Back to Journals » Patient Preference and Adherence » Volume 20
What Matters Most to Patients with NSCLC When Choosing Anticancer Treatments in China? A Best–Worst Scaling Study
Authors Qiao J, Liu S, Bao S, Tao Y, Zhao J, Chen Y
Received 24 November 2025
Accepted for publication 21 February 2026
Published 16 March 2026 Volume 2026:20 584024
DOI https://doi.org/10.2147/PPA.S584024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Jingyi Qiao,1,2 Shimeng Liu,1,2 Shiyi Bao,1– 3 Ying Tao,1,2 Jiaxin Zhao,1,2 Yingyao Chen1,2
1School of Public Health, Fudan University, Shanghai, People’s Republic of China; 2National Health Commission Key Laboratory of Health Technology Assessment (Fudan University), Shanghai, People’s Republic of China; 3Department of Teaching Management, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Shimeng Liu, School of Public Health, Fudan University, 130 Dongan Road, Xuhui, Shanghai, 200032, People’s Republic of China, Tel +8613046006196, Email [email protected] Yingyao Chen, School of Public Health, Fudan University, 130 Dongan Road, Xuhui, Shanghai, 200032, People’s Republic of China, Tel +8613564508981, Email [email protected]
Objective: This study aimed to evaluate treatment preferences for anticancer drugs among patients with non–small cell lung cancer (NSCLC), in order to provide evidence not only for clinical prescribing decisions but also for broader applications such as health insurance reimbursement and policy-making.
Methods: A Best–Worst Scaling object‐case (BWS‐1) questionnaire was administered to NSCLC patients. Thirteen choice sets, each containing four attributes, were generated using Balanced Incomplete Block Design. Respondents were asked to identify the most and least important attribute within each set. The attributes include overall survival (OS), disease control rate, progression-free survival (PFS), dyspnea, pain, objective response, hemoptysis, fever, nausea and vomiting, monthly out-of-pocket expenditure, cough, mode of administration, fatigue. Relative attribute importance and preference heterogeneity were estimated using counting analysis and a conditional logit model (CLM).
Results: A total of 102 NSCLC patients were enrolled. High concordance was observed between counting analysis and conditional logit results. In the CLM, OS (β=3.537, P< 0.01), disease control rate (β=2.025, P< 0.01), and PFS (β=1.574, P< 0.01) showed the strongest positive preferences. Fatigue (β=– 1.158, P< 0.01) and mode of administration (β=– 0.600, P< 0.01) were associated with lower relative importance. Cough showed a negative coefficient but was not statistically significant (β=– 0.185, P=0.11).
Conclusion: This study is the first to explore the NSCLC patient medication preference using a BWS-1. The findings suggest OS, disease control rate, and PFS are prioritized by patients when choosing treatment regimens.
Keywords: patient preferences, best–worst scaling, non–small cell lung cancer, drug therapy
Introduction
The incidence and mortality of malignant tumors in China have been steadily increasing. According to data from the National Cancer Center of China, in 2022, lung cancer remained the leading cause of both cancer incidence and death in the country.1,2 Non-small cell lung cancer (NSCLC), the most common histological subtype, accounts for approximately 80%–85% of all lung cancer cases.3,4 With the advent of precision medicine, survival among NSCLC patients has been significantly prolonged, and therapeutic strategies have grown increasingly complex. In addition to conventional surgery and chemotherapy, molecularly targeted therapies and immunotherapies have emerged as novel options for patients with advanced disease.5–7 Current pharmacological regimens encompass cytotoxic agents, targeted therapies, and immune checkpoint inhibitors.8 The therapeutic landscape for lung cancer has expanded rapidly in recent years, leading to an increasingly diverse array of treatment regimens. These options differ markedly with respect to clinical efficacy, safety profiles, modes of administration, and their broader impact on patients’ quality of life.9,10 Such heterogeneity underscores the importance of tailoring treatment decisions to individual patient characteristics. Accordingly, current clinical guidelines advocate for personalized strategies informed by tumor stage, molecular testing, and evidence-based standards.11 Beyond these clinical determinants, however, the integration of patient values and preferences is indispensable, as they represent a cornerstone of truly individualized and patient-centered care.12
In recent years, a patient-centered model has become a core objective of healthcare reform in China, shifting decision-making from a physician-directed approach to a shared, collaborative process. Studies have shown that patient involvement in clinical decisions is crucial for improving treatment outcomes and satisfaction,13 and that patient preferences are closely linked to adherence and quality of life.14 Chinese Expert Consensus on the Multidisciplinary Team Diagnosis and Treatment of Lung Cancer emphasizes that the optimal treatment plan should integrate individual patient data with the latest evidence and fully respect patient values and preferences.15 Against this backdrop, quantitatively characterizing patient treatment preferences is essential for accurately identifying individual therapeutic goals and health needs, thereby advancing personalized care. Nevertheless, research on medication preferences among NSCLC patients in China remains scarce.
