Back to Journals » Clinical Optometry » Volume 18
Visual Training for Myopia Control: An Independent and Additive Inhibitor of Axial Growth
Authors Meng ZY, Wang H, Wang DD, Yang L, Zhou P ![]()
Received 23 January 2026
Accepted for publication 28 March 2026
Published 9 April 2026 Volume 2026:18 598467
DOI https://doi.org/10.2147/OPTO.S598467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Chris Lievens
Zhao-Yang Meng,1 Hao Wang,2,3 Dan-Dan Wang,4,5 Lin Yang,2,3 Peng Zhou4,5
1Department of Ophthalmology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Ophthalmology, Visionly Plus Eye Hospital, Beijing, People’s Republic of China; 3Department of Ophthalmology, New Vision Eye Hospital, Beijing, People’s Republic of China; 4Department of Ophthalmology, Parkway Hospital, Shanghai, People’s Republic of China; 5Department of Ophthalmology, Parkway Xintiandi Medical Center, Shanghai, People’s Republic of China
Correspondence: Peng Zhou, Department of Ophthalmology, Parkway Xintiandi Medical Center, 138 Huaihai Middle Road, Shanghai, 200001, People’s Republic of China, Email [email protected]
Purpose: To evaluate the efficacy of visual training (VT) in retarding axial elongation in myopic children and to determine its additive clinical value when combined with standard myopia control modalities, including orthokeratology (OK), defocus spectacles (DS), and low-concentration atropine (LCA).
Methods: This is a retrospective, multicenter, self-controlled cohort study. A total of 208 myopic children (mean age 9.73 ± 2.08 years) who underwent a structured visual training program were included. Subjects were stratified into five subgroups based on concurrent treatments: VT monotherapy, VT+DS, VT+OK, VT+DS+LCA, and VT+OK+LCA. Annualized axial elongation rates were calculated for the pre-training (baseline) and post-training intervals. The primary outcome was the reduction in axial elongation rate.
Results: The mean axial elongation rate significantly attenuated from a baseline of 0.38 ± 0.34 mm/year to 0.23 ± 0.30 mm/year following the intervention (P < 0.001), representing a mean reduction of 0.15 ± 0.31 mm/year. There were no statistically significant differences in the magnitude of rate reduction among the five subgroups (P = 0.826), indicating that VT confers a consistent additive benefit independent of concurrent optical or pharmacological therapies. Pearson correlation analysis revealed a good positive association between baseline progression rate and treatment efficacy (r = 0.57, P < 0.001), suggesting that children with faster initial progression derived the greatest therapeutic benefit.
Conclusion: Visual training effectively slows axial elongation, shifting pathological growth trajectories toward physiological norms. It functions as a universal adjunctive therapy, providing robust and independent protective effects regardless of whether the patient is using OK lenses, defocus spectacles, or atropine. These findings support the use of visual training as a priority “rescue therapy” for rapid progressors.
Keywords: myopia, visual training, axial elongation, binocular vision, adjunctive therapy
Introduction
Myopia has emerged as a significant global public health concern, with its prevalence rising at an alarming rate. It is projected that by 2050, nearly half of the world’s population will be myopic, with approximately 10% suffering from high myopia.1 The primary pathological concern associated with myopia is excessive axial elongation, which dramatically increases the risk of vision-threatening complications such as myopic maculopathy, retinal detachment, and glaucoma.2–5 Consequently, slowing axial elongation has become the cornerstone of modern pediatric myopia management.
Currently, the mainstream interventions for myopia control include optical strategies—such as orthokeratology (OK) lenses and peripheral defocus spectacles, and pharmacological agents like low-concentration atropine.6–8 While these modalities have demonstrated efficacy, a subset of children, often termed “rapid progressors”, continues to exhibit substantial axial elongation despite adherence to these treatments.9 This variability in treatment response suggests that current optical and pharmacological approaches may not address all underlying mechanisms driving myopia progression.
Emerging evidence suggests that binocular vision anomalies, such as accommodation lag, high AC/A ratio, and vergence dysfunction, may play a pivotal role in the onset and progression of myopia.10–29,303 The “retinal defocus theory” posits that hyperopic defocus drives axial growth; however, unstable accommodation or poor oculomotor control can induce transient retinal blur, potentially confounding the protective effects of optical devices.11 Visual training (VT), a structured program designed to improve neuromuscular control and sensory fusion, has been widely used to treat strabismus and amblyopia. Recently, interest has grown regarding its potential as an adjunctive therapy for myopia control.12 By normalizing accommodation dynamics and vergence flexibility, VT aims to optimize retinal image quality and reduce visual stress.
