Back to Journals » Clinical Ophthalmology » Volume 19
Visual Performance and Subjective Outcomes with Enhanced Monofocal Intraocular Lens Implantation Targeted for Emmetropia or Modest Monovision
Authors Yeo TK ![]() , Pek DCK, Wong JXH
, Pek DCK, Wong JXH
Received 11 April 2025
Accepted for publication 3 August 2025
Published 20 August 2025 Volume 2025:19 Pages 2847—2857
DOI https://doi.org/10.2147/OPTH.S533814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Tun Kuan Yeo, Don Chern Kuok Pek, John Xin Hao Wong
Department of Ophthalmology, Tan Tock Seng Hospital, Singapore
Correspondence: Tun Kuan Yeo, Department of Ophthalmology, Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, 308433, Singapore, Email [email protected]
Purpose: To determine the visual performance and patient reported outcomes after bilateral implantation of an enhanced monofocal intraocular lens (IOL) (RayOne EMV RAO200E) targeted for emmetropia or modest monovision.
Patients and Methods: This was a prospective, single-centre, comparative, interventional study. Patients were divided into two groups and targeted for bilateral emmetropia or modest monovision (− 1.50 D in the near eye). Manifest refraction, monocular uncorrected and corrected distance visual acuity (UDVA and CDVA), uncorrected and distance-corrected intermediate visual acuity (UIVA and DCIVA), uncorrected and distance-corrected near visual acuity (UNVA and DCNVA), and monocular and binocular defocus curves under photopic and mesopic conditions were measured at 1-month post-surgery. The Catquest 9-SF questionnaire was administered to assess patient reported visual outcomes and quality of life.
Results: 60 patients were enrolled. For the emmetropia group (n = 30), the mean logMAR UDVA, UIVA and UNVA were 0.16± 0.13, 0.35± 0.12 and 0.50± 0.15. In the monovision group (n = 30), the values for the distance eyes were 0.13± 0.11, 0.40± 0.11 and 0.56± 0.13; and for the near eyes 0.41± 0.21, 0.27± 0.16 and 0.34± 0.13. Binocular defocus curves showed similar distance visual acuity but better visual acuity in the monovision group from – 1.00 D to – 4.00 D and − 1.00 D to – 3.50 D defocus under photopic and mesopic conditions respectively (p < 0.05). The defocus range (logMAR 0.2 or better) was 1.3 D for the bilateral emmetropia group and 2.5 D for the monovision group. 90% (emmetropia group) and 96% (monovision group) of patients were very or fairly satisfied with their vision, with the monovision group reporting better performance for intermediate and near tasks.
Conclusion: Patients targeted for bilateral emmetropia achieved good functional intermediate vision, while those with modest monovision experienced enhanced intermediate and near vision. Overall, patients reported high satisfaction and good visual performance when implanted with the enhanced monofocal IOL.
Keywords: enhanced monofocal, bilateral emmetropia, modest monovision
Introduction
There is an increasing demand for spectacle independent vision at different distances after cataract surgery. Intraocular lenses (IOLs) based on different optical designs have been widely used by cataract surgeons to provide patients with good visual acuity at far, intermediate and near distances. An analysis comparing the outcomes of presbyopia-correcting IOLs concluded that for patients considering a multifocal IOL, a bilateral implantation of a trifocal lens might be an optimal option for them without compromising distant visual acuity.1 However, although trifocal IOLs have been reported to be more effective in improving the whole range of unaided vision, they were associated with a higher rate of photic phenomena.2,3 IOLs based on enhanced depth-of-focus technology combined with mini-monovision alternatively provide partial spectacle independence with less photic phenomena than trifocal IOLs.3
Enhanced monofocal IOLs are another category of IOLs that provide some spectacle independence at intermediate distances without significant photic phenomena. A recent meta-analysis, carried out on 3 randomised controlled trials and 9 comparative studies, comparing the outcomes of an enhanced monofocal IOL versus a monofocal IOL, has concluded that enhanced monofocal IOLs effectively improved unaided intermediate vision with similar distance performance compared to monofocal IOLs, without inducing photic phenomena.4
Laboratory optical bench tests5–9 and clinical studies have also shown that bilateral implantation targeted for emmetropia is safe and effective, providing excellent distance and good intermediate vision with a high level of patient satisfaction.10,11 Some surgeons, in order to increase the useful range of vision, have used enhanced monofocal IOLs via a monovision approach.12–14 This has been found to increase intermediate and near vision without affecting subjective visual quality, low contrast distance visual acuity, or patient satisfaction,13 with superiority in intermediate and near vision compared to patients targeted for bilateral emmetropia.12,14 There are different types of monovision strategies: 1) full monovision, 2) modest monovision, 3) mini-monovision and micro-monovision. Full monovision (near target of −2 D to −2.5 D) is rarely performed nowadays due to significant reduction in stereopsis.15 Modest monovision (near target of −1 D to −1.5 D) is much more common, while mini-monovision and micro-monovision (near target of −0.50 D to −0.75 D) are usually used with extended depth of focus (EDOF) IOLs.
