Back to Journals » Clinical Optometry » Volume 14
Wearer Experience and Eye Care Professional Acceptance with a 1 Day Multifocal Contact Lens
Authors McParland M ![]() , Walsh K
, Walsh K ![]() , Comoroda D, Sulley A
, Comoroda D, Sulley A
Received 18 May 2022
Accepted for publication 18 October 2022
Published 22 November 2022 Volume 2022:14 Pages 223—235
DOI https://doi.org/10.2147/OPTO.S375133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Marcella McParland,1 Karen Walsh,1 Daniel Comoroda,2 Anna Sulley3
1Coopervision, Inc. Professional Affairs, San Ramon, CA, USA; 2Lumanity (Formerly Cello Health Insight), Insight Department, Bethesda, MD, USA; 3Coopervision, Inc. Medical Affairs, San Ramon, CA, USA
Correspondence: Marcella McParland, Coopervision, Inc, Delta Park, Concorde Way, Segensworth North, Fareham, PO15 5RL, UK, Tel +44 7976 770575, Email [email protected]
Purpose: A large observational survey was undertaken to determine eye care professional (ECP) and patient experience of stenfilcon A multifocal soft contact lens (MyDay multifocal) when prescribed in a real-world setting.
Methods: A total of 196 ECPs from eleven countries fit up to ten presbyopes with stenfilcon A multifocal. Data were collected on fit success at the initial visit, patient satisfaction with comfort, vision at distance, intermediate, and near, overall vision, overall satisfaction, and handling at the initial and follow-up visits after 1– 2 weeks of wear. ECPs completed questionnaires on multifocal fitting experience and expectations before and after the fitting period.
Results: A total of 196 pre-fitting and 141 post-fitting ECP surveys were collected. A total of 1505 initial fits (mean age 53.4, range 38 to 81 years, 73% female, 27% neophytes) and 1440 follow-up visits were completed. The mean distance vision contact lens prescription was − 1.32DS (range − 12.00DS to +8.00DS) with Add powers: Low 56%, Medium 24%, and High 21%. At the follow-up visit 77% (n=1108) of trials were successful. Mean patient satisfaction ratings (1– 10 scale, where 1 is not at all satisfied, and 10 extremely satisfied) at the initial visit were higher than eight out of ten for comfort, vision, and overall satisfaction, and were not significantly different after 1– 2 weeks of wear. Stenfilcon A multifocal was preferred by 66% of patients over their habitual correction. In most cases mean satisfaction scores and the proportion of patients highly satisfied were not significantly different between myopes and hyperopes, across Add range, between new and habitual wearers, and wearers of frequently replaced and 1 day contact lenses.
Conclusion: ECPs in real-world clinical settings found stenfilcon A multifocal contact lenses easy to fit to a wide range of patients, with a high fit success rate and high levels of patient satisfaction for overall comfort, vision, satisfaction, and handling.
Keywords: presbyope, multifocal, vision, satisfaction, stenfilcon A
Introduction
The number of people affected by presbyopia is estimated to reach 2.1 billion by 2030.1 The typical “modern-day” presbyope is often a young-at-heart, active, device-using individual whose experience of presbyopia may extend beyond the physical inconvenience of needing help with close focusing.2,3 Impacts on quality of life, self-esteem, and work,4,5 along with the emotional burden of not being able to see clearly for reading or device use have all been reported.4 These insights help to illustrate the deeper feelings surrounding presbyopic vision changes, and eye care professionals (ECPs) are acutely aware of the importance of best meeting the visual needs of presbyopes. There are several options available to correct, or alleviate the symptoms of, presbyopia including both single vision spectacles and progressive addition lenses (PALs), contact lenses (CLs), and, in some markets, pharmacological agents. For many patients the convenience afforded by gaze-independent CL correction in comparison to progressive addition lenses (PALs) in spectacles is important, and, in those who have tried both options, soft multifocal designs are preferred over correction with monovision.3,6
Use of soft multifocal CLs has been reported to be relatively low, being prescribed for just 37% of presbyopes over a five-year period as per the international contact lens prescribing survey (2005–2009),7 although their use has increased in recent years,8,9 and they represented 49% of lenses prescribed to presbyopes in a 2021 survey of ECP fitting behavior.10 This still leaves around half of CL-wearing presbyopes being fit with something other than a soft multifocal design. Reasons reported for the relative lack of prescribing this type of lens design relate to both fitting and retention: lack of knowledge to fit multifocal CLs successfully, low success rates, and increased chair time have been reported as barriers;11 drop-out from lens wear is higher in this patient group, most commonly due to lens discomfort and dryness, and poor vision.12,13
To increase ECP prescribing of soft multifocal lenses, a CL needs to be easy and quick to fit, with a high success rate that can instill confidence in both the ECP and the patient. A novel multifocal contact lens system was launched in 2021 using the silicone hydrogel 1 day disposable material, stenfilcon A (MyDay multifocal with the Binocular Progressive System, CooperVision, Inc., San Ramon, California, USA). The multifocal contact lens system is designed to help presbyopes achieve their vision needs using a unique 3-add system, while delivering ease of fit and high levels of fitting success for ECPs. Initial validation and randomized controlled clinical trials reported high fit success rate and patient satisfaction.14–17 To examine the performance of the same lens in a real-world setting a large observational survey was conducted with ECPs in eleven countries, capturing both ECP and wearer outcomes. This allowed for a significantly increased sample size compared to a controlled clinical trial, including feedback from fitting during routine clinical practice, use of the full power range available for the lens (compared to a slightly restricted range used in controlled clinical studies), and the fitting of a wider range of patients including both habitual multifocal soft contact lens wearers and neophytes.
Materials and Methods
The survey was coordinated by Lumanity, an independent insight and analytics agency, and conducted from July to November 2021 in the USA, Canada, UK, France, Italy, Belgium, the Netherlands, Luxembourg, Spain, Portugal, and Singapore. ECP and patient questionnaires were developed by CooperVision and Lumanity. ECPs were contacted and asked if they would like to participate and then provided with a link to a registration survey hosted on Lumanity’s survey platform. Interested ECPs completed the registration form including consent forms and the details and expectations of participation. ECPs completed an initial survey sent by Lumanity about their current habits in fitting patients requiring multifocal CLs. After being supplied with fitting sets, ECPs were trained either face-to-face or virtually by local professional affairs team members from CooperVision on the multifocal contact lens system and fitting approach and were instructed to follow the fitting guide which can be found at https://coopervision.co.uk/sites/coopervision.co.uk/files/myday-mf-fitting-guide-v3.pdf with a summary in Table 1. Some ECPs may have chosen to fit some patients outside the recommended fitting criteria as sometimes happens in normal practice – ECPs selected patients in the normal course of their practice. If a patient came in who was already wearing multifocal lenses, or was a new patient to contact lenses, the ECP may opt to suggest the new 1 Day Multifocal for them to try.