Despite the theoretical rationale, clinical evidence quantifying the effect of visual training on axial elongation—particularly in combination with established myopia control methods—remains sparse. Most existing studies focus on changes in refractive error or accommodative parameters rather than axial length, the gold standard metric for progression.12,13 Furthermore, it remains unclear whether visual training offers additional benefits when added to standard treatments like OK lenses or atropine.
To address this gap, this retrospective cohort study evaluated the efficacy of a structured visual training program in retarding axial elongation among myopic children. Specifically, we aimed to quantify the reduction in axial growth rate following VT intervention; assess whether VT provides an additive benefit across different concurrent treatment modalities (OK lenses, defocus spectacles, and atropine); and identify patient characteristics that predict the most significant therapeutic response.
Materials and Methods
Study Design and Ethical Approval
This retrospective observational study was conducted at two clinical centers: Beijing Visionly Plus Eye Hospital and Beijing New Vision Eye Hospital (Beijing, China). The study adhered to the ethical standards laid out by the Declaration of Helsinki. Ethical clearance was obtained from the Beijing New Vision Eye Hospital’s Ethics Committee and Institutional Review Board (IRB) (approval no. 2025005). Due to its retrospective nature utilizing anonymous data, the study was granted a waiver of informed consent by the IRB. All patient data were de-identified prior to statistical analysis. The data collection period encompassed patients undergoing visual training for myopia control between Jan 1, 2024, and Jan 1, 2025.
Participants and Selection Criteria
A total of 208 myopic children (208 eyes) were included in the final analysis. Inclusion criteria were as follows: (1) age between 5 and 15 years at the commencement of training; (2) diagnosis of myopia with a spherical equivalent (SE) refraction ≤ −0.50 D; (3) completion of a structured visual training program (attending at least 80% of the scheduled in-office sessions and demonstrating adherence to the prescribed home-based exercises); (4) availability of complete axial length (AL) data at three critical time points: at least two examinations prior to training (to establish baseline progression rate) and at least one examination following the training intervention. Exclusion criteria included: (1) presence of other ocular pathologies (eg., amblyopia, strabismus, congenital cataract); (2) history of ocular surgery or trauma; (3) systemic diseases affecting ocular health; (4) any corneal or ocular surface pathology; or (5) incomplete or inconsistent follow-up records preventing the calculation of annualized progression rates. To avoid potential bias arising from the correlation between eyes, only the right eye was selected for analysis.
Myopia Control Modalities and Grouping
To evaluate the independent and adjunctive effects of visual training, subjects were categorized into five subgroups based on their concurrent myopia control modalities utilized during the observation period: (1) Visual Training Monotherapy: Subjects receiving visual training only, with single-vision spectacles (SVS) or no optical correction. (2) Defocus Spectacles: Subjects wearing peripheral defocus management spectacles (eg., DIMS, HAL technology). (3) Defocus Spectacles + Atropine: Combination of defocus spectacles and low-concentration atropine (0.01%). (4) Orthokeratology (OK) Lens: Subjects wearing overnight orthokeratology lenses. (5) OK Lens + Atropine: Combination of OK lenses and low-concentration atropine.
Visual Training Protocol
The visual training intervention targeted binocular vision anomalies, including accommodation and vergence dysfunctions. The regimen consisted of in-office training sessions supplemented by home-based exercises. The core modules included: (1) Static Ocular Alignment: Exercises designed to maintain stable fixation and alignment. (2) Dynamic Ocular Alignment: Tasks focused on accurate saccadic and pursuit eye movements to improve dynamic gaze control. (3) Fusional Convergence: Training aimed at strengthening positive fusional vergence (PFV) reserves. (4) Dynamic Stereopsis: Activities requiring depth perception judgments of moving stimuli. (5) Coarse (Large-range) Stereopsis: Stimulation using large-disparity targets to engage global stereoscopic processing (Table 1).
