Back to Archived Journals » Research and Reviews in Parkinsonism » Volume 9
Voice treatment in Parkinson’s disease: patient perspectives
Authors Gillivan-Murphy P, Miller N, Carding P
Received 2 March 2019
Accepted for publication 1 May 2019
Published 3 July 2019 Volume 2019:9 Pages 29—42
DOI https://doi.org/10.2147/JPRLS.S180183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Peter Hedera
Patricia Gillivan-Murphy,1 Nick Miller,2 Paul Carding3
1Speech and Language Therapy Department, Mater Misericordiae University Hospital, Dublin, Ireland; 2Newcastle University Institute for Ageing, Speech and Language Sciences, Newcastle University, Newcastle-upon-Tyne, UK; 3Midwifery and Allied Health Research, Faculty of Health and Life Sciences, Oxford Institute of Nursing, Oxford, UK
Abstract: Speech and voice changes are a central feature of the symptom complex of people with Parkinson’s disease (pwPD). Speaking is a social activity involving the pwPD, family, and the wider communicative context. Sensory-motor, cognitive-linguistic, and affective changes in Parkinson’s disease (PD) combine to alter communication, impacting on psycho-social quality-of-life, leading to risks of social withdrawal and increased depression and anxiety. The underlying pathophysiology of speech, voice, and communication difficulties in pwPD is multi-factorial and complex. Sensory-motor changes in the respiratory, phonatory, and articulatory subsystems, underscaling of effort, and central processing problems are further affected by broader cognitive-linguistic difficulties, and non-speech motor deficits. Many studies show that, when pwPD are asked to rate their own voice and how it functions in everyday situations, they show increased voice-related disability and negative impact relative to healthy controls. Voice treatment is integral to improving communication in pwPD. Studies show positive benefits from the perspective of pwPD and carers. Treatment approaches vary from one-to-one to group interventions, a singular focus on increasing loudness to more general voice exercises, and choral singing. The nature and underlying pathophysiology of speech, voice, and communication changes in pwPD are reviewed before exploring the effects of voice treatment programs and pwPD and carer perceptions of their effect. Larger scale, better powered, controlled trials of intervention for voice and speech that measure clinically and socially relevant outcomes are finally underway. Future research should also focus on issues of treatment compliance, practicality (for service delivery and use), and long-term follow-up outcomes. The role of carers in longer-term maintenance represents a further important area of exploration.
Keywords: voice, speech, treatment, quality-of-life, patient perspectives
Introduction
Motor and non-motor changes relating to spoken communication are commonly experienced by people with Parkinson’s disease (pwPD).1–3 Indeed, changes to voice quality and loudness frequently represent the first signs for pwPD and their family that something is amiss.4 Communication ability can be altered by (a) direct effects from motor changes to respiratory, laryngeal, and articulatory movements, and (b) cognitive (eg, language processing) and affective consequences (eg, depression or anxiety). Several other common disruptions to oro-motor functioning, including dysphagia and sialorrhea, may also exercise secondary effects on speech and voice.5 (Miller N, Walshe M, Walker R. Sialorrhea in Parkinson's Disease: Prevalence, impact and management strategies, personal communication, March 2019). Several recent articles have reviewed the nature of speech and language changes encountered by pwPD.6–8 However, one area of relative neglect concerns issues around the effects of communication changes on daily living as perceived by the pwPD themselves and their carers. Coupled with this is the issue of how best to capture these perceptions in clinical treatment planning and in the evaluation of outcomes, especially important given the renewed emphasis across recent years to focus content of intervention and measurement of outcomes on patient reported and preferred variables. This represents the focus of this invited review. It aims to provide an update for speech and language therapists/pathologists, and other professions involved in supporting pwPD and their carers on the issue of how communication changes are viewed by those directly impacted and the clinical practice consequences of these changes.
The state-of-the-art review first briefly outlines the scope of communication changes in pwPD and their relationship to more general underlying pathology before focusing centrally on the remit of patient and carer perspectives of these changes and treatment programs designed to address them. Although the title states “voice” treatment, we interpret that here to encompass all aspects of spoken communication—respiration, phonation, prosody, and articulation. For this paper we interpret patient perspectives regarding voice treatment as meaning one or all of the following: the use of patient chosen or patient reported outcome measures (PROMs); documentation of pwPD reports of the impact of communication difficulties on everyday living; pwPD views of the process of voice treatment and of speech and language therapy (SLT) intervention in general; and patients’ contributions to the design of voice treatment. Although the perspectives of pwPD are a key focus of this paper, we also considered the perspectives of a spouse/carer of a pwPD as integral.
Identification of studies for review entailed a literature search of Ovid Medline and CINAHL to identify relevant papers published between 2008 and 2018. Subject headings (MeSH) and text words relating to Parkinson’s disease (PD), Speech & Language Therapy, voice treatment, treatment outcomes, patient reported outcomes, and quality-of-life were used, with the search limited to the English language. We included studies published between 2008 and 2018 which had voice/speech treatment as a main focus, which included PROMs and/or sought to obtain the perspective of pwPD on voice/SLT treatment. The initial search yielded 75 articles of potential interest. We excluded papers if: they were not written in English; did not have voice treatment as the main focus; or did not include a PROM and/or information pertaining to pwPD perspectives on voice/SLT treatment. Sixty papers were excluded on this basis, leaving 16 papers for analysis. Any additional papers meeting inclusion criteria identified from reading the selected articles were also included in the review.
Speech and voice changes in PD
Up to 90% of pwPD report changes to their speech and voice3,9–11 with around 50% experiencing deterioration which renders it difficult to make themselves understood to strangers.9
The underlying pathophysiological bases of voice, speech, and language changes in PD are complex. Voice quality changes, reduced loudness, loss of intonation variation, and imprecise articulation relate in part to rigidity and stiffness in the oral, laryngeal, and respiratory muscles.12–15 However, stiffness and rigidity are insufficient to totally account for changes.
A crucial common denominator that appears to link impairment of articulatory movements, voice production, hand gestures accompanying speech, as well as many other non-communication related motor responses, concerns a failure to adequately scale the dynamics of movement to achieve the required range, force, and velocity, even though basic tone, power, and coordination are sufficient to do so.13,14 Further, pwPD exhibit reduced awareness of the extent and consequences of the under scaling. This appears associated with a deficit in central sensory processing.16,17 Thus, the pwPD is able to achieve adequate loudness, articulatory precision and emphasis when specifically asked to do so—even though increases in loudness may not match those that unaffected speakers make when asked to speak loudly.18,19 However, the pwPD may find it difficult to maintain these features during general conversation.