Stated-preference methods, including best-worst scaling (BWS) and discrete choice experiments (DCE), are widely used to quantitatively elicit patient preferences through choice modelling techniques. Although DCEs have been increasingly applied in oncology, the use of BWS in this field remains relatively limited.16–19 However, DCE typically require respondents to evaluate multiple attribute levels simultaneously and may impose a higher cognitive burden when the number of attributes is large, whereas rating/ranking tasks are susceptible to scale-use heterogeneity and limited discrimination.20 The BWS grounded in random utility theory, asks respondents to repeatedly identify the most and least important items within a set, thereby enabling efficient estimation of relative attribute importance while reducing cognitive burden and mitigating common scale biases.21,22 Moreover, accumulating evidence suggests that BWS may be more reliable for eliciting patient medication preferences.23 In particular, object-case BWS (BWS-1) is well-suited for prioritizing a relatively large set of treatment attributes when the objective is to obtain a stable importance ranking and preference weights.24
Therefore, this study applied BWS-1 to estimate preference weights and rank the relative importance of key anticancer drug attributes among Chinese patients with NSCLC. By quantifying the relative importance of attributes and examining preference heterogeneity, the results aim to support shared decision-making in clinical practice and provide patient-centered input to broader policy and health-technology assessment deliberations.
Materials and Methods
Study Participants and Elicitation Method
A convenience sample of patients was recruited from Hainan Cancer Hospital between July and October 2022. The questionnaire comprised three sections: disease characteristics, patient demographic information, and thirteen BWS-1 choice tasks assessing drug-selection preferences. Eligible participants were aged ≥18 years, had histologically confirmed NSCLC, had received or were candidates for chemotherapy or immunotherapy, and had provided written informed consent. Patients with psychiatric disorders or those unable to complete the survey were excluded. Although no consensus on the optimal sample size for BWS studies exists, prior studies have indicated that at least 100 respondents provide a robust basis for preference modeling.24,25 Consequently, a minimum target of 100 patients was set, and data were collected via face-to-face administration to ensure quality. Given the sample size, analyses of preference heterogeneity were prespecified as exploratory.
Prior the formal survey, a pilot test and a field-based cognitive interviews were conducted to evaluate the questionnaire’s logic flow, layout, and respondent comprehension. The field survey was carried out by a trained research team composed of faculty members and graduate students from Fudan University and Hainan Medical University, together with medical staff from the hospital. All interviewers received systematic training covering study background, methodological principles of BWS, questionnaire design, and interview techniques. Attribute explanation cards and sample tasks were provided to respondents to facilitate comprehension.
To ensure the quality of data collection, the survey was conducted face-to-face. The questionnaire was administered by trained investigators, with support from clinical staff when appropriate. Before participants completed the tasks, one or two investigators explained the rationale of the survey and provided standardized instructions, and clarified technical terms as needed. Completed questionnaires were entered into an EpiData 3.1 database using a double-entry procedure, and any discrepancies were resolved before analysis. The study received ethical approval from the School of Public Health, Fudan University (IRB# 2021–07-0911), and written informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
Experimental Design
The final list of thirteen attributes was determined through a structured multi-step process to ensure comprehensiveness and clinical relevance. First, we conducted a literature review of NSCLC preference studies, treatment guidelines, and pivotal clinical trials/drug labels to compile an initial attribute pool covering efficacy, adverse events, treatment convenience, and economic burden. Second, an in-person expert consultation involving five clinical physicians in March 2022 was conducted to refine the attribute scope, improve clinical interpretability, and ensure coverage of both overall quality-of-life–related domains and specific adverse events (eg., nausea/vomiting). Third, adverse-event attributes were prioritized using multiple criteria: (i) mapping candidate symptoms to commonly used health-related quality-of-life symptom domains; (ii) prioritizing adverse events with greater documented impact on quality of life in the literature; (iii) considering adverse-event frequency profiles extracted from RCT studies trials and drug labels; and (iv) cross-checking adverse-event attributes commonly included in prior NSCLC stated-preference studies. Based on these steps, thirteen attributes were finalized (Table 1).