To the best of our knowledge, there are no studies that assessed the outcomes of the RayOne EMV enhanced monofocal IOL (Rayner Intraocular Lenses Limited, Worthing, UK) with and without a modest monovision approach with a near target of −1.5 D. −1.5 D was chosen as it is commonly used target locally, since it has been reported to improve near vision without a significant drop in stereoacuity.15 Therefore, the purpose of the study was to assess the visual performance and patient reported subjective outcomes after bilateral implantation of the IOL when targeted for bilateral emmetropia or modest monovision.
Materials and Methods
Study Design and Patients
This was a prospective interventional comparative study carried out at the Department of Ophthalmology, Tan Tock Seng Hospital, Singapore between 1st December 2021 and 31st March 2023. The study was approved by the National Healthcare Group Institutional Review Board of Singapore (2021/00925) and followed the principles of the Declaration of Helsinki. All patients were given a detailed explanation of the study and provided written informed consent to undergo cataract surgery and tests with inclusion of their data for research purposes.
Patients were included if they had bilateral visually significant cataracts requiring surgery, aged ≥ 21 years to 90 years old, with an expected best corrected visual acuity of 6/9 or better after cataract surgery, calculated IOL power within range of +10 D to +30 D, corneal astigmatism of ≤ 1.50 D, and were willing to undergo additional investigations (pupillometry, defocus measurements and questionnaire). Screening of corneal astigmatism was performed with the Nidek ARK-1 (Nidek Co. Ltd., Gamagori, Japan). Exclusion criteria included history of ocular trauma, prior incisional or laser refractive surgery or intraocular surgery, irregular corneal astigmatism, corneal decompensation or endothelial insufficiency (cell count < 1500/mm2), pseudoexfoliation, zonulopathy, Adie’s pupil or tonic pupil, glaucoma, strabismus, amblyopia, vitreoretinal or macular diseases (eg exudative age-related macular degeneration, diabetic macular oedema, proliferative diabetic retinopathy), neuro-ophthalmic diseases (eg optic neuropathy), or a history of uveitis.
The patients were divided into two groups: a bilateral emmetropia group and a modest monovision group. Patients in the first group had target refraction of emmetropia for both eyes, while the latter group had target refraction of emmetropia for the first eye and −1.50 D for the second eye. The eye which had worse visual acuity was operated first. The patients were enrolled into each group based on their expressed visual needs after surgery.