It is also important to emphasize that changes in language processing affect the speed at which pwPD can formulate and follow utterances, and can result in some distinct cognitive-linguistic impairments.11,20–22 Importantly, changes may not involve just expressive spoken communication but may also include the understanding and following of the speech of others. These receptive difficulties apply to prosody too. PwPD are poorer than people without PD at comprehending the tone or implications of an utterance that are signaled in the prosodic content.13,17,23,24 Issues with understanding the prosodic content of others’ utterances as well as producing adequate prosodic cues on the part of the pwPD have been particularly linked to the expression and understanding of emotional content.14,25,26 Together, the cognitive-linguistic and prosodic disturbances commonly result in carer reports that their partner with PD no longer seems to appreciate humor in the way they used to or regularly misunderstands conversations where the message relies on decoding prosodic, lexical, or syntactic subtleties.
PwPD perspectives on change in speech and voice
In terms of pwPD perspectives, impaired communication results in significant restrictions on daily living activities and social participation, and is strongly associated with reduced quality-of-life.27–33 Perceived impact can be significant for the pwPD, even when listeners detect no apparent major issues with voice and speech.28,30,34–36 PwPD describe their voice as too quiet, or volume fades fast over an utterance or in conversation; they describe voice quality as hoarse, breathy, tremulous, and that they have difficulty initiating or sustaining utterances.37,38 Freezing of voice can be as troublesome as freezing of gait.27 Disturbance to speech prosody (stress, intonation, rhythm of speech) is also described as a strong feature.39–41 PwPD report the frustrations of listeners seeming to misunderstand or miss the emotion they are aiming to convey, or the constant feeling that people believe them to be depressed, disinterested, and unmotivated when they are not.42–44 Such impressions are reinforced by hypomimia.45,46 To listeners, articulation may sound distorted or sounds omitted and/or syllables and words slurred together, which may give the impression that the pwPD is speaking too fast. Listeners also describe sudden rushes of accelerated speech, maybe in an attempt to complete a sentence on insufficient breath.
Such insights illustrate how challenges in communicating go well beyond (just) a quiet voice. Furthermore, difficulty initiating voice often means the pwPD is unable to signal they want a turn in conversation, with the situation not aided by a masked expression which removes the usual facial expression cues one gives to others that one wishes to say something. Hesitancy and pauses once a pwPD commences speaking may be mistaken by listeners that a turn was not wanted after all or the pwPD has finished their contribution. Conversations require sustained attention with complex switches in topic and between speakers; they require fast processing of what is said and, if a reply is to be made, rapid formulation of a reply. Typically several strands of conversation have to be attended to simultaneously, and speaking is often performed alongside other motor activity (eg, walking and gesturing). Therefore, communication takes place in a dual or competing task situation and all of these demands represent areas affected in pwPD.26,47
However, voice and speech convey much more than merely linguistic messages. They are integral to one’s view of oneself and how people perceive you. Voice and speech convey ones personality (eg, warm, distant, friendly) and how one is feeling (eg, happy, sad, anxious, tired, excited). Voice and speech also signal ones gender, age, class, geographical provenance, as well as ones hopes, allegiances, and aspirations.48 Changes to how all these are signaled when one has dysphonia, dysarthria, dysprosody, and altered language processing can seriously alter ones confidence in the view of oneself, and the view that others might hold of a pwPD. More broadly, people with acquired motor speech disorders similar to pwPD have reported these changes as a kind of personality theft.49,50They feel unable to convey the deeper message they intend, and feel that listeners continually misinterpret the sentiments, emotions, beliefs, and affective intentions they wish to convey. Loss of the ability to communicate in the way they used to, the way they wish to, may lead to a sense of bereavement as much as losing a limb, eyesight, or a friend.51
These factors translate into common threads in reports from pwPD about how communication changes impact on them and their families. In a questionnaire survey,10,30 pwPD rated themselves (compared with before they had PD) as less in control in conversations, that communication was more frustrating, that it was harder to get the message across, and that they felt less confident, less adequate, and less independent. Interviews with pwPD27,33 disclose concerns over the effort (and consequent added fatigue) involved in communicating, challenges from the vigilant attention required, and from the physical challenge of sustaining intelligible speech. Speakers felt they had to make decisions between not always joining in conversations in order to conserve energy but at the same time not wishing to withdraw from social discourse altogether. Frustrations arose too from people talking across them, not permitting enough time for responses, having to repeat over and again, and from being perceived as muddled or stupid. In addition to coping with the impairment arising from communication changes, pwPD also have to cope with issues of loss of confidence, social withdrawal, and change in personality.27,30,33,50
Such reports are consistent with the growing emphasis on patient-centered care and the shift from a narrow focus purely on speech-voice mechanics.52 People experience dysarthria differently, and personal context (including co-existing physical disability) is important in deciding the nature (and delivery) of treatment.28,50,53,54 Yorkston et al55 identify five important themes to consider in treatment for pwPD: (1) the difficulty of thinking about how to speak as well as what to say (thinking about speaking); (2) fatigue related to trying to “make the unconscious conscious” (weighing value vs effort); (3) expressions of frustration, embarrassment, and loss (feelings about speaking); (4) the distracting effect of PD on the other person (people and places); (5) waiting until medication takes effect to talk (PD and speaking). Spurgeon et al56 describe four further considerations: (1) emotional reactions (eg, frustration, embarrassment, lack of confidence, anxiety); (2) physical impact (eg, fatigue, breathing, and swallowing); (3) practical aspects (eg, cost of treatment, waiting times), and (4) expectations about treatment (met vs unmet expectations).
These points offer a number of important implications for assessment and intervention, as discussed in the next section.
Assessment considerations
Traditional assessment of PD speech characteristics concentrate on assessing speech/voice loudness (habitual loudness and variability of loudness), voice quality, articulatory precision, prosody, and intelligibility.54,57,58 However, the patient and carer experience require detailed assessment too, in particular for how communication changes impact on daily living and psychosocial well-being. Increasingly attention to this aspect of outcomes is attended to through use of patient reported outcome measures (PROMs).
