Back to Journals » Medical Devices: Evidence and Research » Volume 17
What is Known About Early Mobilisation After Cardiac Electronic Device Implant? A Scoping Review
Authors Caleffi D ![]() , Ferri P
, Ferri P ![]() , Bellifemine M, Rovesti S
, Bellifemine M, Rovesti S ![]() , Valenti M
, Valenti M
Received 30 August 2024
Accepted for publication 24 October 2024
Published 16 December 2024 Volume 2024:17 Pages 513—524
DOI https://doi.org/10.2147/MDER.S493641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dalia Caleffi,1 Paola Ferri,2 Mauro Bellifemine,2 Sergio Rovesti,2 Miriam Valenti2
1Clinical and Experimental Medicine PhD Program, Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena, Italy; 2Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena, Italy
Correspondence: Dalia Caleffi, Clinical and Experimental Medicine PhD Program, Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Via Piacenza 16, Nonantola (MO), Modena, 41015, Italy, Email [email protected]
Background: The number of cardiac implantable electronic devices (CIEDs) implanted has been growing and the population who receive the device is older and has more comorbidities. Long bed rest and immobilisation have always been common after the implant, but a consensus does not exist on the argument.
Purpose: To map and synthesise available literature on the mobilisation approach after the implant of a CIED and which correlated outcomes exist.
Methods: A literature search was conducted in December 2023 on six databases. Screening of articles, data extraction and quality appraisal were performed by more than one author. Articles included were primary articles exploring bed rest or mobilisation after a CIED procedure. Descriptive analysis was conducted to present and synthesise the results.
Results: Of the 113 records identified, eight matched the inclusion criteria. The majority of the articles were randomised controlled trials (n = 6). Other studies were quasi-experimental (n = 1), retrospective (n = 1) and cross-sectional (n = 1). Data descriptive analysis led to the development of three main topics: (1) mobilisation modalities, (2) potential complications and (3) type of device.
Conclusions: Early mobilisation after a CIED procedure appears to be safe and not associated with other complications. A predominant barrier to early mobilisation is the lack of a consensus on the time and type of mobilisation. Early mobilisation could be applied more safely with the use of an arm support. To strengthen the evidence there is a need for more rigorous research analysing the type of device and the leads utilised.
Keywords: early ambulation, mobilisation, implantable defibrillator, pacemaker, bed rest
Introduction
In currently available literature there is no clear definition of the bed rest time requested after having implanted a cardiac implantable electronic device (CIED). Long bed rest and immobilisation are correlated with the fear of dislocation of the device, the leads and incidence of important hematoma.1 Some studies, however, reflect on the fact that it might not be necessary to have a total bed rest after CIED implantation.1–3 Indeed, a long immobilisation may prolong recovery, induce pain, reduce mobility, create sleep disturbance, and contribute to delirium onset, pressure ulcers and urinary retention. Nurses have a key role in screening and managing patients’ discomfort or complications after post-operative adverse events.2
Furthermore, the prevalence of cardiac arrhythmias and high degree atrioventriculars increase in elderly patients.3 The number of CIEDs implanted is increasing and the patients who receive the device are older and have more comorbidities.4,5 This condition is probably correlated with the growing number of nonischemic cardiomyopathy and heart failure patients requiring primary prevention of sudden cardiac death.6
Hospitalisation can result in rapid functional decline, especially in older adults. One of the major causes is prolonged bed rest and immobility after an operation.7,8
Therefore, in the present scoping review study we sought to investigate how early mobilisation after CIED implantation is analysed and what is the current position of the literature on the topic.
Review
CIEDs are electronic devices that are fundamental in the management of heart diseases or heart rhythm disorders.9 One to three leads, which run transvenous to the implant in the myocardium, and the central canister, which contains the battery, generator, and all programming functions are transversal characteristics of CIED.10
The implanted CIED can differ based on the patient’s clinical disease. They are indicated to manage slow and fast heart rates, and in the treatment of selected patients with heart failure.11 Pacemakers can be implanted in the right atrium, the right ventricle or both (biventricular).11 Bradycardia pacemakers are evaluated for sick sinus syndrome and type II second-degree, high-grade, and complete heart block.9 Implantable cardioverter defibrillators (ICD) are used to prevent sudden death in patients at risk or who have had life-threatening arrhythmias.9,11 People with chronic heart failure may benefit from cardiac resynchronisation therapy (CRT) due to weak and/or poorly coordinated ventricles and because they are at risk of sudden dysrhythmias.10,11
Leadless pacemakers and subcutaneous implantable cardiac defibrillators are being developed. Leadless pacemakers are correlated with less infectious risk, but they are associated with cardiac perforation risk9,11 and they have no indications for patients with implanted vena cava filters, mechanical tricuspid valves, or implanted cardiac devices providing active therapy.12
During a surgical intervention nursing assistance is required. Nurses should understand indications to implant and the correlated potential complications after intervention. Nurses collaborate in patient monitoring but also education.12
Literature reports a lot of indications about post-operative CIED patient assistance: interrogating the device, monitoring cardiac rhythm13 control for potential complication, hemodynamical stability, device malfunction, symptom infections12 or distance monitoring.14 Mobilisation is not a parameter that is always contemplated when talking about patient assistance and education with the related potential complications.