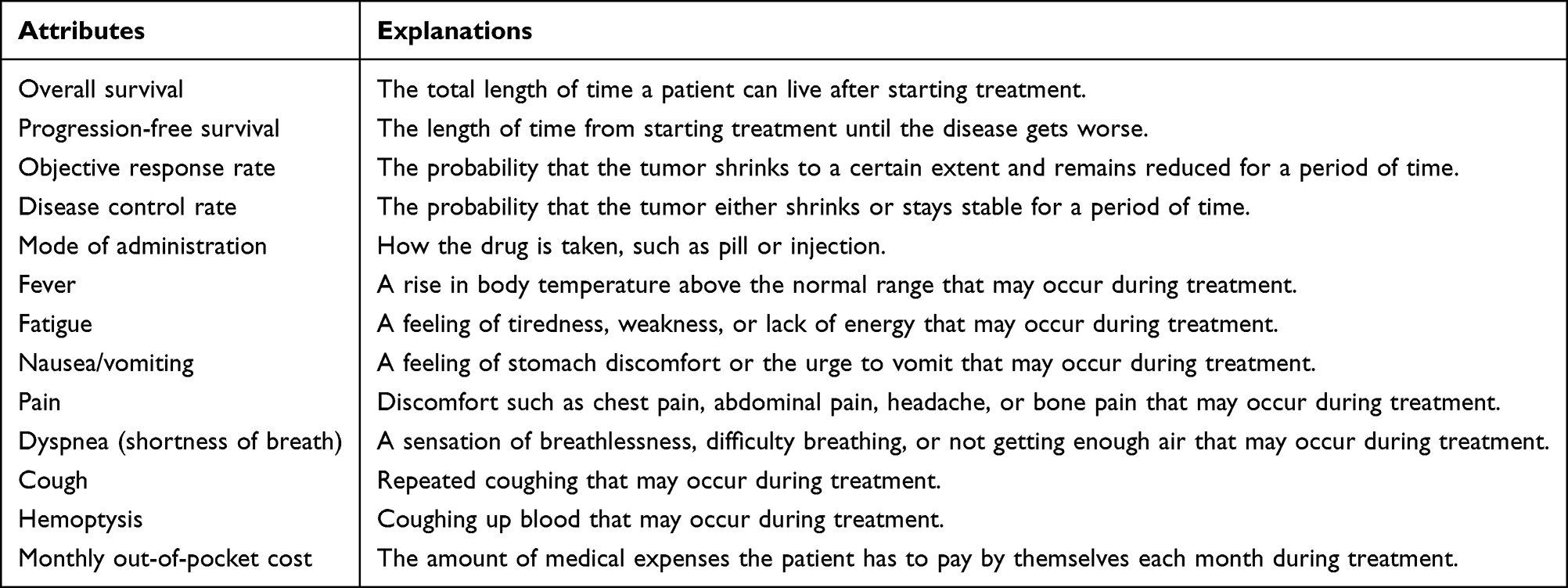 |
Table 1 Attributes of the BWS-1 Study in NSCLC Patients |
For reporting and interpretation, attributes were grouped into four domains—efficacy (OS, disease control rate, PFS), safety/symptoms (eg., dyspnea, pain, fatigue, nausea/vomiting), convenience (mode of administration), and economic burden (monthly out-of-pocket expenditure)—to align with how treatment trade-offs are typically framed in clinical decision-making and stated-preference research.26 Domain grouping was used for descriptive organization only; estimation was conducted at the attribute level.
Following the ISPOR Task Force’s ten design criteria, a Balanced Incomplete Block Design (BIBD) was implemented in R 4.1.3 to generate thirteen BWS-1 choice sets, each containing four attributes. This design ensured that every attribute appeared an equal number of times and co-occurred with every other attribute in a balanced manner, allowing reliable estimation of relative importance while minimizing respondent burden. To reduce cognitive fatigue, the order of tasks was fixed across all questionnaires, consistent with previous BWS studies in China.24 Attribute definitions are provided in Table 1, and a sample task is illustrated in Table 2. Detailed experimental design and analytical procedures have been reported elsewhere.22,24,27 Finally, thirteen choice sets per respondent were chosen to balance statistical precision with respondent burden. This design allowed each attribute to appear an equal number of times across tasks, ensuring reliable estimation of relative importance while maintaining participant engagement.
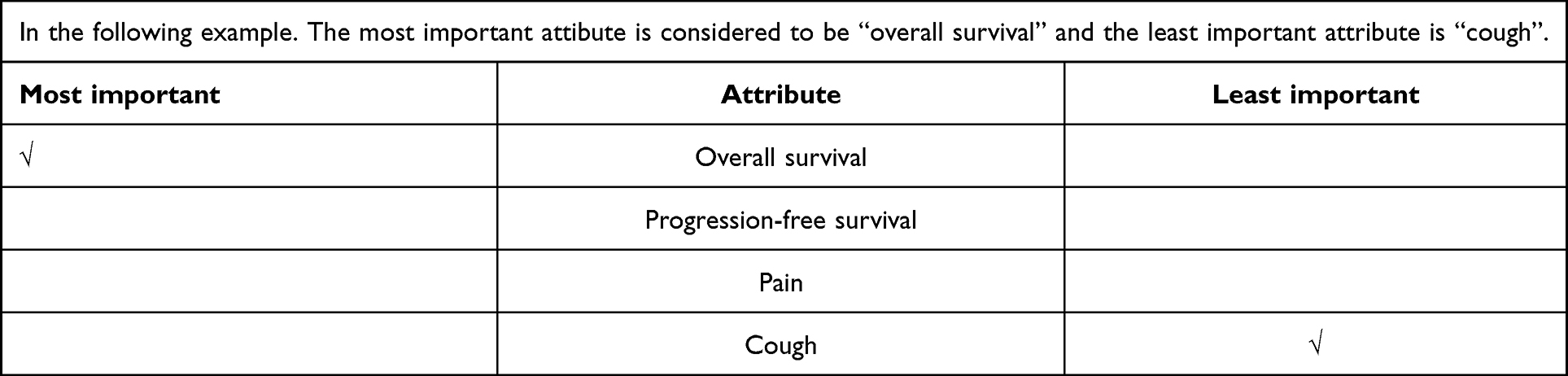 |
Table 2 Example of BWS-1 Question |
Statistical Analysis
Two analytical approaches were applied: counting analysis and a conditional logit model (CLM). For counting analysis, the number of times each attribute i (among the thirteen core attributes, eg., OS, disease control rate) was chosen as “best” or “worst” was tallied at both individual and aggregate levels. Standardized Best–Worst (BW) scores, defined as the difference between best- and worst-selection counts, quantified relative attribute importance. A McFadden CLM was fitted via maximum likelihood estimation to derive preference weights, with monthly out-of-pocket cost designated as the reference attribute; model coefficients represent marginal utility differences relative to this baseline. To explore heterogeneity in preferences, K-means clustering was employed to partition respondents into two subgroups (Cluster 1 and Cluster 2), optimizing the ratio of between-cluster to within-cluster variance.
