Back to Journals » Patient Preference and Adherence » Volume 13
What benefits and harms are important for a decision about cervical screening? A study of the perspective of different subgroups of women
Authors van der Meij AE ![]() , Damman OC, Uiters E, Timmermans DRM
, Damman OC, Uiters E, Timmermans DRM ![]()
Received 5 November 2018
Accepted for publication 7 February 2019
Published 1 July 2019 Volume 2019:13 Pages 1005—1017
DOI https://doi.org/10.2147/PPA.S193522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Amber E van der Meij,1 Olga C Damman,1 Ellen Uiters,2 Danielle RM Timmermans1,3
1Amsterdam UMC, Vrije Universiteit Amsterdam, Department of Public and Occupational Health, Amsterdam Public Health Research Institute, Amsterdam, The Netherlands; 2National Institute for Public Health and the Environment (RIVM), Centre for Nutrition, Prevention and Health Services, Bilthoven, The Netherlands; 3National Institute for Public Health and the Environment (RIVM), Bilthoven, The Netherlands
Background: In cervical screening programs, women typically receive information leaflets to support their decision about participation. However, these leaflets are often based on what experts consider important benefits and harms of screening and not what women themselves consider important to know.
Objective: To identify which benefits and harms women consider important for making a decision about cervical screening.
Design: Cross-sectional study.
Setting and participants: Women from the Dutch target group of cervical screening (N=248; 30–60 years), recruited through an online access panel.
Main variables studied: Perceived importance of different benefits and harms of cervical screening, assessed through two rating items (“How important is the information about [this harm/benefit] for your decision?” and “For me it is a [benefit/harm] that participating in the screening program leads to [the benefit/harm]”), and one ranking item (“Rank the information according to their importance for your own choice”).
Results: Women overall considered the benefits of cervical screening more important than the harms or disadvantages. The most important harm according to women was the chance of false positive results (M=4.88; SD=1.75). Differences between those with lower and higher numeracy/health literacy were found regarding several aspects, e.g. for the chance of false positive results, the chance of false negative results, the chance of overtreatment.
Discussion and conclusion: The results suggest that leaflets could include more explicit information about false positive results.
Keywords: informed decision making, cervical screening, risk communication, lay perspective
Introduction
In many western countries, women are invited to participate in a national cervical screening program that involves getting a smear taken (Pap- or HPV (Human Papilloma Virus)-testing)1–3. Pap- and HPV testing are methods of detecting abnormalities which might put women at risk of cervical cancer. These screening programs have been shown to be effective in reducing the incidence of cervical cancers and cervical cancer-related deaths.4,5 Although the benefits of cervical screening outweigh the harms on a population level, this may not be true for each individual woman. As a result, it is increasingly considered important that women become aware of potential harms/disadvantages associated with screening and that they make an informed decision.6 Information leaflets are thus often attached to the invitation and women are usually also provided with a web address for more extended information.7
According to experts in the field of informed decision making, leaflets should contain complete and evidence-based benefit/harm information.8,9 For cervical screening, important benefits are a reduced risk of developing cervical cancer and a reduced risk of cervical cancer-related death.4,5,10 Potential harms or disadvantages of screening include the chance of a false positive test result, possibly leading to psychological distress,11 and the chance of overtreatment, with associated risks of premature births and miscarriages.12,13 A false negative result may also occur, and there may be additional disadvantages of participating in screening, such as costs of further testing after an abnormal test result, and the fact that getting a smear taken can be associated with discomfort, pain, inconvenience or embarrassment.14,15
An important question is what benefit/harm information should be communicated in leaflets in order to support the target audience’s decisions, because in practice, it is often not feasible to provide all information to avoid information overload. Leaflets already contain much other relevant information, for example about how cervical cancer develops and about the procedure of the screening test. Not only are there quite a number of harms and benefits one could weigh, making the decision making process complex, but these aspects also involve probabilities, such as the risk of cervical cancer or the risks of false positive and false negative test results. In practice, this question is usually resolved by letting screening experts decide on the most essential information to be provided. A recent evaluation of cervical screening leaflets in Scandinavian and English-speaking countries showed that most leaflets provide limited information on potential harms of screening.16 Current practice thus seems to result in a narrow overview of benefits and harms. It is unknown whether the selected information is actually the most important information in the perspective of women themselves. Presenting only the most decision-relevant information from the target group’s perspective is however important, to match information to their needs and to motivate them to act on the information.17,18
Until now, women’s information needs as to cervical screening have been understudied. Leaflets are often user-tested among the target population, but these leaflets typically consist of items selected beforehand. In addition, an important question is whether there are differences between subgroups of women19 and what this means for targeted/tailored information provision (also see20). Benefits and harms of cervical screening may not be perceived in the same way, or considered equally important by all groups of women. For example, the risks associated with overtreatment, such as a higher risk of getting a miscarriage or premature birth,13 are likely to be more important for younger women who still have a wish to have children than for relatively older women.20 Because age is an important risk factor for cervical cancer, older women in the target group have a higher cervical cancer risk in general, and screening may therefore be more beneficial to them.10 A recent review on older women’s decisions to participate in cervical screening suggested that reassurance but also embarrassment and perceived logistic aspects were important for older women.20
Women with relatively low numeracy or health literacy may also perceive benefits and harms differently than those with higher skills, and perhaps especially those aspects that involve probability information. It is known that people with lower literacy and numeracy skills can perceive risks differently than those with higher skills, and also seem to be more vulnerable for the influence of contextual cues in forming their risk perception.21 People with lower health literacy as well as those with lower numeracy also tend to have less knowledge about screening and health conditions in general (eg,22–24) which may impact the value attached to a number of aspects. This may concern both “difficult” aspects such as the chances of false positive and false negative test results,25 but also more practical or emotional aspects related to screening such as the inconvenience of the tests involved.26,27 In the context of colorectal cancer screening, for example, Smith and colleagues have reported that people with lower cognitive skills (i.e. numeracy and educational level) are less knowledgeable and less positive about this screening, and also perceive more emotional and practical barriers.23,27 Also for cervical screening, there is some research showing that women from lower SES (Socio-Economic Status) backgrounds have different perceptions and beliefs than those from higher social classes,28 but it is unknown how such subgroups actually value the different benefits and harms directly related to screening.