Aims
The primary aim of this scoping review was to map and synthesise available literature on the approach to mobilisation after the implant of cardiac implantable devices. The secondary aim was to identify gaps in the literature which could set the basis for future research or a change to clinical practice. This scoping review addresses two questions:
- What is known about early mobilisation after cardiac electronic device implantation?
- What are the gaps in the literature about mobilisation care towards people who received an implantable cardiac electronic device?
Methods
Design
A scoping review was the chosen method to examine emerging evidence; this was due to the fact that a first review of the literature had shown that the conducted studies differ a lot in methodological aspects, time of publication, outcomes and interventions. A scoping review contributes to examining the research conducted on the topic and inform future research studies.15
This scoping review is reported using the Preferred Reporting Items for Systematic Review and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR).16
The protocol for this review is not published.
Search Method
The search strategies were developed with the support and the guidance of an academic librarian. The initial stage of the search was done in Medline to identify the Medical Subject Headings (MeSH) terms and keywords related to the review aims. In order to find all the available evidence a specific research strategy was adapted for each database interrogated, using keywords as indexed terms. With the contribution of the expert academic librarian, hand searching was performed for studies that were not retrieved in the main searches. Finally, reference lists of screened eligible articles were reviewed. The search was undertaken in December 2023 with no limitation applied to publication date. The search strategies were applied to: Medline, CINAHL, Embase, Web of science, PsycInfo, and Scopus.
Inclusion and Exclusion Criteria
Studies were considered for inclusion if eligibility criteria were matched. Peters et al17 underline that an appropriate scoping review has to clarify the following aspects. (1) Participants were people who had received an implantable electronic cardiac device which could be a single, dual chamber or biventricular pacemaker and/or an ICD. (2) The core concept examined by the scoping review was the approach to care provision. Care is inherent on how early mobilisation is applied or intended after the device implant, and what are the time and the modalities of mobilisation during the recovery. (3) The context analysed is all the settings in which CIED procedures are performed.
Early mobilisation is intended to involve any kind of patient mobilisation after CIED implantation which avoids prolonged and obliged laying on the bed allowing the ability to stand up and mobilisation.
The inclusion criteria were applied for all studies in which the method utilised was clearly defined, the full text article was available and the language was English or Italian.
Exclusion criteria were studies which evaluated the postoperative long-term setting and mobilisation intervention without focusing on the effect of early mobilisation and bed rest duration.
Search Outcome
The main question which the scoping review intended to answer is whether early mobilisation may be a possible intervention to apply without negative outcomes after CIED intervention.
Other outcomes which the scoping review would like to understand are the time and modalities of mobilisation exploring how much literature is available and which should be the next areas of research that have to be developed and analysed.
Quality Appraisal
Quality appraisal was undertaken to answer one of the goals of this scoping review: understanding what literature is available and give information for future research. Two authors independently appraised the included articles using the JBI Critical Appraisal Tools: Checklist for Randomised Controlled Trials,18 Checklist for quasi-experimental study,19 Checklist for Prevalence study20 and Checklist for analytical cross-sectional study.21 After independent evaluations any disagreement was discussed by the two members of the team.
Data Abstraction
Three members of the research team screened the title and abstract independently. To assure the blind process Rayyan, a web and mobile app designed for reviews, was used in this selection phase. The full text articles were reviewed by two authors and any disagreement was discussed with the third.
Data of eligible studies were extracted by two authors independently following the Joanna Briggs Institute indications. Aspects included in the data extraction format were: type of study, methodology, country, setting, aim, characteristics of participants, data collection, interventions, outcomes, data analysis and key findings.
Synthesis
A descriptive results analysis is presented in order to point out the current literature on the topic.
In order to identify the existing knowledge, tables are used to present conceptual categories such as intervention type, study population, duration of intervention, aims, methodology adopted, key findings, and gaps in the research.
Results
Selection of Sources Evidence
Database searching identified 113 articles; after removing duplicates, 74 articles were screened for title and abstract. Out of these articles, nine were included for full-text review. Following a full text review five articles were included. Another five potential eligible articles were identified from full text references’ analyses, from which two were excluded. A total of eight articles are included in this review. An outline of the study screening and selection process is presented in the PRISMA-ScR flow chart shown in Figure 1.16
 |
Figure 1 Flow diagram for selection of studies (PRISMA FLOW DIAGRAM). |
Critical Appraisal of Sources of Evidence
Five randomised, controlled trials were appraised using the JBI Critical Appraisal Tools: Checklist for Randomised Controlled Trials. For most of the studies patients and assessors’ blindness was not applied. As a consequence, allocation concealment was unclear for two of them.
One of the quasi-experimental studies did not have similar groups at baseline and for the other one this aspect was not applicable because it did not have a control group. For more than one aspect of the survey study, information was insufficient or unclear. No study was excluded for quality reasons.