Preoperative Assessment, Surgery and IOL
All patients underwent routine preoperative clinical examination and biometric measurements (axial length, keratometry, anterior chamber depth, lens thickness, central corneal thickness and white-to-white) using the IOLMaster 700 biometer (Carl Zeiss Meditec AG, Jena, Germany). The Barrett Universal II formula was used to calculate the required IOL power. Surgery was performed using a standard phacoemulsification technique by 3 experienced surgeons (TKY, DCKP, JXHW) under topical anaesthesia with a 2.2 mm clear corneal incision. All patients were implanted with the enhanced monofocal IOL, RayOne EMV RAO200E. The IOL is based on a non-diffractive aspheric design to provide an extended range of vision by inducing a small amount of positive spherical aberration on the central region of the lens and reduced longitudinal spherical aberration on the periphery to maintain visual acuity under low lighting conditions. It was specifically designed to improve outcomes with a monovision approach, hence its name standing for “Enhanced Monovision”. Postoperatively, the hospital’s standard care routine was followed: levofloxacin eyedrops for 1 week and prednisolone eyedrops for 4 weeks.
Postoperative Assessment
At one month post-surgery, patients underwent manifest refraction, pupil size measurements under photopic and mesopic conditions using the Nidek OPD3 scan (Nidek Co. Ltd., Gamagori, Japan), photopic monocular uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), uncorrected distance intermediate visual acuity (UIVA), distance-corrected intermediate visual acuity (DCIVA) at 66 cm, uncorrected distance near visual acuity (UNVA) and distance-corrected near visual acuity (DCNVA) at 40 cm. Monocular and binocular defocus curves, corrected for the targeted refractive outcome, were measured in each patient using the ETDRS chart positioned at 4 m under photopic and mesopic conditions, from +1.00 D to –4.00 D in 0.50 D steps. To determine patient satisfaction and limitations in certain daily-life activities, all patients completed the Catquest 9-SF questionnaire16,17 both before and 1 month after the surgery. In addition, all patients received standard postoperative examination as per routine cataract surgery with slit-lamp examination, intraocular pressure measurement using Goldmann applanation tonometry and dilated fundus examination. Any surgical complications or postoperative adverse events were also recorded.
Statistical Analysis and Sample Size Calculation
Both preoperative and postoperative values from all the patients recruited were obtained from medical records and transferred to Excel Version 2406 (Microsoft Corporation, Redmont, USA). Statistical analysis was performed using Excel and SPSS Version 29 (IBM, New York, USA). Descriptive values were shown as mean ± the standard deviation and ranges. The Kolmogorov–Smirnov test was used to test for normality. The Student’s t-test was used if the distribution was normal, while the Mann–Whitney test was used if it was not, for comparison between the two groups. Linear regression analysis was performed to identify any correlation of pupil size with visual acuity at different defocus values. Results with p values < 0.05 were considered statistically significant. The clinical results were presented in accordance with the standard for reporting refractive outcomes of intraocular lens-based refractive surgery.18 Considering the binocular near (−3.50 D) visual acuity obtained in the defocus curve as a primary endpoint, a parallel two-group design will be used to obtain a two-sided 95% confidence interval for the difference between the two group means. The standard deviations of the two groups are assumed to be equal and the pooled-variance t-distribution formula will be used to calculate the confidence interval. Assuming the standard deviation of each group is approximately logMAR 0.17 from a previous RayOne EMV study,19 it was determined that to produce a confidence interval with a distance of no more than logMAR 0.09 (which is less than one line in the EDTRS chart) from the sample mean difference to either confidence limit, the number of subjects needed will be 29 in each group. Hence, 60 patients were enrolled in this study: 30 patients in the bilateral emmetropia group, and 30 patients in the modest monovision group.
Results
The analysis included 30 patients in the emmetropia group (mean age of 70.5±8.7 years, with 63.3% being female) and 30 patients in the modest monovision group (mean age of 69.1±5.3 years, with 73.3% being female). The patient demographics and main characteristics for both groups are summarised in Table 1. No complications or adverse events were reported either during surgery or up to the final follow-up visit.
