative characteristics in the two time periods (A/B) and the subperiod of A with correlation to the Clavien–Dindo score |
The higher comorbidity rates in cohort B results in a significantly higher use of incontinent diversions (P=0.025). Continent diversion (continent cutaneous diversions and orthotopic neobladder) was performed in 37% (104 of 281) of cases in period A and 27% (32 of 123) of cases in period B. Ileal conduit was performed in 54.8% (154 of 281) of patients in period A and 69% (85 of 123) in period B. Alternative diversions were performed (ureterocutaneostomy, transureterostomy, percutaneous nephrostomy, etc) in 8.6% (23 of 281) in period A and 4% (six of 123) in period B (Table 2).
A total number of 21 surgeons performed radical cystectomies in time period A. Five surgeons were documented in period B. The mean amount of radical cystectomies performed by each surgeon was 13.4 (range 1–39) in period A and 24.6 (range 4–53) in period B.
There were no reported intraoperative deaths in both time periods.
Overall, 86.1% (242 of 281) of patients suffered one or more early complication in period A and 58% (71 of 123) in period B (Table 1) (P<0.001). Altogether, 670 complications were documented in period A (range 1–7) and 150 complications in period B (range 1–7). A mean of 2.76 (standard deviation ±1.55) complications in period A and 2.14 (standard deviation ±1.32) in period B per patient was noticeable (P=0.024).
In period A, 45.9% (111 of 242) of patients revealed one complication and 21.1% (51 of 242) of patients had two complications (Table 1). The majority of patients in period B (39.4% [28 of 71]) suffered from one complication. Thirty-one percent (22 of 71) of cases had two complications (Table 1).
The distribution of complications in periods A and B is listed in Table 1. Median estimated blood loss was 1,100 mL (range 300–4,000 mL) in period A and 800 mL in period B (range 400–2,500 mL) (P<0.001). Blood transfusion rate in period A was 71.5% (n=200) and 32% (n=40) in period B (P<0.001).
To note, grade 2 complication includes blood transfusion. There are patients who are grouped into grade 2 complication exclusively only because of a low-volume of blood transfusion (1–2 red blood cell concentrate). Rates are n=12 (11.5% of grade 2) for period B and n=15 (48% of grade 2) for period A.
Statistical analysis shows a significant difference in severity of complications between periods A and B in total (P<0.001 [Table 2]). When placing patients into categories, significantly more complications in period A were also seen concerning sex (male, P<0.001; female, P=0.003), age (<70, P<0.001; >70, P<0.001), ECOG performance status (0, P=0.022; 1, P=0.016; ≥2, P=0.041), tumor stage (organ confined, P<0.001; extravesical, P<0.006), and UD (ileal conduit, P<0.001; continent diversion, P<0.001) (Table 2).
We created a subgroup in period A in order to compare the most recent and technically advanced time period (2005 until 2010) of period A with B. In subgroup A, we see 1.8% of patients with no complications and an almost equal distribution of low- (50%) and high-grade (48.2%) complications (Table 1). Only the ECOG distribution shows significant differences (P=0.012) in comparison to period B, but the categorical comparison presents significant variation of complications in nearly every category except stage Nx (P=0.06) (Table 2).
An intraperiodical analysis revealed a statistical relationship between both type of UDs (P=0.002), ECOG performance status (P=0.024), and age (P=0.008) to complication score in period A. Whereas no significant relationship was detected for sex (P=0.801) and tumor stage (P=0.711) in period A. In period B, on the other hand, generally no statistical relationship was detected concerning UD (P=0.987), tumor stage (P=0.440), age (P=0.539), ECOG performance status (P=0.672), and sex (P=0.268) (Table 3).