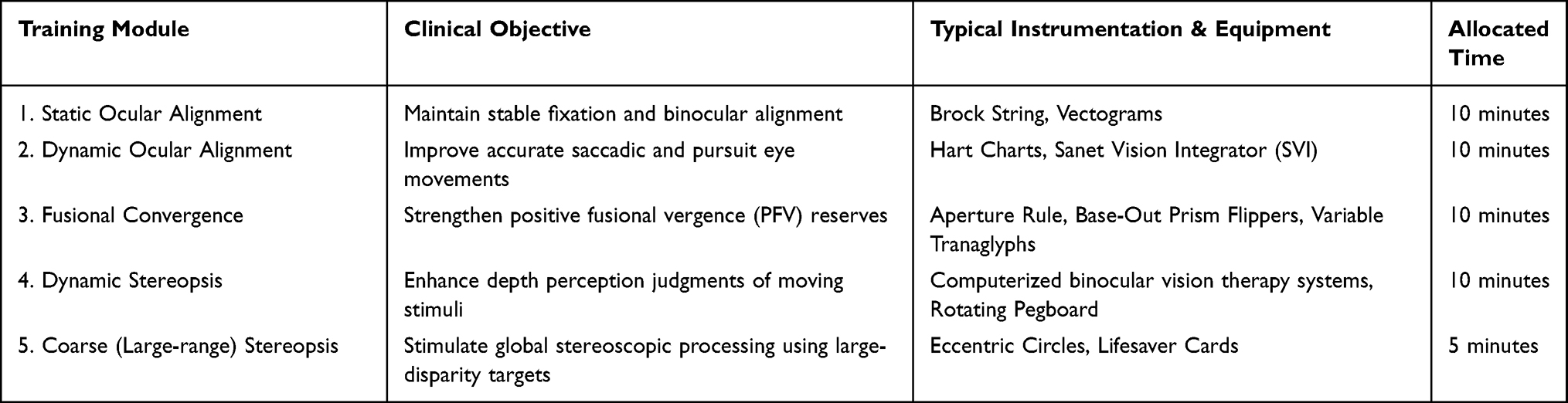 |
Table 1 Visual Training Protocol |
Data Collection and Outcome Measures
The primary outcome measure was the rate of Axial Length (AL) elongation. AL was measured using partial coherence interferometry (IOLMaster 700, Carl Zeiss Meditec, Germany). The Annualized Axial Elongation Rate (mm/year) was calculated for two distinct periods: Pre-training Rate: Calculated based on the AL change over the period immediately preceding the start of visual training. Post-training Rate: Calculated based on the AL change from the start of training to the last follow-up visit. The efficacy of the intervention was quantified as the Reduction in Elongation Rate =Pre-training Rate - \ Post-training Rate. A positive value indicates a slowing of myopia progression (therapeutic benefit).
Statistical Analysis
Although training was binocular, only data from the right eye were analyzed to ensure independence. Statistical analyses were performed using Python (incorporating the SciPy and Pandas libraries). Descriptive statistics were presented as mean ± standard deviation (SD) for continuous variables and frequency (percentage) for categorical variables. The normality of data distribution was assessed using the Shapiro–Wilk test. Since the differences in axial elongation rates followed a non-normal distribution: The Wilcoxon Signed-Rank Test was used to compare paired data (Pre-training vs. Post-training rates) for the entire cohort. The Kruskal–Wallis H-Test was employed to compare the magnitude of rate reduction across the five different treatment subgroups. Pearson Correlation Analysis was conducted to examine the relationship between baseline progression rate and the magnitude of reduction. A two-tailed P-value of <0.05 was considered statistically significant.
Results
Patient Demographics and Baseline Characteristics
A total of 208 subjects (208 eyes) were included in this retrospective analysis. The study cohort had a mean age of 9.73 ± 2.08 years (range: 5 to 15 years) at the commencement of visual training. The baseline mean spherical equivalent (SE) refraction of the right eye was −1.83 ± 1.61 D (range: −8.13 to +1.75 D), and the mean baseline axial length (AL) was 24.23 ± 0.99 mm.
The subjects were categorized into five subgroups based on their concurrent myopia control modalities: Defocus Spectacles (n=68, 32.7%), Orthokeratology (OK) Lenses (n=58, 27.9%), Visual Training Monotherapy (n=33, 15.9%), OK Lenses combined with Low-Concentration Atropine (n=26, 12.5%), and Defocus Spectacles combined with Low-Concentration Atropine (n=23, 11.1%). The detailed baseline characteristics are summarized in Table 2. Prior to the intervention, all included subjects exhibited binocular vision anomalies—predominantly accommodative lag and reduced positive fusional vergence—which served as the clinical indication for the visual training.