Studies summarized in Table 1 show that PROMs are utilized to some extent in treatment studies using the LSVT® programme56,59–62 variants of LSVT,63–65 and programs based on singing and group voice treatment.65–68 The measures are widely used in voice clinics, and include the Voice Handicap Index (VHI),69 the Voice Activity & Participation Profile (VAPP),70 and the Voice Related Quality of Life Measure (V-RQoL).71 PROMs, in addition to measuring disability, allow the clinician to measure the effect of intervention on a person’s quality-of-life regarding activity and participation in social situations. Several such tools specifically devised for pwPD/dysarthria have been developed and psychometrically validated, including the use of semantic differential scales,30 the Dysarthria Impact Profile (DIP),53 the Communicative Effectiveness Survey (CES),72 and the Communicative Participation Item Bank (CPIB).73 Some studies have used questionnaires and/or interviews to find out from pwPD and spouse/carer what are the issues related to communication for them in daily living.2,33,56,65 Together the PROMs designed to measure disability related to voice/speech difficulties and first hand reports from pwPD and spouse/carer point to issues that should be addressed in treatment. These issues will be elaborated on in a later section, titled “PwPD perspectives regarding speaking and voice treatment”.
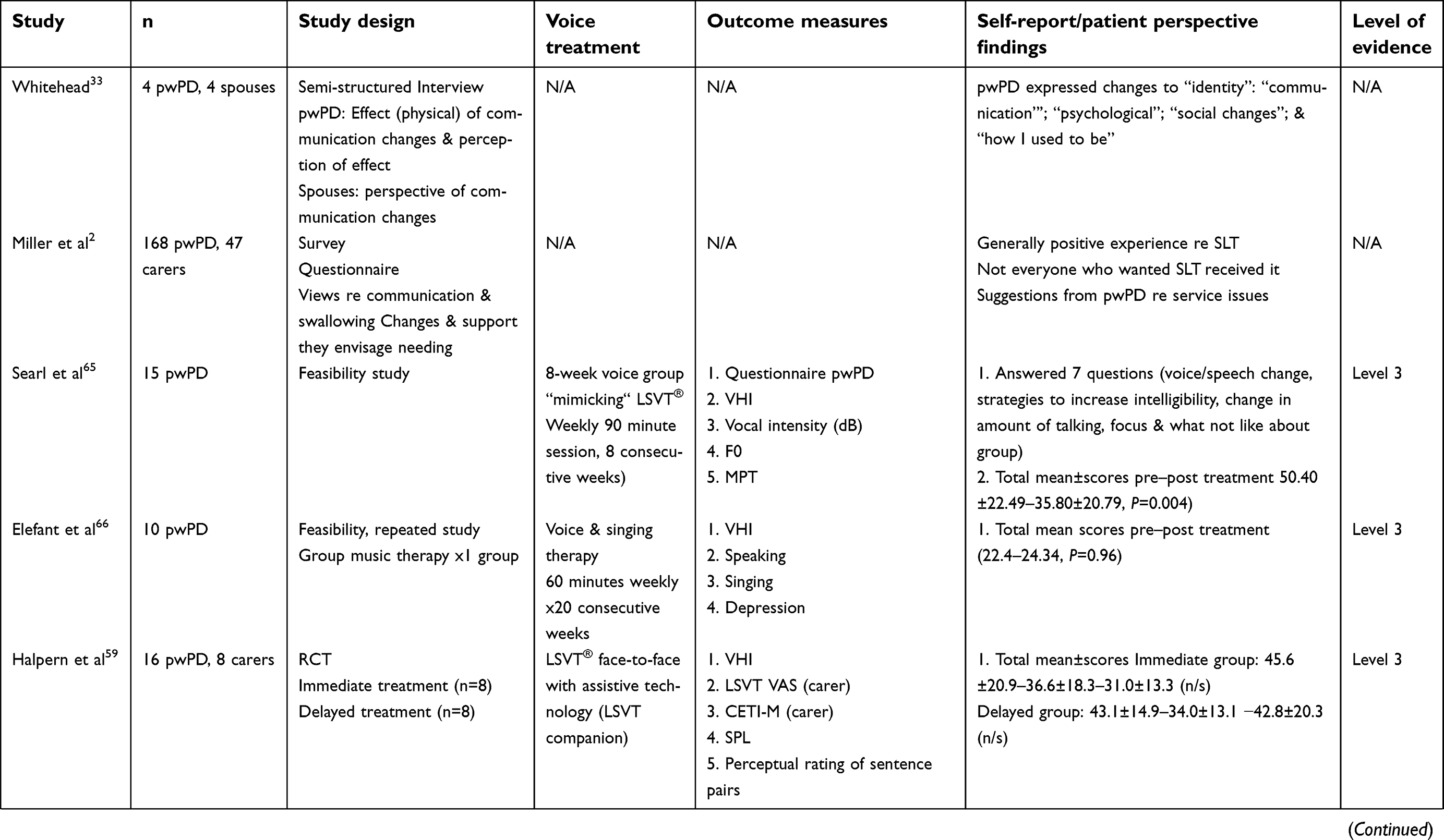 | 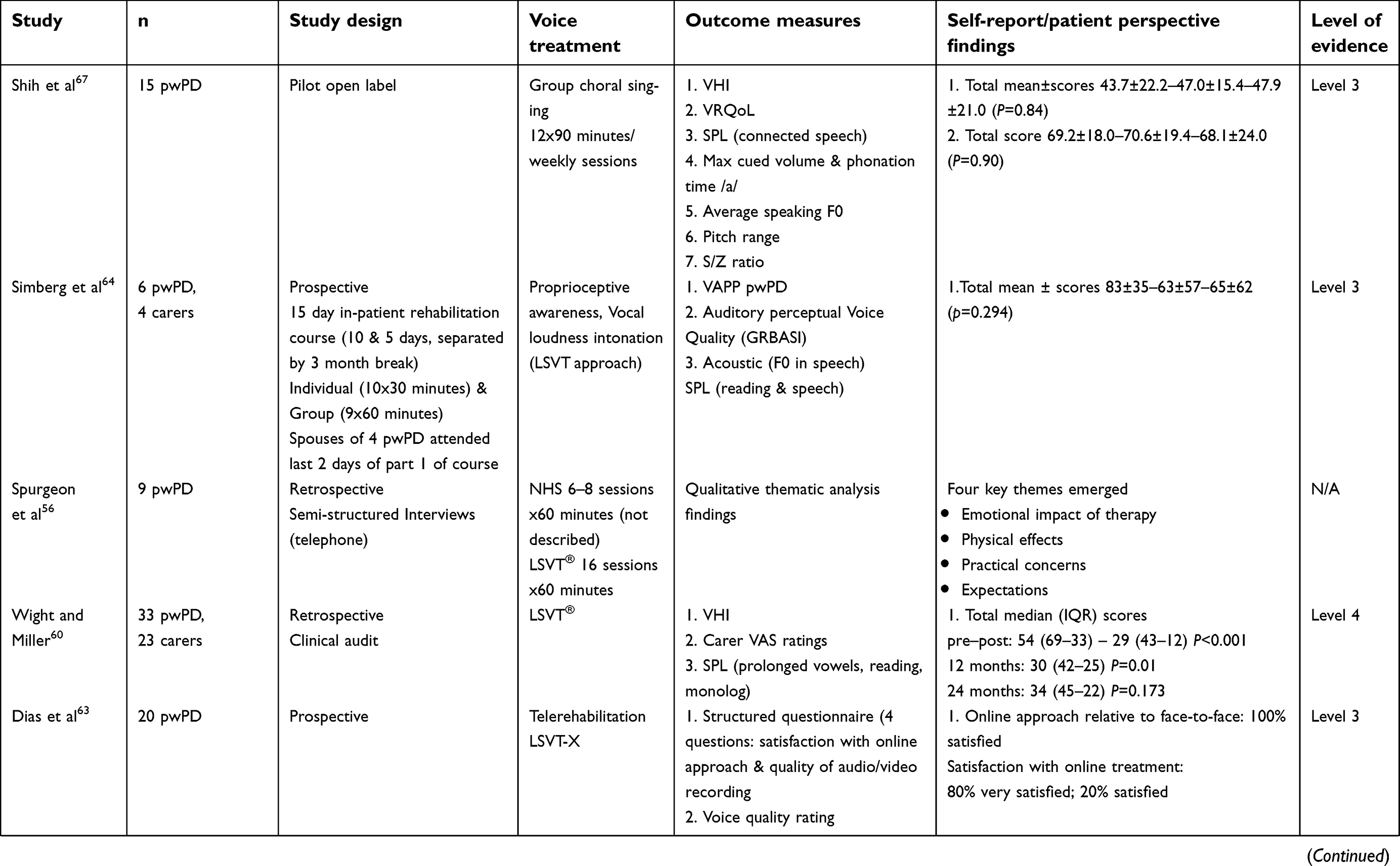 |  |  |
Table 1 Summary of treatment studies incorporating patient perspectives and/or self-report measures |
Treatment outcomes relating to PROMs and patient perspectives
Intervention that focuses on improving loudness, articulatory precision, and unambiguous prosodic signals is a first step in rehabilitation. However, communication is social and, hence, rehabilitation must also address how to employ improvements to gain entry to and maintain an individual’s part in conversations. Further, as problems maintaining intelligibility increase in dual- or competing task contexts, intervention should employ methods that tackle maintenance and generalization of communicative competence outside the clinic room in naturalistic environments that are inherently of a dual and competitive task nature. The treatment studies summarized in Table 1 highlight that different approaches (eg, LOUD®, LSVT variations, standard SLT treatment, voice/singing) and different treatment contexts (one-to one, group, online) have been used.
Considering the salience and functional impact of loudness deficits in pwPD, it is not surprising that a major treatment focus has been on increasing loudness levels (also measured sometimes as sound pressure level, SPL) in an effort to improve overall intelligibility. The Lee Silverman Voice Treatment (LSVT®) approach developed pre-existing attention to effort techniques to specifically address this.62 The main outcome measures are SPL when producing a prolonged /a/, and intelligibility rating of a reading passage and conversational speech. In addition, the LSVT® program evaluates the perception of the spouse/carer regarding a range of parameters, including loudness, intelligibility of speech, initiating conversation, using a 100 m visual analog scale (VAS).
The effect of treatment on voice disability, communicative function, and social interaction and the duration of any treatment benefit is highly relevant. Table 1 summarizes the findings of treatment studies (2008–2018) which incorporated a patient reported outcome measure (PROM) and/or sought to determine the perspective of pwPD of speech/voice and/or treatment. A range of PROMs including the VHI,59–61,65–67,74 the V-RQOL,74 VAPP,64 LSVT VAS,59,60 and CETI- M59,62 for spouse/carers were used to determine the effects of treatment.
