Back to Journals » Journal of Healthcare Leadership » Volume 17
Wellness-Centered Leadership: A Key Differentiator for Successfully Reducing Burnout and Building a Culture of Well-Being Among Physicians and APPs
Authors Hartung K, Swann-Thomsen HE ![]() , Schneider KR
, Schneider KR
Received 2 January 2025
Accepted for publication 1 April 2025
Published 24 April 2025 Volume 2025:17 Pages 145—157
DOI https://doi.org/10.2147/JHL.S513209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Krispen Hartung,1 Hillary E Swann-Thomsen,2 Kathryn R Schneider1
1Physician and APP Well-Being Center of Excellence, St. Luke’s Health System, Boise, ID, USA; 2Applied Research Division, St. Luke’s Health System, Boise, ID, USA
Correspondence: Kathryn R Schneider, Physician and APP Well-being Center of Excellence, St. Luke’s Health System, 190 E Bannock St, Boise, ID, 83712, USA, Email [email protected]
Abstract: Physician and advanced practice provider (APP) burnout is a significant issue in healthcare, exacerbated by the COVID-19 pandemic. Burnout rates remain high, with severe implications for both clinicians and patient care. This paper acknowledges the multifaceted causes of burnout, including environmental and individual factors, and evaluates the effectiveness of wellness-centered leadership as a mitigation strategy. St. Luke’s Health System implemented a comprehensive wellness-centered leadership program, including training and toolkits, to improve well-being. Surveys conducted in 2022, 2023, and 2024 assessed burnout levels, feeling valued by the organization, intent to leave, and leadership alignment among physicians and APPs. Results indicated a decrease in burnout and intent to leave, alongside improved leadership alignment, and improved feeling valued by the organization. The findings suggest that wellness-centered leadership can significantly reduce burnout and enhance job satisfaction, highlighting the importance of leading with well-being in healthcare settings.
Keywords: organizational culture, workforce development, employee retention, job satisfaction, leadership development
Introduction
Physician and advanced practice provider (APP), such as physician assistants, nurse practitioners, and other clinicians, burnout is a critical and escalating issue within modern healthcare, with profound consequences not only for clinicians but also for the patients they serve. Burnout has reached alarming levels, peaking during the COVID-19 pandemic at above 50% nationally, and while they have slightly decreased, they remain near that level.1–4 Notably, there is a dearth of literature examining burnout in APPs with most existing data focusing on burnout among physicians. However, limited studies have found that rates of burnout among APPs, particularly physician assistants, are similar to physician burnout rates but may be lower.5–7 This is supported by additional research examining burnout among nurse practitioners that found that around 25% of respondents endorsed burnout.8 Collectively, these findings point to lower rates of burnout among APPs compared to physicians. Existing literature has well established that the consequences of burnout are widespread and worth critical attention. Physician suicide rates and suicidal ideation, often linked to burnout, continue to raise significant concerns due to the continued high prevalence.9–11 Growing evidence also suggests burnout negatively affects patient outcomes through sub-optimal or lowered standards of care,12–15 increased medical errors,16 and increased healthcare costs, particularly through clinician attrition.17,18
Addressing physician and APP burnout and well-being requires a multi-faceted approach that includes both environmental (ie, system and institutional) and individual factors.15,19 Historically, individual factors have been the focus of burnout and include personality or temperament, interpersonal skills, coping strategies, personal experiences, gender, age, moral distress, and resilience among others.15,19 Existing research has demonstrated that physicians are already among the most resilient professionals and expecting them to simply “be more resilient” is insufficient.20 Individual support, not resiliency training, includes peer-to-peer support, access to counseling, removal of fear of retaliation from accessing mental health resources, and personal development such as coaching. More focus is now placed on the environmental drivers of burnout, which broadly include work environment and processes, workload and administrative demands, leadership and team dynamics, work–life balance and autonomy, and social and psychological support.15,19 Notably, expert opinion suggests that environmental factors account for 80% of the drivers of burnout, whereas individual factors account for only 20%.21,22 As such, the focus has shifted from emphasizing individual responsibility to addressing organizational and systematic factors that contribute to burnout and acknowledges that the solution lies in transforming healthcare organizations to better support clinicians at the institutional level.
One promising strategy to mitigate burnout is wellness-centered leadership. This leadership model prioritizes the well-being of clinicians by emphasizing the role of healthcare leaders in fostering a culture that supports the well-being of those they lead, integrates wellness practices into their leadership style, and promotes meaningful work. Wellness-centered leadership also focuses on developing leaders who actively engage with their teams, cultivate meaningful relationships, recognize and support individuals, and promote a culture of gratitude and feedback which can have a significant impact on reducing burnout and enhancing job satisfaction.23,24 The core tenets of wellness-centered leadership are drawn from important scholarly leadership models, including transformational leadership, situational leadership, and interpersonal power in leadership.24 Additionally, addressing systemic issues such as inefficient workflows, lack of autonomy, poor teamwork, and inadequate leadership alignment must be considered in all leadership decisions. Research has shown that leadership engagement is a key factor in reducing burnout. For instance, a study found that for each 1-point increase in a composite of leadership engagement behaviors that physician leaders demonstrated, physician burnout decreased 3% and job satisfaction increased 9%23 Essential elements of wellness-centered leadership include caring for people, cultivating team relationships, and inspiring change.24 Successful leaders in this model lead by example, promote well-being, foster open and transparent communication, and build consensus and alignment.
Ultimately, wellness-centered leadership provides a framework for healthcare organizations to systematically reduce burnout, improve well-being, and create a high-performing, patient-focused workforce. By focusing on both the structural and interpersonal elements of healthcare delivery, organizations can better support the clinicians who are the backbone of the healthcare system. This approach not only improves the work environment for physicians and APPs but also leads to better patient care outcomes, reduced healthcare costs, and a more sustainable and effective healthcare system overall.
Initiating the Organizational Well-Being Journey
Physician and APP Well-Being Center of Excellence
St. Luke’s Health System is the only state-based, not-for-profit, community-owned and community-led health system within Idaho. The health system is composed of 8 medical centers, over 1000 staffed beds, more than 370 clinics and centers, and approximately 17,000 employees and 2000 physicians and APPs on medical staff. In 2021, St. Luke’s Health System established its Physician and APP Well-being Center of Excellence (CoE), in response to increasing national evidence demonstrating the relationship between burnout and patient outcomes, with a vision to transform the culture of physician and APP well-being and ensure that impacts to well-being are considered in all strategic and operational decisions. The CoE was responsible for the creation of a system physician and APP well-being strategy and continues to maintain and adapt the strategy. In addition, the CoE plans, coordinates, and measures existing well-being efforts and programs while promoting physician and APP well-being resources systemwide.