 |
Table 1 Fit Guide for Initial Lens Selection for Stenfilcon A Multifocal |
Initial lens selection was recommended to be based on an up-to-date back vertex corrected spectacle prescription, with a maximum of 0.75DC of refractive astigmatism. Eye dominance was determined using the +1.00D blur method as recommended by the lens fitting guide. Following assessment with the initial trial lenses, enhancements were offered if required, using ±0.25D steps to the dominant eye to enhance distance vision, and ±0.25D steps to the non-dominant eye for near vision. ECPs fitted up to 10 of their presbyopic patients with the stenfilcon A multifocal during the normal course of their clinical practice, recording data from the fit in an online patient record form. Patients returned for a follow-up visit 1–2 weeks later, and lens enhancements were offered if required, with data from the visit also being recorded in an online form. ECP participants completed a final online 10-min survey at the end, in which they evaluated their experience fitting the stenfilcon A multifocal over the course of the in-market assessment. Survey questions included 5-point scales for expectation (1, did not meet my expectations, to 5, exceeded expectations) and agreement (1, disagree, to 5, agree); and 0–10 scores for subjective responses from wearers (0 poor to 10 excellent). Participants were paid an honorarium for participating, where it was acceptable in their country, based on fair market value of ECP time to complete other market research of a similar length. Any personalized information was destroyed as per national laws and as indicated in the consent form; anonymized data were retained.
Ethics committee or institutional review board approval was not required as this was a market research survey. The ECPs who participated agreed not to intervene or change the patient’s normal standard of care, to protect patient’s confidentiality, and to report any significant adverse events encountered during the course of the survey. All participants were asked to read an Informed Consent Form at the beginning of the online survey and provided their consent by providing a signature and date in an online registration survey. A pdf copy of the informed consent was provided to all participants after registration. Participants were apprised of their rights as per the appropriate national laws, including but not limited to the European Data Protection Law or Data Protection Act of 2018 (UK), and advised that any adverse events in the course of the research would be reported to the relevant authorities. Lumanity is bound by the principles of Intellus Worldwide, BHBIA (British Healthcare Business Intelligence Association), EphMRA (European Pharmaceutical Market Research Association), ESOMAR (European Society for Opinion and Marketing Research), and the Market Research Society’s Code of Professional Conduct which govern the collection, retention, use, disclosure, and transfer of information about subjects of, and participants in, market and social research.
The collected data were processed and analyzed by Lumanity at a 95% confidence interval (P<0.05), including descriptive statistics used for associative analysis in certain populations of interest (eg neophytes). P values from all proportions were derived from the resulting Z score of a two-tailed hypothesis Z test, whereas all means were derived from the resulting T score of a two-tailed hypothesis T test.
Results
A total of 196 ECPs completed pre-fitting surveys, 1505 initial fits of stenfilcon A multifocal were conducted, and 1440 follow-up visits and 141 final ECP surveys completed (Table 2).
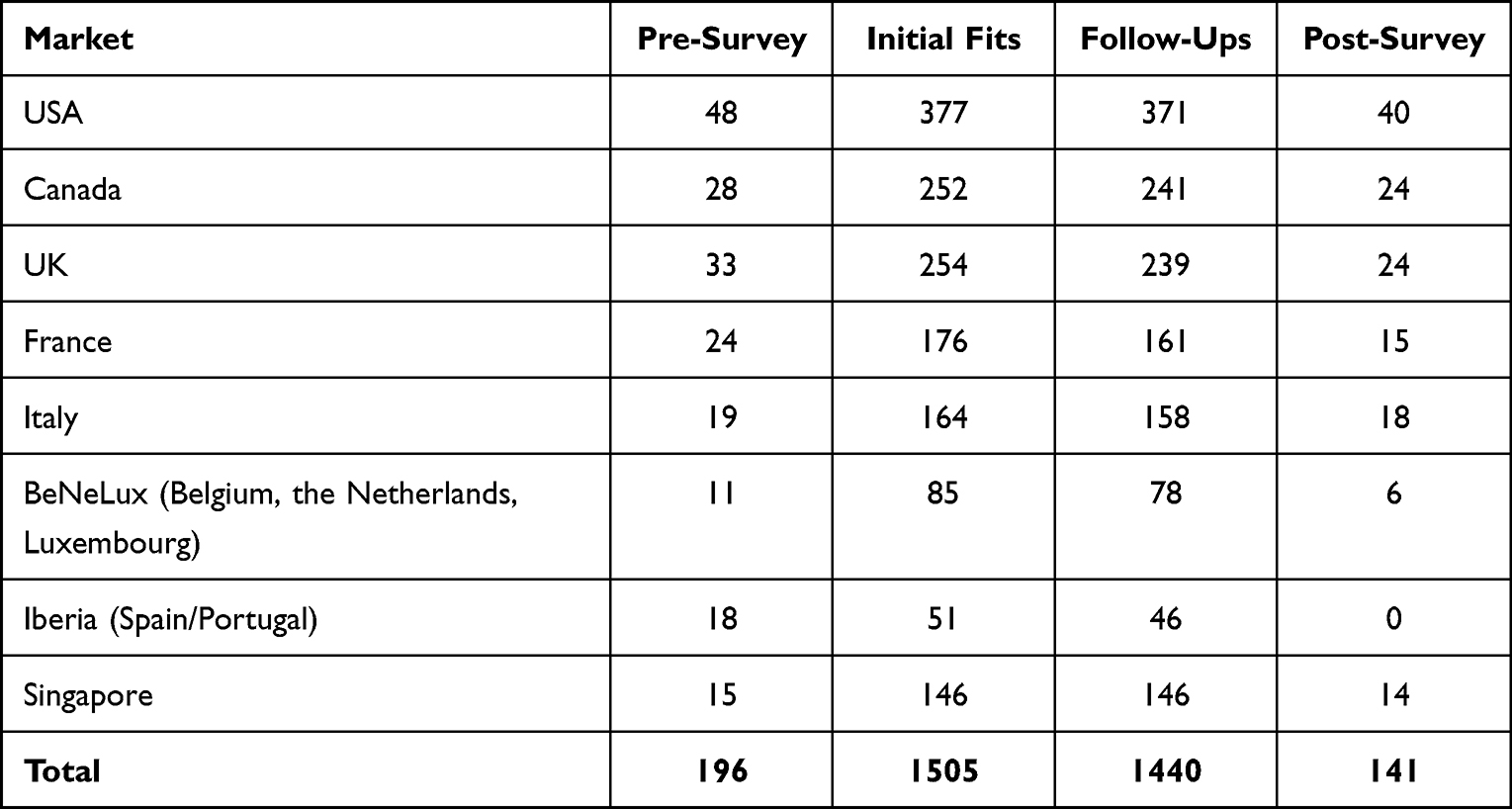 |
Table 2 Number of Surveys, Initial Fits, and Follow-Up Visits by Region |
Pre-Fitting Survey
Just over half (53%) of ECPs worked in independent practice, with the remainder split between alliance/buying group/retail affiliation (8%), small optical chain (≤20 stores, 13%), large optical chain (>20 stores, 5%), ophthalmology practice 16%, and “other” 6%. The mean number of CL patients fit per month was 74, of which 46% were spherical fits, 28% toric, and 26% multifocal. The most common CL-related options offered to presbyopes were soft multifocals, 1 day disposable (97% of respondents), and frequent replacement (91%), followed by monovision 77%, distance CLs with reading spectacles over 75%, and multifocal rigid CLs 62%. The importance of a number of criteria related to multifocal fitting were given on a five-point scale (1, unimportant, to 5, important), with the “overall vision performance”, “comfort”, and “high fit success rate” ranking as important to most ECPs. With a “top two box” approach (adding scores 4 and 5 from the five point scale), ECPs agreed that overall vision performance, comfort, and high fit success were important to ECPs, and the top two box score was 99%, 99%, and 97%, respectively (Figure 1). ECP experience of the same criteria captured in the post-fitting survey is also displayed in Figure 1 and discussed in the section on the post-fit survey.