Results
Participant Characteristics
A total of 102 respondents provided informed consent and completed the survey; all questionnaires passed the embedded quality-control task and were included in the final analysis The mean age was 60.24 ± 10.64 years; 72.5% were male, 71.6% were urban residents, and 98% were married. More than half (54.9%) had a smoking history of over 10 years. Annual household income was predominantly below 150,000 CNY. Insurance coverage was primarily provided by Urban Employee Basic Medical Insurance (53.9%) and Urban–Rural Resident Basic Medical Insurance (37.3%). Regarding disease characteristics, 60.8% were diagnosed with lung cancer in 2022; adenocarcinoma accounted for 71.6% and squamous cell carcinoma for 22.5%; most patients presented at stage IIIA or later. Driver mutations were detected in 57.8% of patients (Table 3).
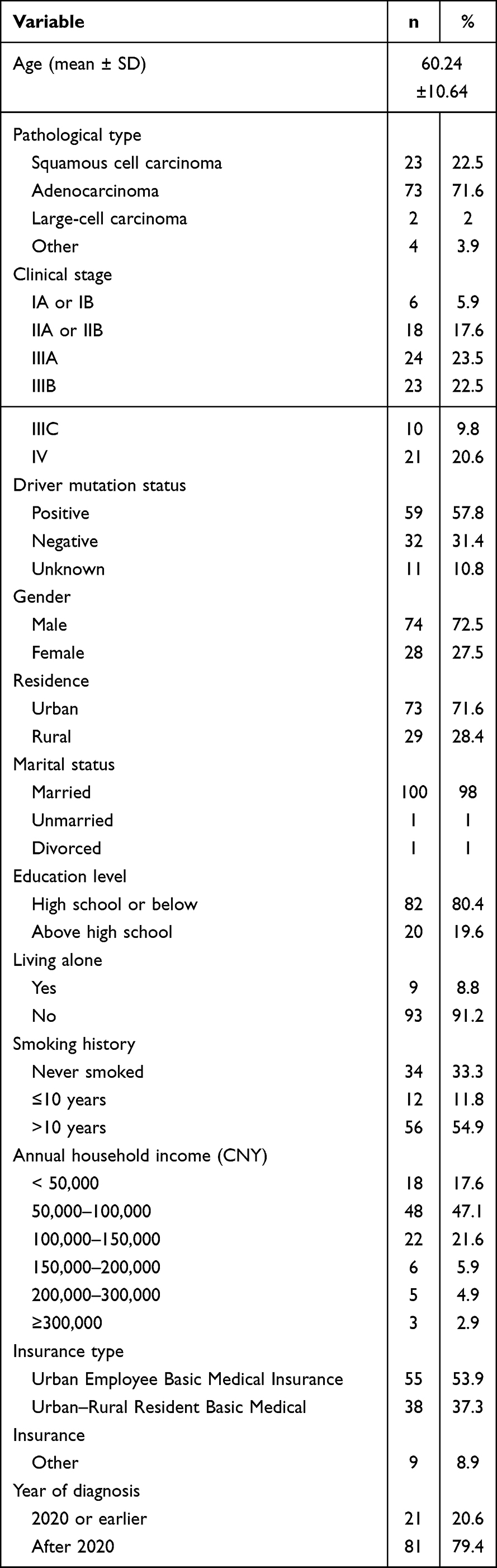 |
Table 3 Demographic and Disease Information for BWS-1 Respondents (N=102) |
Treatment Preferences in NSCLC Patients
Counting‐Analysis Results
Table 4 summarizes the counting‐analysis outcomes. At the aggregate level, OS received the highest “best” count (358) and the lowest “worst” count,2 whereas fatigue demonstrated the opposite pattern (“best” = 2; “worst” = 257). The top three attributes by standardized BW score were OS (BW = 356; standardized = 0.873), disease control rate (BW = 219; standardized = 0.537), and PFS (BW = 170; standardized = 0.417), indicating that survival benefit and disease control were most highly valued. Conversely, fatigue (BW = –255; standardized = –0.625), mode of administration (BW = –186; standardized = –0.456), and cough (BW = –108; standardized = –0.265) were most frequently rated as least important. At the individual level, the smallest standard deviation was observed for OS (SD = 0.265), reflecting consensus regarding its importance, whereas monthly out‐of‐pocket cost exhibited the greatest variability (SD = 0.641), indicating heterogeneous economic preferences. Overall, the attributes most often selected as “most important” were OS, disease control rate, PFS, dyspnea, and pain; those most often selected as “least important” were objective response rate, hemoptysis, fever, nausea/vomiting, monthly out‐of‐pocket cost, cough, mode of administration, and fatigue.