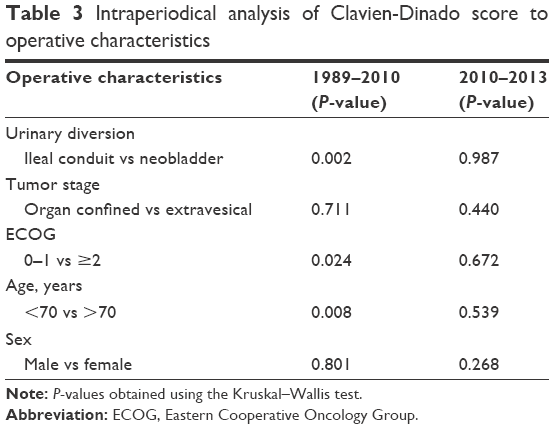 | Table 3 Intraperiodical analysis of Clavien-Dinado score to operative characteristics |
On multivariable analyses, age (P=0.037), ECOG performance status (P=0.034), and type of UD (P=0.022) maintained an association with the presence of complications in period A. No particular association with complications could be detected in period B regarding age, sex, ECOG performance status, type of UD, and tumor stage. When joining the two periods together for multivariable analysis, the type of UD (P=0.038), ECOG performance status (P=0.033), age (P=0.042), and the time period (period A/ B) (P<0.001) showed a significant association with the presence of complications.
Discussion
Radical cystectomy and UD is the most complex standardized surgical procedure in the field of urology.14 Accurate reporting of postoperative complications is important for exact patient counseling, combined modality treatment planning, clinical trial design, assessment of surgical success, and perioperative patient education.14 The surgical morbidity after radical cystectomy varies in different studies from 20% to 64%.3,15–20
For a long time, these complications were not uniformly graded. Estimated blood loss, operative time, perioperative deaths, readmission rates, reoperation rates, or intensive care stays were defined in different studies as an endpoint.15 Consequently, it was difficult to compare the data of these studies. But when using the Clavien–Dindo classification, a validated, strict, and straightforward grading guideline, the data can be compared and rated.2,4
So far, no study has directly compared the different periods of surgical expertise and case volumes in the same hospital. In the mentioned setting, the structural, social, and demographic circumstances remained the same and only became subject to the changing times. But at the Department of Urology of Goethe University Hospital, Frankfurt, Germany, the surgical focus of a urological academic center has changed under a new chairman, now with an emphasis on oncology and pelvic surgery. Thus, the center changed from a medium cystectomy volume center to a high cystectomy volume center. The main difference in our study after evaluation of our data was that, period A could be considered to be a medium-volume period and period B could be considered a high-volume period.10
Of course, over time, the surgical techniques as well as the perioperative conditions have been optimized, but over the last decade there were no major changes in the technique of performing open surgery.21,22 The initial pioneering work in radical cystectomy may be a reason why the quality of the period A stands worse in comparison to period B. It has been proven that the implementation of any new urological surgical method requires a learning curve.23 However, after standardization and refinement of technique, this usually results in a plateau phase with stable results on an international expert-derived competency level with higher amount of patients with no complications,24 which was not the case here, especially as the number of cases remained at a medium-volume level. Also the analysis of the most recent years of period A did not show improvement in the amount and severity of the complications. Paradoxically, this subperiod even showed the highest amount of high-grade complications.
Period B, however, showed concerning quantity and quality characteristics of a high-volume hospital, with complication rates comparable to those of other international high-volume hospitals. The high-volume period B showed significantly better rates in every examined subcategory like age, sex, ECOG performance status, tumor stage, and UD. These parameters have been identified as independent predictors of severity of complications in other high-volume settings.4
Previous studies have compared cystectomy in different hospitals with the Clavien–Dindo grading of complications. Here, differences especially between low- and high-volume hospitals in the total number and the severity of complications were evident.25
Remarkable in our cohort was the total blood transfusion rate of 71.5% in period A and 32% in period B. Other studies have already shown great discrepancy in total transfusion rates after cystectomy from 30%26 to 69%;27 a striking fact that is represented by the high incidence of grade 2 complications, which is also defined through the supportive postoperative blood transfusion. We saw up to 48% of grade 2 complications in period A and 11.5% of grade 2 complication in period B only due to blood transfusion. Obviously, in this low-grade section, we also observed the most significant differences between periods A and B complications, assuming a shift from no to low complication, especially in period A. But frankly, period A has a significantly higher estimated blood loss. Thus, in this case, the high transfusion rate can not only be biased through the action of the assisting anesthesia department, who often manage the short postoperative phase and have their own changing transfusion policies,28 but can be considered a complication resulting from the higher estimated blood loss.