Organizational Biopsy and Physician and APP Well-Being and Burnout Survey
In 2022, the CoE completed the American Medical Association’s (AMA) Organization Biopsy. This process included an online survey, including the Mini Z 2.0 burnout and well-being survey to identify key drivers of burnout among physicians and APPs. Additional questions related to respondent demographics, work pace, electronic health record (EHR) frustration, stress, team dynamics, and supportive work environment were also included in the survey for a total of 60 questions. A total of 1977 employed, contracted, and independent physicians and APPs of the health system (all physicians and APPs on med staff) were recruited via internal email from system leadership for participation in an online anonymous survey. The survey remained open for approximately 4 weeks and reinforcement communications were shared through system websites, existing weekly physician and APP communications, as well as service line leader communications. A final reminder was sent in the last week from the CoE to all physicians and APPs on med staff. There was a 29% response rate (n = 573) with physicians accounting for 57% of respondents compared to 43% for APPs. A descriptive profile of respondent characteristics can be found in Table 1. Approximately 55% of respondents endorsed feeling burnout at some level, ranging from at least one or more symptoms of burnout to feeling completely burned out, and nearly 40% of respondents reported moderate-to-high likelihood of leaving the organization within 2 years (see Table 2). Less than half of respondents (44%) reported feeling valued by the organization. Physicians were more likely to endorse feeling burnout at some level compared to APPs (χ2= 6.98 (1, N = 573), p = 0.008; see Figure 1A); however, feeling valued by the organization (see Figure 1B) and likelihood to leave the organization (see Figure 1C) were not significantly different across physicians and APPs (p = 0.07 and p = 0.06, respectively). Despite high rates of burnout, most respondents indicated that their professional values were well aligned with their direct