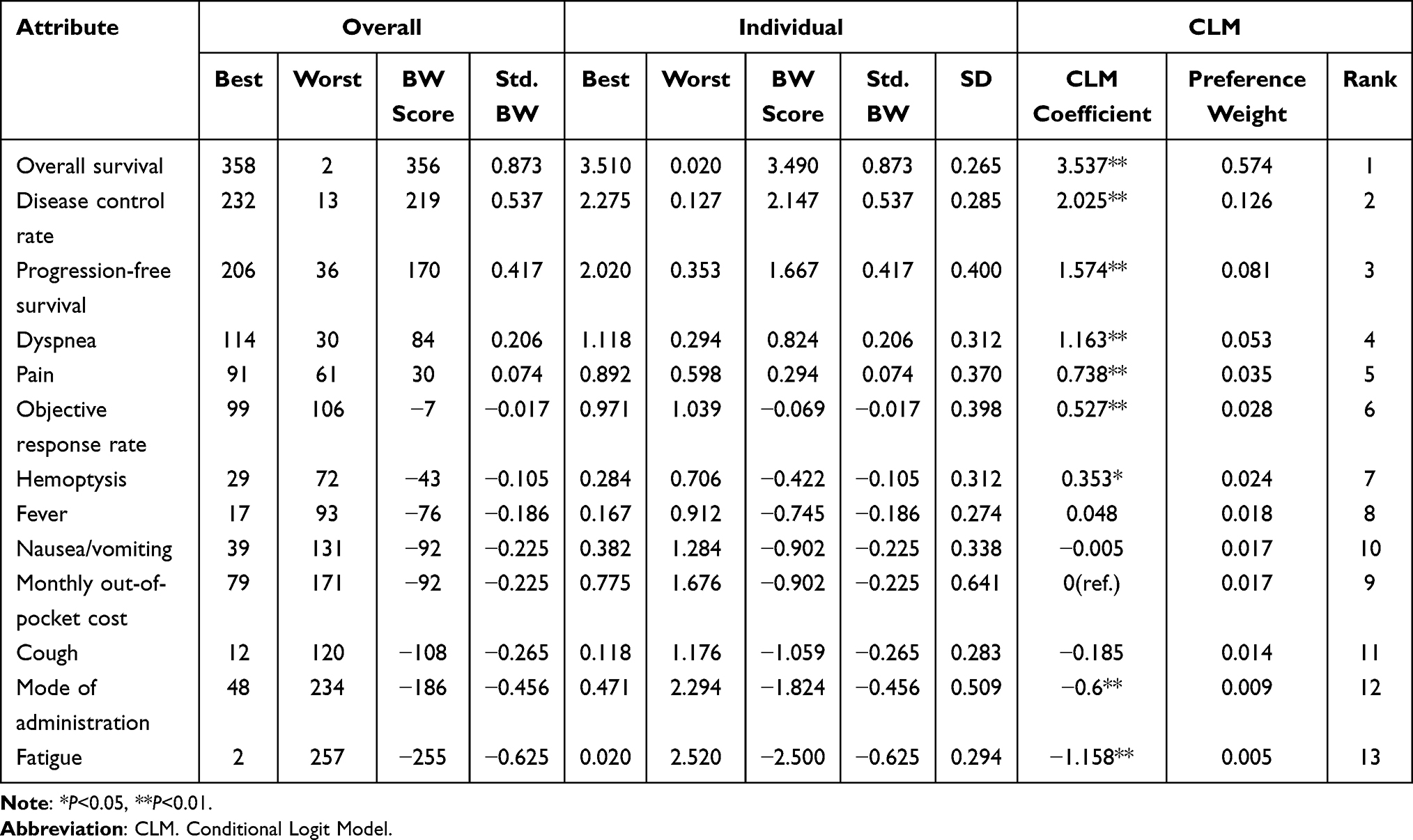 |
Table 4 BWS-1 Results |
Conditional Logit‐Model Results
CLM (Table 4) corroborated the primary role of survival-related attributes. The model showed good overall fit (likelihood ratio χ2=1932, df=12, P<0.001) and strong discrimination based on predicted choice probabilities (AUC=0.92, 95% CI: 0.90–0.94), which is generally considered outstanding (AUC>0.90).28 OS (β= 3.537; preference weight = 0.574), disease control rate (β= 2.025; preference weight = 0.126), and PFS (β= 1.574; preference weight = 0.081) held the highest coefficients and weights, consistent with counting analysis. Although monthly out‐of‐pocket cost served as the reference attribute, its relatively low preference weight (0.017; rank 9) suggests a modest negative impact on treatment choice, potentially owing to insurance coverage or sample heterogeneity. Adverse events such as nausea/vomiting (β= –0.005), fever (β= 0.048), and cough (β= –0.185) did not reach statistical significance (P ≥ 0.05), indicating limited influence on overall preferences.
Preference Heterogeneity
K-means clustering was applied to the counting‐analysis results to examine subgroup differences. As illustrated in Figure 1, the greatest heterogeneity was observed for dyspnea, pain, mode of administration, and objective response rate—particularly for mode of administration—while other attributes exhibited relatively homogeneous preferences across clusters.