This study aimed to identify which benefits and harms women consider important for making a decision concerning cervical screening, in an attempt to provide suggestions for improvement of the content of leaflets that are aimed to support informed decision-making of women. We also studied the differences between the following subgroups of women: women of different age groups; women with high educational level versus low educational level; women with high levels of numeracy skills versus low levels of numeracy skills; and women with low levels of health literacy skills versus high levels of health literacy skills.
Methods
The present study was a cross-sectional study using a questionnaire among women in the target group of the Dutch national cervical screening program. This program invites women between 30 and 60 years old to participate in cervical screening. At the time of the present study, the Dutch screening program involved getting a Pap smear taken at the GP (General Practitioner; cytology only, no HPV testing). The study was exempted from review by a medical research ethics committee in accordance with local regulatory guidelines and standards for human subjects’ protection in the Netherlands (Medical Research Involving Human Subjects Act (WMO), 2005).
Participants
Participants were recruited via a Dutch online access research panel (FlyCatcher Internet Research, 20,000 panel members in total, ISO 20252- and ISO 26362-certified). Members of the Flycatcher Panel register voluntarily by means of a ‘double-active-opt-in’ approach. They give explicit consent to be included in the panel. Participation in any survey is completely voluntary and panel members may terminate their panel membership at any time. We invited 538 women between the ages of 30 and 60 years old. Women were ineligible if they had ever had surgery where part of their cervix had been removed. We oversampled low educated women because we wanted to ensure enough women in our sample with relatively low socioeconomic status (SES), health literacy and numeracy. The initial response rate was 55.8% (N=300), but several cases were deleted because participants were either not eligible (N=19), their responses were of bad quality (N=4; these participants either gave the same answer on all questions or they answered the questions too fast to be able to have read them), or because participants did not complete the entire questionnaire (N=29), leading to a final response rate of 46.1% (N=248).
Procedure
Participants read a general study introduction, and were then asked about their screening intentions and perception of the severity of cervical cancer (see variables). These questions were posed to be able to characterize the sample in terms of screening before being exposed to potentially novel information. Next, participants read some minimal background information about the Dutch cervical screening program, about human papilloma virus (HPV) and the relation with cervical cancer, about what the screening program entails, and the implications of the possible screening outcomes. Additionally, they saw an image illustrating the process of HPV developing into cervical cancer. All this information was based on the content of the leaflet of the national cervical screening program of the Dutch National Institute for Public Health and the Environment (RIVM) at the time of our study. After reading the background information, participants were provided with instructions, where we emphasized that we wanted to know their personal opinions and not what they thought other women would think.
Subsequently, participants were provided with the following two pieces of information, which was information that was not provided as such in the then existing leaflet:
- A fact box about benefits and harms of cervical screening expressed through numerical information (see Figure 1).
- A fact box about additional benefits and harms of cervical screening not expressed through numerical information (see Figure 1).
 |
Figure 1 The two presented fact boxes with benefits and harms. |
After seeing each fact box, participants viewed each benefit and harm separately and were provided with items about the importance of these benefits and harms (see variables). Finally, questions about socio-demographic variables, health literacy and numeracy were posed and participants were thanked for participation.
Materials
Nine benefits and harms were selected in consultation with communication specialists working at the Centre for Population Screening (CvB) of the RIVM, which is the center that coordinates the Dutch cervical screening program. The selection was based on the extended information on the RIVM website at that time as well as on what women from the target group had emphasized in previous qualitative user testing of the CvB (To put this in context: the current leaflet of the Dutch screening program lists only one benefit (reduced risk of getting cervical cancer) and one harm (unnecessary treatment). These aspects are textually described without providing numerical risk information). The following benefits and harms were selected:
- the reduced risk of getting cervical cancer;
- the reduced risk of dying from cervical cancer;
- the chance of an abnormal result, which later turns out to be incorrect (false positive result);
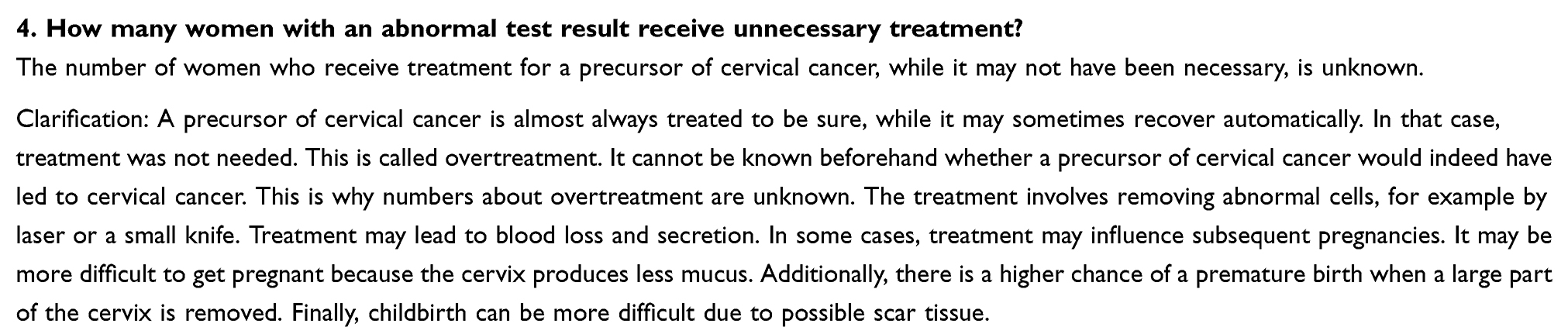
- the chance of unnecessary treatment;
- the chance of a falsely reassuring result (false negative result);
- the costs of the test (consisting of two parts: the initial test is free of charge and follow-up testing may not be free of charge, depending on insurance and deductible);
- the fact that getting a smear taken can be unpleasant;
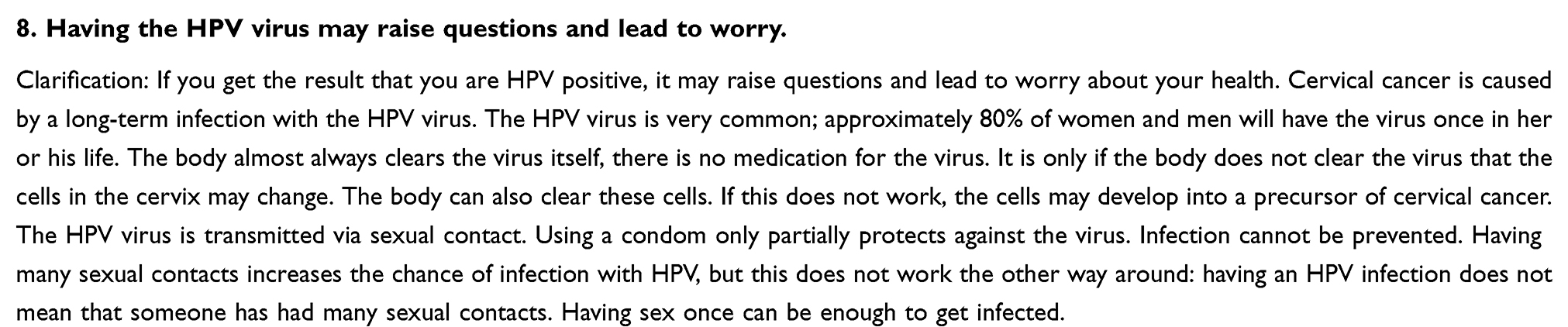
- the fact that having the HPV virus can lead to questions and worry;
- the fact of knowing where you stand and therefore being reassured.