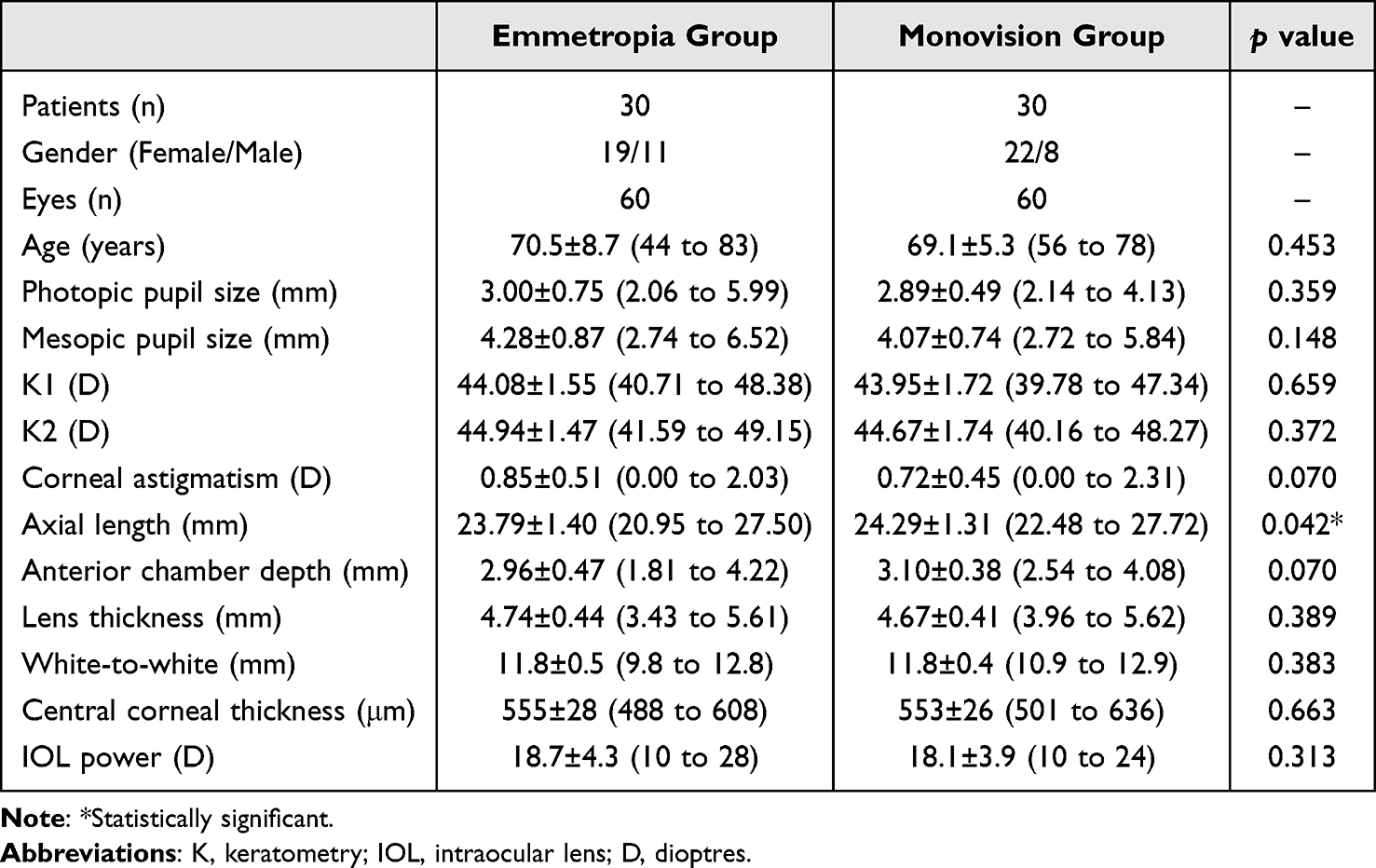 |
Table 1 Demographics and Characteristics of Eyes Included in This Study, Shown as Means, Standard Deviations (SDs), and Ranges |
Postoperative Refraction
Figure 1A shows the distribution of the postoperative spherical equivalent refraction for both groups, distinguishing between eyes targeted at 0 D and those at –1.50 D for the monovision group. This graph shows that 76.7% of eyes were within ±0.50 D and 98.3% were within ±1.00 D for the emmetropia group (n=60 eyes). These percentages were 90.0% and 100.0% respectively for the monovision far group (n=30 eyes). For the monovision near group (target refraction of –1.50 D), 76.7% of eyes were between –1.01 D and –2.00 D. The mean spherical equivalent refraction was –0.38±0.39 D, –0.22±0.36 D and –1.68±0.42 D for the bilateral emmetropia group, monovision far group and monovision near group, respectively. The analysis of the postoperative refractive astigmatism is shown in Figure 1B and revealed that 45.0%, 33.3% and 43.3% of eyes were within ≤0.50 D for the bilateral emmetropia, monovision far group and monovision near group, respectively. These percentages changed to 80.0%, 80.0% and 73.3% for values ≤1.00 D. The mean refractive astigmatism was –0.84±0.55 D, –0.83±0.44 D and –0.89±0.60 D for the bilateral emmetropia, monovision far group and monovision near group, respectively.