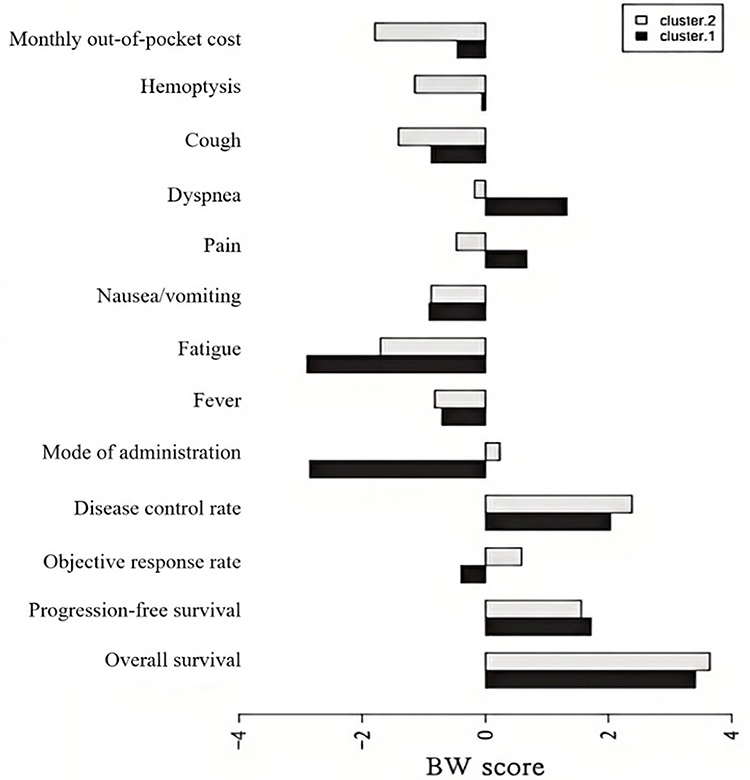 |
Figure 1 K-means Clustering Results Based on Counting Analysis. |
Discussion
This study applied a BWS-1 approach to systematically characterize anticancer drug-attribute priorities among NSCLC patients in China. Comparative analyses using counting and CLM yielded largely consistent patterns, supporting the stability of the main findings across analytical approaches. Minor discrepancies were observed for a small number of attributes (eg., monthly out-of-pocket cost and nausea/vomiting), which likely reflect differences in model parameterization and the fact that some attributes had weaker or non-significant effects in the CLM.
Patients’ preference intensities were found to be markedly greater for survival‐related attributes—namely, OS, disease control rate, and PFS—than for other considerations. Given the importance-ranking nature of BWS-1 tasks, the strong dominance of OS may partly reflect a ceiling effect whereby universally salient outcomes attract repeated “best” selections. In contrast, attributes related to treatment convenience and symptom management, such as cough, mode of administration, and fatigue, were deemed relatively less important. These findings are consistent with international studies that have examined lung cancer patients’ preferences using DCE. Similar to our results, those studies also emphasized the importance of survival benefits and disease control.29–32 Although targeted therapies and immunotherapies have substantially prolonged survival, long‐term outcomes remain suboptimal: many advanced NSCLC patients, even when treated with combinations of targeted agents, chemotherapy, and immunotherapy, exhibit median OS of less than two years.33–35 Moreover, the challenge of balancing treatment efficacy against side effects remains, as tumor heterogeneity often drives resistance to molecularly targeted drugs, thereby reducing therapeutic benefit.36 Current modalities therefore continue to fall short of fully meeting patients’ expectations for durable disease control.
Interestingly, objective response rate—a commonly reported endpoint in clinical trials—received relatively low scores. This may reflect patients’ limited understanding of this technical term, making it less relevant to their perceived treatment priorities. This suggests that, in future preference studies, attribute selection should strive to maintain scientific rigor while avoiding overly specialized clinical or biochemical metrics, thereby ensuring that patients can readily comprehend the significance of each attribute.
In addition, adverse reactions such as dyspnea, fever, and nausea/vomiting had varying impacts on NSCLC patients’ preferences, with dyspnea being the most strongly avoided symptom. For NSCLC patients who already suffer from impaired pulmonary function, the onset of dyspnea can significantly compromise their quality of life and overall physical and mental well-being. Therefore, in the selection and optimization of treatment regimens, patients’ desire to avoid adverse effects like dyspnea should be carefully considered. A balance must be struck between the incidence of side effects and the symptom burden, and proactive measures should be taken to prevent and alleviate such adverse events.
With the widespread adoption of innovative therapies such as targeted treatments and immunotherapy, NSCLC patients now face an increasingly diverse range of drug options. However, clinical decision-making and reimbursement evaluations still lack systematic evidence from the patient perspective. Our findings indicate that NSCLC patients in China place the highest value on survival-related outcomes (overall survival, disease control, progression-free survival), while showing relatively less concern for endpoints such as objective response rate, treatment mode of administration, or specific side effects. This pattern was observed in the aggregate results, but some attributes (eg., fever, nausea/vomiting, cough) did not reach statistical significance in the CLM and should be interpreted cautiously. This contrasts with the emphasis often placed by oncologists on biomarker-driven efficacy and minimizing adverse events. Previous studies have reported similar discrepancies: physicians tend to focus on reducing toxicity, whereas patients are more concerned with treatment benefits and the treatment process itself.37 In China, survey evidence also revealed that while clinicians and family caregivers prioritize survival, patients emphasize financial burden and quality of life.38 These divergences highlight the need to strengthen shared decision-making in NSCLC care, ensuring that patients’ voices and priorities are integrated into clinical consultations. Our heterogeneity findings further suggest that preferences for symptoms and treatment convenience may vary across individuals, underscoring the value of individualized preference elicitation in practice.