As can be seen from our selection of benefits and harms, we focused on aspects that can be considered advantages or disadvantages of the screening itself, and not so much on aspects that are known barriers for screening, such as access or distance to screening. We do acknowledge that such factors also influence women’s decisions, but these were not considered as direct disadvantages of the screening itself. An exception was made for “costs”; this can be seen as a barrier, but is qualified as a potential disadvantage in the Dutch leaflet.
The first fact box additionally provided the risk of dying from another type of cancer as a comparative anchor value; the second fact box presented getting the smear taken both as a harm (it can be unpleasant) and as a benefit (it usually does not hurt). The first fact box contained numerical probability information displayed in frequencies (X in 100,000, Figure 1), based on fact box design principles.29–31 The second fact box consisted of benefits and harms not expressed by numbers. Examples of the way the separate benefits and harms were presented are shown in Figure 2 (Figure S1 provides the complete list). These aspects were described in the leaflet through text without providing numerical information.
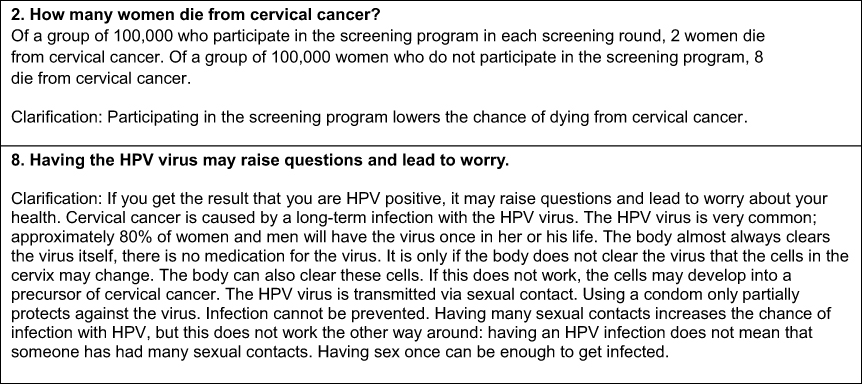 |
Figure 2 Two of the nine benefits and harms when presented separately with additional explanation. |
Variables
Items before being exposed to the two fact boxes with benefits and harms
- Screening intentions: “If I were to be invited to participate in the cervical screening program right now, I would participate” (7-point Likert scale from 1 (I would definitely not participate) to 7 (I would definitely participate)).
- Perception of severity of cervical cancer: “Cervical cancer is a ...” (7-point Likert scale from 1 (completely non-severe condition) to 7 (very severe condition)).
Items about the importance of the benefits and harms after being exposed to the two fact boxes
For each benefit and harm, women were asked to respond to three items:
- “How important is the information about [this harm/benefit] for your decision?” (7-point Likert scale from 1 (very unimportant) to 7 (very important)).
- “For me it is a [benefit/harm] that participating in the screening program leads to [the benefit/harm]” (7-point Likert scale from 1 (totally disagree) to 7 (totally agree)).
- “Rank the following information from parts 1 and 2 of this questionnaire according to their importance for your own choice to participate in the screening program or not. Give the number 1 to the benefit/harm you find the most important, number 2 to the benefit/harm you find the second most important, etc. Give the number 9 to the benefit/harm you find the least important. There are 9 benefits/harms in total.” (Based on these rankings, we calculated the average rankings for all the benefits and harms).
Although the second and third item measured the perceived importance less directly than the first question, we explicitly chose to pose multiple (i.e. three)items, to be able to get a firm idea of the importance attached to different aspects.32 The ranking question was explicitly added because we expected that participants might give high importance ratings to all benefits and harms presented. Ranking more directly forces participants to prioritize aspects.
Health literacy and numeracy
Health literacy was measured using the NVS-D,33,34 which measures performance-based health literacy by letting participants read a nutrition label and answering six questions. We split the participants into two groups; those who had five or six questions correct (relatively high health literacy) and those who had less than five questions correct (relatively low health literacy). Fransen and colleagues showed that with this cut-off point, 63% of the people with adequate health literacy could be identified and 70% of the people with inadequate health literacy.34 Numeracy was measured using a one-item version of the Berlin Numeracy (Out of 1,000 people in a small town 500 are members of a choir. Out of these 500 members in the choir 100 are men. Out of the 500 inhabitants that are not in the choir 300 are men. What is the probability that a randomly drawn man is a member of the choir? Please indicate the probability in percent. ___ %) test. We used a median split, dividing the participants into two groups; relatively low and relatively high numeracy.35 Participants were allowed to skip the questions about health literacy and numeracy. Women who did so were given a score of 0 and treated as low numeracy/health literacy.