leader (79%), with their service line leaders (63%), and with system leadership (54%) as shown in Table 2. Physicians and APPs reported similar rates of direct leader value alignment (p = 0.52; see Figure 1D), however APPs were more likely to indicate that their professional values were well aligned with their service line leaders (χ2= 8.56 (1, N = 573), p = 0.003; see Figure 1E) and with system leadership (χ2=2.10 (1, N = 573), p = 0.04; see Figure 1F) compared to physicians.
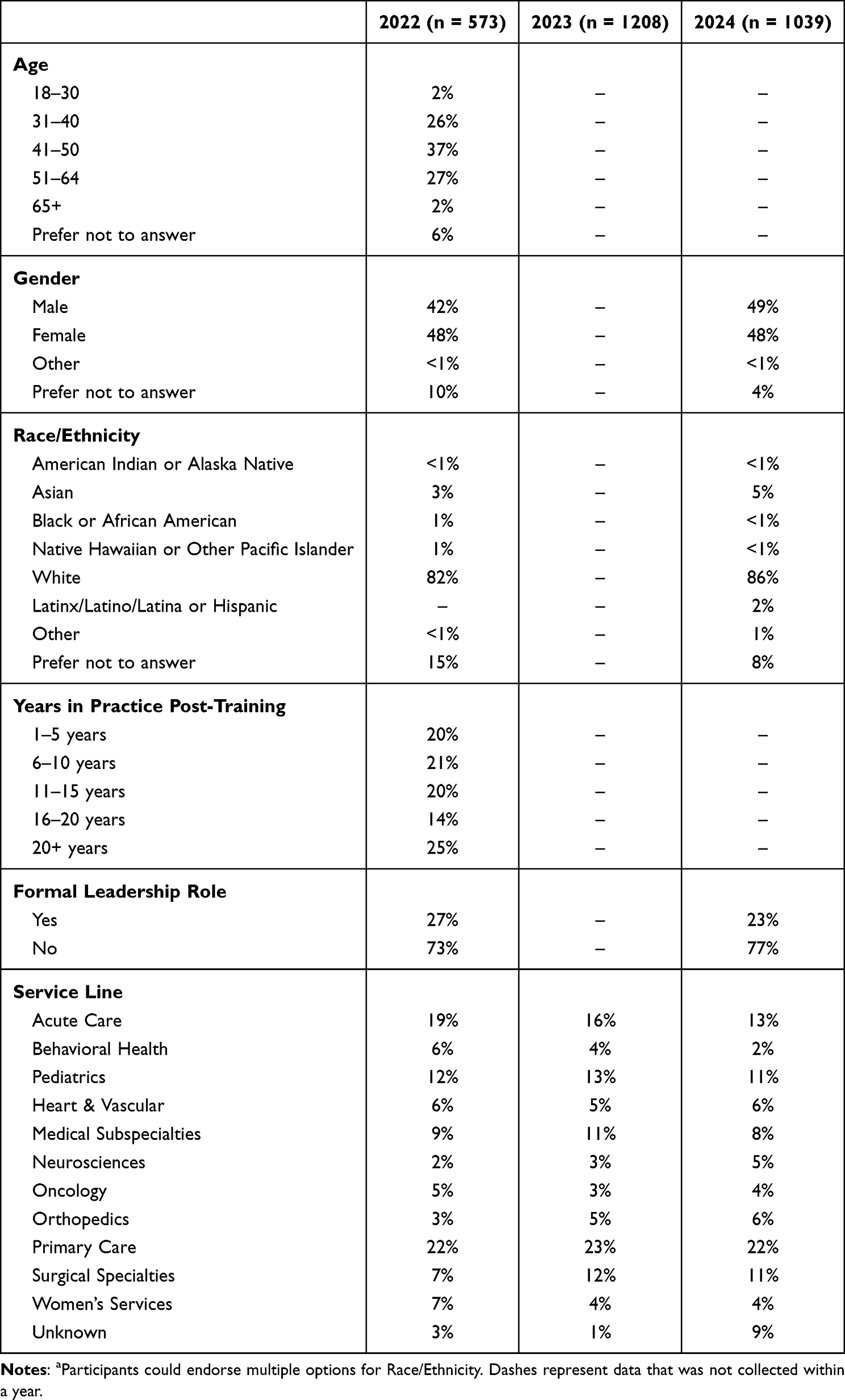 |
Table 1 Sample Demographicsa |
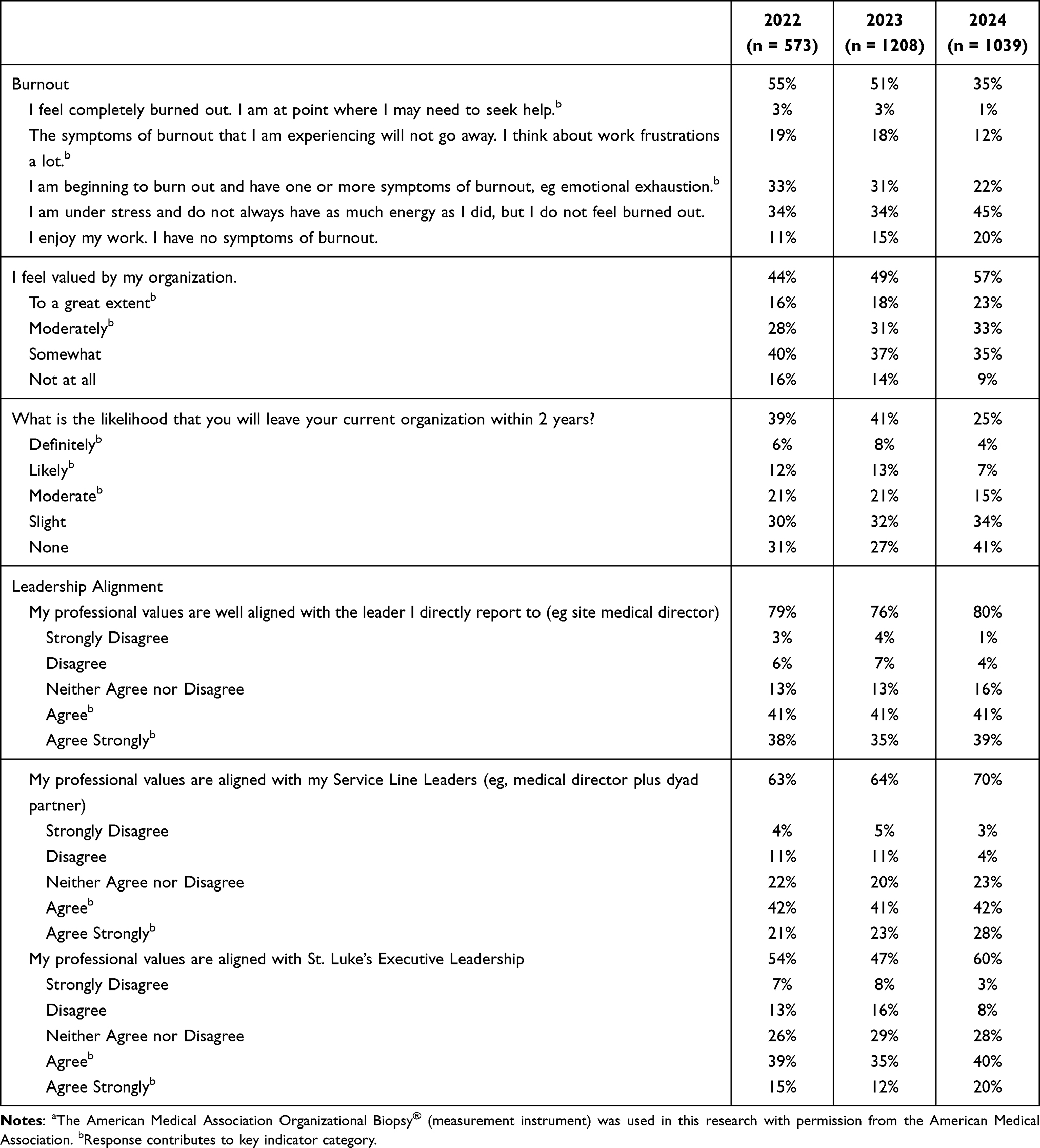 |
Table 2 AMA Organizational Biopsy and Burnout and Well-Being Survey Responsesa |
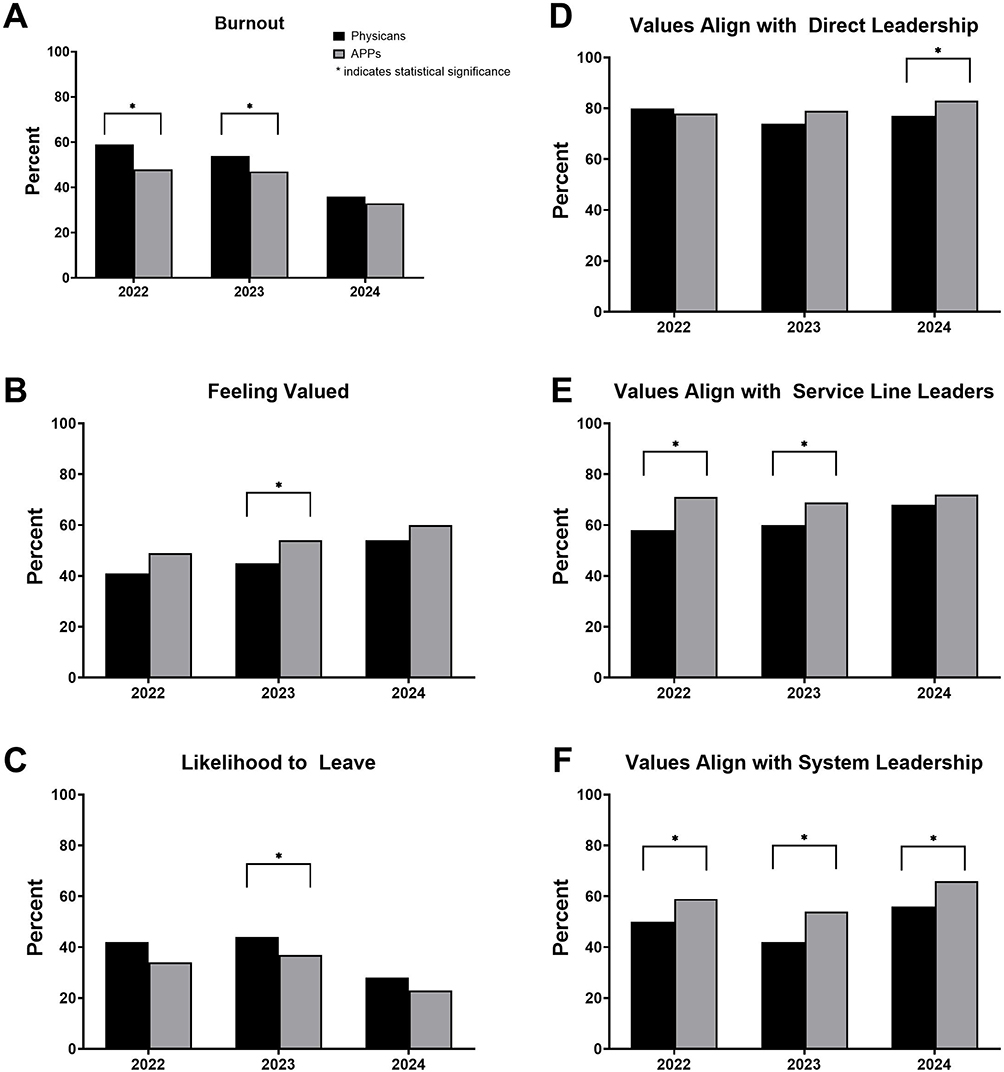 |
Figure 1 2022–2024 Physician and APP Comparison on Well-being and Burnout Key Performance Indicators and Leadership Value Alignment. (A) Physician and APP Burnout Comparisons. (B) Physician and APP Feeling Valued Comparisons. (C) Physician and APP Likelihood to Leave Organization Comparisons. (D) Physician and APP Professional Values Alignment with Direct Leadership Comparisons. (E) Physician and APP Professional Values Alignment with Service Line Leaders Comparisons. (F) Physician and APP Professional Values Alignment with System Leadership Comparisons. Asterisks represent statistically significant differences. |
Based on the survey results, a correlational analysis was conducted as part of the AMA Organizational Biopsy to examine relationships between a key driver of burnout, professional value alignment with leadership, and key performance indicators, including overall job satisfaction, job stress, burnout, intent to leave, and feeling valued. A series of Pearson’s correlations revealed moderate to strong positive correlations across key performance indicators, as well as between performance indicators and leadership value alignment as shown in Table 3. Overall, individuals who reported higher symptoms of burnout were also more likely to have lower job satisfaction scores (rp= 0.65, p < 0.0001), higher job stress (rp= 0.71, p < 0.0001), more likely to leave the organization (rp= 0.47, p < 