From a broader perspective, patient preference data can also inform health policy and reimbursement decisions. Internationally, frameworks such as value-based insurance design demonstrate how patient values can be systematically incorporated into coverage evaluations by incentivizing high-value care. In China, health preference evidence can provide patient-centered input to policy and health technology assessment deliberations by clarifying the relative importance of outcomes and treatment features, and by supporting more transparent communication of value.
This study has several limitations. First, participants were recruited from one hospital and the sample size was relatively small, which may limit generalizability. Given the sample size, we did not conduct subgroup analyses across different patient groups; future studies should use multi-center sampling and larger cohorts to enable more robust preference heterogeneity assessment. Second, despite pilot testing and interviewer support, some attributes—especially those describing clinical endpoints and disease-related symptoms—may have been interpreted heterogeneously across respondents. This highlights the importance of clear and concise attribute formulation in preference surveys. Future studies should further optimize attribute descriptions and implement additional comprehension checks to minimize misinterpretation. Third, compared with DCE, BWS-1 allows fewer straightforward ways to incorporate explicit quality-control items, such as clearly dominant choice tasks. As a result, identifying inattentive responses may be more challenging, and additional design or analytic measures may be needed to support data-quality assessment.
Conclusion
Our study found that OS, disease control rate, and PFS are the most important attributes for NSCLC patients in China when selecting anticancer drug treatments. Heterogeneity in cost preferences was observed, but these subgroup patterns should be interpreted as exploratory given the sample size. Overall, the findings provide patient-centered evidence on treatment priorities that can support shared decision-making and the development of patient-centered communication and care pathways.
Abbreviations
NSCLC, Non-small cell lung cancer; BWS-1, Best–Worst Scaling object‐case; CLM, conditional logit model; OS, overall survival; PFS, progression-free survival; DCE, discrete choice experiments.
Data Sharing Statement
The raw datasets generated during this study can be obtained from the corresponding author, Yingyao Chen, upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the School of Public Health, Fudan University (IRB# 2021-07-0911). All participants provided written informed consent prior to enrollment.
Consent for Publication
All authors have read and approved the final version.
Acknowledgments
We sincerely thank all patients who participated in this survey and the clinical staff at Hainan Cancer Hospital for their valuable support during data collection. We also thank the research teams from Fudan University and Hainan Medical University for their assistance in field coordination and data management.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 72074047).
Disclosure
The authors declare that they have no commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Zheng R, Chen R, Han B, et al. Cancer incidence and mortality in China, 2022. Chinese J Oncol. 2024;46(3):221–11. doi:10.3760/cma.j.cn112152-20240119-00035
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J National Cancer Center. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Lung Cancer Expert Committee of the China Anti-Cancer Association, Chinese Thoracic Oncology Group, Lung Cancer Expert Committee of the Chinese Medical Association Oncology Society. Perioperative immunotherapy for non-small cell lung cancer: consensus and controversy (2024 edition). Chinese J Oncol. 2024;46:1107–1126. doi:10.3760/cma.j.cn112152-20240821-00361
4. Reck M, Rabe KF, Longo DL. Precision diagnosis and treatment for advanced non–small-cell lung cancer. N Engl J Med. 2017;377(9):849–861. doi:10.1056/NEJMra1703413
5. Miller M, Hanna N. Advances in systemic therapy for non-small cell lung cancer. BMJ. 2021;375:n2363. doi:10.1136/bmj.n2363
6. Chinese Medical Association, Oncology Society of Chinese Medical Association, Chinese Medical Association Publishing House. Chinese Medical Association guidelines for clinical diagnosis and treatment of lung cancer (Edition 2018). Chinese J Oncol. 2018;40(12):935–964. doi:10.3760/cma.j.issn.0253-3766.2018.12.012
7. Xu Z. The investigational and translation study of treatment strategies in non-small cell lung cancer [PhD]. 2023.
8. Zheng K, Hao Z, Li F, Xu T, Zhang J. Survival prognosis of patients with advanced non-small cell lung cancertreated with anti-tumor drugs. Anti-Tumor Pharmacy. 2024;14(06):738–746.
9. Myers RE, Advani SM, Myers P, et al. Engaging patients with late-stage non-small cell lung cancer in shared decision making about treatment. J Pers Med. 2021;11(10):998. doi:10.3390/jpm11100998
10. Aumann I, Kreis K, Damm K, Golpon H, Welte T, Graf von der Schulenburg JM. Treatment-related experiences and preferences of patients with lung cancer: a qualitative analysis. Health Expect. 2016;19(6):1226–1236. doi:10.1111/hex.12417
11. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA A Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
12. Sun H, Chen Y, He L, et al. Doctor’s choice preference for non-small cell lung cancer treatment. Health Eco Res. 2018;(09):10–13.
13. Huang R, Xu M, Guo H. Status and challenges of shared decision-making in China. National Med J China. 2020;(30):2346–2350.
14. Liu S, Liu J, Si L, et al. Patient preferences for anti-hyperglycaemic medication for type 2 diabetes mellitus in China: findings from a national survey. BMJ Global Health. 2023 8,April;(4):e010942 doi:10.1136/bmjgh-2022-010942.