Analyses
Descriptive analyses were performed to identify which benefits and harms were considered most important. Next, we performed several one-way ANOVAs to study the subgroup differences, with age, education, numeracy and health literacy as the independent variables and the perceived importance score (How important is the information about [this harm/benefit] for your decision?) as the dependent variable. We conducted post hoc tests if the ANOVA revealed significant group differences for age and education (i.e. p< .05).
Results
Participants’ characteristics
Our sample consisted of 248 women between 30 and 60 years old. Table 1 shows their characteristics; their average age was 45.8 years and half of them (51.2%) were low educated. Most participants stated that they would participate in cervical screening if they were to be invited right now; 68.1% stated that they would definitely participate and 13.3% that they would probably do so. In the actual current Dutch cervical screening program, approximately two-thirds of the invited women participate every year.36 A total of 90.2% of our participants considered cervical cancer to be a severe or very severe condition.
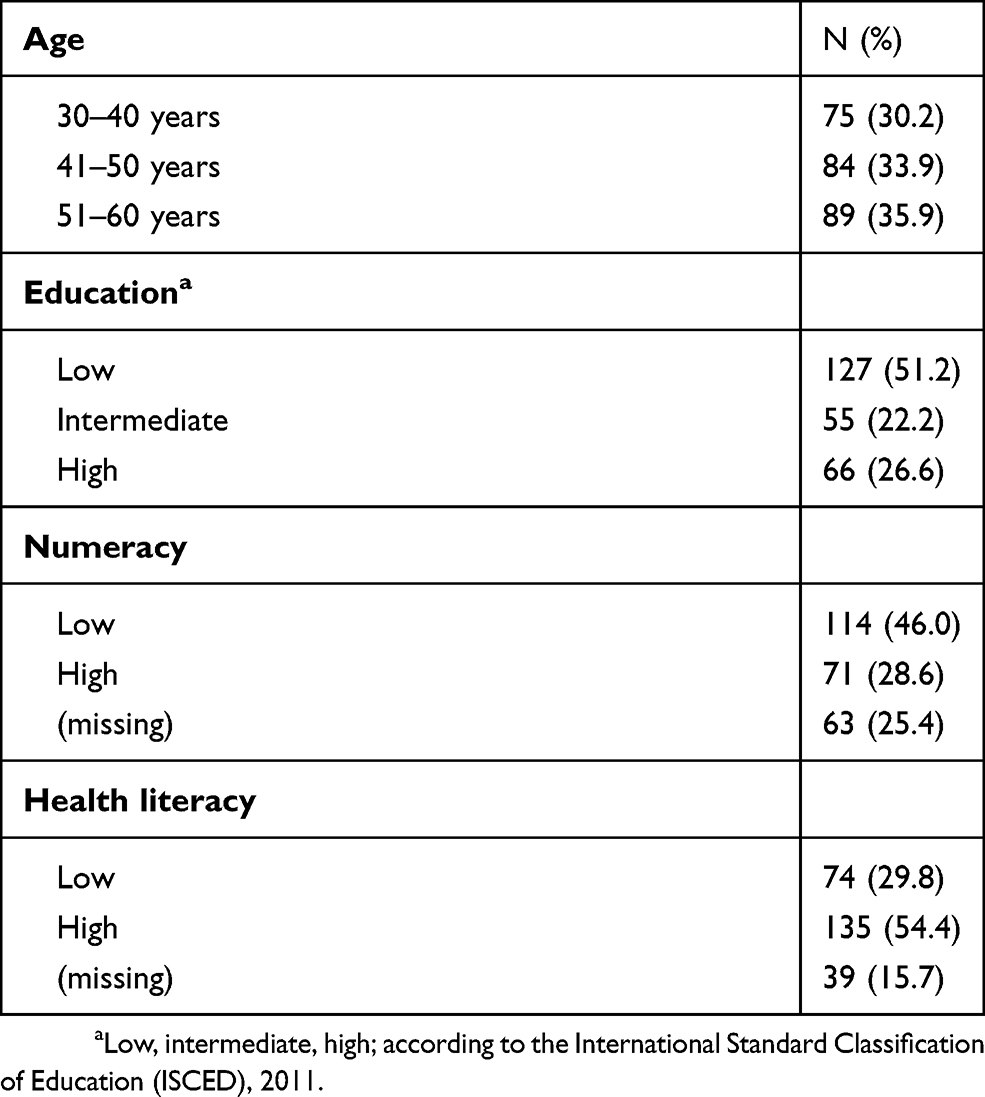 |
Table 1 Participants’ characteristics. Missing values were not analyzed |
Importance of the benefits and harms
Table 2 shows the average scores participants gave concerning the perceived importance as well as the extent to which they perceived the benefits and harms to actually be a benefit or harm. Participants attached most importance to the reduced risk of dying from cervical cancer (M=5.37, SD=1.79) and the least importance to the fact that getting a smear taken can be unpleasant (M=4.35, SD=1.86). For the harms, the chance of getting an abnormal result only to find out later that nothing was wrong (i.e. a false positive result) was considered most important (M=4.88, SD=1.75). In general, participants rated the benefits as being more important than harms; the average importance score over all benefits was 5.05 (SD=1.25) whereas for the harms this was 4.55 (SD=1.36) (difference t(247)=8.01, p<.001), although it should be noted that this difference was quite small. Participants also considered the presented benefits to be actual benefits (overall average score M=5.63 (SD=1.01)) more than they considered the presented harms to be actual harms (overall average score M=4.12 (SD=1.13) (difference t(247)=15.96, p<.001).