Characteristics of Source of Evidence
General characteristics and data extraction from each article22–29 are presented in Table 1. The majority were randomised controlled trials (n = 5), other studies were quasi-experimental (n = 1), retrospective (n = 1) and cross-sectional (n = 1). Most studies were conducted in Italy (n = 5), one in the United States, one in the United Kingdom and one in Thailand. Study participants were patients who received cardiac implantable electronic devices. Three studies included pacemaker and ICD implantation.22–24 One study generically talks about cardiac rhythm device25 and four other studies referred to pacemaker implantation.24,26–29 Sample sizes of the randomised controlled studies ranged from 30 to 200 patients.22,26–29 The retrospective studies involved 411 patients, the quasi-experimental one, 1023 and the survey, 100 participants.25 A total of 459 patients of the studies included received an experimental intervention, of which 219 were male with a mean age of at least more than 60 years old. A total of 1017 patients were included in the experimental or control group of the studies.
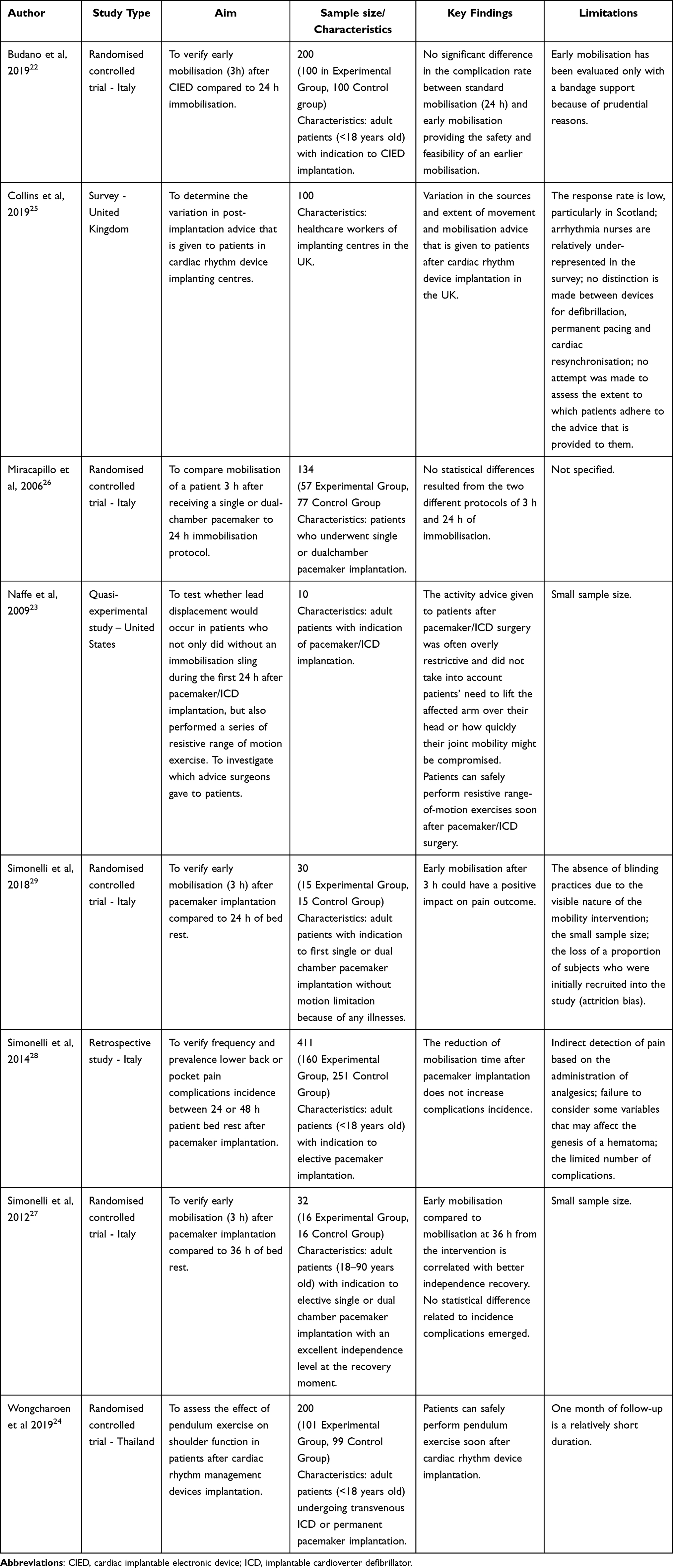 |
Table 1 Characteristics and main results of the studies considered in this review |
The experimental intervention analyzed by the quantitative experimental study was based on early mobilisation after pacemaker implantation. Five studies compared early mobilisation after three hours of bed rest to later mobilisation after 24 or 36 hours.22,26,27,29 Simonelli et al28 examined mobilisation after 24 hours instead of 48 hours. Early CIED implantation arm activity has been analyzed by Naffe et al23 the same day and by Wongcharoen et al24 the day after. Lead dislodgement was not the main outcome for all experimental studies, but it was always contemplated. Other outcomes presented were hematoma,22,24,26,28,29 pain,28,29 shoulder flexion range,24 and functional independence.27 In their survey, Collins et al25 presented data about how many different kinds of advice were given by different specialists after cardiac rhythm devices. A similar investigation had been carried out also by Naffe et al23 towards clinicians.