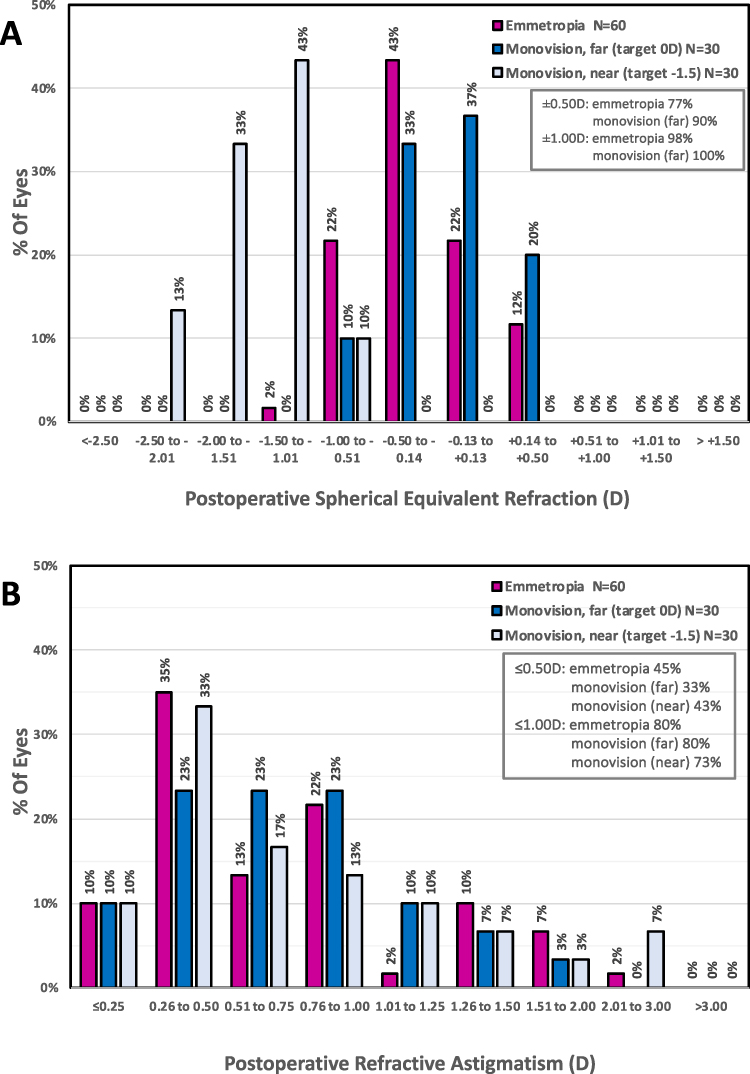 |
Figure 1 (A) Postoperative spherical equivalent refractive accuracy in diopters for the emmetropia group and for monovision group distinguishing between eyes targeted at 0 D (far) and those at –1.50 D (near) 1 month after enhanced monofocal intraocular lens implantation. (B) Postoperative refractive astigmatism in diopters for the emmetropia group and for monovision group distinguishing between eyes targeted at 0 D (far) and those at –1.50 D (near) 1 month after enhanced monofocal intraocular lens implantation. |
Visual Acuity
Table 2 shows the postoperative mean and ranges for monocular and binocular visual acuities at different distances for both groups. For the monovision group, eyes targeted at 0 D and –1.50 D were further differentiated. Monocular UDVA and UIVA values were similar, with no statistically significant difference between the emmetropia group and the monovision far group (p = 0.43 and 0.09 respectively). The emmetropia group had better monocular UDVA compared to the monovision near group (p < 0.01), while the monovision near group had better monocular UIVA and UNVA compared to the emmetropia group (p < 0.01 for both). The monovision far group also had better monocular UDVA than the monovision near group (p < 0.01), while the monovision near group had better monocular UIVA and UNVA compared to the monovision far group (p < 0.01 for both). There was no statistically significant difference in binocular CDVA between the bilateral emmetropia and monovision groups. However, both binocular DCIVA and DCNVA were statistically significantly better in the monovision group compared to the bilateral emmetropia group (p < 0.01 for both). Figure 2 depicts the