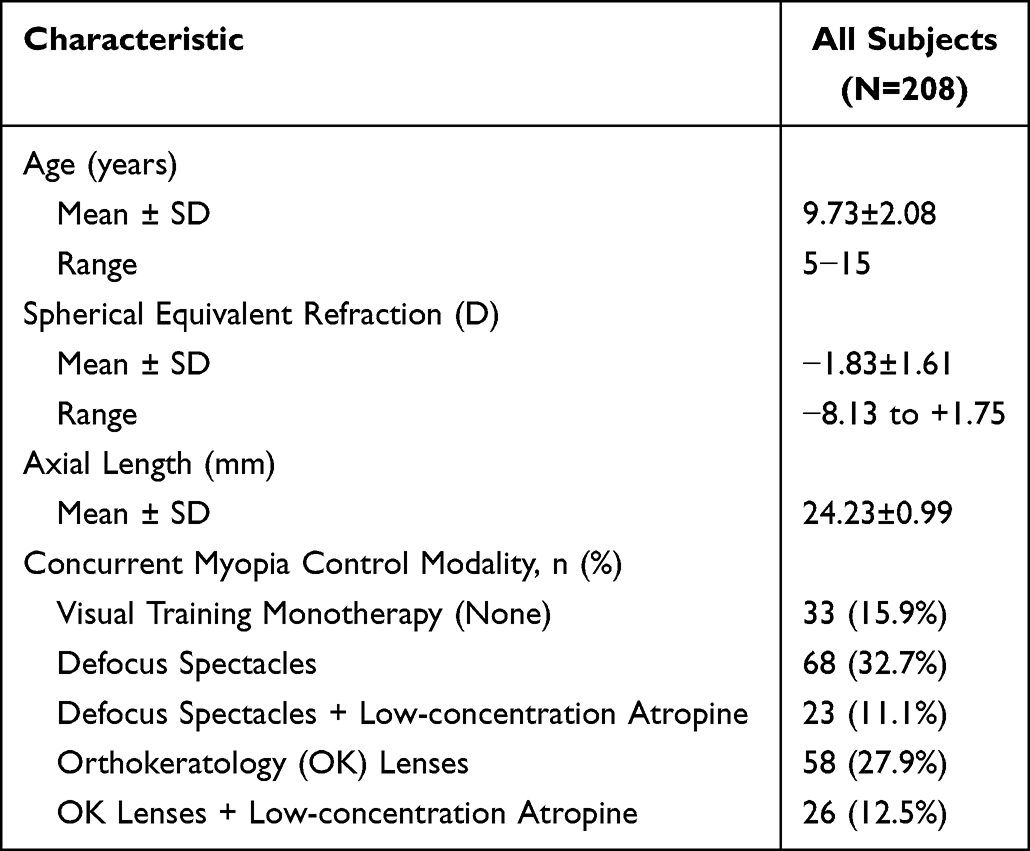 |
Table 2 Baseline Characteristics of the Study Population |
Overall Efficacy of Visual Training in Retarding Axial Elongation
A longitudinal self-controlled analysis was conducted on 208 subjects to evaluate the efficacy of visual training in controlling axial length (AL) elongation. Prior to the intervention, the cohort exhibited a rapid phase of myopia progression, characterized by a mean right eye axial elongation rate of 0.38 ± 0.34 mm/year. Following the visual training intervention, the mean axial elongation rate significantly decreased to 0.23 ± 0.30 mm/year (Figure 1A). A Wilcoxon signed-rank test demonstrated that this reduction was statistically significant (Z = 16,935.0, P < 0.001). The intervention resulted in a mean reduction in axial growth speed of 0.15 ± 0.31 mm/year (Figure 1B), effectively decelerating the pathological elongation rate to a level approaching physiological eye growth (typically 0.1–0.2 mm/year). Effect size analysis yielded a Cohen’s d of approximately 0.48, indicating a moderate clinical effect. These findings provide robust evidence that visual training serves as a potent independent intervention capable of significantly altering the natural history of myopia progression.