Descriptive data analysis leads to the development of three main topics: mobilisation modalities, potential complications, type of device.
As shown in Table 2, mobilisation after CIED implantation is not always the same. It can occur after 3 hours of bed rest or after 24 hours or more. The modality is not always specified. Naffe et al23 and Wongcharoen et al24 in the intervention groups provide arm activities, instead, Budano et al,22 Miracapillo et al,26 Simonelli et al29 and Simonelli et al27 talk about early mobilisation with a bandage or support of the ipsilateral arm. Similarly, the two-survey shows evidence that advice given to patients about inherent mobilisation are not always the same and have important differences.
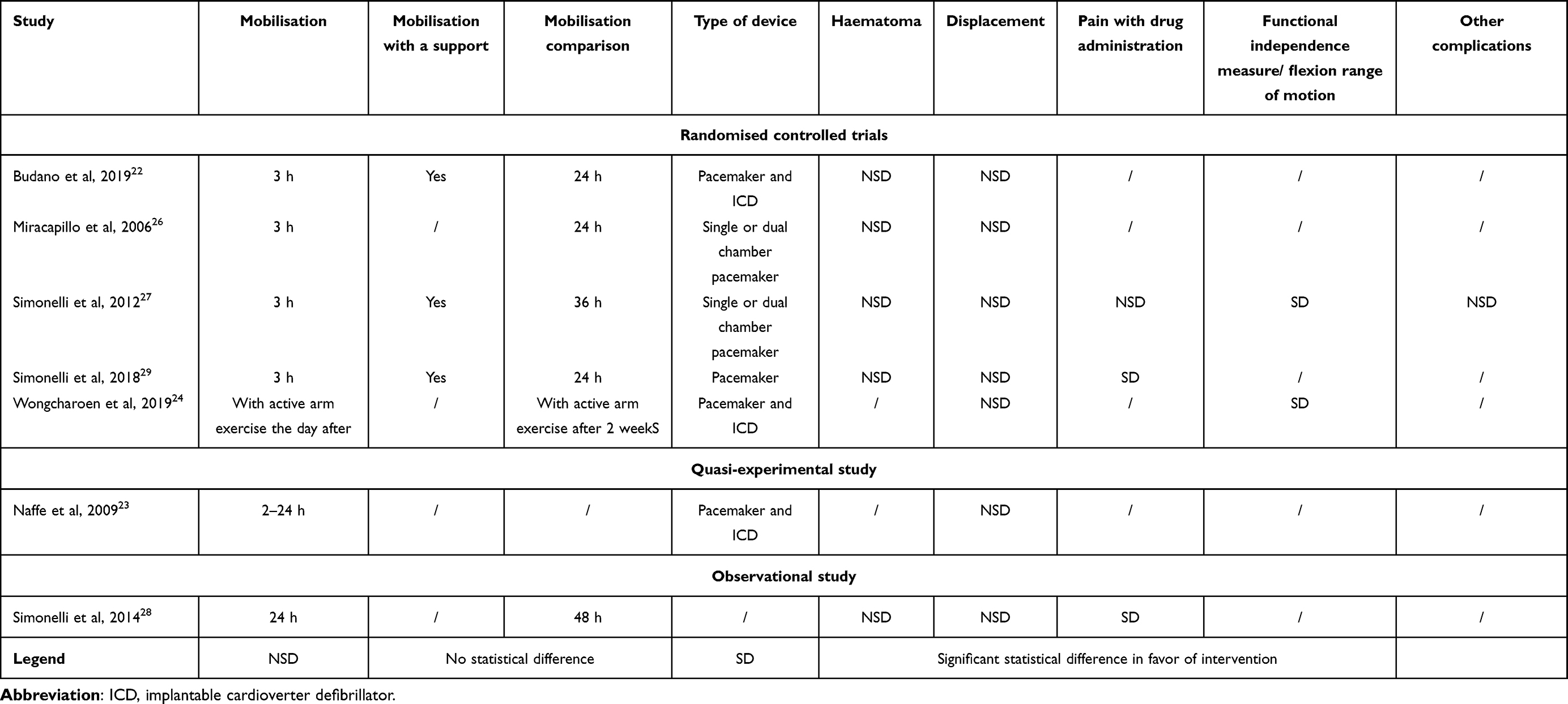 |
Table 2 Main topic synthesis |
Outcomes and complications identified differ between the studies, but hematoma and lead displacement are almost ever present. As shown in Table 2, the rate of complications between experimental and control group, if present, is not particularly high and does not significantly differ between the analysed groups.