cumulative percentage of eyes that achieved the specified monocular UDVA (A), UIVA (B), UNVA (C), CDVA (D), DCIVA (E) and DCNVA (F) values for the two groups. The monovision near group was corrected to target refraction of −1.50 D in Figure 2A–C, to illustrate the effect of monovision. In Figure 2D–F, all the eyes were corrected for distance. The monocular UDVA was 0.2 logMAR or better in 78% of eyes in the bilateral emmetropia group and 83% of eyes in the monovision far group (Figure 2A). These values increased to 93% for CDVA 0.1 logMAR or better for both groups (Figure 2D). The mean values of postoperative monocular CDVA were about 0 logMar for both the emmetropia and the monovision far groups (Table 2). For intermediate vision, the monocular UIVA was 0.3 logMAR or better in 57%, 43% and 73% of eyes in the bilateral emmetropia, monovision far and monovision near groups (Figure 2B). For near vision, the cumulative percentages of monocular UNVA achieving 0.3 logMAR or better were 23%, 10% and 47% for the emmetropia, monovision far and monovision near groups, respectively (Figure 2C).
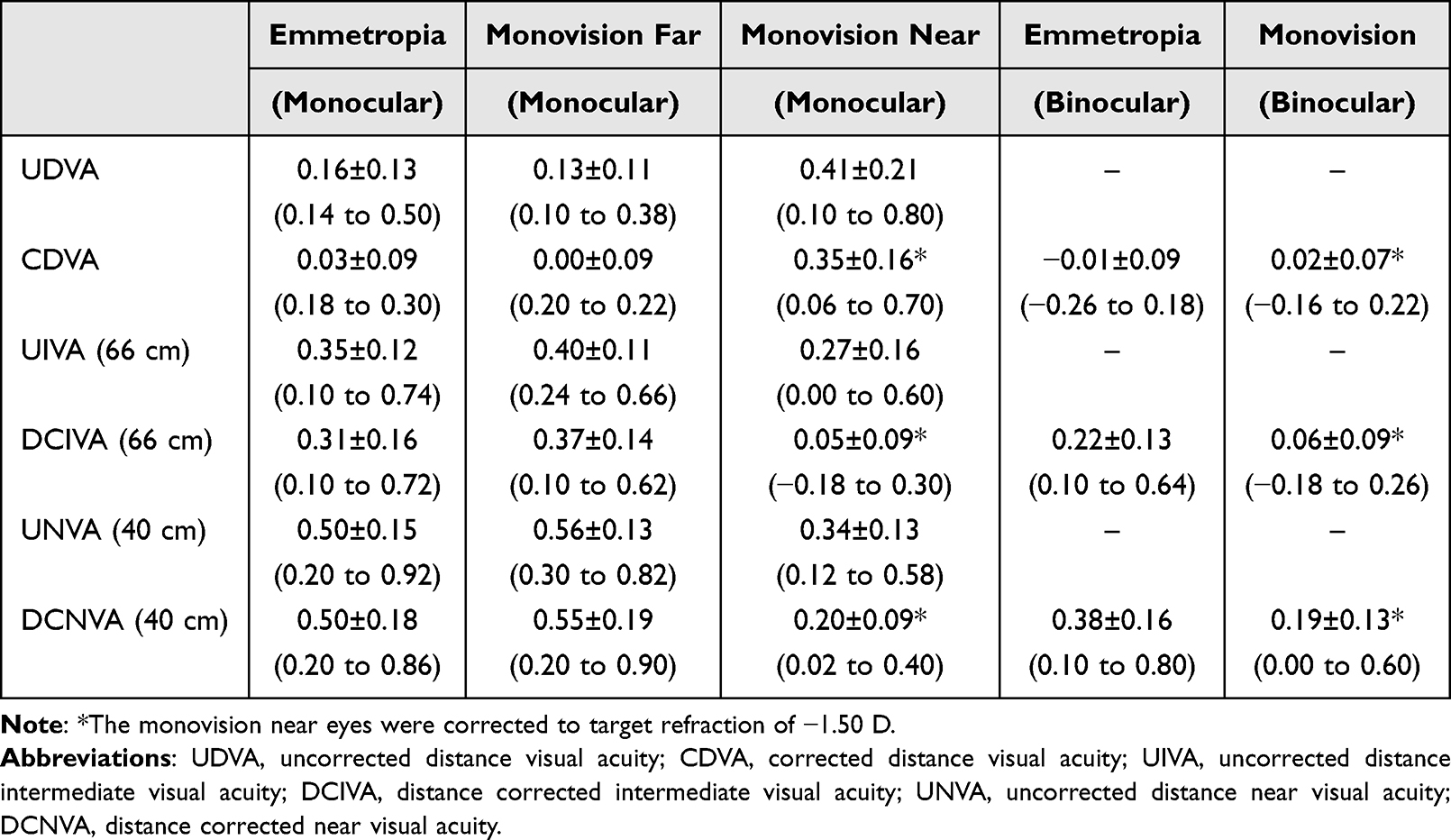 |
Table 2 Monocular and Binocular logMAR Visual Acuity Outcomes of Eyes Implanted with the RayOne EMV Intraocular Lens Shown as Means, Standard Deviations (SDs), and Ranges at a 1-month Follow-Up |
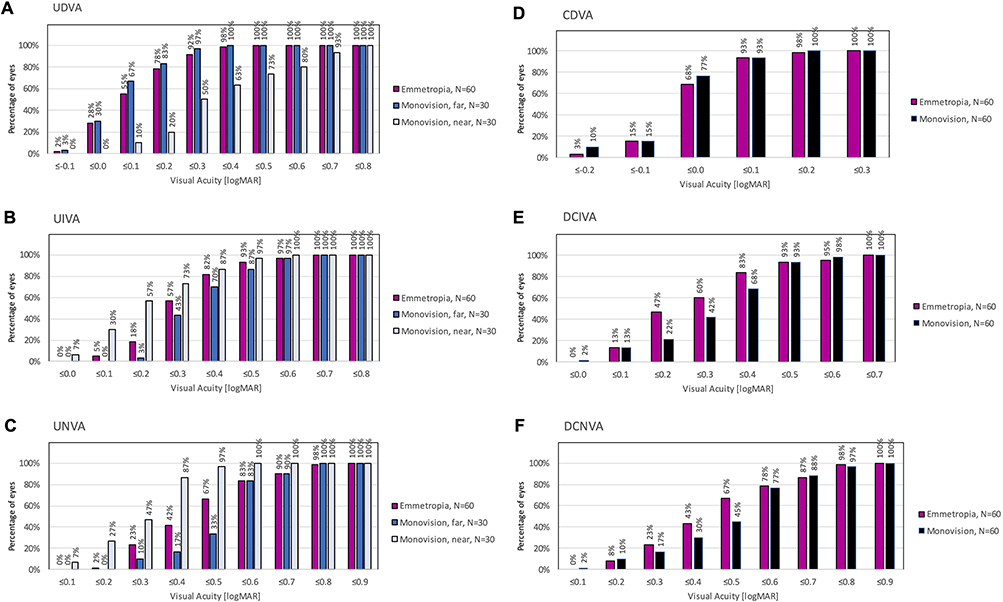 |
Figure 2 Visual acuity outcomes 1 month after enhanced monofocal intraocular lens implantation for emmetropia and monovision groups, and for monovision group separating between eyes targeted at 0 D (far) and those at –1.50 D (near): (A) cumulative uncorrected distance visual acuity (UDVA); (B) cumulative uncorrected intermediate visual acuity (UIVA); (C) cumulative uncorrected near visual acuity (UNVA); (D) cumulative corrected distance visual acuity (CDVA); (E) cumulative distance corrected intermediate visual acuity (DCIVA); (F) cumulative distance corrected near visual acuity (DCNVA). |