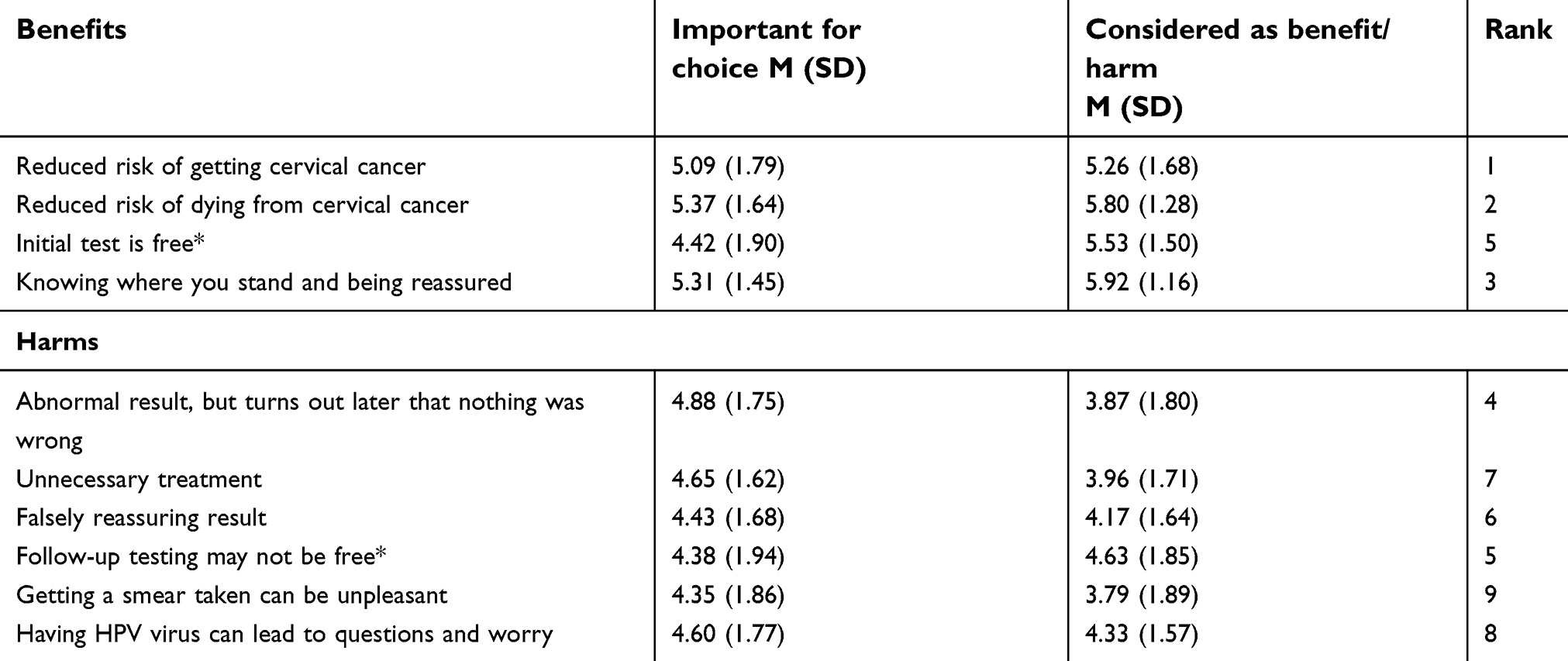 |
Table 2 Average importance scores for each benefit and harm, with possible scores ranging from 1 to 7 |
The average top 3 (out of 9), resulting from participants’ ranking consisted of only benefits (i.e. the reduced risk of getting cervical cancer, the reduced risk of dying from cervical cancer, and the fact that the test result can be reassuring). The highest ranked harm (number 4) was the chance of getting an abnormal result only to find out later that nothing was wrong (i.e. false positive result).
Group differences
Table 3 displays all average importance scores among different subgroups. Age groups were not found to differ with regard to perceived importance. Participants with low educational level considered the costs of screening more important than intermediate and highly educated participants (F(2,245) =4.01, p= .019), F(2,245) =7.96, p< .001). Participants with low numeracy considered unnecessary treatment (F(1,246) =6.20, p= .013) and a falsely reassuring result (false negative result) (F(1,246) =11.38, p= .001)) more important than those with high numeracy. Furthermore, low numerate participants considered the fact that having the HPV virus can lead to questions and worry also more important (F(1,246) =4.18, p= .042). Similar differences were found between participants with lower health literacy and higher health literacy(see Table 3). For health literacy, we also found differences with regard to the chance of an abnormal test result (F(1,246) =5.43, p= .021), the fact that the initial test is free (F(1,246)=4.01), p= .046), the possible costs of follow-up testing (F(1,246) =10.16, p= .002) and the fact that getting a smear taken can be unpleasant (F(1,246) =8.49, p= .004). In particular, those with relatively low health literacy attached more importance to the costs and that getting a smear taken can be unpleasant compared to those with relatively high health literacy. Given the fact that there was some overlap between findings for numeracy and health literacy, we also assessed the correlation between these measures and this correlation was .365 (p< .001).