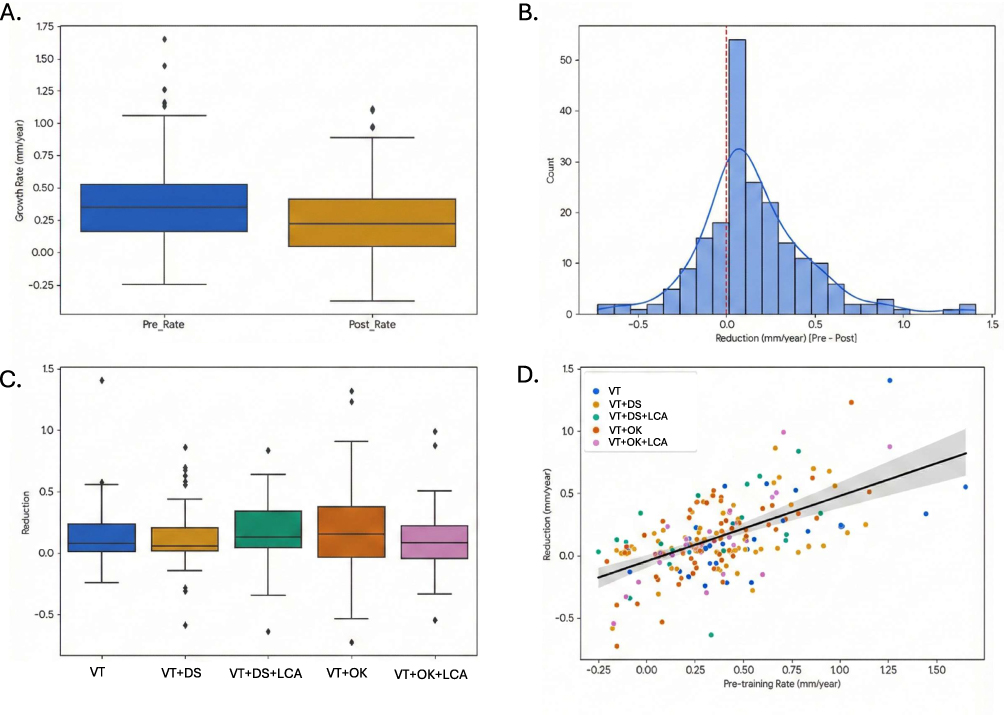 |
Figure 1 Efficacy of visual training on retarding axial elongation in myopic children. (A) Paired boxplot comparison of annualized axial elongation rates before (Pre) and after (Post) the visual training intervention. The intervention resulted in a significant reduction in the median axial growth rate. The central lines represent medians, box edges denote the interquartile range (IQR), and whiskers extend to 1.5×IQR. (B) Histogram showing the distribution of the reduction in axial elongation rate (defined as Pre-rate minus Post-rate). The red dashed line marks zero change; the right-skewed distribution indicates that the majority of subjects experienced a positive reduction (slowing) of axial growth. (C) Boxplot comparing the therapeutic effect (reduction in elongation rate) across five subgroups stratified by concurrent myopia control modalities. The Kruskal–Wallis test revealed no statistically significant differences among the groups (P = 0.826), suggesting a consistent additive benefit of visual training regardless of the combined therapy. (D) Scatter plot with a linear regression line illustrating the relationship between the baseline pre-training axial elongation rate (x-axis) and the magnitude of rate reduction (y-axis). A significant positive correlation (Pearson’s r = 0.57, P < 0.001) indicates that subjects with faster initial progression derived greater therapeutic benefit from visual training. Abbreviations: VT, visual training; DS, Defocus Spectacles; LCA, Low-concentration Atropine; OK, Orthokeratology. |
Universality and Independence of Visual Training as an Adjunctive Therapy
To determine whether the efficacy of visual training is dependent on concurrent optical or pharmacological treatments, subjects were stratified into five subgroups based on their combined myopia control modalities (Table 3, Figure 1C): Orthokeratology (OK) lenses, Defocus Spectacles (DS), OK lenses + Atropine, DS + Atropine, and Visual Training monotherapy (None). A Kruskal–Wallis H-test revealed no statistically significant difference in the magnitude reduction of AL rate among the groups (P = 0.826). Specifically, subjects receiving visual training monotherapy achieved a mean reduction of 0.16 mm/year, which was highly comparable to the reductions observed in the OK lens group (0.18 mm/year) and the DS + Atropine group (0.18 mm/year). This lack of significant inter-group difference underscores the “additive effect” of visual training. Regardless of whether a patient is currently managing myopia with orthokeratology or low-concentration atropine, the addition of visual training provides a consistent and independent benefit of approximately 0.15 mm/year. This suggests that visual training has broad clinical indications and can be effectively integrated as a universal adjunctive therapy into existing myopia management protocols.