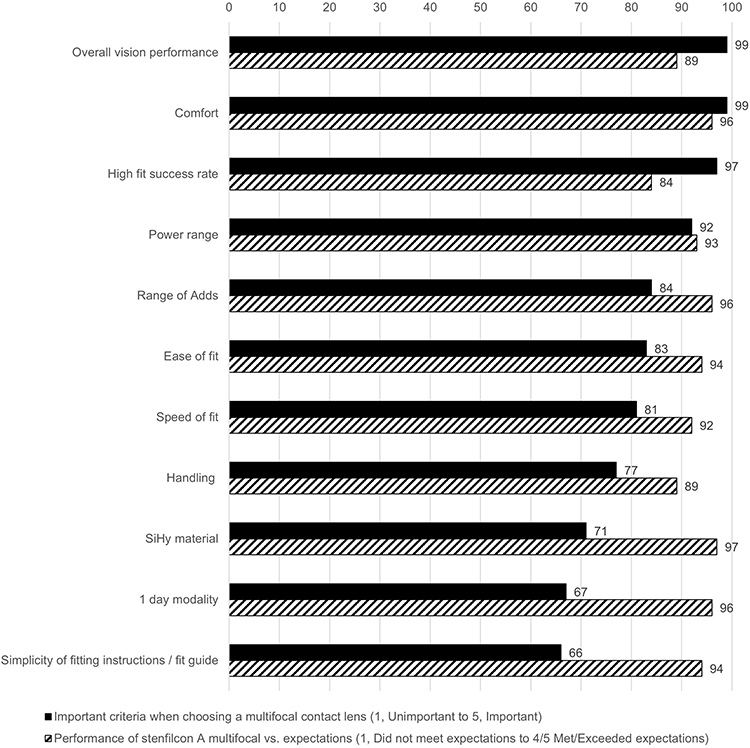 |
Figure 1 Top two box agreement (%) to importance of soft lens multifocal criteria in pre-fitting survey (n=196) vs performance of stenfilcon A multifocal to same criteria in post-fitting survey (n=141). |
Overall Initial Fit and Follow-Up
Patient demographics are shown in Table 3.
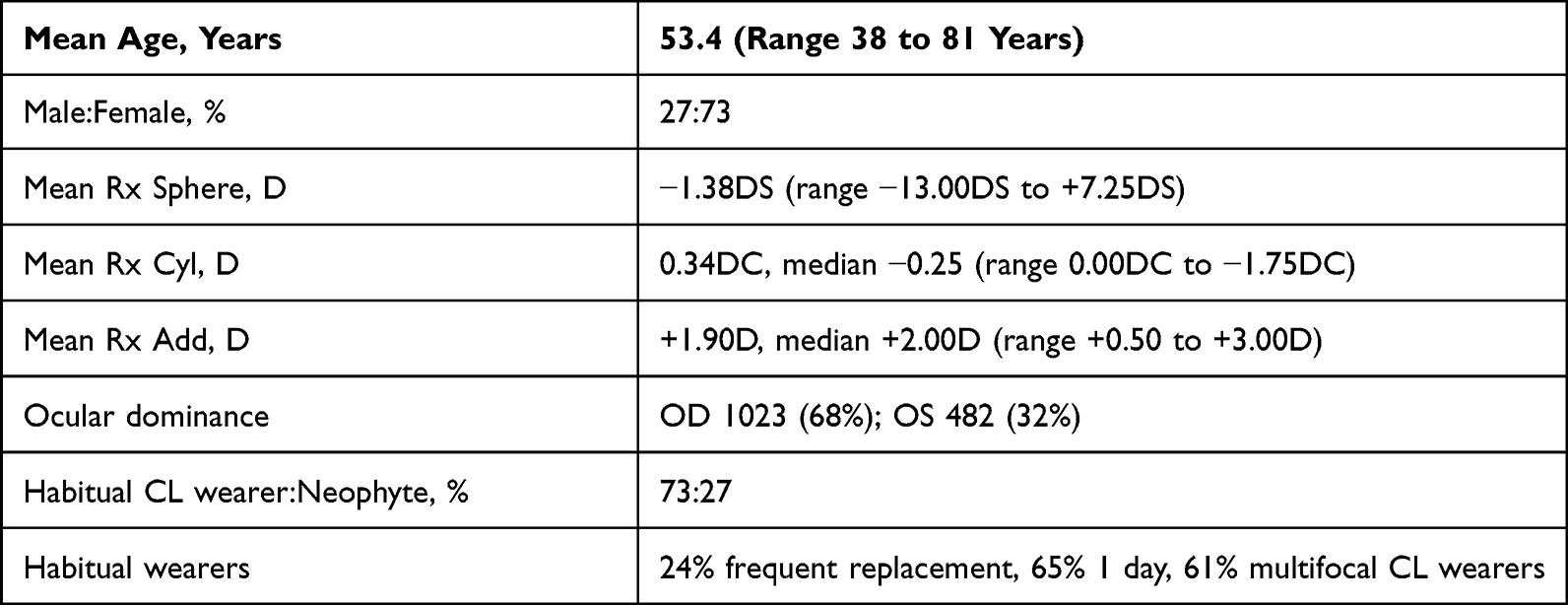 |
Table 3 Wearer Demographics at Fitting, n=1505 |
An acceptable fit at the initial visit was achieved with stenfilcon A multifocal 95% of the time, and the fit guide was used for 78% of fits. The mean distance vision CL prescription was −1.32DS (range −12.00DS to +8.00DS) with Add powers distributed as follows: OD Low 76%, Medium 18%, High 15%; OS Low 44%, Medium 30%, High 27%. Three-quarters (75%) of initial lenses were dispensed as the final lens, with 16% requiring an enhancement to the CL prescription. At the follow-up visit 77% (n=1108) of trials were successful. Of those that were not (n=332), the most common reasons given were related to near vision (22%), distance vision (21%), and overall vision (20%).