0.0001), and lower feeling valued scores (rp= 0.43, p < 0.0001). These relationships are anticipated as key indicators of physician and APP well-being. Key performance indicators were also positively correlated with leadership value alignment at most levels of leadership (see Table 3). Overall, individuals who reported that their professional values were well aligned with their direct leader had lower burnout (rp= 0.32, p < 0.0001), lower intent to leave (rp= 0.36, p < 0.0001), higher feeling valued scores (rp = 0.42, p < 0.0001), and higher job satisfaction scores (rp=0.50, p < 0.0001). Similarly, alignment with Service Line leaders was associated with lower burnout (rp= 0.40, p < 0.0001), lower intent to leave (rp= 0.42, p < 0.0001), higher feeling valued scores (rp= 0.57, p < 0.0001), and higher job satisfaction scores (rp= 0.57, p < 0.0001). Lastly, alignment with St. Luke’s Executive Leadership correlated with lower burnout (rp= 0.45, p < 0.0001), lower intent to leave (rp= 0.47, p < 0.0001), higher feeling valued scores (rp= 0.65, p < 0.0001), and higher job satisfaction scores (rp= 0.60, p < 0.0001). These relationships suggested that leadership alignment may play an important role within the system for addressing well-being among physicians and APPs.
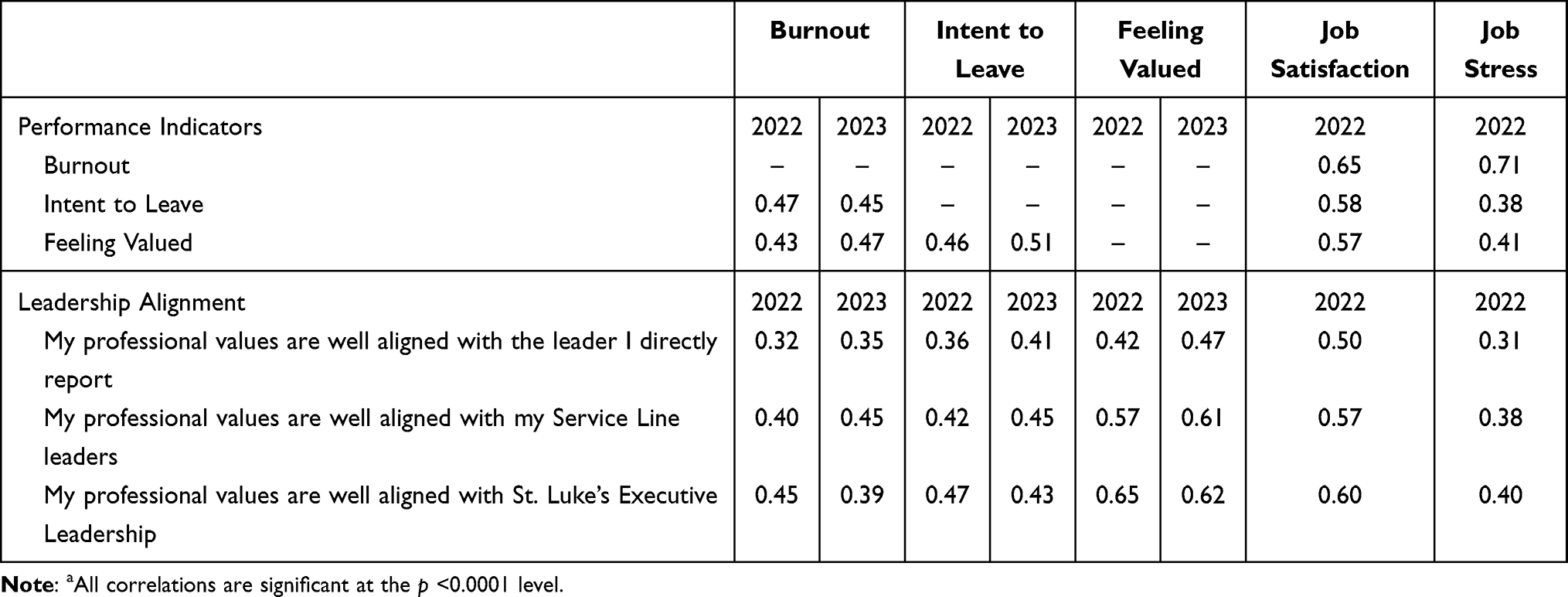 |
Table 3 Correlational Analysis of Performance Indicators and Leadership Value Alignmenta |
Wellness-Centered Leadership Implementation
Given this initial correlational analysis, as well as existing research on the importance of a culture of well-being and leadership impact on burnout reduction, the Physician and APP Well-being CoE led and partnered with key stakeholders in the development and implementation of multiple evidence-based interventions in support of wellness-centered leadership, which included a) physician and APP leader training, b) non-physician and APP leader training, c) physician and APP leader wellness-centered leadership toolkit. A detailed overview of physician and APP leader training and non-physician and APP leader training are provided below (see Table 4 for details on the interventions).
