Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 10
Vitamin D and orthodontics: an insight review
Authors Almoammar K
Received 22 November 2017
Accepted for publication 26 January 2018
Published 30 July 2018 Volume 2018:10 Pages 165—170
DOI https://doi.org/10.2147/CCIDE.S157840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Khalid Almoammar
Department of Pediatric Dentistry & Orthodontics, College of Dentistry, King Saud University, Riyadh, Saudi Arabia
Abstract: Vitamin D is known as the oldest of all hormones. 7-Dehydrocholesterol is converted to previtamin D3. It becomes a secosteroid when it is later converted to 1,25-dihydroxyvitamin D3 (1,25(OH)2D3). A number of factors influence vitamin D3 production, including skin pigmentation, the use of sunscreen lotions, season, latitude, and altitude. Vitamin D is important for bone metabolism and calcium hemostasis. Researchers have linked a deficiency in vitamin D levels to a number of systemic complications, including cardiovascular disease, diabetes, immune deficiency, and infectious diseases. In orthodontics, laboratory studies have revealed some evidence that vitamin D enhances tooth movement and the stability of the tooth position. This review is an attempt to understand the role and systemic consequences of vitamin D deficiency and to examine its relevance to orthodontics.
Keywords: orthodontics, tooth movements, vitamin D, vitamin deficiency
Historical and physiological perspectives
Vitamin D is known as the oldest of all hormones, and researchers have discovered the presence of this vitamin in the early phytoplankton species Emiliani huxleyi,1 which produces vitamin D following sun exposure.1 Other oceanic life forms utilize the high calcium content of E. huxleii for neuromuscular and metabolic activities. As vertebrates evolved in areas surrounding oceans, they retained their need for calcium, an essential element in the development of the skeleton and bone mineralization.1 However, vertebrates needed to maintain vitamin D production for calcium absorption on land.1
A human body needs approximately 3,000–5,000 IU of vitamin D each day.2 A substantial proportion of the body’s daily requirement of vitamin D3 comes from dietary intake, especially fatty fish, eggs, and fortified foods.3,4 A recent cross-sectional study in the UK compared meat and fish eaters to vegetarians and vegans, revealing that vitamin D plasma levels were significantly higher among nonvegetarians compared to vegetarians.5
Hossein-nezhad and Holick6 showed that when people ingest vitamin D, the body incorporates it into chylomicrons. The body then releases it into the lymphatic system, and from there, it enters the venous blood.6 In the venous blood, vitamin D binds to vitamin D-binding proteins and lipoproteins, which are transported to the liver.6 Next, the liver processes vitamin D2 and vitamin D3 by 25-hydroxylation to make vitamin D metabolite, which clinicians and researchers use to determine patients’ vitamin D status.6 Then, in the kidneys, the vitamin D metabolite undergoes further hydroxylation to form the secosteroid hormone calciferol.6,7 However, the main source of vitamin D is sunlight exposure. In another study, Hollik indicated that following sun exposure, the body converts vitamin D into previtamin D3, lumisterol, and tachysterol via a process known as photoconversion, and that sun exposure improves isomerization to vitamin D3 by a heat-induced membrane.4 Once vitamin D3 is formed, vitamin D-binding proteins carry it to the dermal capillary bed.7,8 During this process, the presence of tachysterol and lumisterol prevents vitamin D intoxication when individuals are exposed to solar ultraviolet B (UVB) radiation for prolonged durations.8
A number of factors have been shown by researchers to influence vitamin D3 production, including skin pigmentation, age, clothing, the use of sunscreen lotions, time of the day, season, latitude, and altitude.2,7–9 In winter, the wide zenith angle of the sun causes the solar UVB photons to travel longer through the ozone layer before reaching the earth.8 This may explain why above and below approximately 33° latitude, little, if any, vitamin D3 is produced in the skin during winter.10 This may also explain why vitamin D3 synthesis occurs only between approximately 10 in the morning and 3 in the afternoon in equatorial regions.10
Consequences of vitamin D deficiency