Radiological monitoring is analysed by studies which included dislodgement between complications observed. Miracapillo et al26 and Budano et al22 evaluated chest X-rays. Wongcharoen et al24 included X-ray monitoring at 1 day and 1 month after implantation. Simonelli et al28 and Simonelli et al29 specified the radiological monitoring to evaluate lead dislodgment before patient discharge. Simonelli et al27 did not clarify radiological monitoring while Naffe et al23 evaluated dislodgement through electrophysiology parameters.
Finally, the type of CIED taken into account can be pacemaker without specifying if it is with a single or dual chamber, an ICD or generically a cardiac rhythm device without specifying the characteristics.
The PAGER methodology was used for data analysis to establish greater methodological rigour in this review, and it is presented in Table 3.30
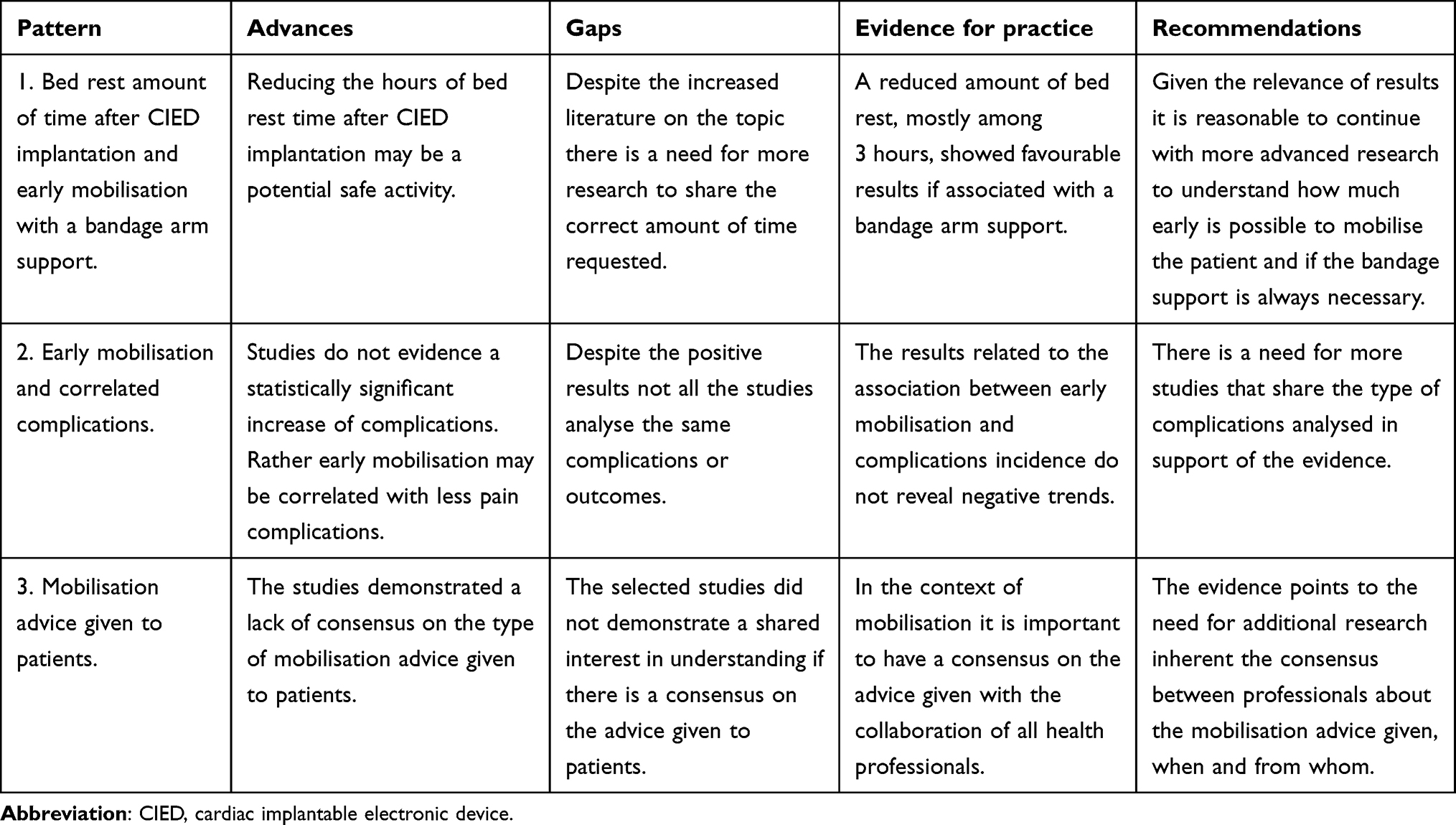 |
Table 3 PAGER structure obtained from the analysis of the selected articles |
Discussion
This scoping review synthesises the approaches to early mobilisation care after a CIED elective procedure, and makes an overview of the current literature, methodological difference and gaps.
The optimal management of patient bed rest and mobilisation after a CIED procedure is an issue for which there has not been a clear consensus yet.1
Findings from this review add to the existing literature that interest in the argument is growing as the increasing number of studies demonstrates.