Mean patient satisfaction (0–10 scale) at the initial and follow-up visits are shown in Figure 2. At the initial visit all mean scores were higher than eight out of ten. After 1–2 weeks of wear, similar scores were reported with mean score not more than 0.1 different from the patient’s initial impression in any of the six criteria, which covered satisfaction with vision performance at different distances and overall comfort, vision, and satisfaction with the lenses. The mean score for lens handling at the follow-up visit (0–10 scale) was 8.8. The proportions of patients reporting satisfaction of 7–10 on a 0–10 scale are shown in Table 4 for both the initial and follow-up visit.
 |
Table 4 Stenfilcon A Multifocal Wearers Reporting Satisfaction Scores of 7–10 on a 0–10 Scale at the Initial Fitting (n=1505) and Follow-Up Visit (n=1440), % |
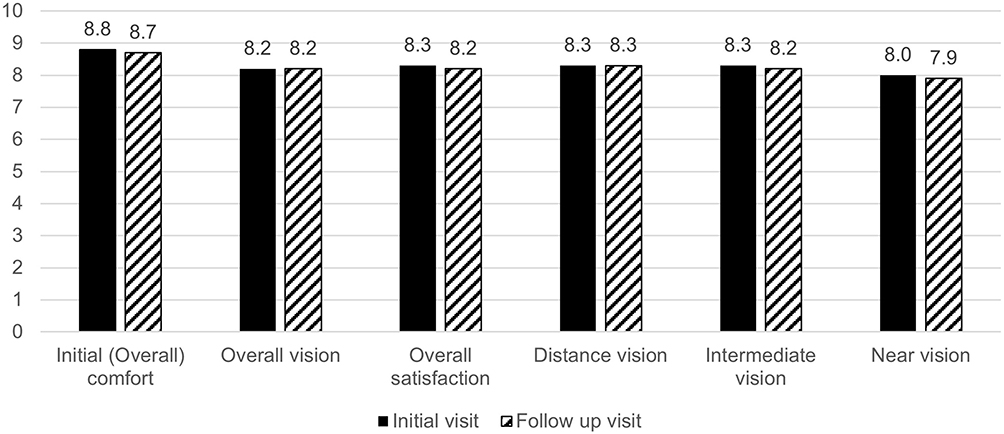 |
Figure 2 Wearer satisfaction scores (mean, 1–10 scale) at initial (n=1505) and follow-up visit (n=1440). |
Two-thirds (66%) of patients expressed a preference for stenfilcon A multifocal over their habitual correction, and more than two-thirds (67%) agreed they would recommend the lens.
Comparison Between Patient Groups
Habitual CL Wearers
Habitual vs Neophyte CL Wearers
At the follow-up visit, a significantly greater proportion of habitual CL wearers were successfully fit with stenfilcon A multifocal compared to neophytes (79% vs 71%, P=0.0015). Mean satisfaction scores at the follow-up visit were significantly higher for habitual compared to neophyte wearers for overall comfort (8.8, SD = 1.4, vs 8.5, SD = 1.5; P<0.001), overall vision (8.3, SD = 1.3 vs 7.9, SD = 1.5; P<0.001), overall satisfaction (8.3, SD = 1.5 vs 7.8, SD = 1.7; P<0.001), and handling (8.8, SD = vs 8.5, SD =; P<0.001). Similar proportions of habitual lens wearers and neophytes were highly satisfied (7–10 score on a 1–10 scale) at the follow-up visit with overall comfort (93% vs 93%) and handling (93% vs 91%); with significantly more habitual wearers being highly satisfied with overall vision (92% vs 83%, P<0.0001) and with significantly more overall satisfaction (89% vs 79%, P<0.0001) at follow-up compared to neophyte wearers.
Habitual CL Wearer Baseline Compared to Post-Fit Experience with Stenfilcon A Multifocal
The follow-up visit was completed by 1062 habitual CL wearers. Overall comfort, vision, and overall satisfaction (1–10 scale) were scored for the habitual lenses at the initial visit, and for stenfilcon A multifocal at the follow-up visit. Significantly higher scores were found for stenfilcon A multifocal compared to the habitual correction, and significantly more patients rated high satisfaction (7–10 on a 1–10 scale) for all three criteria (Table 5).
 |
Table 5 Patient Mean Satisfaction Scores (1–10) and Proportion Satisfied (7–10 Score, 1–10 Scale) with Habitual Lenses (Initial Visit) vs Stenfilcon A Multifocal (Follow-Up Visit), n=1062 |
Habitual Multifocal vs Single Vision CL Wearers
Fits to existing CL wearers were categorized into refits from a single vision CL (n=281) and those refit from a soft multifocal CL design (n=673). Trial success (81% vs 75%, P=0.04) was significantly higher in existing multifocal wearers compared to single vision CL wearers. At initial fitting, there was no difference in mean scores for comfort (8.9 for both), overall vision (8.3 for both), and overall satisfaction (8.4 for both), with significantly more habitual multifocal wearers highly satisfied (7–10 score on 1–10 scale) with overall vision (95% vs 90%, P=0.005) and with significantly more overall satisfaction (95% vs 88%, P<0.001). By the follow-up visit, however, there was no significant difference in the proportion of patients scoring high levels of overall satisfaction between the groups (90% vs 87%) or the mean satisfaction score (8.3, SD = 1.4 vs 8.2, SD = 1.6).
Habitual 1 Day vs Frequently Replaced
For all but one instance, no significant difference was found in scores for comfort, vision, and overall satisfaction, or in the proportion scoring between 7–10 for these performance attributes at either the initial fit or follow-up visit between habitual 1 day or frequently replaced soft lens wearers. The one exception was a significantly higher overall comfort score reported by habitual frequently replaced soft lens wearers at the follow-up visit compared to habitual 1 day wearers (8.9 vs 8.7, P=0.04), with no difference between groups for the proportion highly satisfied (7–10 on a 1–10 scale; 95% vs 91%).