The function of vitamin D is to maintain serum calcium and phosphate concentrations, which are important for many physiological functions.10 These include normal mineralization of bone, muscle contraction, nerve conduction, and prevention of hypocalcemic tetany.7,11 Researchers believe that 1,25(OH)2D is essential for the body’s ability to elevate intestinal calcium absorption to 40% and intestinal phosphorus absorption to 80%, which are necessary for skeletal well-being in humans.7 Sniadecki argued that inadequate exposure to sunlight in childhood causes devastating bone deformities known as rickets.8 Exposing children to UVB radiation (290–315 nm) using a mercury arc lamp or sunlight was shown to be an effective treatment for this condition, and even prevented it from occurring.12 In the 1930s, these findings led the US government to promote recommendations to parents regarding the benefits of sunlight exposure for bone health and the prevention of rickets.12,13 At the same time, the governments of the United States and Europe attempted to fortify milk with 100 IU of vitamin D2 per eight ounces to help with the widespread problem of rickets.12 However, in the 1950s, the UK government was criticized for the spread of hypercalcemia due to milk fortification with vitamin D.15 This rise in the incidence of hypercalcemia led authorities to prohibit the fortification of milk and other dairy products with vitamin D.14
Researchers have linked vitamin D deficiency to muscle pain and muscle weakness.7,15 In severe scenarios, researchers have found that muscle atrophy is related to secondary hyperparathyroidism, resulting in hypophosphatemia.7,15,16 A recent meta-analysis of elderly people showed that taking supplemental and active forms of vitamin D daily reduced the incidence of falls by 19% and 23%, respectively.17 In addition, a number of investigators have shown that the incidence of certain types of cancer was higher among populations in higher latitudes, who experienced reduced sun exposure.10,18 However, a double-blind, randomized clinical trial evaluating the effectiveness of high doses of vitamin D in improving the lower extremity activities and reducing the risks of falls showed that high doses of up to 60,000 IU neither significantly improved body functions nor reduced the incidence of falls despite adjusting the level of vitamin D in blood levels to 30 ng/mL.19
Previous studies have shed light on the connection between vitamin D deficiency and cardiovascular diseases.20–22 In the prospective Intermountain Heart Collaborative Study, which had more than 40,000 participants, the researchers showed that participants with levels of 1,25(OH)2D less than 15 ng/mL were more likely to suffer from hypertension, hyperlipidemia, peripheral vascular disease, coronary artery disease, myocardial infarction, heart failure, and stroke compared with healthy controls.23 In 2012, a meta-analysis evaluation through two prospective clinical trials revealed that a U-shaped relationship exists between vitamin D deficiency and the occurrence of cardiac problems. This confirms the increased susceptibility of individuals with low levels of vitamin D to the development of cardiovascular disease.24
In addition, a meta-analysis of 8 cohort studies and 11 randomized control trials revealed a strong correlation between low levels of vitamin D and incidence of diabetes mellitus.25 In fact, the incidence of type 2 diabetes mellitus was 52% higher among individuals with vitamin D levels above 25 ng/mL compared to those with levels below 14 ng/mL.25
From another perspective, some studies have shown links between the level of vitamin D and the incidence of autoimmune diseases.26–28 Multiple sclerosis, inflammatory bowel disease, rheumatoid arthritis, and Crohn’s disease are more common in high latitudes and in areas with low sun exposure.26–29 This relationship was further supported by a number of experiments demonstrating the role of vitamin D in regulating chemokine production, counteracting autoimmune inflammation, and encouraging the differentiation of immune cells.26,27,29 Furthermore, researchers have shown that vitamin D helps to improve immunity against tuberculosis, influenza, and viral upper respiratory tract infections.30
Numerous studies have evaluated the consequences of vitamin D deficiency. However, the data have been inconsistent, which might be due to variations in the diagnostic measures and cut-off values in defining a deficiency state.31
Prevalence of vitamin D deficiency