The studies reviewed show a mixed picture regarding voice treatment effect on disability both in the immediate post-treatment and longer term period. Using the VHI in an 8 -week voice group “mimicking” LSVT, Searl et al65 reported a statistically significant reduction in VHI scores in the immediate post-treatment period whereas Elefant et al,66 in a 20 -week music therapy group, reported a slight increase (increasing disability) without significance post-treatment. Studies have also looked at the longer-term effects of intervention using the VHI.59–61,67 Moya-Galé et al,61 using LSVT®, reported a reduction in scores without significance 1 month post-treatment. Shih et al67 reported a slight non-significant increase in scores (increased disability) 3 months post-treatment using group choral singing. Halpern et al,59 using LSVT® with assisted technology, reported a reduction in VHI scores without statistical significance 6 months post-treatment. Finally, in a retrospective clinical audit of pwPD receiving LSVT®, Wight andMiller60 reported a significant reduction (improvement) in VHI scores at 12 months, which was not maintained at 24 months.
Using different PROMs measures to the VHI, other studies also show mixed findings regarding the effect of treatment on voice disability and communication. Shih et al67 found no significant change in VRQoL scores in the immediate or 3-months post-treatment period when pwPD engaged in a group singing therapy. Simberg et al64 reported a reduction in VAPP scores (improvement) following an intensive 15 day rehabilitation course in speech and voice treatment 6 months and 12 months post-treatment without significance. Finally, using the CETI-M, which is a broader communicative measure than any of the aforementioned voice disability measures, Ramig et al,62 using LSVT® in an RCT, reported a significant change in median CETI-M scores at 1 and 7 months post-treatment.
To take a broader look at the level of evidence for voice treatment studies covered by this review, we also applied the Oxford Centre of Evidence-Based Medicine 2011 Levels of Evidence table,75 which ranges from level 1 (systematic review of randomized trials) to level 5 (mechanism-based reasoning studies). Table 1 shows that the majority of intervention studies (n=8) were prospective non-randomized controlled cohort studies (Level 3), but with two RCT studies (Level 2). Clearly a larger range of high quality (Level 2) intervention studies would strengthen the evidence base.
Improved social participation is an important indicator of treatment outcomes, since it shows that intervention has made a meaningful impact on the ability of a pwPD to do the things he/she wants and needs to do.53,72,73 The World Health Organization, International Classification of Functioning, Disability and Health (ICF)76 defines participation as “involvement in life situations”. The Communicative Participation Item Bank (CPIB)77 was designed as a self-report measure, intended for community dwelling adults across a range of communication disorders and life situations specifically to measure communicative participation. Used in a large cohort of 378 pwPD in the US and New Zealand, the CPIB results (alongside other PD specific, a Global Health Instrument, and self-report measures) showed that communicative participation in pwPD is influenced by demographic and disease-based variables.73 The findings call for a broader view of the communicative experiences of pwPD. Increased use of the CPIB, DIP, and similar tools in future PD treatment studies would enhance the knowledge of pwPD communicative participation in everyday life and how it changes in response to SLT and/or voice intervention.