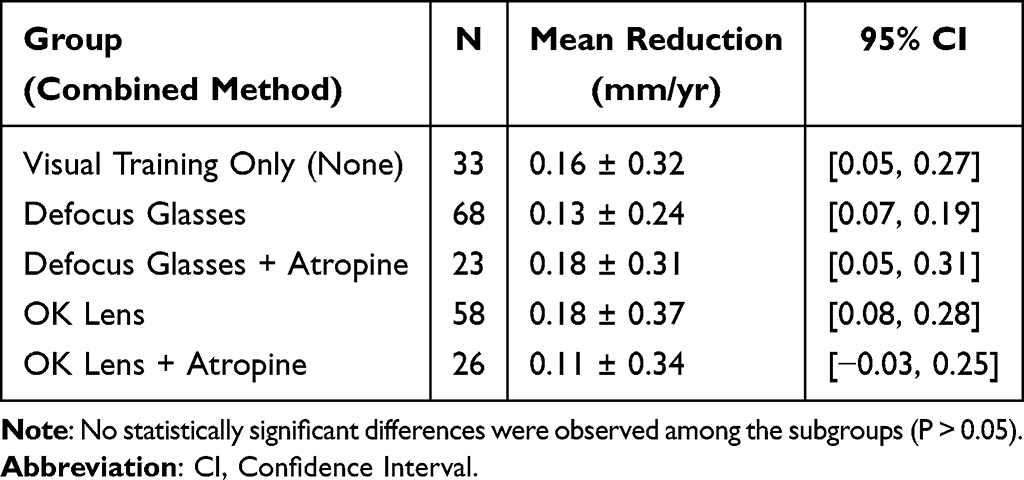 |
Table 3 Subgroup Analysis of Axial Growth Reduction by Combined Treatment Method |
Identification of Optimal Candidates and Precision Intervention Strategies Based on Baseline Progression
Correlation analysis between baseline axial elongation rates and the magnitude of post-training reduction was performed to identify the population that benefits most from this intervention (Figure 1D). Pearson correlation analysis indicated a significant positive correlation (r = 0.57, P < 0.001), suggesting that children whose eyes were elongating at a faster rate (mm/year) prior to the intervention experienced the larger drop in their growth rate after the intervention. Scatter plot analysis further elucidated that for “rapid progressors”—children exhibiting explosive axial growth (eg., >0.5 mm/year) despite conventional control measures—visual training exerted a dramatic inhibitory effect, substantially curtailing the rate of elongation. Conversely, while children with slower baseline growth also benefited, the magnitude of reduction was more moderate. These findings provide a critical basis for clinical decision-making: for refractory cases where myopia continues to progress rapidly despite standard treatments, visual training should be prioritized as a “rescue therapy.” Its significant “peak-shaving” effect on axial growth velocity is crucial for preventing the transition of these high-risk individuals into high myopia.
Discussion
The present study provides compelling retrospective evidence regarding the efficacy of visual training (VT) as a potent intervention for myopia control. Our findings demonstrate that a structured VT program significantly reduced the mean annualized axial elongation rate from a rapid, pathological trajectory (0.38 mm/year) to a level approaching physiological emmetropic growth (0.23 mm/year). This reduction of approximately 0.15 mm/year is clinically meaningful, comparable to the treatment effects reported for 0.01% low-concentration atropine or defocus-incorporated spectacles in recent landmark trials. To our knowledge, this is one of the first studies to quantify the “additive” efficacy of visual training across a spectrum of concurrent myopia control modalities based on axial length—the gold standard metric for progression.
The mechanism by which visual training retards axial elongation is likely multifactorial, centering on the amelioration of binocular vision anomalies that drive myopigenesis. High accommodative lag and unstable accommodation have been implicated in producing hyperopic retinal defocus, a potent stimulus for axial growth.14–18 Furthermore, vergence dysfunction can induce transient visual blur and visual fatigue.19–21 We postulate that the VT protocol employed in this study, which emphasized improving accommodative facility and fusion reserves, effectively reduced accommodative lag and stabilized retinal image quality. By refining the oculomotor control system, VT may minimize the cumulative duration of retinal blur during near work, thereby downregulating the scleral signaling pathways responsible for elongation.
A pivotal finding of this study is the uniformity of therapeutic benefit across diverse subgroups. We observed no statistically significant difference in the magnitude of axial slowing between children using VT alone, VT with orthokeratology, or VT with atropine. This suggests that the therapeutic pathway of visual training is distinct from and complementary to optical and pharmacological mechanisms. While orthokeratology and defocus spectacles operate primarily by imposing peripheral myopic defocus,22,23 and atropine acts via muscarinic receptor pathways,24–26 visual training targets the neuromuscular and sensory processing aspects of vision.12 Consequently, VT acts as a universal “booster”, providing an additive effect regardless of the primary control modality. This finding supports the integration of VT as a standard adjunctive therapy in multimodal myopia management protocols.