Defocus Curve
Figure 3 shows the monocular and binocular defocus curves recorded under photopic (Figure 3A and B) and mesopic (Figure 3C and D) conditions for both groups. In the monovision group, monocular defocus curves were further separated for eyes targeted for far and near distances. Under photopic conditions, the monocular defocus range achieving 0.2 logMAR or better, measured from 0 D to near, was 1.1 D for both the emmetropia and monovision far groups, and 1.0 D when measured from −1.5 D to near for the monovision near group. For total monocular defocus range achieving 0.2 logMAR or better, it was 2.1 D for both the emmetropia and monovision far groups, and 2.0 D for the monovision near group. Under mesopic conditions, the monocular defocus range achieving 0.2 logMAR or better, measured from 0 D to near, was 1.0 D for the emmetropia group, 1.2 D for the monovision far group, and 1.0 D for the monovision near group when measured from −1.5 D to near. The total monocular defocus range achieving 0.2 logMAR or better was 1.8 D for the emmetropia group, 2.1 D for the monovision far group, and 2.0 D for the monovision near group. Under photopic conditions, the binocular defocus range achieving 0.2 logMAR or better, measured from 0 D to near, was 1.3 D for the emmetropia group and 2.6 D for the monovision group. The total binocular defocus range achieving 0.2 logMAR or better was 2.6 D for the emmetropia group and 3.6 D for the monovision group. Under mesopic