Comparison Between Add Powers
At the follow-up visit the distribution of the spectacle Add groups was: Low (Add +0.75D to +1.25D) n=335, Medium (Add +1.50 to +1.75D) n=552, and High (Add ≥+2.00D) n=553. Trial success rate at the follow-up visit was significantly higher with the Low Add compared to the High Add (80% vs 74%, P=0.06), but not significantly different to the Medium Add (78%). Where the initial trial lens was not successful at follow-up, significantly more wearers using a Low Add cited distance vision as the reason than did Medium and High Add users (38% vs 21% and 13%, P<0.001 for both). There was no significant difference in patient preference compared to habitual correction between the Low, Medium, and High Adds (70%, 67%, and 64%, respectively); significantly more Low Add wearers would recommend the lens compared to High Add wearers (72% vs 65%, P=0.05). There was no significant difference between spectacle add groups in the percentage of wearers rating between 7–10 for overall comfort (95% Low, 92% Med, 92% High), vision (92% Low, 90% Med, 88% High), and satisfaction (90% Low, 86% Med, 84% High) at the follow-up visit. Mean scores (1–10) at follow-up were significantly higher with the Low Add compared to the Medium and High Adds for overall comfort (8.9, SD = 1.2 vs 8.6, SD = 1.5 and 8.7, SD = 1.5; P=0.002; P=0.04), overall vision (8.5, SD = 1.3 vs 8.2, SD = 1.4 and 8.1, SD = 1.4; P<0.001; P<0.001), and overall satisfaction (8.4, SD = 1.5 vs 8.1, SD = 1.6 and 8.1, SD = 1.6; P<0.001; P=0.002).
Comparison Between Type of Ametropia
For analysis, the spherical element of the distance prescription was categorized into being myopic (−0.50D or greater, n=845), emmetropic (−0.25D to +0.50D, n=154), or hyperopic (+0.75D or greater, n=506). The proportion of wearers expressing high levels of satisfaction (7–10 on a 1–10 scale) at the initial fitting for initial comfort and overall vision were not significantly different between myopes and hyperopes (97% myopes vs 97% hyperopes for comfort; 93% myopes vs 92% hyperopes for vision), but both were significantly higher than emmetropes (90% comfort, P<0.001 vs myopes and P=0.001 vs hyperopes; 87% vision, P=0.01 vs myopes and P=0.05 vs hyperopes). In emmetropes, 71% of initial fits were successful, compared to 73% of hyperopes and 81% of myopes fit. Distance vision was given as the reason for unsuccessful fitting more often with emmetropes (32% of those unsuccessful) compared to myopes (18%) and hyperopes (20%). At the follow-up visit, a significantly greater number of both myopes and hyperopes were satisfied (7–10 on a 0–10 scale) with their overall vision (92% myopes; 89% hyperopes) compared to emmetropes (81%, P<0.001 vs myopes and P=0.01 vs hyperopes), but there was no significant difference between myopes and hyperopes. Mean overall vision scores were significantly higher for myopes (8.3, SD = 1.3) compared to both hyperopes (8.1, SD = 1.3, P=0.004) and emmetropes (7.8, SD = 1.6, P<0.001). When myopes were further subdivided into low (−0.50D to −5.00D, n=644) and high (−5.25D and higher, n=201) prescriptions, no difference was found in trial success (both 81%), mean overall comfort, vision, and satisfaction scores (8.9, SD = 1.3; 8.3, SD = 1.3; 8.3, SD = 1.5; respectively, for low myopes vs 8.7, SD = 1.6; 8.3, SD = 1.4; 8.2, SD = 1.7; for high myopes, 1–10 scale) or the proportion highly satisfied for the same three attributes (95%, 92%, 89% for low myopes vs 91%, 92%, 88% for high myopes).
Comparison of low (up to −0.75DC, n=1290) and high (−1.00 to −1.75DC, n=150) astigmats revealed no significant difference in overall comfort (8.7, SD = 1.4 vs 8.6, SD = 1.5), vision (8.2, SD = 1.4 vs 8.1, SD = 1.5), and satisfaction (8.2, SD = 1.6 vs 8.0, SD = 1.6) scores at the follow-up visit, but a significantly greater number of low astigmats were satisfied (7–10 score, 1–10 scale) with their distance vision (90% vs 84%, P=0.05).
ECP Post-Fitting Survey
Satisfaction with currently available soft multifocal lenses was established in both the pre-fit and post-fit survey (Figure 3). Before the start of the observational survey, 71% of ECPs were either satisfied or extremely satisfied with the soft multifocal options available; this increased to 84% of ECPs who completed the post-fitting survey. The number of ECPs extremely satisfied with available multifocal options significantly increased between the pre- and post-fitting surveys with the availability of stenfilcon A multifocal (6% vs 24%, P<0.001).
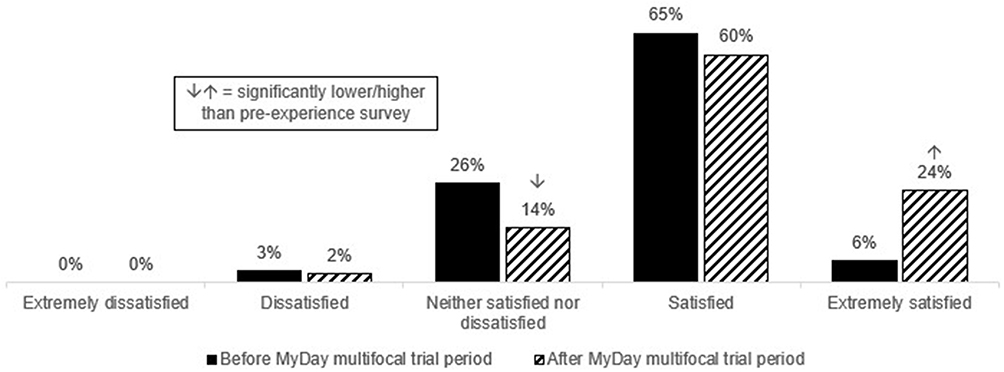 |
Figure 3 ECP satisfaction with available multifocal options pre- (n=196) and post- (n=141) use of stenfilcon A multifocal. |
After experience with stenfilcon A multifocal, a high proportion of ECPs responded that it met or exceeded expectations for all criteria relating to lens performance, with a range from 84% agreement for high fit success rate to 97% agreement for silicone hydrogel material (Figure 1). In 8 out of 11 performance criteria, ECPs rated the lenses based on their experience higher than their original thoughts as to what was important when choosing a multifocal lens.
ECP response to statements about stenfilcon A multifocal showed top two box agreement (1–5 scale) ranging from 75% (stenfilcon A multifocal CLs have exceeded my expectations on their overall performance) to 98% (stenfilcon A multifocal will help my stenfilcon A wearers continue to wear contact lenses as they become presbyopic) (Table 6). More than 90% of ECPs agreed they would recommend the lens (92%), that it was fast and easy to fit (94%), and that the fit guide was easy to use (95%). In relation to suitability with different patient groups, ECPs agreed stenfilcon A multifocal was a better option than monovision (94%), a better option than stenfilcon A single vision with reading glasses (96%), an excellent option for neophytes with presbyopia (96%), and that it would help keep existing 1 day lens wearers in CLs as they become presbyopic (97%).