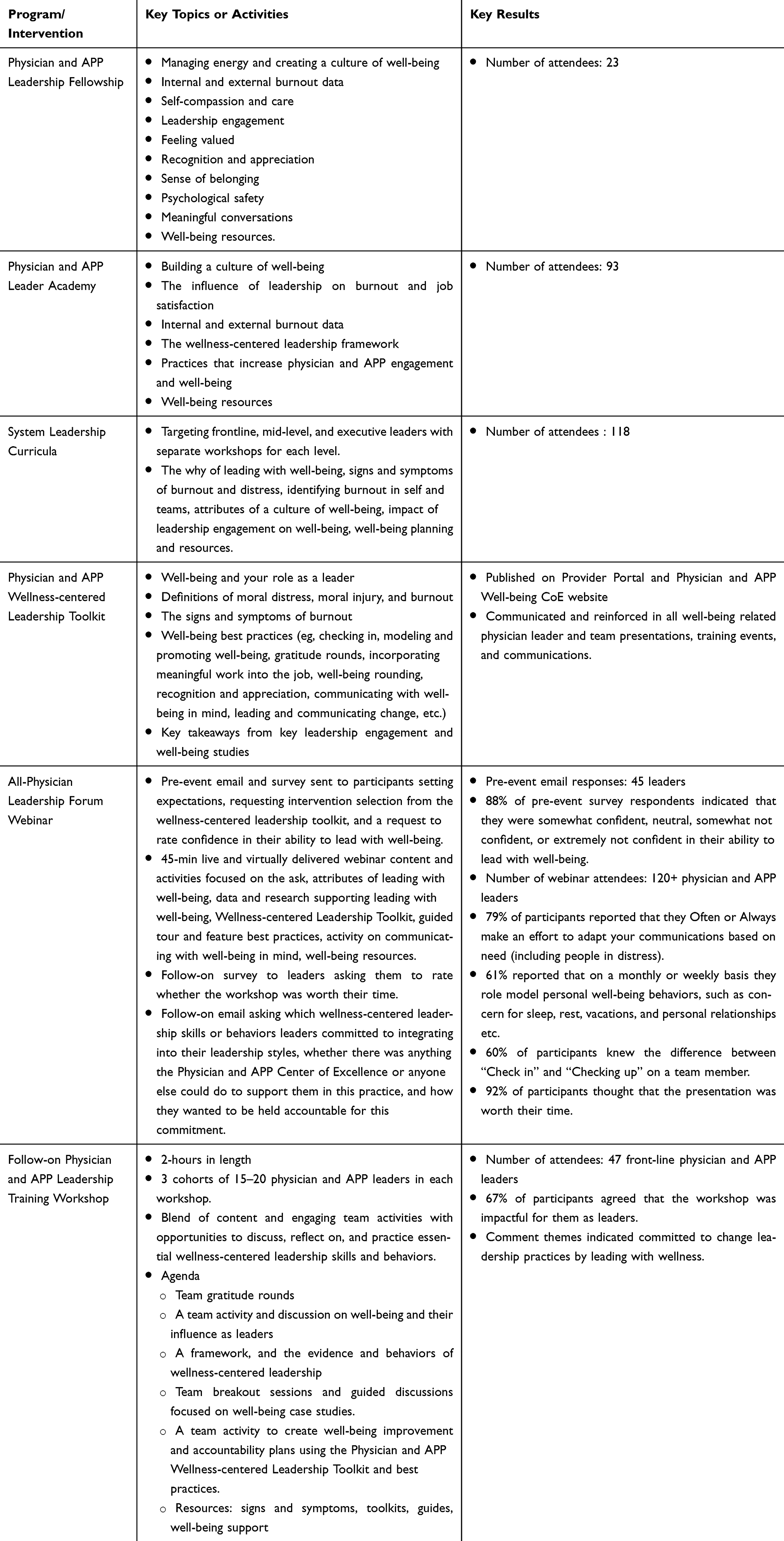 |
Table 4 Wellness-Centered Leadership Development Interventions |
Physician and APP and Non-Physician and APP Leader Training
In collaboration with an external vendor (Healthcare Leadership Institute), and as part of a broad leadership development program, a wellness-centered leadership development curriculum was designed and implemented for both service line dyad leaders (medical and administrative leaders) and frontline physician and APP leaders. Service line dyad leaders participated in a 12-month fellowship development program, which consisted of 12 4-hour in-person workshops and leadership coaching, of which one 4-hour session was focused on leading with well-being. Frontline physician and APP leaders participated in a 6-month leadership academy that included a series of 6 2-hour virtual workshops, of which one session focused on leading with well-being. The content of the workshops focused on the importance of creating a culture of well-being and the leader’s role in creating this culture, internal and external burnout data, recognition of burnout in self and teams, evidence supporting wellness-centered leadership and engagement as a driver of well-being and feeling valued, and well-being best practices and resources. The curriculum utilized a blended learning approach, including lecture, team discussions, and learning activities. A combined total of 116 physician and APP leaders attended either the fellowship or academy programs representing 58% of all physician and APP leaders within the health system in 2022.