It is important to evidence that a number of unpublished studies which could add important information on the topic exist. Orlando et al31 describe in a poster a descriptive study on the effect of immobilisation after pacemaker and ICD implantation. Another abstract by Feldman et al32 was focused on early mobilisation after 4 hours from implantation. Golian et al33 published a protocol of their randomised controlled trial which will be concluded in the future on the unrestricted mobilisation of the ipsilateral arm.
A clear indication about the correct time after which mobilisation can be allowed is not given by European Society of Cardiology Guidelines34 on cardiac pacing, implantable cardioverter defibrillator and cardiac resynchronisation therapy. However, the European Heart Rhythm Association (EHRA) position paper supports free mobilisation after a CIED procedure.35 In practice this expert consensus is not always received and other studies to clarify the topic have been conceptualised.2,33
There is evidence about the long-term rehabilitation in people with pacemakers, ICDs and CRTs correlated with the benefits arising from the implant therapy.36 Adams et al37 evidence that the American College of Sports Medicine (ACSM) for patients who have undergone pacemaker or ICD implantation speak about traditional resistance training for 4–6 weeks but it does not talk about postoperative bed rest.
As such, It can be stated that there has not been a clear consensus on the question yet.
Immediate postoperative care is an important part of patient assistance. Nurses have a key role in screening and managing patients’ discomfort or complications. Orlando et al2 in a prospective study shows that in the first 24 hours of bed rest many adverse clinical events can occur: delirium, sleep disturbance, severe pain and urinary retention requiring catheterisation.
Simonelli et al,27–29 have had positive results on pain incidence correlated with early mobilisation before the usual care time expected. Pain is an important aspect of patient assistance. Biocic et al38 in their retrospective and prospective study reported that patients can reveal pain during implant procedures but also in the postoperative phase and that often a share and efficacy pain treatment does not exist.
All included studies results do not highlight negative effects of early mobilisation after CIED implantation which differ from the standard or compared care.
It is known that prolonged bed rest may prolong patient hospitalisation and contribute to complications incidence. Hospitalisation may result in rapid functional decline, especially in older adults. One of the major causes is prolonged bed rest and immobility after an operation.7,8
Long bed rest and immobilisation is correlated with the fear of dislocation of the device and the leads and important hematomas; however, Budano et al,22 Miracapillo et al,26 Naffe et al,23 and Simonelli et al,27–29 demonstrated that early mobilisation does not increase the risk of dislodgement at the hematoma onset.
Nevertheless, these evidences are not sufficient to give a clear and unique indication about the correct mobilisation time and modalities because of the different methodological studies approach and intervention type. It can be supposed, anyway, that early mobilisation can be expected. It is not directly correlated with adverse clinical events.
It is interesting and important to notice that the literature on the topic has been increasing over time. Still, other studies on the argument are necessary to contribute to a shared consensus.
Other aspects that the scoping review elucidates are that it may be important to understand not only early mobilisation in the imminent postoperative period but also long-term mobilisation. Collins et al25 and Naffe et al23 with their survey underline that the piece of advice given by team members differs in modalities but also time. Mobilisation after CIED implantation has to be evaluated also in a long-term perspective. One of the excluded studies, not pertinent with our objectives,39 investigated the development of pathologies because of prolonged immobilisation in the shoulder on the affected side in patients with cardiac implantable electronic devices.
Future studies may correlate the lead dislodgement with the type of device and the different shapes and thicknesses. Ghani et al40 in their prospective study demonstrated that risk of dislodgement is not the same for all types of devices. There is a difference between the type and the number of chambers in which the leads are implanted.
It should not be overlooked that studies on same-day CIED implantation discharge have already been conducted. Same-day discharge was not included in this scoping review because the aim was to investigate mobilisation. The studies included in the systematic review and meta-analysis conducted by Trongtorsak et al41 in fact analysed same-day discharge without specifying mobilisation and bed-rest time and modalities. Future studies combining same-day discharge and mobilisation modalities could be interesting.
Another aspect that has to be considered in future studies is the development of leadless pacemaker technology. Nowadays, leadless pacemakers or subcutaneous implantable cardioverter defibrillators are not indicated in all patients and other studies are necessary to compare the short- and long-term efficacy and safety profiles of these pacing devices.42
Our intent was to scope the field of research on the early mobilisation after CIED implantation. The database research has demonstrated that other potential eligible unpublished studies on the topic exist. These studies could have contributed to the results precision. However, this can be a starting point for other reflections and research. Some studies included are written in Italian and this could be an obstacle to the scoping review repetition and inclusion of these studies in other research.
Conclusion
In our scoping review we found that early mobilisation after CIED implantation is a topic increasingly investigated. However, a clear consensus on the argument is not present yet and the studies included in this scoping review demonstrate that there is no statistically significant difference between early mobilisation about more bed rest time after CIED implantation. A methodology that can be used to reduce complications with early mobilisation is the use of a bandage or an arm support. Further studies are needed to support these results and to be sure of any implementation of the clinical practice. However, this evidence supports the need to clarify which is the more appropriate intervention taking into account all the clinical aspects and variability.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Ethical Considerations
An ethical review was not required for this scoping review of previously published works.