The levels of 25(OH)D3 in the serum are routinely used to assess vitamin D levels in routine clinical practice.31 In the United States, the Institute of Medicine stated that adults require 20 ng/mL of vitamin D (to convert this, nmol/L= ng/mL multiplied by 2.496).32 There is no evidence to suggest that serum concentrations greater than 20 ng/mL of vitamin D are harmful for individuals.32 Researchers have suggested that the ideal level of vitamin D that should be maintained in individuals is between 40 and 60 ng/mL, and levels up to 100 ng/mL are likely harmless.19 However, caution has been advised when considering daily supplementation doses exceeding >10,000 IU/d (>250 mg/d).33,34
The Endocrine Society considers children and adults with 25(OH)D levels of 20 ng/mL or less to be vitamin D deficient.19 Vitamin D insufficiency occurs when individuals have levels between 21 and 29 ng/mL, while vitamin D sufficiency is when individuals have levels of 30 ng/mL or greater.7
Generally, vitamin D levels are influenced by several factors, such as age, gender, diet, sunlight exposure, climate, and altitude.1 In the UK, more than 40% of the population experiences vitamin D insufficiency.35 Researchers have shown that this figure is usually much higher during winter and that the risk of vitamin D insufficiency increases with age, with adolescents being the most affected group among the young population. In one study, children and adolescents of Asian descent were less affected compared with age-matched participants of Caucasian origin.1,8 This may be attributed to the increased skin melanin pigmentation among Caucasians.1,8 The prevalence of low levels of vitamin D in adolescents in other parts of Europe is relatively high, ranging from 19% to 96%.6,36 As mentioned earlier, many factors affect vitamin D levels in the body. In line with this, high levels of vitamin D are generally found in the populations of Norway and Sweden, and it is believed that this is due to the high intake of fish and cod liver oil.3 The relatively lower levels of vitamin D that are found in the populations of Spain, Italy, and Greece have been attributed to sun avoidance and air pollution.3
In the United States, 32% of the population has vitamin D levels of <20 ng/mL.6,36 Those at risk of developing vitamin D deficiency include 70% of the Caucasian population and around 40% of the Hispanic/Mexican population.6,36 In a national cohort study in Canada, vitamin D levels below 30 ng/mL were found in 57.5% of men and 60.7% of women. During winter, these levels are even higher, with 73.5% of men and 77.5% of women experiencing deficiency. In the United States, vitamin D deficiency is estimated to occur in 27% to 91% of pregnant women.6,36,37 In other parts of the world, 45% to 100% of the population in Asia and 25% to 87% of the population in Australia have vitamin D deficiency.6 In New Zealand, children are at a high risk of developing vitamin D insufficiency due to their dietary intake, living at a low latitude, and their reduced skin melanin pigmentation.38 Researchers thus anticipate that in New Zealand, vitamin D deficiency ranged from 25% to 59%.38 In Australia, vitamin D levels were <30 ng/mL in 73% of adults.3
In the Middle East and Asia, vitamin D deficiency in children and adults is high, which is probably related to skin pigmentation and sun avoidance.7,39 In a recent meta-analysis, researchers found evidence to suggest that the prevalence of vitamin D deficiency is as high as 81% in Saudi Arabia.40 This was in line with recorded vitamin D levels in neighboring countries: 83% in Kuwait,41 86.4% in Bahrain,42 82.5% in the United Arab Emirates,43 and 84.7% among adult females in Qatar.44 Numerous other studies in Saudi Arabia showed that vitamin D deficiency was highly prevalent across all demographic groups.40,45–49 Specifically, a range of cut-offs between 25 and 50 nmol/L showed deficiency levels in 40% and 87% of the sample.40,45–49
Vitamin D and orthodontics