Physician and APP Wellness-Centered Leadership Toolkit
To reinforce the skills and knowledge taught in the wellness-centered leadership programs, the Physician and APP Well-being CoE developed a Wellness-Centered Leadership Toolkit, which was published on internal provider portals and internal websites. In addition, the availability of the toolkit was communicated and reinforced in all well-being physician leader and team presentations, training events, and communications. The toolkit included sections focused on well-being and the role as a leader, well-being best practices, and highlights extracted from key leadership engagement and well-being studies. Well-being practices outlined in the toolkit included checking in, modeling and promoting well-being, gratitude rounds, incorporating meaningful work into the job, well-being rounding, recognition and appreciation, communicating with well-being in mind, and leading and communicating change.
Physician and APP Well-Being and Burnout 2023 Survey Outcomes
In continuation of the AMA Organizational Biopsy, a condensed version of the Mini Z 2.0 burnout and well-being survey was sent out to 2025 employed, contracted, or independent physicians and APPs (all physicians and APPs on med staff) in 2023 for annual data collection. The initial survey invitations were distributed via email from system leadership with several reinforcement communications as described previously for the 2022 survey. In addition, COE leadership sent personal reminders via Microsoft Teams with a final email reminder from the COE. A condensed survey was intentionally distributed to avoid survey fatigue among respondents, increase the response rate, and provide validated benchmarks to continue implementation of wellness-centered leadership interventions. Despite its condensed format, the 2023 survey maintained the ability to evaluate the impact that wellness-centered leadership programs had on key well-being metrics. The condensed survey consisted of 8 questions: burnout, feeling valued by the organization, leadership alignment by level, likelihood to leave organization within 2 years, intent to retire, service line, role, and an open-ended question for comments. A total of 1208 responses were received (60% of targeted sample) with physicians accounting for 58% of responses and APPs accounting for the remaining 42% of responses. A descriptive profile of respondent characteristics can be found in Table 1. Half of respondents (51%) reported experiencing burnout at some level with 49% of respondents reported feeling valued by the organization. Approximately 41% indicated a moderate-to-high likelihood of leaving the organization within 2 years (see Table 2). A significantly higher number of physicians endorsed feeling some level of burnout compared to APPs (χ2= 5.33 (1, N = 1208), p = 0.021; see Figure 1A). In addition, physicians were more likely to report that they did not feel valued by the organization (χ2= 3.12 (1, N = 1208), p = 0.002) and were more likely to indicate that they would leave the organization within 2 years (χ2= 2.23 (1, N = 1208), p = 0.026) as shown in Figure 2. As seen in the previous year, despite high rates of burnout symptoms, 76% of physicians and APPs indicated that their professional values were aligned with direct medical leader, 64% indicated that their professional values aligned with their service line leaders, and 47% reported that their professional values aligned with executive leadership as shown in Table 2. Similar to the 2022 survey, physicians and APPs reported similar rates of direct leader value alignment (p = 0.051), however APPs were more likely to indicate that their professional values were well aligned with their service line leaders (χ2=10.59 (1, N = 1208), p = 0.001) and with system leadership (χ2= 16.92 (1, N = 1208), p < 0.001) compared to physicians as shown in Figure 2.
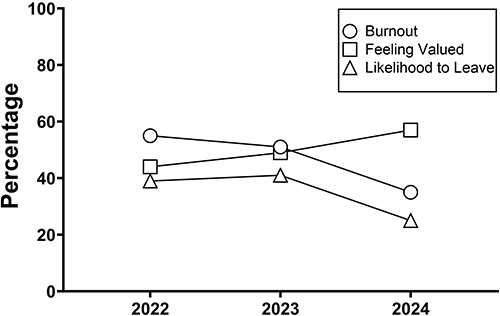 |
Figure 2 2022–2024 Physician and APP Well-being and Burnout Key Performance Indicators. |
In comparison to 2022, there was 4% decrease in burnout symptoms (p = 0.126), a 5% increase in feeling valued by the organization (p = 0.064), a 3% decrease in direct medical leadership value alignment (p = 0.199), a 0.3% increase in service line leadership value alignment (p = 0.897), a 7% decrease in executive leadership value alignment (χ2= 7.42 (1, N = 1781), p = 0.006), and lastly, a 2% increase in the likelihood of leaving the organization within 2 years (p = 0.369; see Figure 2). Although these differences between 2022 and 2023 were not statistically significant on most well-being indicators and leadership value alignment, the data suggested that wellness-centered leadership implementation had the potential to reduce burnout and promote feeling valued by the organization. The AMA Organizational Biopsy correlational analysis of the well-being and burnout 2023 survey data again revealed significant positive correlations between leadership value alignment and key performance indicators similar to those found with the 2022 survey (see Table 3), which reinforced the focus on wellness-centered leadership. Hence, a strategic focus for the CoE continued to be wellness-centered leadership training and support efforts.
Continuing Wellness-Centered Leadership
The Physician and APP Well-being CoE continued the foundational work started in 2022, including promoting the Physician and APP Wellness-centered Leadership Toolkit. To further enhance prior efforts to educate and support leaders on wellness-centered leadership, the Physician and APP Well-being Center of Excellence developed and introduced two new development programs: a) an all-physician leadership forum webinar, and b) a follow-on and internally developed physician and APP wellness-centered leadership training workshop.
A 45-minute interactive webinar that focused on wellness-centered leadership was developed and facilitated for system-wide physician leadership. Prior to the event, leaders received several communications to enhance interest and bolster participation, including an email foreshadowing the event, an inter-office candy-gram invite, and an email that set expectations for the webinar and asked them to select one new well-being practice from the Physician and APP Wellness-Centered Leadership Toolkit to bring into their leadership style moving forward. Invited leaders were also asked to complete an anonymous survey sharing successes or opportunities for improvement in terms of leading with well-being, as well as their confidence in their leading with well-being skills. A total of 45 leaders completed the pre-survey with only 12% of survey respondents indicating that they felt extremely confident in their leading with well-being skills, highlighting the need to elevate wellness-centered leadership skills. Roughly 115 leaders participated in the webinar, which included both lecture and interactive learning activities. The webinar concluded with leaders committing to one wellness-centered leadership skill to implement and a follow-up email asking them how they wanted to be held accountable was sent out individually.
The follow-on physician and APP leadership training workshop was a highly interactive workshop for frontline physician and APP leaders offered to 3 cohorts of 15–20 leaders per workshop. The CoE Medical Director and CoE manager led the 2-hour workshop, which provided content on the framework of wellness-centered leadership and provided opportunities to practice wellness-centered leadership skills and behaviors through practical activities, such as creating well-being improvement and accountability plans, and well-being case studies. Additional resources were provided to attendees, including toolkits and guides. A total of 47 frontline physician and APP leaders attended the training workshop.