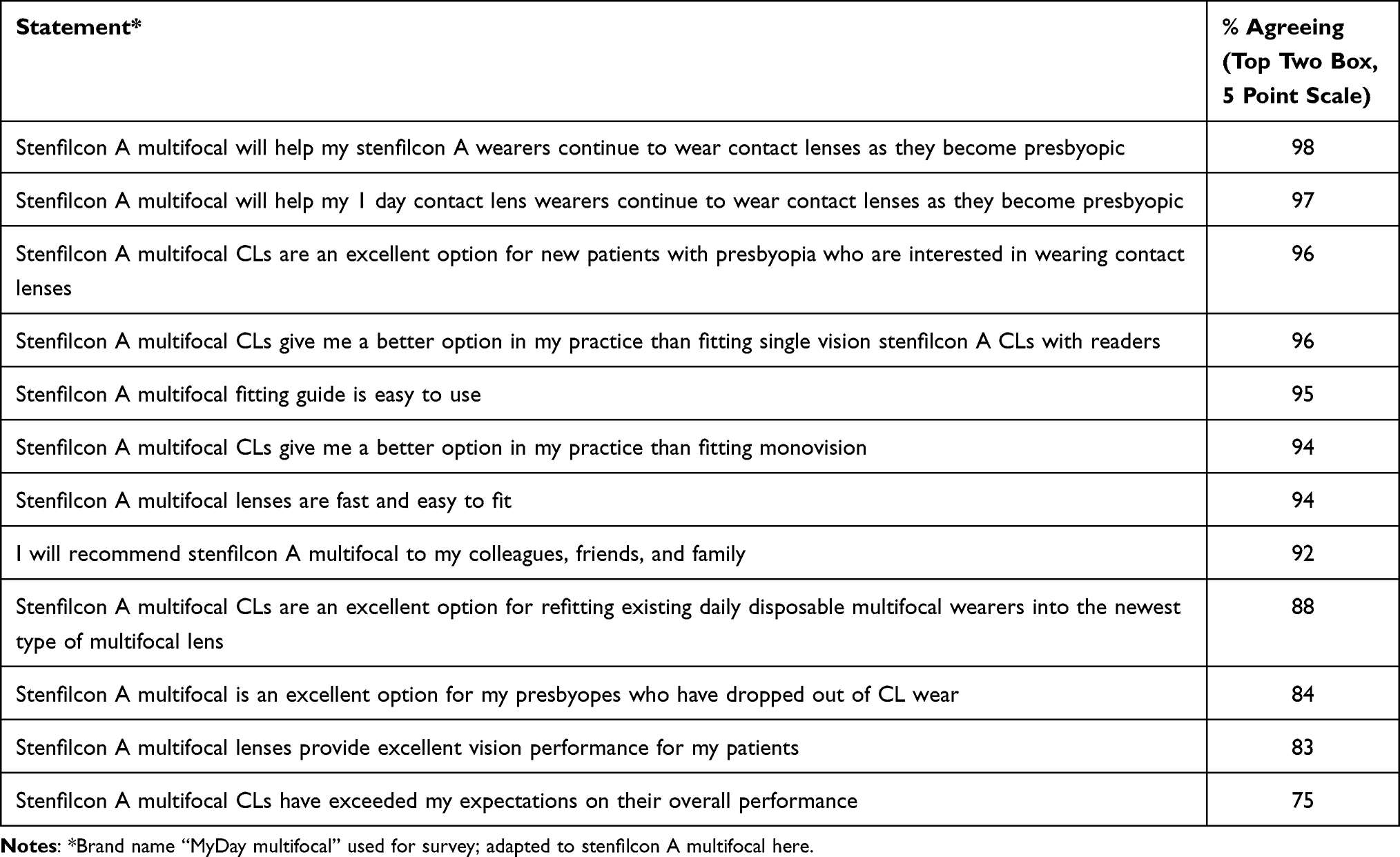 |
Table 6 Perceptions of Stenfilcon A, Post-Fit Survey, % Top Two Box Agreement, n=141 |
Discussion
Successful soft multifocal fitting is an increasingly important part of clinical CL practice with a growing number of presbyopes worldwide. Additionally, there is an increasing choice of multifocal lens designs, materials, and prescription ranges which enable more patients to be offered the option. This large observational in-market survey collected ECP and patient feedback of multifocal fitting pre- and post-experience with fitting stenfilcon A multifocal. The factors which contribute to historically lower numbers of multifocal fitting7 are well understood and were echoed in the importance ECPs placed on certain lens criteria in the pre-fitting survey: overall vision performance, comfort, and high success rate. Following experience with fitting stenfilcon A multifocal, 89% of ECPs in this survey agreed the lens met or exceeded their expectations for overall vision performance, and 96% agreed it met or exceeded expectations for comfort. Furthermore, 84% of ECPs agreed the lens had a high fit success rate, with more than 90% agreeing that stenfilcon A multifocal delivered ease of fit, speed of fit, and that the fit guide was simple and easy to use. The fit guide was used in the majority, but not every single fit. When ECPs were trained in fitting this lens they were strongly recommended to use the fitting guide every time. It is possible ECPs found the guide so simple to use and easy to remember that they did not need to consult it in every case; it is also possible that some ECPs prefer not to consult a fit guide, choosing their own route when selecting trial lenses.
Reports of low confidence in lens fit success and vision performance, along with increased chair time, have been cited as reasons for hesitation among some ECPs to proactively and routinely recommend multifocal soft CLs.11 The outcomes of this observational survey in relation to these attributes should help provide confidence that stenfilcon A multifocal performs well, meeting or exceeding ECP expectations. The very high proportion of ECPs agreeing to the perception statements at the end of the survey illustrates that these performance criteria were met or exceeded for stenfilcon A multifocal, with more than 90% agreeing that the fit guide was easy to use, the lenses fast and easy to fit, and that they would be a good option for both existing 1 day single vision wearers as they become presbyopic and presbyopes who do not currently wear CLs.