Bone remodeling, following the application of orthodontic forces, includes resorptive and bone formation phases at the alveolar process.50 A correlation has been shown between vitamin D receptor polymorphisms and periodontitis and bone metabolism.51 Researchers have shown that vitamin D, parathyroid hormone, and calcitonin regulate calcium and phosphorus levels.50,52 In various studies, vitamin D stimulated bone resorption by inducing the differentiation of osteoclasts from their precursors and increasing the activity of existing osteoclasts.53–55 One of the earlier attempts was made by Boyce and Weisbrode,56 who evaluated the effects of calcium-rich diets and vitamin D metabolite injection on bone formation in rats. On day 1, osteoclasts in treated rats increased in comparison to controls. On days 3 and 4, the researchers observed a decrease in the number of osteoclasts. This sequela continued through days 6, 8, and 10. Meanwhile, in the same experimental period, there was a substantial increase in the number of osteoblasts in treated rats compared to controls. As anticipated, the calcium and phosphorus levels were increased. Boyce and Weisbrode56 concluded that the experimental group experienced a net increase in bone formation (Table 1). Collins and Sinclair57 demonstrated that intraligamentary injections of vitamin D metabolites cause an increase in the number of osteoclasts, and consequently in the rate of bone resorption, leading to an increase in the rate of tooth movement during canine retraction (Table 1). Later, in 2004, Kale et al58 compared the effect of the administration of prostaglandin and 1,25-dihydroxy cholecalciferol (1,25 DHCC) on tooth movement. Both were found to increase the amount of tooth movement significantly when compared to controls. An increase in the number of Howship lacunae and capillaries on the pressure side was found in the experimental group. In addition, the number of osteoblasts on the external surface of the alveolar bone was increased following the administration of 1,25 DHCC in comparison to prostaglandin administration. Thus, the authors outlined the role of 1,25 DHCC in facilitating tooth movement through the regulation of bone deposition and the resorption processes (Table 1).58
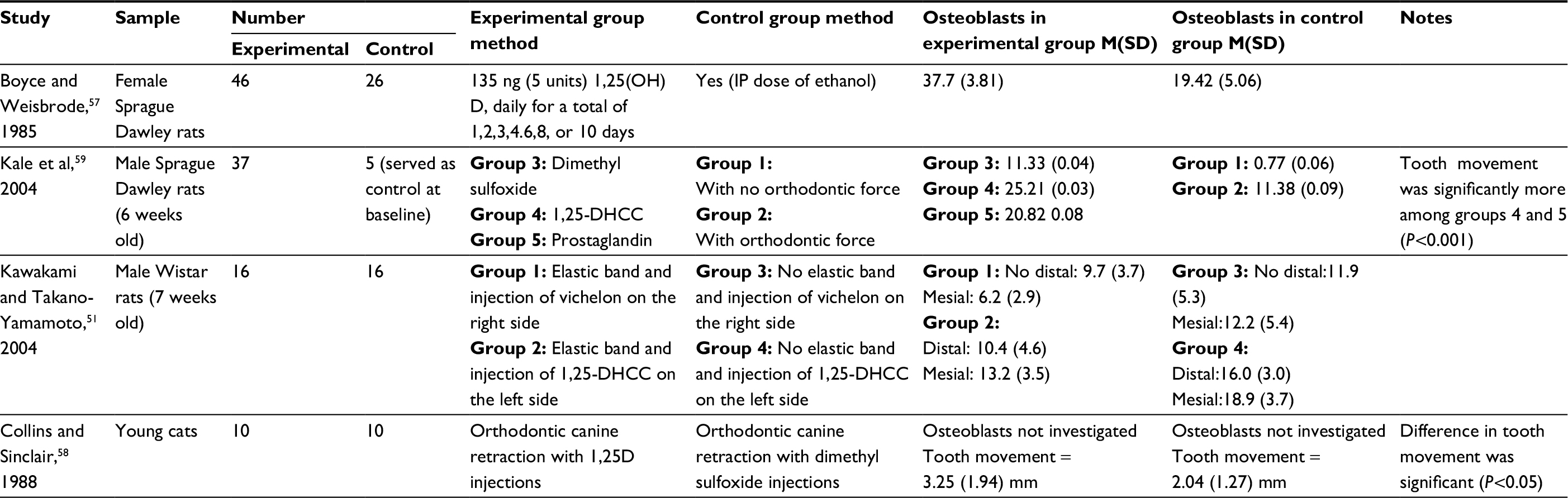 | Table 1 Summaries of the main findings of the studies evaluating the effects of vitamin D and orthodontic movement Abbreviations: 1, 25 DHCC, 1,25-dihydroxy cholecalciferol; M, mean; SD, standard deviation; IP, intraperitoneal; 1,25D, vitamin D metabolites. |
Some investigators have suggested that in addition to faster teeth movement, localized administration of vitamin D enhances tooth position stability. Kawakami and Takano-Yamamoto50 hypothesized that calcitriol may improve bone formation and periodontal tissue remodeling by increasing osteoblastic activity, which in turn would improve the stability of the teeth position after orthodontic movement. In this experiment, the authors divided a sample of 16 Wistar rats into experimental and control groups. In the experimental group, orthodontic elastics were inserted around the upper molars bilaterally. Every 3 days, calcitriol was injected locally and palatally to the upper molars on the right side. In the control group, calcitriol was injected locally but orthodontic elastic was not applied. The researchers found an increase in the mineral appositional rate on alveolar bone after they applied an orthodontic force and injected calcitriol in the submucosal palatal area of the rats, who were subjected to tooth movement. On day 7, researchers reported a significant increase in the number of osteoblasts and osteoclasts at the mesial side of the interradicular septum, and on day 14 an increase in osteoblasts only. In so doing, they showed that calcitriol has a potent effect on bone formation. The authors concluded that the use of calcitriol may promote the reestablishment of tissue supporting the teeth after orthodontic treatment (Table 1).50 Similar findings were shown by Boyce and Weisbrode,56 who found a temporary rise in the rate of bone resorption on the first 2 days followed by a progressive rise in bone formation after 14 days of calcitriol adminstration.50
These laboratory studies suggest that orthodontic patients with vitamin D deficiency may experience a slower rate of tooth movement.50,56,58 There was a substantial initial increase in osteoclastic activity followed by osteoblastic activity. These findings suggest that vitamin D and its metabolites may facilitate orthodontic treatment. Further evidence is needed to determine the safety of vitamin D treatment in orthodontic patients as well as the optimal amount and site of application for this purpose. In addition, given the high prevalence of vitamin D deficiency worldwide,1–3,6,12,13 it is important that researchers explore the clinical application of vitamin D metabolites to enhance the rate of tooth movement during orthodontic therapy.