PwPD perspectives regarding speaking and voice treatment
Consistent with the growing emphasis on patient-centered care,52 we need to understand the issues for a pwPD communicating on a day-to-day basis and to hear their experience of living with a communication disability, their experience of voice treatment, and what they would like to see happen in the future. Important contributions emerge when patients and spouses are asked directly to give their opinions through interviews and surveys.55,56 When the views of 24 community dwelling pwPD were sought regarding their communication experiences, five subthemes emerged including: difficult to think about how to speak as well as what to say (thinking about speaking); fatigue related to trying to make the unconscious conscious (weighing value vs effort); expressions of frustration, embarrassment, and loss (feelings about speaking); the distracting effect of PD on the other person (people and places); waiting until the PD pills take effect to talk (PD and speaking).55
Regarding voice treatment and/or SLT, pwPD have reported positive comments in studies.54,56,64 However, since the focus of the above studies was to identify areas of potential improvement (rather than what SLT intervention is working well for pwPD), there is little elaboration in the studies regarding what pwPD and or carers found helpful. PwPD commonly report the importance of peer support (meeting others with PD) during treatment.54,64,67,78 For example, the participants in Simberg et al’s64 15-day treatment study emphasized the positive effect of peer support during the course which had combined one-to-one and group therapy. This is highly relevant feedback since the LSVT LOUD treatment approach delivered in a one-to-one context (face-to-face or remotely) is used more frequently than any other voice treatment approach for pwPD in many countries. Stegemoller et al78 reported findings from an 8 -week group program delivered by a music therapist to 20 pwPD, with a focus on voice exercises and singing. PwPD found the group fun, enjoyed the social aspect of meeting others with PD, and valued an outlet independent of family members and close friends.
Studies that have focussed specifically on pwPD perspectives provide valuable insight into the issues for pwPD embarking on a rehabilitation journey, and how SLT intervention could address these concerns.2,33,54–56 Using a survey approach, Miller et al2 reported on 168 pwPD and 47 carers views regarding SLT service provision relating to communication and swallowing. Their goal was to ascertain the issues that were a priority for attention for pwPD (those who had received an SLT referral, and those who had not), the methods of delivery and organization, and the level of support that might be favored. Pointers for improvement centered on the timing, intensity, duration, and access to SLT, as well as issues around transfer and maintenance of gains outside the clinic and (lack of) attention to psychosocial dimensions. Availability of ongoing support as the situation evolved and access to SLT when it was needed were two prominent features in pwPD feedback.
Other studies report negative issues which could impact adversely on rehabilitation outcomes. Spurgeon et al,56 in a qualitative telephone interview pilot study of nine pwPD who had received voice treatment (NHS standard treatment or LSVT), found that emotional factors associated with having speech/voice problems and treatment were the biggest issue for the interviewees.56 The pwPD talked about the persistence of speech problems after treatment (the embarrassment, lack of confidence, disappointment, and anxiety related to their communication difficulties), and fatigue related to getting to and from sessions. On a practical level, issues related to the cost of treatment, waiting list times, and the actual clinical experience were also raised by pwPD during the interviews. A final issue emerged relating to met vs unmet expectations around therapy outcomes and maintenance of therapy over time. PwPD with high expectations from therapy were typically disappointed with the clinical outcomes and maintenance over time, in contrast to those with lower expectations, who gave more positive feedback on the process and the results.56
These aforementioned studies provide important insight into the perspectives of pwPD regarding their lived experiences with a communication disability and their views on voice treatment. Another and often forgotten aspect is finding out from the pwPD spouse and/or caregiver their views on the impact of the communication disability on their relationship and social.
The spouse/carer perspective
Communication changes occur in a social context. Consequently, it is important to explore the views of the spouse/carer of a pwPD views concerning the communication difficulty, the impact on everyday living, social interaction, and emotional well-being, and the value of the treatment approaches. In Miller et al’s2 study, carers reported a number of issues in relation to their specific pwPD including “reduced loudness” (25%), a reluctance to engage in conversations (21%), social isolation (23%), and a reduction in confidence. Whitehead33 interviewed three spouses of pwPD in a qualitative interview based study. The spouses considered that, for their respective pwPD, communication was limited because of a number of factors including speech & language changes, loss of confidence, and social withdrawal. These carer observations are clearly similar to the pwPD self-reports.
A number of carer’s questionnaires,59,60,64 interviews,64 and surveys30,54 have been used to as a voice treatment outcome measure. Wight and Miller60 in their LSVT treatment study showed that spouse/carers rated all areas on the LSVT VAS as having improved significantly post-therapy. However, at 12 months, only perceived loudness, strain, mumbling, and intelligibility remained statistically significantly above baseline with no significant gains persisting to 24 months. Halpern et al59 used the CETI-M and the LSVT VAS with carers. The CETI-M asks significant others to indicate how effective they believe that the participant is at communicating in each of 10 different situations. Simberg et al,64 in their interviewing of six spouses of pwPD post in-patient intensive treatment, focused on loud voicing and intonation, reported that all spouses had noticed a change in the voices of the respective pwPD, with voice being more vivid and expressive, easier to understand, and with no need for repeating utterance as before. These changes remained relatively constant 3 months after the first part of the course, when all the spouses were interviewed by telephone.
In conclusion it would seem that the carer’s perspective of the impact of voice and speech therapy treatment provides valuable information, but is currently limited and worthy of significantly more investigation.
Conclusion
This review has highlighted that the motor changes of PD may influence voice and speech, but there are additional issues related to the disease process itself, including fatigue, cognitive decline, and medication effects that together impact on social functioning, and emotional well-being for the pwPD and his/her spouse.
This review shows that voice treatment studies (2008–2018) are primarily impairment focused, with PROMs used to measure disability pre- and post-treatment. Alongside this, some studies extend voice treatment into singing and group voice work, as an adjunct to traditional one-to-therapy, or as a sole treatment approach. A number of voice and speech therapy treatment programs show promise at improving speech and voice parameters as well as quality-of-life. In general terms, pwPD appear positive about SLT and/or voice treatment.54–56,62,64,65,78 However, it seems as though emotional factors and long-term maintenance issues are rarely addressed in current treatment programs.54,56
Similarly, practical issues such as fatigue related to traveling to sessions, treatment cost, and waiting list times are rarely considered.54,56
Moving forward, greater cognisance should be given to the lived experiences of pwPD (and their spouses) with a communication disability, and how SLT/voice treatment can best support the patient. Issues for consideration are optimum location for treatment (transport issues), timing (medication-related), frequency and duration of treatment (fatigue), one-to-one and/or group treatment, etc.