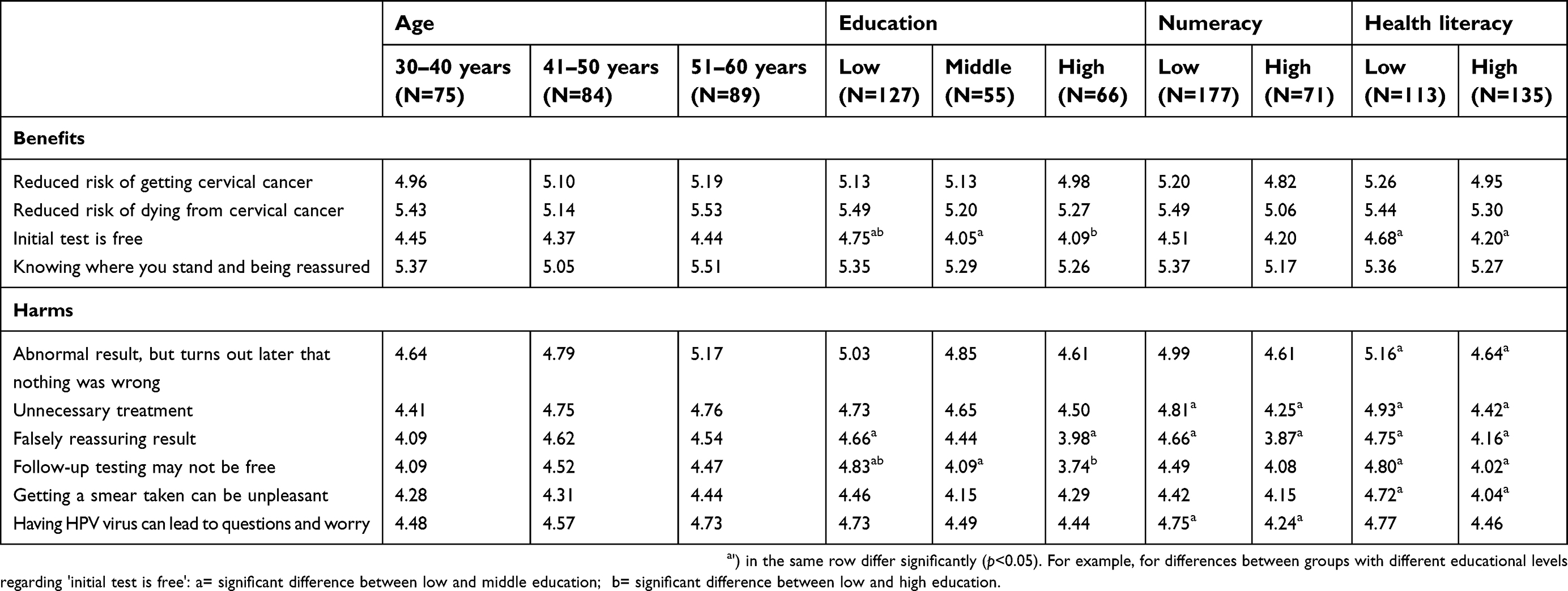 |
Table 3 Mean perceived importance scores are presented |
Discussion
This study aimed to investigate which benefits and harms women from the target population of cervical screening considered important for making a decision concerning this screening. In doing so, we also studied differences between subgroups of women regarding age, educational level, numeracy and health literacy. Women appeared to attach more importance to a number of benefits compared to the harms, namely: the reduced risk of getting cervical cancer, the reduced risk of dying from cervical cancer, and that they know where they stand and can therefore be reassured by the test result. The harm or disadvantage considered most important was the chance of getting an abnormal test result only to find out later that nothing was wrong (i.e. false positive result). We also demonstrated several subgroup differences in the importance attached to a number of benefits and harms, for example that women with lower numeracy/health literacy considered the chances of unnecessary treatment and a falsely reassuring result (false negative result) more important than women with higher numeracy/health literacy.
Women overall considered the benefits of cervical screening more important than the harms. Related to this, women did not consider most of the harms presented in this study to be actual harms for themselves. This finding corresponds to other studies showing positive attitudes in general towards cervical screening as well as towards other screening programs.37,38 One could argue that this overall importance attached to screening benefits is not problematic for cervical screening, because the possible harms or disadvantages are considered relatively small compared to, for example, breast cancer screening. When women are properly informed about benefits and harms, it can be argued that it is up to women themselves how they weigh the benefits and harms. However, a positive attitude toward cervical screening and (cancer) screening in general may also be rooted in a common positive societal attitude. Such an attitude may have an unwarranted effect on information processing, for example a positivity bias in information search and in weighing the harms against the benefits. Although cervical screening does actually not test for cancer, but for abnormalities which might put women at risk of cervical cancer, the benefits in terms of reduced risk of getting cervical cancer and of dying from cervical cancer will probably play a similar role in decision making as in actual cancer screening. For cancer screening in general, we know that it is not only the general public that is generally positive, but that experts seem to be positive as well.39 For example, information guidelines for clinicians regarding cancer screening have been shown to be not neutral, lacking information in general (mostly about the harms), or only consisting of non-numerical information.40 This may mean that even when benefit/harm information is adequately provided to the public, people may not process this information neutrally, but instead focus on positive information. Cervical screening can be harmful to individual women12,13. (e.g. unnecessary treatment, anxiety and stress associated with screening and with false positive or false negative results), and we therefore believe that women should be aware of these possible harms/disadvantages when making a decision.
We found a number of differences in perceived importance of benefits and harms between women with lower numeracy/health literacy and women with higher numeracy/literacy. Notably, these differences mostly concerned the harms, including the harms expressed by numerical information, but also some of the benefits. For example, women with lower numeracy/health literacy considered the chance of overtreatment and the chance of a false negative result relatively more important compared to those with higher numeracy/health literacy. It could be that those with lower skills specifically focused on these harms, because they were notable in the accompanying fact box and looked more easy to compare than the numbers relating to the benefits (i.e. there was no comparative information about harms for the option of not screening). An alternative explanation might be that the numerical fact box was always presented first to participants, and that those with lower skills did not pay much attention to information in the second fact box. Of course it can also be that those with lower numeracy/health literacy actually intrinsically attached more importance to the harms than those with higher skills, from a more negative attitude or skepticism towards screening23,27 and thus processed the benefit/harm information in light of this. Such differences could be related to the socio-economic position of women with lower numeracy/health literacy, although it should be said that we did not find that much difference between educational levels.
An important finding was that the costs of the screening program were especially important for women with a lower educational level. It makes sense that women with a low educational level consider this more important since they often have less money to spend. It is important to present the information about the costs of screening in such a way that all women can understand it, because information about costs and insurances can be difficult to understand. This may depend on the way screening is financed in different countries. In the Netherlands, the smear in the screening program is free of charge, but further testing may lead to costs, depending on women’s health insurance and particularly their deductible.