Physician and APP Burnout and Well-Being 2024 Survey Outcomes
In 2024, the full-length AMA Organizational Biopsy and Mini Z 2.0 surveys were again implemented and sent out to 2171 physicians and APPs who were employed, contracted, or independent medical staff. The survey was initially distributed by COE leadership via individual Teams messages with additional text messages sent to independent groups and clinics. Weekly reinforcement communication was delivered via leadership reporting, weekly communications, and integration into existing service line communications. A total of 48% of the targeted sample (n = 1039) responded to the survey with 53% of responses from physicians and 47% of responses from APPs. A descriptive profile of respondent characteristics can be found in Table 1. Approximately 35% of physicians and APPs respondents endorsed experiencing symptoms of burnout, with 25% indicating that they were likely to leave the organization within 2 years. In addition, 57% of respondents indicated that they felt valued by the organization (see Table 2). Physicians and APPs did not significantly differ on burnout (p = 0.334), likelihood to leave the organization (p = 0.089), or feeling valued by the organization (p = 0.077) as shown in Figure 2. Respondents endorsed high alignment of professional values with their direct medical leader (80%), service line leaders (70%), and executive leadership (60%). Notably, a higher proportion of APPs were aligned with their direct medical leader (χ2= 4.85 (1, N = 1039), p = 0.028; see Figure 1D) and executive leadership (χ2= 11.21 (1, N = 1039), p < 0.001; see Figure 1E) than physicians. There was not a significant difference for service line leadership and value alignment for 2024 between physicians and APPs (p = 0.104; see Figure 1F).
In comparison to 2023, burnout significantly decreased from 51% to 35% (χ2= 58.51 (1, N = 2248), p < 0.001), and intent to leave the organization significantly decreased from 41% to 25% (χ2= 60.52 (1, N = 2247), p < 0.001), as well as an 8% significant increase, from 49% to 57% (χ2= 13.70 (1, N = 2247), p < 0.001), in the number of respondents who reported feeling valued by the organization (see Figure 2). Leadership value alignment increased across the board, 4% for direct leadership (χ2= 3.90 (1, N = 2247), p = 0.048), 6% for service line leadership (χ2= 10.52 (1, N = 2247), p = 0.001), and 13% for executive leadership (χ2= 40.42 (1, N = 2247), p < 0.001).
Discussion
The current project found that the implementation of wellness-centered leadership led to significant reductions in burnout and intent to leave the organization, as well as increases in feeling valued and leadership value alignment. Specifically, there was a 16% reduction in burnout, a 16% reduction in intent to leave the organization, an 8% increase in feeling valued by the organization. In addition, professional value alignment increased by 4% for direct leadership, 6% for service line leadership, and 13% of executive leadership. Notably, APPs endorsed significantly lower rates of burnout, higher rates of feeling valued, lower likelihood to leave the organization, and higher professional value alignment across multiple levels of leadership. This is consistent with previous studies that found lower rates of burnout among APPs.5–8 Overall, the significant reduction in burnout and other performance indicators suggests that wellness-centered leadership can be an effective tool for improving physician and APP well-being and for increasing value alignment with multiple levels of leadership across the health system. Despite differences in performance indicators, these findings are encouraging that the framework implemented supports both physicians and APPs without the need for different programmatic interventions. Additionally, the positive shifts in performance indicators, particularly the reduction in burnout, and value alignment due to organizational-level changes support that environmental factors are a significant contributor over individual factors.
The initiative undertaken by our health system and CoE provides support for the importance of investing in physician and APP well-being at a system level. The initial investments for such an initiative included compensation support for a medical director and CoE manager and external vendor partnership fees for the leadership training. Internal efforts conducted in collaboration with the vendor did not have costs associated other than staffing. Our estimates for the cost-savings are conservatively based on reduction on intent to leave and actual reduction in attrition, which is estimated at $5 million in savings as a result of reduced attrition among physicians and APPs. Enhanced retention can be achieved by demonstrating a commitment to well-being, reducing turnover costs, and enhancing team stability. Beyond the cost savings from reduced attrition, additional cost savings may be realized through decreased absenteeism and increased productivity. The success of this wellness-centered leadership implementation can serve as a model for other organizations. The partnership with AMA to conduct the Organizational Biopsy, which AMA offers free of cost as part of their mission work, provides a cost-effective means of better understanding unique factors impacting physician and APP well-being within specific organizations, allowing for tailored interventions that can then be implemented by the organization.
Lessons Learned
This systematic change in well-being suggests that improvement or worsening does not occur in a vacuum. While wellness-centered leadership is a significant factor in its ability to shift a culture of well-being and, as outlined in the data above, there are several other factors that contribute to well-being. Institutionally, other areas of focus over 2022–2024 that also likely had an impact on institutional well-being included removing intrusive language from credentialing forms, developing access to free anonymous counseling to all employed physicians and APPs, and piloting an AI scribe opportunity. With the current project, we are unable to control for these additional factors but hope to capture these through continued surveys in subsequent years. In addition, participation rates greatly increased from 2022 to 2023 and 2024. It is suspected that individual reach outs contributed to this marked increase in survey participation rates. As mentioned earlier, well-being is multi-faceted and wellness-centered leadership is a critical component, but it is not the only component. Another observation around wellness-centered leadership was that leaders often seemed to overstate their ability to lead with well-being, and they likely had more opportunity to learn and gain skills than they originally believed. Holding leaders accountable for leading with well-being continues to be an opportunity to further solidify this journey. A key take away is that wellness-centered leadership needs to be promoted routinely to allow leaders to maintain skills, add new skills to their repertoire, and keep well-being front of mind. It is also critical to recognize that each individual has their own journey with well-being and improvements found in the survey may not resonate with them. Wellness-centered leadership interventions implemented in the current initiative did not factor in individual needs and preferences for learning style, such as mode, content, or frequency of training. Future work should examine how tailored approaches to leader training will help in developing personalized training that addresses unique needs and may result in more effective training approaches. Notably, the work presented reflects performance improvement/quality improvement efforts and therefore was not designed as a formal research study. Reproducibility based solely on the methodology described here is neither feasible nor appropriate. Similarly, we did not evaluate which elements of wellness-centered leadership implemented had the most impact. Future work should include evaluation of intervention impact to better inform implementation.