Future research should also focus on treatment compliance, practicality, and long-term follow-up. It is acknowledged the carer of the pwPD is a key partner, especially for wider implementation and maintenance of gains and judging intervention efficacy.
Abbreviation list
CES, Communicative Effectiveness Survey; CETI-M, Modified Communication Effectiveness Index; CPIB, Communicative Participation Item Bank; GSI, Group Singing Intervention; HC, healthy controls; LSVT-X, LSVT extended; MPT, maximum phonation time; MEP, maximum expiratory pressure; MIP, maximum inspiratory pressure; NHS, National Health Service; N/A, not applicable; UNTXPD, Untreated PD; SPL, sound pressure level; VAPP, voice activity and participation profile; VAS, Visual Analog Scale; VHI, Voice Handicap Index; V-RQoL, voice related quality-of-life measure.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Miller N, Allcock L, Jones D, Noble E, Hildreth A, Burn D. Prevalence and pattern of perceived intelligibility changes in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2007;78(11):1188–1190.
2. Miller N, Noble E, Jones D, Deane KH, Gibb C. Survey of speech and language therapy provision for people with Parkinson’s disease in the United Kingdom: patients’ and carers’ perspectives. Int J Lang Commun Disord. 2011;46(2):179–188. doi:10.3109/13682822.2010.484850
3. Schalling E, Johansson K, Hartelius L. Speech and communication changes reported by people with Parkinson’s disease. Folia Phoniatrica Et Logopaedica. 2017;69(3):131–141. doi:10.1159/000479927
4. Rusz J, Cmejla R, Ruzickova H, Ruzicka E. Quantitative acoustic measurements for characterization of speech and voice disorders in early untreated Parkinson’s disease. J Acoust Soc Am. 2011;129(1):350–367. doi:10.1121/1.3514381
5. Miller N. Swallowing in Parkinson’s disease: clinical issues and management. Neurodegener Dis Manag. 2017;7(3):205–217. doi:10.2217/nmt-2017-0006
6. Sapir S. Multiple factors are involved in the dysarthria associated with Parkinson’s disease: a review with implications for clinical practice and research. J Speech Lang Hearing Res. 2014;57(4):1330–1343. doi:10.1044/2014_JSLHR-S-13-0039
7. Atkinson-Clement C, Sadat J, Pinto S. Behavioral treatments for speech in Parkinson’s disease: meta-analyses and review of the literature. Neurodegener Dis Manag. 2015;5(3):233–248. doi:10.2217/nmt.15.16
8. Dashtipour K, Tafreshi A, Lee J, Crawley B. Speech disorders in Parkinson’s disease: pathophysiology, medical management and surgical approaches. Neurodegener Dis Manag. 2018;8(5):337–348. doi:10.2217/nmt-2018-0021
9. Miller N, Allcock L, Jones D, Noble E, Hildreth AJ, Burn DJ. Prevalence and pattern of perceived intelligibility changes in Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2007;78(11):1188–1190. doi:10.1136/jnnp.2006.110171
10. Miller N, Noble E, Jones D, Deane KHO, Gibb C. Survey of speech and language therapy provision for people with Parkinson’s disease in the United Kingdom: patients’ and carers’ perspectives. Int J Lang Commun Disord. 2011;46(2):179–188.
11. Miller N. Communication changes in Parkinson’s disease. Pract Neurol. 2017;17(4):266–274. doi:10.1136/practneurol-2017-001635
12. Gruszka A, Hampshire A, Barker RA, Owen AM. Normal aging and Parkinson’s disease are associated with the functional decline of distinct frontal-striatal circuits. Cortex. 2017;93:178–192. doi:10.1016/j.cortex.2017.05.020
13. Mollaei F, Shiller DM, Baum SR, Gracco VL. Sensorimotor control of vocal pitch and formant frequencies in Parkinson’s disease. Brain Res. 2016;1646:269–277. doi:10.1016/j.brainres.2016.06.013
14. New AB, Robin DA, Parkinson AL, et al. The intrinsic resting state voice network in Parkinson’s disease. Hum Brain Mapp. 2015;36(5):1951–1962. doi:10.1002/hbm.22748
15. Read J, Miller N, Kitsou N. Is there an order of loss of sounds in speakers with Parkinson’s disease? Clin Linguist Phon. 2018;32(11):997–1011. doi:10.1080/02699206.2018.1504989
16. Martens H, Van Nuffelen G, Wouters K, De Bodt M. Reception of communicative functions of prosody in hypokinetic dysarthria due to Parkinson’s disease. J Parkinson’s Dis. 2016;6(1):219–229. doi:10.3233/JPD-150678
17. Brajot FX, Shiller DM, Gracco VL. Autophonic loudness perception in Parkinson’s disease. J Acoust Soc Am. 2016;139(3):1364–1371. doi:10.1121/1.4944569
18. Iddon H, Read J, Miller N. Does voice amplification increase intelligibility in people with Parkinson’s disease? Int J Ther Rehabil. 2015;22(10):479–486. doi:10.12968/ijtr.2015.22.10.479
19. Neel AT. Effects of loud and amplified speech on sentence and word intelligibility in Parkinson disease. J Speech Lang Hear Res. 2009;52(4):1021–1033. doi:10.1044/1092-4388(2008/08-0119)
20. Bocanegra Y, García AM, Pineda D, et al. Syntax, action verbs, action semantics, and object semantics in Parkinson’s disease: dissociability, progression, and executive influences. Cortex. 2015;69:237–254. doi:10.1016/j.cortex.2015.05.022
21. Walsh B, Smith A. Linguistic complexity, speech production, and comprehension in Parkinson’s disease: behavioral and physiological indices. J Speech Lang Hear Res. 2011;54(3):787–802. doi:10.1044/1092-4388(2010/09-0085)
22. MacPherson MK, Huber JE, Snow DP. The intonation-syntax interface in the speech of individuals with Parkinson’s disease. J Speech Lang Hear Res. 2011;54(1):19–32. doi:10.1044/1092-4388(2010/09-0079)