The large data set enabled division of the patient cohort into additional defined groups. This allowed comparison of patient satisfaction and fit success between groups. Fit success and mean satisfaction scores were unsurprisingly significantly higher for habitual CL wearers compared to neophytes, although the results for neophytes were still high for overall satisfaction, vision, and comfort at the follow-up visit. Ease of handling is a key factor in the success of new wearers,12 and handling was rated highly by neophytes at the follow-up visit, with no difference between new and habitual wearers for the proportion that were highly satisfied with the experience. Given the time needed to adapt to becoming a confident CL wearer along with the time required to adapt to multifocal vision, it would be expected that habitual wearers of either single vision or multifocal CLs have fewer changes to get used to in the 1–2 week trial period compared to neophytes. It is helpful to understand how the neophyte experience differs, and, when fit with stenfilcon A multifocal, just how close their satisfaction scores are to fully adapted wearers. The process of adapting to multifocal vision was evident when comparing habitual single vision and multifocal wearers. Existing multifocal wearers had higher levels of satisfaction at the initial fit compared to single vision CL wearers, but by the follow-up visit there was no difference in overall satisfaction between the two groups. This experience agrees with advice highlighted in the BCLA CLEAR Evidence-Based Contact Lens Fitting review that suggests that patients should be given time to adapt to the vision in multifocals.18 It was also interesting to note that similar levels of satisfaction were recorded in habitual wearers of either 1 day or frequently replaced (2-week or 1-month replacement) CLs, suggesting refits would be successful from both groups. The only significant difference present in this cohort comparison was a significantly higher overall mean comfort score from the habitual frequently replaced lens group at the follow-up visit. This suggests that wearers of frequently replaced CLs may also experience an improvement in comfort by transferring to a daily disposable replacement frequency, a result that is in agreement with previous controlled clinical study.19
It would be logical to hypothesize that fit success and patient satisfaction may be impacted by the patient’s refraction. As presbyopia advances and the prescribed reading addition increases, presbyopes rely more on their reading correction. For those patients requiring a Low or Medium spectacle Add, there was no significant difference in fit success rate. Fit success rate for patients with a High spectacle Add was significantly lower than Low Add fit success, although, as a standalone value of 74%, it demonstrates that three out of four advanced presbyopes can still be successfully fit with stenfilcon A multifocal. Interestingly, once again, with time to adapt, there was no significant difference between any of the spectacle Add groups for the proportion of wearers giving high scores for overall comfort, vision, and satisfaction at the follow-up visit.
No significant differences were found for mean overall scores for comfort, vision, and satisfaction between myopes or hyperopes at either the initial fit or follow-up visit. Fit success and overall comfort, vision, and satisfaction scores were not impacted by the level of myopia. There were two groups related to refraction where differences were apparent. While ECPs were recommended to fit patients with no more than 0.75DC of astigmatism in this observational survey, 10% of fits were to astigmats with cylinder powers ranging between −1.00 and −1.75DC. Although this group experienced similar overall comfort, vision, and satisfaction to the majority of fits to wearers with a maximum of −0.75DC of astigmatism, a significantly lower percentage of the higher astigmats were highly satisfied with their distance vision. Given the vision benefits of fully correcting astigmats from 0.75DC with toric lenses,20,21 this result was not surprising and reinforces the use of spherical multifocal designs for low levels of astigmatism, with toric multifocal designs recommended for higher levels of astigmatism to help maximize the visual experience.
The other refractive group where differences were apparent was with emmetropic presbyopes. By definition, this group likely required no distance correction, but did need a reading addition for close and possibly intermediate distances. While results were good for emmetropes, with 71% of fits being successful, a greater proportion of fits to hyperopes (73%) and myopes (81%) were successful. The most common reason for unsuccessful fitting in emmetropes was related to distance vision and was reported 1.6 times more often than with hyperopes or myopes. Overall vision satisfaction was highly rated at the follow-up visit by 81% of emmetropes, and, while this was a high proportion of the group, it was still significantly lower than either hyperopes (89%) or myopes (92%). These data provide useful information for ECPs when fitting emmetropic presbyopes. It is helpful to bear in mind that while overall adaptation, success rates, and satisfaction remain high in this group, it is expected that patient feedback may be a little lower than myopes and hyperopes. This logical outcome can help frame conversations with emmetropic presbyopes when recommending multifocal CLs and help ECPs better anticipate what success may be possible in this group of patients.
Drop-out from multifocal lens wear is known to be driven by poor comfort and suboptimal vision.12,13,22 The overall wearer experience in this survey showed high levels of satisfaction at the initial and follow-up visit overall for comfort, vision, and satisfaction, as well as for vision at specific distances of near, intermediate, and distance. These outcomes illustrate that it is possible to achieve patient satisfaction with multifocal CLs, which is an important point to help ECPs feel more comfortable with proactive recommendation of this category of CLs. While not specifically addressed in this survey of routine practice, ECPs should also be aware that assessing vision in multifocals using “real-world” targets and tasks rather than relying on high contrast visual acuity is recommended as it has been shown to better inform the likelihood of success for each patient.2,3,23–25 Comfort and visual performance are closely related in multifocal lens wear, and poor vision can potentially impact comfort.26 Additionally, vision performance may be a better indicator of the likelihood of the wearer wanting to continue with multifocals compared to end-of-day comfort and dryness performance.17 These relationships further highlight the importance of achieving optimal vision correction for presbyopes to help contribute to their overall satisfaction with lens wear.
Stenfilcon A multifocal contact lenses have produced strong results in randomized controlled clinical studies, with outcomes that address both wearer expectations of vision performance and ECP needs for simple, successful fitting. Results from 133 subjects across two studies showed that high fit success of 97% and 100% was achieved using two pairs of lenses or fewer when using the fit guide.14 Results from the second study also established that overall vision clarity at 2 weeks met or exceeded expectations for 88% of subjects.14 Intermediate vision was significantly better with stenfilcon A multifocal than either the subject’s habitual lens or an alternate test lens in a study of 58 adapted multifocal wearers.15 Similarly high levels of vision satisfaction were achieved at all distances for all three Add powers, with overall vision satisfaction >80 for all three Adds (0–100 scale).16
This large observational survey enabled a number of different conditions to be explored that are not possible in a controlled clinical trial. Significantly more patients were involved for both fit and follow-up visits, the cohort included a wider range of prescriptions, and the full range of stenfilcon A multifocal was available (+8.00 to –12.00DS and three Add powers, compared to +4.00 to –6.00DS and three Add powers in the clinical studies). It is often unknown how transitioning a lens from the controlled space of a clinical trial to real-world practice will impact its performance and success. This is especially true of multifocal lenses where fit success can be significantly impacted by many reasons, for example not following the fit guide, not using an up-to-date refraction, and selecting non-optimal refractions to try and fit. It is therefore encouraging to see how similar fit success and patient satisfaction are between the previously reported clinical trial results and this large observational survey. Data from real-world settings should provide confidence to ECPs that the lens used in this survey performs well across a wide range of their presbyopic patients.
A survey of this kind is limited to providing subjective feedback from both ECPs and patients, with little detailed information gathered on clinical aspects such as the ocular response, lens fit, and visual acuity. These more detailed outcomes are better sought in a controlled interventional trial. A possible limitation of this survey is the recall bias of subjects. A further limitation of the survey relates to the potential bias of ECPs choosing to participate: agreement to be in the trial and initial contact from CooperVision may have predisposed the ECP to think favorably of the lens. Overall, however, gaining insight into the performance of stenfilcon A multifocal across both controlled clinical trials and observational large-scale surveys aims to deliver a useful combination of data to help inform ECPs in their CL fitting of presbyopic patients.