Strengths and limitations
To our knowledge, the present study is the first that looks into the perspective of women themselves regarding how much importance they attach to the benefits and harms of cervical screening, including aspects presented through numerical probability information. Our study might be limited by its exploratory nature, which is why we cannot be sure about the reasons why women find particular aspects important and not others. We acknowledge the online lab setting in which our study was performed, which might have biased participants in putting more effort in the information content than what they would normally do at home when receiving a leaflet. However, we do think that the materials used were adequate for our research purposes, as we were interested in how women perceived different potential benefits and harms, which are not all provided in current leaflets.
The way we processed the data about numeracy and health literacy may have led to some bias in our data. Participants were allowed to skip these questions, and, following Cokely et al35 we considered the missing data as incorrect (i.e. low numeracy and health literacy). Additional analysis showed that women with missing data on these questions were also more often low educated. It could be that those women were the ones with the lowest levels of health literacy and numeracy, leading to an underestimation of the differences between the low and high skilled groups.
Practice implications
Our findings suggest that more explicit information about the chances of false positive results could be provided in leaflets about cervical screening. This aspect is not typically given in cervical screening leaflets,16 while in the present study women considered it to be the most important possible harm or disadvantage of screening. Aspects that seem to be relatively less important to emphasize in information leaflets are the fact that getting a smear taken can be unpleasant and that having the HPV virus can lead to questions and worry. Such information may be referred to in web-based materials.
In our sample, most participants intended to participate in cervical screening and it therefore seems reasonable that they would consider the benefits more important than the harms. Only a few participants stated they would not participate. This is however in line with the actual target population of the Dutch cervical screening program, where approximately two-thirds of the invited women participate every year. It would be interesting to compare women who participate in the screening program to women who do not, to see whether their information needs are different.
An important question remains whether information about benefits and harms should be tailored to different groups of people. Web-based information may offer opportunities to do so. However, based on our findings, we have reason to believe that differences in the perceived importance of information items might be, at least in part, related to differences in how particular subgroups of women understood these items, especially some of the numerical information. Further studies are needed to unravel the mechanisms behind these patterns. Nonetheless, leaflets about cervical screening should at least contain balanced information about the possible benefits and harms. Information about the possible harms is generally more difficult for women to understand because it contains numerical information, very small probabilities and reflects risks that are less concrete or less affective compared to the chance of preventing getting cervical cancer or dying from it. However, not providing those numbers often leads to an even larger overestimation according to previous research41 and we would therefore not recommend presenting only non-numerical information.
Acknowledgments
The authors would like to thank Marleen Haaijer for her assistance in collecting the data. In addition, the authors acknowledge the contribution of the national cervical screening program of the Dutch National Institute for Public Health and the Environment (RIVM) in the development of the stimulus materials.
Disclosure
The authors declare they have no conflicts of interest.
References
1. Anttila A, Ronco G, Clifford G, et al. Cervical cancer screening programmes and policies in 18 European countries. Br J Cancer. 2004;91(5):935–941. doi:10.1038/sj.bjc.6602069
2. Linos A, Riza E. Comparisons of cervical cancer screening programmes in the European Union. Eur J Cancer. 2000;36(17):2260–2265.
3. Tota J, Ramana–Kumar A, El-Khatib Z, Franco E. The road ahead for cervical cancer prevention and control. Cur Oncol. 2014;21(2):e255. doi:10.3747/co.21.1720
4. Quinn M, Babb P, Jones J, Allen E. Effect of screening on incidence of and mortality from cancer of cervix in England: evaluation based on routinely collected statistics. BMJ. 1999;318(7188):904. doi:10.1136/bmj.318.7188.904
5. Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev. 2010;19(8):1893–1907. doi:10.1158/1055-9965.EPI-10-0437
6. Briss P, Rimer B, Reilley B, et al. Promoting informed decisions about cancer screening in communities and healthcare systems. Am J Prev Med. 2004;26(1):67–80.
7. Forbes C, Jepson R, Martin-Hirsch P. Interventions targeted at women to encourage the uptake of cervical screening. Cochrane Database Syst Rev. 2002;(3):CD002834..
8. Gigerenzer G. Towards a paradigm shift in cancer screening: informed citizens instead of greater participation. BMJ. 2015;350:h2175. doi:10.1136/bmj.h2175
9. Wegwarth O, Kurzenhäuser-Carstens S, Gigerenzer G. Overcoming the knowledge–behavior gap: the effect of evidence-based HPV vaccination leaflets on understanding, intention, and actual vaccination decision. Vaccine. 2014;32(12):1388–1393. doi:10.1016/j.vaccine.2013.12.038
10. Sasieni P, Castanon A, Cuzick J. Effectiveness of cervical screening with age: population based case-control study of prospectively recorded data. Bmj. 2009;339:b2968. doi:10.1136/bmj.b2651
11. Lerman C, Miller SM, Scarborough R, Hanjani P, Nolte S, Smith D. Adverse psychologic consequences of positive cytologic cervical screening. Am J Obstet Gynecol. 1991;165(3):658–662.
12. Korfage IJ, Essink-Bot M-L, Westenberg SM, Helmerhorst T, Habbema JDF, van Ballegooijen M. How distressing is referral to colposcopy in cervical cancer screening?: A prospective quality of life study. Gynecol Oncol. 2014;132(1):142–148. doi:10.1016/j.ygyno.2013.11.001
13. Kyrgiou M, Koliopoulos G, Martin-Hirsch P, Arbyn M, Prendiville W, Paraskevaidis E. Obstetric outcomes after conservative treatment for intraepithelial or early invasive cervical lesions: systematic review and meta-analysis. Lancet. 2006;367(9509):489–498. doi:10.1016/S0140-6736(06)68181-6
14. Waller J, Bartoszek M, Marlow L, Wardle J. Barriers to cervical cancer screening attendance in England: a population-based survey. J Med Screen. 2009;16(4):199–204. doi:10.1258/jms.2009.009073
15. Van Til L, MacQuarrie C, Herbert R. Understanding the barriers to cervical cancer screening among older women. Qual Health Res. 2003;13(8):1116–1131. doi:10.1177/1049732303255975
16. Kolthoff SK, Hestbech MS, Jørgensen KJ, Brodersen J. Do invitations for cervical screening provide sufficient information to enable informed choice? A cross-sectional study of invitations for publicly funded cervical screening. J R Soc Med. 2016;109(7):274–281.