23. De Keyser K, Santens P, Bockstael A, et al. The relationship between speech production and speech perception deficits in Parkinson’s disease. J Speech Lang Hearing Res. 2016;59(5):915–931. doi:10.1044/2016_JSLHR-S-15-0197
24. Albuquerque L, Martins M, Coelho M, et al. Advanced Parkinson disease patients have impairment in prosody processing. J Clin Exp Neuropsychol. 2016;38(2):208–216. doi:10.1080/13803395.2015.1100279
25. Kwan LC, Whitehill TL. Perception of speech by individuals with Parkinson’s disease: a review. Parkinson’s Dis. 2011;2011:389767. doi:10.4061/2011/153979
26. Pell MD, Monetta L, Rothermich K, Kotz SA, Cheang HS, McDonald S. Social perception in adults with Parkinson’s disease. Neuropsychology. 2014;28(6):905–916. doi:10.1037/neu0000090
27. Miller N, Noble E, Jones D, Burn D. Life with communication changes in Parkinson’s disease. Age Ageing. 2006;35(3):235–239. doi:10.1093/ageing/afj053
28. Walshe M, Miller N, Leahy M, Murray A. Intelligibility of dysarthric speech: perceptions of speakers and listeners. Int J Lang Commun Disord. 2008;43(6):633–648. doi:10.1080/13682820801887117
29. Miller N, Andrew S, Noble E, Walshe M. Changing perceptions of self as a communicator in Parkinson’s disease: a longitudinal follow-up study. Disabil Rehabil. 2011;33(3):204–210. doi:10.3109/09638288.2010.508099
30. Miller N, Noble E, Jones D, Allcock L, Burn DJ. How do I sound to me? Perceived changes in communication in Parkinson’s disease. Clin Rehabil. 2008;22(1):14–22. doi:10.1177/0269215507079096
31. Saldert C, Ferm U, Bloch S. Semantic trouble sources and their repair in conversations affected by Parkinson’s disease. Int J Lang Commun Disord. 2014;49(6):710–721. doi:10.1111/1460-6984.12105
32. McAuliffe M, Baylor C, Yorkston K. Variables associated with communicative participation in Parkinson’s disease and its relationship to measures of health-related quality-of-life. Int J Speech Lang Pathol. 2017;19(4):407–417. doi:10.1080/17549507.2016.1193900
33. Whitehead B. The psychosocial impact of communication changes in people with Parkinson’s disease. Br J Neurosci Nurs. 2010;6(1):30–36. doi:10.12968/bjnn.2010.6.1.46056
34. Hartelius L, Miller N. The ICF framework and its relevance to the assessment of people with motor speech disorders. In: Lowit A, Kent R, editors. Assessment of Motor Speech Disorders. San Diego: Plural; 2010;1:1–20.
35. Kim HA, Kim SW, Yoon JH. Comparison between self-reported and objective measures on speech characteristics in patients with Parkinson’s disease. Commun Sci Disord-Csd. 2018;23(1):228–241. doi:10.12963/csd.17453
36. Dykstra AD, Adams SG, Jog M. Examining the relationship between speech intensity and self-rated communicative effectiveness in individuals with Parkinson’s disease and hypophonia. J Commun Disord. 2015;56:103–112. doi:10.1016/j.jcomdis.2015.06.012
37. Skodda S, Grönheit W, Schlegel U. Intonation and speech rate in Parkinson’s disease: general and dynamic aspects and responsiveness to levodopa admission. J Voice. 2011;25(4):e199–e205. doi:10.1016/j.jvoice.2010.04.007
38. Motta S, Cesari U, Paternoster M, Motta G, Orefice G. Aerodynamic findings and voice handicap index in Parkinson’s disease. Eur Arch Oto-Rhino-Laryn. 2018;275(6):1569–1577. doi:10.1007/s00405-018-4967-7
39. Ma JKY, Schneider CB, Hoffmann R, Storch A. Speech prosody across stimulus types for individuals with Parkinson’s disease. J Parkinson’s Dis. 2015;5(2):291–299. doi:10.3233/JPD-140451
40. Elfmarková N, Gajdoš M, Mračková M, Mekyska J, Mikl M, Rektorová I. Impact of Parkinson’s disease and levodopa on resting state functional connectivity related to speech prosody control. Parkinsonism Relat Disord. 2016;22(Supplement 1):S52–S55. doi:10.1016/j.parkreldis.2015.09.006
41. Galaz Z, Mekyska J, Mzourek Z, et al. Prosodic analysis of neutral, stress-modified and rhymed speech in patients with Parkinson’s disease. Comput Methods Programs Biomed. 2016;127:301–317. doi:10.1016/j.cmpb.2015.12.011
42. Lyons K, Tickle-Degnen L, DeGroat E. Inferring personality traits of clients with Parkinson’s disease from their descriptions of favourite activities. Clin Rehabil. 2005;19(7):799–809. doi:10.1191/0269215505cr897oa
43. Jaywant A, Pell M. Listener impressions of speakers with Parkinson’s disease. J Int Neuropsychol Soc. 2010;16(1):49–57. doi:10.1017/S1355617709990919
44. Balash Y, Korczyn A, Knaani J, Migirov A, Gurevich T. Quality-of-life perception by Parkinson’s disease patients and caregivers. Acta Neurol Scand. 2017;136(2):151–154. doi:10.1111/ane.12726
45. Gunnery SD, Habermann B, Saint-Hilaire M, Thomas CA, Tickle-Degnen L. The relationship between the experience of hypomimia and social wellbeing in people with Parkinson’s disease and their care partners. J Parkinson’s Dis. 2016;6(3):625–630. doi:10.3233/JPD-160782
46. Bandini A, Orlandi S, Escalante HJ, et al. Analysis of facial expressions in parkinson’s disease through video-based automatic methods. J Neurosci Methods. 2017;281:7–20. doi:10.1016/j.jneumeth.2017.02.006
47. Holmes JD, Jenkins ME, Johnson AM, Adams SG, Spaulding SJ. Dual-task interference: the effects of verbal cognitive tasks on upright postural stability in Parkinson’s disease. Parkinson’s Dis. 2010;2010:696492.