Conclusion
Physician and APP well-being have significant implications on individual quality of life, patient outcomes, and healthcare costs. To address physician and APP well-being and burnout, St. Luke’s Health System and its Physician and APP Well-being CoE systematically utilized annual burnout and well-being survey data to implement wellness-centered leadership as a strategic priority for reducing physician and APP burnout. A multi-faceted approach and a set of system-wide and evidence-based interventions focused on leadership training and development, and tools and resources yielded significant improvements in burnout, feeling valued by the organization, leadership alignment, and likelihood to leave the organization. These efforts and results validate that systematic and consistent efforts to empower leaders with the skills, tools, and resources required to engage their teams through the lens of well-being is a critical driver of building a culture of well-being.
Acknowledgments
The authors would like to thank Dr. James Souza, Dr. Robert Cavagnol, and Raquel Hartman for their participation, engagement, and support of this work, as well as the St. Luke’s Health System Executive Leadership, Human Resources, and Leadership Development Team.
Disclosure
The author(s) report no conflicts of interest in this work. No funding was received for this work. The St. Luke’s Health System IRB deemed this work to be non-human subjects research, as defined by 45 CFR 4621 and was therefore exempt for ethical review and determined that informed consent was not required. The participants of this project did not give written consent for their data to be shared and due to the sensitive nature of the project, supporting data is not available.
References
1. Shanafelt TD, West CP, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clin Proc. 2022;97(12):2248–2258. doi:10.1016/j.mayocp.2022.09.002
2. Linzer M, Jin JO, Shah P, et al. Trends in clinician burnout with associated mitigating and aggravating factors during the COVID-19 pandemic. JAMA Health Forum. 2022;3(11):e224163. doi:10.1001/jamahealthforum.2022.4163
3. Berg S. Physician burnout rate drops below 50% for first time in 4 years. American Medical Association Web site. Available from: https://www.ama-assn.org/practice-management/physician-health/physician-burnout-rate-drops-below-50-first-time-4-years.
4. McKenna J. Medscape Physician Burnout & Depression Report 2024: ‘We Have Much Work to Do’. Medscape Web site. Available from: https://www.medscape.com/slideshow/2024-lifestyle-burnout-6016865?reg=1#2.
5. Essary AC, Bernard KS, Coplan B, et al. Burnout and job and career satisfaction in the physician assistant profession: a review of the literature. NAM Perspect. 2018. doi:10.31478/201812b
6. Benson MA, Peterson T, Salazar L, et al. Burnout in rural physician assistants: an initial study. J Physician Assistant Educ. 2016;27(2):81–83. doi:10.1097/JPA.0000000000000069
7. Varner DF, Foutch BK. Depression and burnout symptoms among air force family medicine providers. JAAPA. 2014;27(5):42–46. doi:10.1097/01.JAA.0000446373.63790.c9
8. Abraham CM, Zheng K, Norful AA, Ghaffari A, Liu J, Poghosyan L. Primary care practice environment and burnout among nurse practitioners. J Nurse Pract. 2021;17(2):157–162. doi:10.1016/j.nurpra.2020.11.009
9. Zimmermann C, Strohmaier S, Herkner H, Niederkrotenthaler T, Schernhammer E. Suicide rates among physicians compared with the general population in studies from 20 countries: gender stratified systematic review and meta-analysis. BMJ. 2024;386:e078964. doi:10.1136/bmj-2023-078964
10. Gold KJ, Schwenk TL, Sen A. Physician suicide in the United States: updated estimates from the national violent death reporting system. Psychol Health Med. 2021;27(7):1563–1575. doi:10.1080/13548506.2021.1903053
11. Shanafelt TD, Dyrbye LN, West CP, et al. Suicidal ideation and attitudes regarding help seeking in us physicians relative to the US working population. Mayo Clin Proc. 2021;96(8):2067–2080. doi:10.1016/j.mayocp.2021.01.033
12. Williams ES, Manwell LB, Konrad TR, Linzer M. The relationship of organizational culture, stress, satisfaction, and burnout with physician-reported error and suboptimal patient care: results from the MEMO study. Health Care Manag Rev. 2007;32(3):203–212. doi:10.1097/01.HMR.0000281626.28363.59
13. Firth-Cozens J, Greenhalgh J. Doctors’ perceptions of the links between stress and lowered clinical care. Soc Sci Med. 1997;44(7):1017–1022. doi:10.1016/S0277-9536(96)00227-4
14. Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Ann Internal Med. 2002;136(5):358–367. doi:10.7326/0003-4819-136-5-200203050-00008
15. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Internal Med. 2018;283(6):516–529. doi:10.1111/joim.12752
16. Li CJ, Shah YB, Harness ED, Goldberg ZN, Nash DB. Physician burnout and medical errors: exploring the relationship, cost, and solutions. Am J Med Qual. 2023;38(4):196–202. doi:10.1097/JMQ.0000000000000131
17. Han S, Shanafelt TD, Sinsky CA, et al. Estimating the attributable cost of physician burnout in the United States. Ann Internal Med. 2019;170(11):784–790. doi:10.7326/m18-1422
18. Burnout KD. Professionalism, and the quality of US health care. JAMA Health Forum. 2023;4(3):e230024. doi:10.1001/jamahealthforum.2023.0024
19. National Academy oM. National Academies of Sciences, Engineering, and Medicine. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being. The National Academies Press; 2019.
20. West CP, Dyrbye LN, Sinsky C, et al. Resilience and burnout among physicians and the general US working population. JAMA Network Open. 2020;3(7):e209385. doi:10.1001/jamanetworkopen.2020.9385
21. Berg S. To address burnout’s underlying causes, look to team-based care. AMA Web site. Available from: https://www.ama-assn.org/practice-management/physician-health/address-burnout-s-underlying-causes-look-team-based-care.
22. Shanafelt T. Organizational efforts to cultivate healthcare professional well-being: before and after the COVID-19 pandemic.
23. Shanafelt TD, Gorringe MD, G MS, et al.; EdD. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015;90(4):432–440. doi:10.1016/j.mayocp.2015.01.012.
24. Shanafelt T, Trockel M, Rodriguez A, Logan D. Wellness-centered leadership: equipping health care leaders to cultivate physician well-being and professional fulfillment. Acad Med. 2021;96(5):641–651. doi:10.1097/ACM.0000000000003907
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.