Patient Consent
Patient consent was not required for this scoping review of previously published works.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
All authors approved the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The authors report no conflicts of interest in this work.
References
1. Ceroni A, Busca E, Caristia S, et al. Bed rest after cardiovascular implantable electronic device placement: systematic review and meta-analysis. Ann Ist Super Sanità. 2018;54(1):28–34. doi:10.4415/ANN_18_01_07
2. Orlando F, Giuffrida S, Vicari R, et al. Adverse clinical events during the first 24 h of bedrest following cardiac electronic device implantation: a prospective observational study. Eur J Cardiovasc Nurs. 2023;22(2):175–183. doi:10.1093/eurjcn/zvac050
3. Shan R, Ning Y, Ma Y, et al. Prevalence and risk factors of atrioventricular block among 15 million Chinese health examination participants in 2018: a nation-wide cross-sectional study. BMC Cardiovasc Disord. 2021;21(1):289. doi:10.1186/s12872-021-02105-3
4. Lee JH, Lee SR, Choi EK, et al. Temporal trends of cardiac implantable electronic device implantations: a nationwide population-based study. Korean Circ J. 2019;49(9):841. doi:10.4070/kcj.2018.0444
5. Vaidya VR, Asirvatham R, Kowlgi GN, et al. Trends in cardiovascular implantable electronic device insertion between 1988 and 2018 in Olmsted County. JACC Clin Electrophysiol. 2022;8(1):88–100. doi:10.1016/j.jacep.2021.06.006
6. Yokoshiki H, Shimizu A, Mitsuhashi T, et al. Trends in the use of implantable cardioverter‐defibrillator and cardiac resynchronization therapy device in advancing age: analysis of the Japan cardiac device treatment registry database. J Arrhythmia. 2020;36(4):737–745. doi:10.1002/joa3.12377
7. Chen B, Xie G, Lin Y, et al. A systematic review and meta-analysis of the effects of early mobilization therapy in patients after cardiac surgery. Medicine. 2021;100(15):e25314. doi:10.1097/MD.0000000000025314
8. Tazreean R, Nelson G, Twomey R. Early mobilization in enhanced recovery after surgery pathways: current evidence and recent advancements. J Comp Eff Res. 2022;11(2):121–129. doi:10.2217/cer-2021-0258
9. Al-Khatib SM. Cardiac implantable electronic devices. N Engl J Med. 2024;390(5):442–454. doi:10.1056/NEJMra2308353
10. Hiestand B. Cardiac implantable electric devices: indications and complications. Curr Emerg Hosp Med Rep. 2017;5(2):56–63. doi:10.1007/s40138-017-0128-3
11. Rao A, Bennett S. Cardiac implantable electronic devices: an overview for primary care. Br J Gen Pract. 2022;72(721):402–404. doi:10.3399/bjgp22X720461
12. Fowler LH. Nursing management for patients postoperative cardiac implantable electronic device placement. Crit Care Nurs Clin North Am. 2019;31(1):65–76. doi:10.1016/j.cnc.2018.11.007
13. American Society of Anestesiology. Practice advisory for the perioperative management of patients with cardiac implantable electronic devices: pacemakers and implantable cardioverter–defibrillators 2020. Anesthesiology. 2020;132(2):225–252. doi:10.1097/ALN.0000000000002821
14. Reinhardt A, Ventura R. remote monitoring of cardiac implantable electronic devices: what is the evidence? Curr Heart Fail Rep. 2023;20(1):12–23. doi:10.1007/s11897-023-00586-1
15. Lockwood C, Dos Santos KB, Pap R. Practical guidance for knowledge synthesis: scoping review methods. Asian Nurs Res. 2019;13(5):287–294. doi:10.1016/j.anr.2019.11.002
16. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
17. Peters MDJ, Godfrey C, McInerney P, et al. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evidence Synth. 2022;20(4):953–968. doi:10.11124/JBIES-21-00242
18. Barker TH, Stone JC, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synth. 2023;21(3):494–506. doi:10.11124/JBIES-22-00430
19. Aromataris E, Munn Z. Chapter 3: systematic reviews of effectiveness. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. 2020.
20. Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Chapter 5: systematic reviews of prevalence and incidence. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. 2020.
21. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: systematic reviews of etiology and risk. In: JBI Manual for Evidence Synthesis. 2020. doi:10.46658/JBIMES-20-08
22. Budano C, Garrone P, Castagno D, et al. Same-day CIED implantation and discharge: is it possible? The E-MOTION trial (Early MObilization after pacemaker implantaTION). Int J Cardiol. 2019;288:82–86. doi:10.1016/j.ijcard.2019.04.020
23. Naffe A, Iype M, Easo M, et al. Appropriateness of sling immobilization to prevent lead displacement after pacemaker/implantable cardioverter-defibrillator implantation. Baylor University Medical Center Proceedings. 2009;22(1):3–6. doi:10.1080/08998280.2009.11928456
24. Wongcharoen W, Petvipusit W, Prasertwitayakij N, et al. Effect of early pendulum exercise on shoulder function after cardiac rhythm management device implantation. J Interv Card Electrophysiol. 2019;55(3):343–347. doi:10.1007/s10840-019-00541-y
25. Collins G, Hamill S, Laventure C, Newell S, Gordon B. A survey of post-cardiac rhythm device implantation movement and mobilisation advice in the UK. Br J Cardiol. 2019. doi:10.5837/bjc.2019.002
26. Miracapillo G, Costoli A, Addonisio L, et al. Early mobilization after pacemaker implantation. J Cardiovasc Med. 2006;7(3):197–202. doi:10.2459/01.JCM.0000215273.70391.bf
27. Simonelli N, Di Mauro S, Di Minno MND, Salvini L. Livelli di Autonomia dei pazienti sottoposti a impianto di pacemaker cardiaco: studio pilota sugli effetti della mobilizzazione precoce[Patient undergoing cardiac pacemaker implant autonomous levels: pilot study on early mobilisation effects.]. L’Infermiere. 2012;49:1.
28. Simonelli N, Lusignani M, Veglia F, Giovannardi M, Tondo C. Sicurezza e comfort dei pazienti con impianto <BR>di pacemaker mobilizzati dopo 24 e 48 ore: <BR>studio retrospettivo[Safety and comfort of patient with pacemaker implant mobilised after 24 and 48 hours.]. Assistenza Infermieristica e Ricerca. 2014;33(3):127–133. doi:10.1702/1648.18028
29. Simonelli N, Lusignani M, Veglia F, Tedesco C, Tondo C. Mobilità a tre ore dall’impianto di pacemaker: studio degli effetti sulla sicurezza dei pazienti durante il ricovero[Three hours mobility after pacemaker implant: study on patients safety during hospitalisation.]. L’Infermiere. 2018;3.
30. Bradbury-Jones C, Aveyard H, Herber OR, Isham L, Taylor J, O’Malley L. Scoping reviews: the PAGER framework for improving the quality of reporting. Int J Soc Res Methodol. 2022;25(4):457–470. doi:10.1080/13645579.2021.1899596
31. Orlando F, Vicari R, Sansalone A, Dell’Avo A, Giuffrida S, Bernasconi S. Nursing outcomes ed allettamento dopo impianto di device cardiaco: Studio descrittivo presso l’istituto cardiocentrico Ticino. 2021.
32. Feldman A, Freedberg NA, Dante A, Poletaev V, Rosner E, Turgeam Y. Early Mobilization After Cardiac Implantable Electrical Device Implantation (EMCIEDI Trial). 2017.
33. Golian M, Sadek MM, Aydin A, et al. A randomized trial of lenient versus strict arm instruction post cardiac device surgery (LENIENT). Am Heart J. 2023;259:52–57. doi:10.1016/j.ahj.2023.01.016
34. Glikson M, JC Nielsen, MB Kronborg, et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021;42:3427–3520. doi:10.1093/eurheartj/ehab364
35. Burri H, Starck C, Auricchio A, et al. EHRA expert consensus statement and practical guide on optimal implantation technique for conventional pacemakers and implantable cardioverter-defibrillators: endorsed by the heart rhythm society (HRS), the Asia Pacific heart rhythm society (APHRS), and the Latin-American heart rhythm society (LAHRS). EP Europace. 2021;23:983–1008.
36. Iliou MC, JC B, Lamar-Tanguy A, et al. Cardiac rehabilitation in patients with pacemakers and implantable cardioverter defibrillators. Monaldi Arch Chest Dis. 2016;86:1–2. doi:10.4081/monaldi.2016.756
37. Adams J, Cline MJ, Hubbard M, McCullough T, Hartman J. A new paradigm for post-cardiac event resistance exercise guidelines. Am j Cardiol. 2006;97(2):281–286. doi:10.1016/j.amjcard.2005.08.035
38. Biocic M, Vidosevic D, Boric M, et al. Anesthesia and perioperative pain management during cardiac electronic device implantation. JPR. 2017;10:927–932. doi:10.2147/JPR.S132241
39. Findikoglu G, Yildiz BS, Sanlialp M, et al. Limitation of motion and shoulder disabilities in patients with cardiac implantable electronic devices. Int J Rehabil Res. 2015;38(4):287–293. doi:10.1097/MRR.0000000000000122
40. Ghani A, Delnoy PPHM, Ramdat Misier AR, et al. Incidence of lead dislodgement, malfunction and perforation during the first year following device implantation. Neth Heart J. 2014;22(6):286–291. doi:10.1007/s12471-014-0556-6
41. Trongtorsak A, Kewcharoen J, Thangjui S, et al. Same‐day discharge after implantation of cardiac implantable electronic devices: a systematic review and meta‐analysis. Pacing Clin Electrophysiol. 2021;44:1925–1933. doi:10.1007/s12471-014-0556-6
42. Bencardino G, Scacciavillani R, Narducci ML. Leadless pacemaker technology: clinical evidence of new paradigm of pacing. Rev Cardiovasc Med. 2022;23(2):043. doi:10.31083/j.rcm2302043
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.