17. Hibbard JH, Peters E. Supporting informed consumer health care decisions: data presentation approaches that facilitate the use of information in choice. Annu Rev Public Health. 2003;24(1):413–433. doi:10.1146/annurev.publhealth.24.100901.141005
18. Evans JSB. In two minds: dual-process accounts of reasoning. Trends Cogn Sci. 2003;7(10):454–459.
19. Eiser JR, Cole N. Participation in cervical screening as a function of perceived risk, barriers and need for cognitive closure. J Health Psychol. 2002;7(1):99–105. doi:10.1177/1359105302007001657
20. Hope KA, Moss E, Redman CW, Sherman SM. Psycho-social influences upon older women‘s decision to attend cervical screening: a review of current evidence. Prev Med. 2017. doi:10.1016/j.ypmed.2017.05.002
21. Peters E. Beyond comprehension the role of numeracy in judgments and decisions. Curr Dir Psychol Sci. 2012;21(1):31–35. doi:10.1177/0963721411429960
22. Smith SG, Forster AS, Kobayashi LC. Predictors of human papillomavirus awareness and knowledge in 2013. Am J Prev Med. 2015;49(1):e5–e7. doi:10.1016/j.amepre.2015.03.013
23. Smith SG, Kobayashi LC, Wolf MS, Raine R, Wardle J, von Wagner C. The associations between objective numeracy and colorectal cancer screening knowledge, attitudes and defensive processing in a deprived community sample. J Health Psychol. 2016;21(8):1665–1675. doi:10.1177/1359105314560919
24. Pignone MP, DeWalt DA. Literacy and health outcomes: is adherence the missing link? J Gen Intern Med. 2006;21(8):896–897. doi:10.1111/j.1525-1497.2006.00545.x
25. Smith SK, Barratt A, Trevena L, Simpson JM, Jansen J, McCaffery KJ. A theoretical framework for measuring knowledge in screening decision aid trials. Patient Educ Couns. 2012;89(2):330–336. doi:10.1016/j.pec.2012.07.009
26. Dolan NC, Ferreira MR, Davis TC, et al. Colorectal cancer screening knowledge, attitudes, and beliefs among veterans: does literacy make a difference? J Clin Oncol. 2004;22(13):2617–2622. doi:10.1200/JCO.2004.10.149
27. Smith S, McGregor L, Raine R, Wardle J, Wagner C, Robb K. Inequalities in cancer screening participation: examining differences in perceived benefits and barriers. Psycho‐Oncology. 2016;25(10):1168–1174. doi:10.1002/pon.4195
28. Tacken MA, Braspenning JC, Hermens RP, et al. Uptake of cervical cancer screening in The Netherlands is mainly influenced by women‘s beliefs about the screening and by the inviting organization. Eur J Public Health. 2006;17(2):178–185. doi:10.1093/eurpub/ckl082
29. Schwartz LM, Woloshin S, Welch HG. The drug facts box: providing consumers with simple tabular data on drug benefit and harm. Med Decis Making. 2007. doi:10.1177/0272989X07306786
30. Schwartz LM, Woloshin S. The drug facts box: improving the communication of prescription drug information. Proc National Acad Sci. 2013;110(Supplement 3):14069–14074. doi:10.1073/pnas.1214646110
31. Gigerenzer G. Breast cancer screening pamphlets mislead women. BMJ. 2014;348:g2636.
32. Ryan M, Scott DA, Reeves C, et al. Eliciting public preferences for healthcare: a systematic review of techniques. Health Technol Assess. 2001;5(5):1–186.
33. Fransen M, Van Schaik T, Twickler T, Essink-Bot M. Applicability of internationally available health literacy measures in the Netherlands. J Health Commun. 2011;16(sup3):134–149. doi:10.1080/10810730.2011.604383
34. Fransen MP, Leenaars KE, Rowlands G, Weiss BD, Maat HP, Essink-Bot M-L. International application of health literacy measures: adaptation and validation of the newest vital sign in The Netherlands. Patient Educ Couns. 2014;97(3):403–409. doi:10.1016/j.pec.2014.08.017
35. Cokely ET, Galesic M, Schulz E, Ghazal S, Garcia-Retamero R. Measuring risk literacy: the Berlin numeracy test. Judgm Decis Mak. 2012;7(1):25.
36. Van Ballegooijen M, Rebolj M, Essink-Bot M, Meerding W, Berkers L, Habbema JJREM. De effecten en kosten van het bevolkingsonderzoek naar baarmoederhalskanker in Nederland na de herstructurering [The effects and costs of the cervical cancer screening program in the Netherlands after the reorganization] . Rotterdam, Dutch: ErasmusMC; 2006.
37. Douma LN, Uiters E, Timmermans DR. The Dutch public are positive about the colorectal cancer-screening programme, but is this a well-informed opinion? BMC Public Health. 2016;16(1):1208. doi:10.1186/s12889-016-3870-7
38. Hudson B, Zarifeh A, Young L, Wells JE. Patients‘ expectations of screening and preventive treatments. Ann Fam Med. 2012;10(6):495–502. doi:10.1370/afm.1407
39. Wegwarth O, Wagner GG, Gigerenzer G. Can facts trump unconditional trust? Evidence-based information halves the influence of physicians’ non-evidence-based cancer screening recommendations. PLoS One. 2017;12(8):e0183024. doi:10.1371/journal.pone.0183024
40. Caverly TJ, Hayward RA, Reamer E, et al. Presentation of benefits and harms in US cancer screening and prevention guidelines: systematic review. J Natl Cancer Inst. 2016;108(6):djv436. doi:10.1093/jnci/djv436
41. Peters E, Hart PS, Tusler M, Fraenkel L. Numbers matter to informed patient choices a randomized design across age and numeracy levels. Med Decis Making. 2014;34(4):430–442. doi:10.1177/0272989X13511705
Supplementary material
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.