Our correlation analysis revealed a good positive relationship between baseline progression rate and the magnitude of treatment effect. Children with the most rapid initial axial growth experienced the most dramatic deceleration. While this observation may partially reflect the statistical phenomenon of regression to the mean, the magnitude of the effect suggests a genuine biological response.27 Clinically, this identifies a clear target demographic, the non-responders to standard care. For children whose myopia continues to spiral despite optimal optical or pharmacological intervention, visual training may serve as a critical rescue therapy to brake the acceleration phase of axial elongation.
Several limitations of this study warrant consideration. First, the retrospective nature and the absence of a concurrent control group receiving no intervention (or a “sham” training group) limit our ability to strictly infer causality, although the self-controlled design mitigates inter-subject variability. Second, the follow-up duration was variable; while annualized rates were used for standardization, longer-term studies are needed to assess the sustainability of the training effect after cessation. Furthermore, detailed binocular function parameters (eg., AC/A ratio changes) were not analyzed in this specific report, which limits our ability to directly correlate functional improvements with structural changes. Finally, near-work duration and exposure to visual display units (VDUs) were not systematically quantified, which could introduce confounding variables.
Conclusion
In conclusion, visual training serves as an effective, safe, and universally applicable strategy for slowing axial elongation in myopic children. It offers a significant additive benefit when combined with existing treatments like orthokeratology and atropine, and demonstrates particular efficacy in children with rapid baseline progression. These findings advocate for a paradigm shift in myopia management—moving from a purely optical/pharmacological approach to a holistic model that includes functional visual rehabilitation.
Data Accessibility
Data associated with this paper can be requested from the corresponding author.
Ethics Guidelines
Ethical clearance was obtained from the Beijing New Vision Eye Hospital’s Ethics Committee and Institutional Review Board (IRB) (approval no. 2025005).
Consent to Publish
All authors confirm their consent for the publication of this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was self-funded and received no outside grants.
Disclosure
The authors declare no relevant financial or non-financial interests in this work.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123:1036–8. doi:10.1016/j.ophtha.2016.01.006
2. Haarman AEG, Enthoven CA, Tideman JWL, et al. The complications of myopia: a review and meta-analysis. Invest Ophthalmol Vis Sci. 2020;61:49. doi:10.1167/iovs.61.4.49
3. Arrigo A, Aragona E, Bianco L, et al. The clinical role of the choroidal assessment in high myopia: characteristics and association with neovascular and atrophic complications. Invest Ophthalmol Vis Sci. 2023;64(16):16. doi:10.1167/iovs.64.12.16
4. Iwase A, Araie M. Implications of myopia in diagnosis and screening of open angle glaucoma. Curr Opin Ophthalmol. 2025;36(2):107–114. doi:10.1097/ICU.0000000000001116
5. Wang -D-D, Zhou P. Myopia: pathogenesis and intervention. Nat Cell and Sci. 2025;3:62–76. doi:10.61474/ncs.2024.00049
6. Chen M, Lei H, Yang X, et al. Comparative efficacy of optical correction methods combined with 0.01% atropine in myopia control. BMC Ophthalmol. 2025;25:703. doi:10.1186/s12886-025-04523-9
7. Zhu J, Yang Z, Sun D, et al. Association between pupil area and the efficacy of peripheral defocus spectacle lenses in myopia control. Transl Vis Sci Technol. 2026;15:9. doi:10.1167/tvst.15.1.9
8. Liu J, Lu Y, Huang D, et al. The efficacy of defocus incorporated multiple segments lenses in slowing myopia progression: results from diverse clinical circumstances. Ophthalmology. 2023;130:542–550. doi:10.1016/j.ophtha.2023.01.007
9. Cho P, Cheung SW, Boost MV. Categorisation of myopia progression by change in refractive error and axial elongation and their impact on benefit of myopia control using orthokeratology. PLoS One. 2020;15:e0243416. doi:10.1371/journal.pone.0243416