Conclusion
With the knowledge that the presbyopic population is increasing, it is important that ECPs have high performing soft multifocal CLs to offer those patients interested in wearing contact lenses. Key attributes for a soft multifocal lens are to deliver comfort, vision, and ease of fit. The results from more than 1500 fits and 1400 follow-up visits from both ECPs and wearers demonstrate that stenfilcon A multifocal meets these expectations across a wide range of patients, habitual wear options, refraction types, and stages of presbyopia. Ensuring that soft multifocal fitting is straightforward and successful in routine clinical practice is key to demonstrating the value of the lens design in question. ECPs can have confidence in the data from this large-scale survey and add this information to the clinical management of their presbyopes.
Acknowledgments
We would like to thank the 196 ECPs for their participation in this observational survey.
Funding
The survey was funded by CooperVision and run independently by Lumanity.
Disclosure
Marcella McParland, Karen Walsh, and Anna Sulley are all employees of CooperVision, Inc. Mr Comoroda reports that CooperVision funded the study which was executed by Lumanity. Funding was used for study design, scripting, hosting, analysis, and payment of a fair market value honorarium to participating ECPs. The authors report no other conflicts of interest in this work.
References
1. Fricke TR, Tahhan N, Resnikoff S., et al. Global Prevalence of Presbyopia and Vision Impairment from Uncorrected Presbyopia: systematic Review, Meta-analysis, and Modelling. Ophthalmology. 2018;125(10):1492–1499. doi:10.1016/j.ophtha.2018.04.013
2. Sivardeen A, Laughton D, Wolffsohn JS. Investigating the utility of clinical assessments to predict success with presbyopic contact lens correction. Cont Lens Anterior Eye. 2016;39(5):322–330. doi:10.1016/j.clae.2016.05.002
3. Woods J, Woods CA, Fonn D. Early symptomatic presbyopes--what correction modality works best? Eye Contact Lens. 2009;35(5):221–226. doi:10.1097/ICL.0b013e3181b5003b
4. Wolffsohn JS, Leteneux-Pantais C, Chiva-Razavi S, et al. Social Media Listening to Understand the Lived Experience of Presbyopia: systematic Search and Content Analysis Study. J Med Internet Res. 2020;22(9):e18306. doi:10.2196/18306
5. Goertz AD, Stewart WC, Burns WR, et al. Review of the impact of presbyopia on quality of life in the developing and developed world. Acta Ophthalmol. 2014;92(6):497–500. doi:10.1111/aos.12308
6. Richdale K, Mitchell GL, Zadnik K. Comparison of multifocal and monovision soft contact lens corrections in patients with low-astigmatic presbyopia. Optom Vis Sci. 2006;83(5):266–273. doi:10.1097/01.opx.0000216098.62165.34
7. Morgan PB, Efron N, Woods CA, et al. An international survey of contact lens prescribing for presbyopia. Clin Exp Optom. 2011;94(1):87–92. doi:10.1111/j.1444-0938.2010.00524.x
8. Efron N, Nichols JJ, Woods CA, et al. Trends in US Contact Lens Prescribing 2002 to 2014. Optom Vis Sci. 2015;92(7):758–767. doi:10.1097/OPX.0000000000000623
9. Jones D, Woods C, Jones L, et al. A sixteen year survey of Canadian contact lens prescribing. Cont Lens Anterior Eye. 2016;39(6):402–410. doi:10.1016/j.clae.2016.09.002
10. Morgan P, Woods C, Tranoudis IG, et al. International Contact Lens Prescribing in 2021. Contact Lens Spectrum. 2022;37(1):32–38.
11. Morgan PB, Efron N. Influence of practice setting on contact lens prescribing in the United Kingdom. Cont Lens Anterior Eye. 2015;38(1):70–72. doi:10.1016/j.clae.2014.07.014
12. Sulley A, Young G, Hunt C. Factors in the success of new contact lens wearers. Cont Lens Anterior Eye. 2017;40(1):15–24. doi:10.1016/j.clae.2016.10.002
13. Dumbleton K, Woods CA, Jones LW, et al. The impact of contemporary contact lenses on contact lens discontinuation. Eye Contact Lens. 2013;39(1):93–99. doi:10.1097/ICL.0b013e318271caf4
14. Sulley A, Orsborn G, Lazon P. Fitting success with a multifocal lens across two randomized controlled clinical studies. Optom Vis Sci. 2021;98:215046.
15. Luensmann D, Schulze M, Woods J, et al. Intermediate vision with multifocal contact lenses. Optom Vis Sci. 2021;98:215047.
16. Guillon M, Pepe P, Gupta R, et al. Influence of Near Addition Power on the Acceptance and Performance of Progressive Contact Lenses. Optom Vis Sci. 2021;98:215043.
17. Guthrie S, Luensmann D, Woods J, et al. Relationships between success factors in daily disposable multifocal lenses. Optom Vis Sci. 2021;98:215045.
18. Wolffsohn JS, Morgan PB, Barnett M, et al. Contact Lens Evidence-Based Academic Reports (CLEAR). Cont Lens Anterior Eye. 2021;44(2):129–131. doi:10.1016/j.clae.2021.02.011
19. Lazon de la Jara P, Papas E, Diec J, et al. Effect of lens care systems on the clinical performance of a contact lens. Optom Vis Sci. 2013;90(4):344–350. doi:10.1097/OPX.0b013e318288e10c
20. Cho P, Cheung SW, Charm J. Visual outcome of Soflens Daily Disposable and Soflens Daily Disposable for Astigmatism in subjects with low astigmatism. Clin Exp Optom. 2012;95(1):43–47. doi:10.1111/j.1444-0938.2011.00649.x
21. Kruse A, Lofstrom T. How much visual benefit does an astigmat achieve being corrected with a toric correction? Int Contact Lens Clin. 1996;23(3/4):59–65. doi:10.1016/0892-8967(96)00006-5
22. Sulley A, Young G, Hunt C, et al. Retention Rates in New Contact Lens Wearers. Eye Contact Lens. 2018;44(Suppl 1):S273–S282. doi:10.1097/ICL.0000000000000402
23. Diec J, Tilia D, Naduvilath T, et al. Predicting Short-term Performance of Multifocal Contact Lenses. Eye Contact Lens. 2017;43(6):340–345. doi:10.1097/ICL.0000000000000286
24. Papas EB, Decenzo-Verbeten T, Fonn D, et al. Utility of short-term evaluation of presbyopic contact lens performance. Eye Contact Lens. 2009;35(3):144–148. doi:10.1097/ICL.0b013e3181a20361
25. Woods J, Woods C, Fonn D. Visual Performance of a Multifocal Contact Lens versus Monovision in Established Presbyopes. Optom Vis Sci. 2015;92(2):175–182. doi:10.1097/OPX.0000000000000476
26. Guthrie S, Luensmann D, Woods J, et al. Comfort and vision correlations in daily disposable multifocal lenses.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.