Conclusion
Approximately 3,000–5,000 IU of vitamin D is required daily for appropriate bone hemostaisis.2 The body should maintain daily levels of vitamin D amounting to at least 30 ng/mL.7,32 This requirement can be attained through sunlight exposure and intake of such dietary products as fatty fish, eggs, and fortified foods.3 A deficiency in vitamin D levels will lead to detrimental effects to the normal mineralization of bone, muscle contraction, and nerve conduction.7,11
In orthodontics, vitamin D deficiency may lead to a slower rate of tooth movement, as evidenced by several laboratory-based investigations.50,56,58 Further exploration is needed to determine the safety of vitamin D treatment in orthodontic patients as well as the optimal amount and site of application for this purpose. In addition, given the high prevalence of vitamin D deficiency worldwide,1–4,6–8 it is important for researchers to investigate the clinical application of these findings, including the potential use of vitamin D metabolites to enhance the rate of tooth movement during orthodontic therapy.
Disclosure
The author reports no conflicts of interest in this work.
References
Holick MF. Vitamin D: A millenium perspective. J Cell Biochem. 2003;88(2):296–307. | ||
Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80 (Suppl 6):1678S–1688S. | ||
Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–281. | ||
Holick MF, Chen TC, Lu Z, Sauter E. Vitamin D and skin physiology: a D-lightful story. J Bone Miner Res. 2007;22 (Suppl 2):V28–V33. | ||
Crowe FL, Steur M, Allen NE, Appleby PN, Travis RC, Key TJ. Plasma concentrations of 25-hydroxyvitamin D in meat eaters, fish eaters, vegetarians and vegans: results from the EPIC–Oxford study. Public Health Nutrition. 2011;14(2):340–346. | ||
Hossein-nezhad A, Holick MF. Optimize dietary intake of vitamin D: an epigenetic perspective. Curr Opin Clin Nutr Metab Care. 2012;15(6):567–579. | ||
Yetley EA, Brulé D, Cheney MC, et al. Dietary reference intakes for vitamin D: justification for a review of the 1997 values. Am J Clin Nutr. 2009;89(3):719–727. | ||
Sniadecki SJJ, Sniadecki J. On the cure of rickets (1840) Cited by W Mozolowski. Nature. 1939;143:121–124. | ||
Holick MF. Resurrection of vitamin D deficiency and rickets. J Clin Invest. 2006;116(8):2062–2072. | ||
Hess AF, Gutman P. The cure of infantile rickets by sunlight as demonstrated by a chemical alteration of the blood. Proc Soc Exp Biol Med. 1921;19(1):31–34. | ||
Samuel HS. Infantile hypercalcaemia, nutritional rickets, and infantile scurvy in great britain. A British Paediatric Association Report. Br Med J. 1964;1(5399):1659–1661. | ||
van Schoor NM, Lips P. Worldwide vitamin D status. Best Pract Res Clin Endocrinol Metab. 2011;25(4):671–680. | ||
Stroud ML, Stilgoe S, Stott VE, Alhabian O, Salman K. Vitamin D - a review. Aust Fam Physician. 2008;37(12):1002–1005. | ||
Alshishtawy MM. Vitamin D deficiency: this clandestine endemic disease is veiled no more. Sultan Qaboos Univ Med J. 2012;12(2):140–152. | ||
Schott GD, Wills MR. Muscle weakness in osteomalacia. Lancet. 1976;1(7960):626–629. | ||
Glerup H, Mikkelsen K, Poulsen L, et al. Hypovitaminosis D myopathy without biochemical signs of osteomalacic bone involvement. Calcif Tissue Int. 2000;66(6):419–424. | ||
Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, et al. Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. Bmj. 2009;339:b3692. | ||
Garland CF, Garland FC. Do sunlight and vitamin D reduce the likelihood of colon cancer? Int J Epidemiol. 1980;9(3):227–231. | ||
Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr. 2006;84(1):18–28. | ||
Grandi NC, Breitling LP, Brenner H. Vitamin D and cardiovascular disease: systematic review and meta-analysis of prospective studies. Prev Med. 2010;51(3–4):228–233. | ||
Vacek JL, Vanga SR, Good M, Lai SM, Lakkireddy D, Howard PA. Vitamin D deficiency and supplementation and relation to cardiovascular health. Am J Cardiol. 2012;109(3):359–363. | ||
Wang TJ, Pencina MJ, Booth SL, et al. Vitamin D deficiency and risk of cardiovascular disease. Circulation. 2008;117(4):503–511. | ||
Anderson JL, May HT, Horne BD, et al. Relation of vitamin D deficiency to cardiovascular risk factors, disease status, and incident events in a general healthcare population. Am J Cardiol. 2010;106(7):963–968. | ||
Wang L, Song Y, Manson JE, et al. Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease: a meta-analysis of prospective studies. Circ Cardiovas Qual Outcomes. 2012;5(6):819–829. | ||
Mitri J, Muraru MD, Pittas AG. Vitamin D and type 2 diabetes: a systematic review. Eur J Clin Nutr. 2011;65(9):1005–1015. | ||
Antico A, Tampoia M, Tozzoli R, Bizzaro N. Can supplementation with vitamin D reduce the risk or modify the course of autoimmune diseases? A systematic review of the literature. Autoimmun Rev. 2012;12(2):127–136. | ||
Ponsonby AL, McMichael A, van der Mei I. Ultraviolet radiation and autoimmune disease: insights from epidemiological research. Toxicology. 2002;181–182:71–78. | ||
Mohr SB, Garland CF, Gorham ED, Garland FC. The association between ultraviolet B irradiance, vitamin D status and incidence rates of type 1 diabetes in 51 regions worldwide. Diabetologia. 2008;51(8):1391–1398. | ||
Vieira VM, Hart JE, Webster TF, et al. Association between residences in U.S. northern latitudes and rheumatoid arthritis: a spatial analysis of the Nurses’ Health Study. Environ Health Perspect. 2010;118(7):957–961. | ||
Sasidharan PK, Rajeev E, Vijayakumari V. Tuberculosis and vitamin D deficiency. J Assoc Physicians India. 2002;50:554–558. | ||
Tsuprykov O, Chen X, Hocher CF, LianghongYin, Hocher B. Why should we measure free 25(OH) vitamin D? J Steroid Biochem Mol Biol. Epub 2017 Dec 5. | ||
Ross AC, Manson JAE, Abrams SA, et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011; 96(1):53–58. | ||
Grant WB, Karras SN, Bischoff-Ferrari HA, et al. Do studies reporting ‘U’-shaped serum 25-hydroxyvitamin D-health outcome relationships reflect adverse effects? Dermatoendocrinol. 2016;8(1):e1187349. | ||
Manson JE, Bassuk SS, Lee IM, et al. The VITamin D and OmegA-3 TriaL (VITAL): rationale and design of a large randomized controlled trial of vitamin D and marine omega-3 fatty acid supplements for the primary prevention of cancer and cardiovascular disease. Contemp Clin Trials. 2012;33(1):159–171. | ||
Smithers G, Gregory JR, Bates CJ, Prentice A, Jackson LV, Wenlock R. The National Diet and Nutrition Survey: young people aged 4–18 years. Nutr Bulletin. 2000;25(2):105–111. | ||
Sullivan SS, Rosen CJ, Halteman WA, Chen TC, Holick MF. Adolescent girls in Maine are at risk for vitamin D insufficiency. J Am Diet Assoc. 2005;105(6):971–974. | ||
Looker AC, Dawson-Hughes B, Calvo MS, Gunter EW, Sahyoun NR. Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. Bone. 2002;30(5):771–777. | ||
Rockell JE, Green TJ, Skeaff CM, et al. Season and ethnicity are determinants of serum 25-hydroxyvitamin D concentrations in New Zealand children aged 5–14 y. J Nutr. 2005;135(11):2602–2608. | ||
El-Hajj Fuleihan G, Nabulsi M, Choucair M, et al. Hypovitaminosis D in healthy schoolchildren. Pediatrics. 2001;107(4):E53. | ||