The Clavien system for classifying surgical complications was originally designed for hepatobiliary surgery and has subsequently been validated in a general surgery population.29 This grading system has been modified by the Memorial Sloan Kettering Cancer Center for the radical cystectomy procedure, which defines the type, incidence, and severity of early postoperative morbidities after radical cystectomy using ten critical reporting elements.4 In our opinion, especially the low-grade complications need some alteration and further customization to open radical cystectomy because the current classification tends to overinterpret the complications. Minor grade 1 complications, like opening of a previously placed gastrostomy tube or a temporary placement of a nasogastric tube, represent essential marginal invasive interventions, which also may be essential to guarantee a further normal postoperative course, just like application of antiemetics, antipyretics, and diuretics. These procedures can hardly be considered complications and should be relativized because usually they do not further affect the quality of life.
Otherwise, through the alleged overestimation of complications, the patient might be misled and guided to alternative, but only potentially curing methods, like radiotherapy, who report complications respectively toxicity in only 4.7%–29%.30–32 This is much less than stated in radical cystectomy complication evaluation studies (49%–68%).2–6
As our data suggests, in any case, it is of crucial importance to disclose key performance markers, like surgical volume of the center together with its rate of surgical complications, to provide information for the patient’s decision making for the optimal therapy option. But physicians and patients should be aware that these key performance markers are naturally subject to change bidirectionally, even in the same hospital, for example, like in our case, due to increased expertise through change of chairmanship.
The vast majority of surgical patients clearly want to get adequate preoperative education about their illness and the planned treatment along with the possible complications affecting the oncological outcome and the quality of life.
In general, the relationship between physicians and patients has undergone important changes, and the current emancipation of patients should lead to a real, open, truthful, and even partnership in medical decision making.33
Conclusion
This is the first study to directly compare complications after radical cystectomy using the Clavien–Dindo classification in two time periods with different surgical focus, and thus volume, in one hospital. Surgical expertise in a department is prone to changes, especially through transition of leading authority. Categorization shows that patients should prefer having a radical cystectomy performed in a center of excellence or high-volume hospital. Surgical expertise and volume information must be accessible to the referring physicians and patients for the sake of perioperative patient education and decision making.
Disclosure
The authors report no conflicts of interest in this work.
References
Ploeg M, Aben KK, Kiemeney LA. The present and future burden of urinary bladder cancer in the world. World J Urol. 2009;27(3):289–293. | ||
Hautmann RE, de Petriconi RC, Volkmer BG. Lessons learned from 1,000 neobladders: the 90-day complication rate. J Urol. 2010;184(3):990–994; quiz 1235. | ||
Novara G, De Marco V, Aragona M, et al. Complications and mortality after radical cystectomy for bladder transitional cell cancer. J Urol. 2009;182(3):914–921. | ||
Shabsigh A, Korets R, Vora KC, et al. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology. Eur Urol. 2009;55(1):164–174. | ||
Stimson CJ, Chang SS, Barocas DA, et al. Early and late perioperative outcomes following radical cystectomy: 90-day readmissions, morbidity and mortality in a contemporary series. J Urol. 2010;184(4): 1296–1300. | ||
Takada N, Abe T, Shinohara N, et al. Peri-operative morbidity and mortality related to radical cystectomy: a multi-institutional retrospective study in Japan. BJU Int. 2012;110(11 Pt B):E756–E764. | ||
Begg CB, Cramer LD, Hoskins WJ, Brennan MF. Impact of hospital volume on operative mortality for major cancer surgery. JAMA. 1998;280(20):1747–1751. | ||
Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346(15):1128–1137. | ||
Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume and operative mortality in the United States. N Engl J Med. 2003;349(22):2117–2127. | ||
Mayer EK, Bottle A, Aylin P, Darzi AW, Athanasiou T, Vale JA. The volume-outcome relationship for radical cystectomy in England: an analysis of outcomes other than mortality. BJU Int. 2011;108(8 Pt 2):E258–E265. | ||
McCabe JE, Jibawi A, Javle P. Defining the minimum hospital case-load to achieve optimum outcomes in radical cystectomy. BJU Int. 2005;96(6):806–810. | ||
Davison BJ, Breckon E. Factors influencing treatment decision making and information preferences of prostate cancer patients on active surveillance. Patient Educ Couns. 2012;87(3):369–374. | ||
Daneshmand S, Bartsch G. Improving selection of appropriate urinary diversion following radical cystectomy for bladder cancer. Expert Rev Anticancer Ther. 2011;11(6):941–948. | ||
Hautmann RE, Hautmann SH, Hautmann O. Complications associated with urinary diversion. Nat Rev Urol. 2011;8(12):667–677. | ||
Donat SM. Standards for surgical complication reporting in urologic oncology: time for a change. Urology. 2007;69(2):221–225. | ||
Knap MM, Lundbeck F, Overgaard J. Early and late treatment-related morbidity following radical cystectomy. Scand J Urol Nephrol. 2004;38(2):153–160. | ||
Novotny V, Hakenberg OW, Wiessner D, et al. Perioperative complications of radical cystectomy in a contemporary series. Eur Urol. 2007;51(2):397–401; discussion 401–402. | ||
Parekh DJ, Gilbert WB, Koch MO, Smith JA Jr. Continent urinary reconstruction versus ileal conduit: a contemporary single-institution comparison of perioperative morbidity and mortality. Urology. 2000; 55(6):852–855. | ||
Ramani VA, Bromage SJ, Clarke NW. A contemporary standard for morbidity and outcome after radical cystectomy. BJU Int. 2009;104(5):628–632. | ||
Skinner DG, Crawford ED, Kaufman JJ. Complications of radical cystectomy for carcinoma of the bladder. J Urol. 1980;123(5): 640–643. | ||
Rogers E, Scardino PT. A simple ileal substitute bladder after radical cystectomy: experience with a modification of the Studer pouch. J Urol. 1995;153(5):1432–1438. | ||
Montie JE. Textbook of Operative Urology. Philadelphia, PA: Saunders; 1996. | ||
Abboudi H, Khan MS, Guru KA, et al. Learning curves for urological procedures: a systematic review. BJU Int. 2014;114(4): 617–629. | ||
Khan N, Abboudi H, Khan MS, Dasgupta P, Ahmed K. Measuring the surgical ‘learning curve’: methods, variables and competency. BJU Int. 2014;113(3):504–508. | ||
Brunken C, Tauber S, Wohlmuth P. Morbidität, Mortalität und Gesamtüberleben nach radikaler Zystektomie. Abgleich eigener Daten mit der Literatur und einem Normogramm [Morbidity, mortality, and overall survival after radical cystectomy: comparison of single-center results with the literature and a nomogram]. Urologe A. 2014;53(3):362, 364–367. | ||
Chang SS, Smith JA Jr, Wells N, Peterson M, Kovach B, Cookson MS. Estimated blood loss and transfusion requirements of radical cystectomy. J Urol. 2001;166(6):2151–2154. | ||
Abel EJ, Linder BJ, Bauman TM, et al. Perioperative blood transfusion and radical cystectomy: does timing of transfusion affect bladder cancer mortality? Eur Urol. 2014;66(6):1139–1147. | ||
Meier J, Meininger D, Zacharowski K. Patient blood management: from blood-sparing techniques to the rationale use of blood products. Curr Opin Anaesthesiol. 2012;25(1):48–49. | ||
Morgan M, Smith N, Thomas K, Murphy DG. Is Clavien the new standard for reporting urological complications? BJU Int. 2009;104(4):434–436. | ||
Esco Baron R, Baquedano Baquedano JE. Complicaciones de la radioterapia del cáncer vesical invasor: efectos agudos y tardíos. Evaluación del daño: escalas de la RTOG/EORTC, SOMA/LENT [Complications of radiotherapy for invasive bladder cancer: acute and chronic effects. Method of evaluation: measurement by RTOG/EORTC, SOMA/LENT]. Arch Esp Urol. 1999;52(6):675–683. | ||
Henningsohn L, Wijkstrom H, Dickman PW, Bergmark K, Steineck G. Distressful symptoms after radical radiotherapy for urinary bladder cancer. Radiother Oncol. 2002;62(2):215–225. | ||
Park JH, Kim YS, Park J, et al. Incidence and dose-volume analysis of acute bladder toxicity following pelvic radiotherapy. Tumori. 2014;100(2):195–200. | ||
Uldry E, Schafer M, Saadi A, Rousson V, Demartines N. Patients’ preferences on information and involvement in decision making for gastrointestinal surgery. World J Surg. 2013;37(9):2162–2171. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.