15. Zhong W, Chinese Thoracic Oncology Group, Chinese Society of Lung Cancer, Lung Cancer Group of Oncology Branch Chinese Medical Association. Chinses expert consensus on the multidisciplinary team diagnosis and treatment of lung cancer. Chinese J Oncol. 2020;42(10):817–828. doi:10.3760/cma.j.cn112152-20200812-00731
16. Purnell TS, Joy S, Little E, Bridges JFPJF, Maruthur N. Patient preferences for noninsulin diabetes medications: a systematic review. Diabetes Care. 2014;37(7):2055–2062. doi:10.2337/dc13-2527
17. von Arx L-BL-B, KjærKjeer T. The patient perspective of diabetes care: a systematic review of stated preference research. Patient Patient Centered Outcomes Res. 2014;7(3):283–300. doi:10.1007/s40271-014-0057-0
18. Cheung KL, Wijnen BFMBF, Hollin IL, et al. Using Best–worst scaling to investigate preferences in health care. Pharmacoeconomics. 2016;34(12):1195–1209. doi:10.1007/s40273-016-0429-5
19. Crossnohere NL, Janse S, Janssen E, Bridges JFPJFP. Comparing the preferences of patients and the general public for treatment outcomes in type 2 diabetes mellitus. Patient Patient Centered Outcomes Res. 2021;14(1):89–100. doi:10.1007/s40271-020-00450-7
20. Ratcliffe J, Kaambwa B, Hutchinson C, Lancsar E. Empirical investigation of ranking vs best–worst scaling generated preferences for attributes of quality of life: one and the same or differentiable? Patient Patient Centered Outcomes Res. 2020;13(3):307–315. doi:10.1007/s40271-019-00406-6
21. Liu S, Yang Y, Sun H, Ming J, Chen Y. The significance, approaches and challenges of integrating patient preference evidence into health technology assessment. Chinese J Health Policy. 2022;15(05):52–58.
22. Tao Y, Liu S, Chen Y. Optimizing the attribute selection process for stated preference study: a study based on best-worst scaling. Chinese J Evidence Based Med. 2024;24(09):1079–1084.
23. Liu S, Chen Y, Tao Y, Lian D, Jiang S, Li S. et al. Is best-worst scaling suitable for patient preference elicitation? A nationwide representative comparison with discrete choice experiments among patients with type 2 diabetes in China. BMJ Public Health. 2026;4(1):e003571. doi:10.1136/bmjph-2025-003571
24. Liu S, Liu J, Yu Y, et al. What is valued most by patients with type 2 diabetes mellitus when selecting second-line antihyperglycemic medications in China. Front Pharmacol. 2021;12:802897. doi:10.3389/fphar.2021.802897
25. Pearmain D, Kroes EP, editors. Stated Preference Techniques: A Guide to Practice. 1990.
26. Mühlbacher AC, de Bekker-Grob EW, Rivero-Arias O, Levitan B, Vass C. How to present a decision object in health preference research: attributes and levels, the decision model, and the descriptive framework. Patient Patient Centered Outcomes Res. 2025;18(4):291–302. doi:10.1007/s40271-024-00673-y
27. Bao S. Research on drug preference of patients with non-small cell lung cancer [MS]. 2023.
28. Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thoracic Oncol. 2010;5(9):1315–1316. doi:10.1097/JTO.0b013e3181ec173d
29. Mühlbacher AC, Bethge S. Patients’ preferences: a discrete-choice experiment for treatment of non-small-cell lung cancer. Euro J Health Eco. 2015;16(6):657–670. doi:10.1007/s10198-014-0622-4
30. Bridges JF, la Cruz M, Pavilack M, et al. Patient preferences for attributes of tyrosine kinase inhibitor treatments for EGFR mutation-positive non-small-cell lung cancer. Future Oncol. 2019;15(34):3895–3907. doi:10.2217/fon-2019-0396
31. Hauber B, Penrod JR, Gebben D, Musallam L. The value of hope: patients’ and physicians’ preferences for survival in advanced non-small cell lung cancer. Patient Prefer Adher. 2020;14:2093–2104. doi:10.2147/PPA.S248295
32. Janssen EM, Dy SM, Meara AS, Kneuertz PJ, Presley CJ, Bridges JFP. Analysis of patient preferences in lung cancer – estimating acceptable tradeoffs between treatment benefit and side effects. Patient Prefer Adher. 2020;14:927–937. doi:10.2147/PPA.S235430
33. Soria J-C, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR -mutated advanced non–small-cell lung cancer. New England J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
34. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1–positive non–small-cell lung cancer. New England J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
35. Deng J, Chen D, Zhao D, et al. Recent advances in chemotherapy combined with immunotherapy for non-small cell lung cancer. Adv Clin Med. 2023;13(8):13645–13653. doi:10.12677/ACM.2023.1381907
36. Jia Q, Jin Z, Zhu B. Dilemmas in cancer treatment and exploration of pathways for precision therapy. Bulletin Nat Nat Sci Found China. 2025;39(01):24–33.
37. Zhang M, He X, Wu J, Xie F. Differences between physician and patient preferences for cancer treatments: a systematic review. BMC Cancer. 2023;23(1):1126. doi:10.1186/s12885-023-11598-4
38. He X, Zhang M, Wu J, et al. Differences in lung cancer treatment preferences among oncologists, patients and family members: a semi-structured qualitative study in China. Patient Prefer Adher. 2021;15:775–783. doi:10.2147/PPA.S299399
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.