Al-Daghri NM. Vitamin D in Saudi Arabia: prevalence, distribution and disease associations. J Steroid Biochem Mol Biol. 2018;175:102–107. | ||
Zhang FF, Al Hooti S, Al Zenki S, et al. Vitamin D deficiency is associated with high prevalence of diabetes in Kuwaiti adults: results from a national survey. BMC Public Health. 2016;16:100. | ||
Golbahar J, Al-Saffar N, Altayab Diab D, Al-Othman S, Darwish A, Al-Kafaji G. Predictors of vitamin D deficiency and insufficiency in adult Bahrainis: a cross-sectional study. Public Health Nutr. 2014;17(4):732–738. | ||
Haq A, Svobodova J, Imran S, Stanford C, Razzaque MS. Vitamin D deficiency: a single centre analysis of patients from 136 countries. J Steroid Biochem Mol Biol. 2016;164:209–213. | ||
Gerber LM, Giambrone AE, Al-Ali HM, Verjee MA. Validity of self-reported vitamin D deficiency among midlife Arab women living in Qatar. Am J Hum Biol. 2016;28(2):181–185. | ||
Ardawi MS, Qari MH, Rouzi AA, Maimani AA, Raddadi RM. Vitamin D status in relation to obesity, bone mineral density, bone turnover markers and vitamin D receptor genotypes in healthy Saudi pre- and postmenopausal women. Osteoporos Int. 2011;22(2):463–475. | ||
Ardawi MS, Sibiany AM, Bakhsh TM, Qari MH, Maimani AA. High prevalence of vitamin D deficiency among healthy Saudi Arabian men: relationship to bone mineral density, parathyroid hormone, bone turnover markers, and lifestyle factors. Osteoporos Int. 2012;23(2):675–686. | ||
BinSaeed AA, Torchyan AA, AlOmair BN, et al. Determinants of vitamin D deficiency among undergraduate medical students in Saudi Arabia. Eur J Clin Nutr. 2015;69(10):1151–1155. | ||
Alfawaz H, Tamim H, Alharbi S, Aljaser S, Tamimi W. Vitamin D status among patients visiting a tertiary care center in Riyadh, Saudi Arabia: a retrospective review of 3475 cases. BMC Public Health. 2014;14:159. | ||
Kanan RM, Al Saleh YM, Fakhoury HM, Adham M, Aljaser S, Tamimi W. Year-round vitamin D deficiency among Saudi female out-patients. Public Health Nutr. 2013;16(3):544–548. | ||
Kawakami M, Takano-Yamamoto T. Local injection of 1,25-dihydroxyvitamin D3 enhanced bone formation for tooth stabilization after experimental tooth movement in rats. J Bone Miner Metab. 2004;22(6):541–546. | ||
Martelli FS, Martelli M, Rosati C, Fanti E. Vitamin D: relevance in dental practice. Clin Cases Miner Bone Metab. 2014;11(1):15–19. | ||
Diravidamani K, Sivalingam SK, Agarwal V. Drugs influencing orthodontic tooth movement: an overall review. J Pharm Bioallied Sci. 2012;4 (Suppl 2):S299–S303. | ||
Castillo L, Tanaka Y, DeLuca HF. The mobilization of bone mineral by 1,25-dihydroxyvitamin D3 in hypophosphatemic rats. Endocrinology. 1975;97(4):995–999. | ||
Reynolds JJ, Holick MF, De Luca HF. The role of vitamin D metabolites in bone resorption. Calcif Tissue Res. 1973;12(4):295–301. | ||
Weisbrode SE, Capen CC, Norman AW. Ultrastructural evaluation of the effects of 1,25-dihydroxyvitamin D3 on bone of thyroparathyroidectomized rats fed a low-calcium diet. Am J Pathol. 1978;92(2):459–472. | ||
Boyce RW, Weisbrode SE. Histogenesis of hyperosteoidosis in 1,25(OH)2D3-treated rats fed high levels of dietary calcium. Bone. 1985;6(2):105–112. | ||
Collins MK, Sinclair PM. The local use of vitamin D to increase the rate of orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 1988;94(4):278–284. | ||
Kale S, Kocadereli I, Atilla P, Asan E. Comparison of the effects of 1,25 dihydroxycholecalciferol and prostaglandin E2 on orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2004;125(5):607–614. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.