48. Llamas C, Watt D, editors. Language and Identities. Edinburgh: Edinburgh University Press; 2010.
49. Miller N, Taylor J, Howe C, Read J. Living with foreign accent syndrome: insider perspectives. Aphasiology. 2011;25(9):1053–1068. doi:10.1080/02687038.2011.573857
50. Walshe M, Miller N. Living with acquired dysarthria: the speaker’s perspective. Disability Rehabil. 2011;33(3):195–203. doi:10.3109/09638288.2010.511685
51. Lawson RA, Collerton D, Taylor J-P, Burn D, Brittain K. Coping with cognitive impairment in people with Parkinson’s disease and their carers: a qualitative study. Parkinson’s Dis. 2018;2018:1–10. Article ID 1362053. doi:10.1155/2018/1362053.:10
52. Cleary PD. Evolving concepts of patient-centered care and the assessment of patient care experiences: optimism and opposition. J Health Politics Policy Law. 2016;41(4):675–696. doi:10.1215/03616878-3620881
53. Walshe M, Peach R, Miller N. Dysarthria impact profile: development of a scale to measure psychosocial effects. Int J Lang Commun Disord. 2009;44(5):693–715. doi:10.1080/13682820802317536
54. Miller N, Deane KH, Jones D, Noble E, Gibb C. National survey of speech and language therapy provision for people with Parkinson’s disease in the United Kingdom: therapists’ practices. Int J Lang Commun Disord. 2011;46(2):189–201. doi:10.3109/13682822.2010.484849
55. Yorkston K, Baylor C, Britton D. Speech versus speaking: the experiences of people with Parkinson’s disease and implications for intervention. Am J Speech Lang Pathol. 2017;26(2S):561–568. doi:10.1044/2017_AJSLP-16-0087
56. Spurgeon L, Clarke CE, Sackley C. Subjective experiences of speech and language therapy in patients with Parkinson’s disease: a pilot study. Rehabil Res Pract. 2015;2015:1–11. [Erratum appears in Rehabil Res Pract. 2016;1654282; PMID: 27630774]. doi:10.1155/2015/839895
57. Tjaden K, Lam J, Wilding G. Vowel acoustics in Parkinson’s disease and multiple sclerosis: comparison of clear, loud, and slow speaking conditions. J Speech Lang Hear Res. 2013;56(5):1485–1502. doi:10.1044/1092-4388(2013/12-0259)
58. Anand S, Stepp C. Listener perception of monopitch, naturalness, and intelligibility for speakers with Parkinson’s disease. J Speech Lang Hearing Res. 2015;58(4):1134–1144. doi:10.1044/2015_JSLHR-S-14-0243
59. Halpern A, Ramig L, Matos C, et al. Innovative technology for the assisted delivery of intensive voice treatment (LSVTLOUD) for Parkinson disease. Am J Speech Lang Pathol. 2012;21(4):354–367. doi:10.1044/1058-0360(2012/11-0125)
60. Wight S, Miller N. Lee silverman voice treatment for people with Parkinson’s: audit of outcomes in a routine clinic. Int J Lang Commun Disord. 2015;50(2):215–225. doi:10.1111/1460-6984.12132
61. Moya-Galé G, Goudarzi A, Bayés A, McAuliffe M, Bulté B, Levy E. The effects of intensive speech treatment on conversational intelligibility in Spanish speakers with Parkinson’s disease. Am J Speech Lang Pathol. 2018;27(1):154–165. doi:10.1044/2017_AJSLP-17-0032
62. Ramig L, Halpern A, Spielman J, Fox C, Freeman K. Speech treatment in Parkinson’s disease: randomized controlled trial (RCT). Mov Disord. 2018;33(11):1777–1791. doi:10.1002/mds.27460
63. Dias A, Limongi J, Barbosa E, Hsing W. Voice telerehabilitation in Parkinson’s disease. CoDAS. 2016;28(2):176–181. doi:10.1590/2317-1782/20162015161
64. Simberg S, Rae J, Kallvik E, Salo B, Martikainen K. Effects of speech therapy on voice and speech in Parkinson’s after a 15-day rehabilitation course: a pilot study. Int J Ther Rehabil. 2012;19(5):273–285. doi:10.12968/ijtr.2012.19.5.273
65. Searl J, Wilson K, Haring K, Dietsch A, Lyons K, Pahwa R. Feasibility of group voice therapy for individuals with Parkinson’s disease. J Commun Disord. 2011;44(6):719–732. doi:10.1016/j.jcomdis.2011.05.001
66. Elefant C, Baker FA, Lotan M, Lagesen SK, Skeie GO. The effect of group music therapy on mood, speech, and singing in individuals with Parkinson’s disease–a feasibility study. J Music Ther. 2012;49(3):278–302.
67. Shih LC, Piel J, Warren A, et al. Singing in groups for Parkinson’s disease (SING-PD): a pilot study of group singing therapy for PD-related voice/speech disorders. Parkinsonism Relat Disord. 2012;18(5):548–552. doi:10.1016/j.parkreldis.2012.02.009
68. Stegemöller E, Radig H, Hibbing P, Wingate J, Sapienza C. Effects of singing on voice, respiratory control and quality of life in persons with Parkinson’s disease. Disabil Rehabil. 2017;39(6):594–600. doi:10.3109/09638288.2016.1152610
69. Jacobson B, Johnson A, Grywalski C, et al. The Voice Handicap Index (VHI). Am J Speech Lang Pathol. 1997;6(3):66–70. doi:10.1044/1058-0360.0603.66
70. Ma EP, Yiu EML. Voice activity and participation profile. J Speech Lang Hearing Res. 2001;44(3):511–524. doi:10.1044/1092-4388(2001/040)
71. Hogikyan ND, Sethuraman G. Validation of an instrument to measure voice-related quality of life (V-RQOL). J Voice. 1999;13(4):557–569.
72. Donovan N, Kendall D, Young M, Rosenbek J. The communicative effectiveness survey: preliminary evidence of construct validity. Am J Speech Lang Pathol. 2008;17:335–347. doi:10.1044/1058-0360(2008/07-0010)
73. Baylor C, McAuliffe M, Hughes Louise E, et al. A Differential Item Functioning (DIF) Analysis of the Communicative Participation Item Bank (CPIB): comparing individuals with Parkinson’s disease from the United States and New Zealand. J Speech Lang Hearing Res. 2014;57(1):90–95. doi:10.1044/1092-4388(2013/12-0414)
74. Sackley C, Smith C, Rick C, et al. Lee silverman voice treatment versus standard speech and language therapy versus control in Parkinson’s disease: a pilot randomised controlled trial (PD COMM pilot). Pilot Feasibility Stud. 2018;4(1):30. doi:10.1186/s40814-017-0222-z
75. Oxford Centre for Evidence-Based Medicine. Levels of Evidence. University of Oxford; 2011. Available from: http://www.cebm.net. Accessed March 02, 2019.
76. World Health Organisation. 2001 International Classification of Functioning, Disability and Health (ICF). Geneva,Switzerland.
77. Baylor C, Yorkston K, Eadie T, Kim J, Chung H, Amtmann D. The Communicative Participation Item Bank (CPIB): item bank calibration and development of a disorder-generic short form. J Speech Lang Hearing Res. 2013;56(4):1190–1208. doi:10.1044/1092-4388(2012/12-0140)
78. Stegemöller EL, Hurt TR, O’Connor MC, et al. Experiences of persons with Parkinson’s disease engaged in group therapeutic singing. J Music Ther. 2017;54(4):405–431. doi:10.1093/jmt/thx012
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.