10. Logan NS, Radhakrishnan H, Cruickshank FE, et al. IMI accommodation and binocular vision in myopia development and progression. Invest Ophthalmol Vis Sci. 2021;62:4. doi:10.1167/iovs.62.5.4
11. Erdinest N, London N, Lavy I, et al. Peripheral defocus and myopia management: a mini-review. Korean J Ophthalmol. 2023;37:70–81. doi:10.3341/kjo.2022.0125
12. Xu Z, Zou A, Li L, et al. Effect of virtual reality-based visual training for myopia control in children: a randomized controlled trial. BMC Ophthalmol. 2024;24:358. doi:10.1186/s12886-024-03580-w
13. Vasudevan B, Ciuffreda KJ, Ludlam DP. Accommodative training to reduce nearwork-induced transient myopia. Optom Vis Sci. 2009;86:1287–1294. doi:10.1097/OPX.0b013e3181bb44cf
14. Thakur S, Verkicharla PK. Greater axial elongation associated with low accommodative lag: new insights on accommodative lag theory for myopia. Ophthalmic Physiol Opt. 2021;41(6):1355–1362. doi:10.1111/opo.12893
15. Chaurasiya RK, Gupta A. Greater axial elongation associated with low accommodative lag: new insights on accommodative lag theory for myopia. Ophthalmic Physiol Opt. 2023;43(2):284. doi:10.1111/opo.13081
16. Berntsen DA, Sinnott LT, Mutti DO, Zadnik K. Accommodative lag and juvenile-onset myopia progression in children wearing refractive correction. Vision Res. 2011;51(9):1039–1046. doi:10.1016/j.visres.2011.02.016
17. Meng Z-Y, Yang L, Zhou P, Fogt N. Analysis of axial shortening induced by orthokeratology lenses and its mechanical mechanisms. PLoS One. 2025;20(5):e0323546. doi:10.1371/journal.pone.0323546
18. Meng Z-Y, Yang L, Zhou P, Bhattacharya S. Ciliary muscles contraction leads to axial length extension——The possible initiating factor for myopia. PLoS One. 2024;19(4):e0301844. doi:10.1371/journal.pone.0301844
19. Zhao S, Hao J, Liu J, Cao K, Fu J. Fusional vergence dysfunctions in acute acquired concomitant esotropia of adulthood with myopia. Ophthalmic Res. 2023;66(1):320–327. doi:10.1159/000527884
20. Chen AM, Roberts TL, Cotter SA, et al. Effectiveness of vergence/accommodative therapy for accommodative dysfunction in children with convergence insufficiency. Ophthalmic Physiol Opt. 2021;41:21–32. doi:10.1111/opo.12747
21. Sreenivasan V, Irving EL, Bobier WR. Effect of heterophoria type and myopia on accommodative and vergence responses during sustained near activity in children. Vision Res. 2012;57:9–17. doi:10.1016/j.visres.2012.01.011
22. Xu W, Li X, Zhang J, et al. The peripheral defocus designed spectacle lenses might increase astigmatism in myopic children. Transl Vis Sci Technol. 2025;14:8. doi:10.1167/tvst.14.3.8
23. Erdinest N, London N, Lavy I, et al. Peripheral defocus as it relates to myopia progression: a mini-review. Taiwan J Ophthalmol. 2023;13:285–292. doi:10.4103/tjo.TJO-D-22-00100
24. Upadhyay A, Beuerman RW. Biological mechanisms of atropine control of myopia. Eye Contact Lens. 2020;46:129–135. doi:10.1097/ICL.0000000000000677
25. Zhou P, Wang -D-D, Fan L, Yang L, Zhao M-W, Gatzioufas Z. Thin central corneal thickness may be a risk factor for myopia progression in children. J Ophthalmol. 2023;2023(1):3815863. doi:10.1155/2023/3815863
26. Zhou P, Wang D. Comparing the efficacy of low-dose atropine eye drops, orthokeratology, and combined treatment for myopia progression control. Nat Cell Sci. 2025;3:1–6. doi:10.61474/ncs.2024.00048
27. Yam JC, Zhang XJ, Zaabaar E, et al. Interventions to reduce incidence and progression of myopia in children and adults. Prog Retin Eye Res. 2025;109(101410). doi:10.1016/j.preteyeres.2025.101410
28. Kaphle D, Varnas SR, Schmid KL, et al. Accommodation lags are higher in myopia than in emmetropia: measurement methods and metrics matter. Ophthalmic Physiol Opt. 2022;42:1103–1114. doi:10.1111/opo.13021
29. Mutti DO, Mitchell GL, Jones-Jordan LA, et al. The response AC/A ratio before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2017;58:1594–1602. doi:10.1167/iovs.16-19093
30. Ma J, Yang X, Liu Z, et al. The impact of vergence dysfunction on myopia control in children wearing defocus spectacle lenses. Clin Ophthalmol. 2024;18:799–807. doi:10.2147/OPTH.S453731
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.