conditions, the binocular defocus range achieving 0.2 logMAR or better, measured from 0 D to near, was 1.3 D for the emmetropia group, and 2.5 D for the monovision group. The total binocular defocus range achieving 0.2 logMAR or better was 2.6 D for the emmetropia group and 3.5 D for the monovision group. A comparative statistical analysis performed between both groups under binocular conditions revealed similar visual acuity at distance (0 D: p = 0.32 and 0.61) but statistically significant better visual acuity in the monovision group from –1.00 D to –4.00 D for photopic and –3.50 D for mesopic conditions (p < 0.04 in all cases). This range of defocus is equivalent to a range of vision from 1 m to 25–30 cm.
 |
Figure 3 Defocus curves for monocular (A) and binocular (B) photopic, and monocular (C) and binocular (D) mesopic conditions for the emmetropia group and for monovision group distinguishing between eyes targeted at 0 D (far) and those at –1.50 D (near) implanted with the enhanced monofocal intraocular lens at the 1-month postoperative visit. Standard deviation bars are also shown for each defocus value. P values were shown for the comparative analysis between both groups under binocular photopic and mesopic conditions. * statistically significant difference (p < 0.05). Abbreviation: VA, visual acuity. |
Pupil Size
Under photopic conditions, the mean pupil size was 2.97 ± 0.68 cm (range 2.06 cm to 5.99 cm). Under mesopic conditions, the mean pupil size was 4.23 ± 0.83 cm (range 2.74 cm to 6.52 cm). Linear regression analysis was performed to identify any linear correlation between visual acuity in both groups under photopic and mesopic conditions, and pupil size. There was no statistically significant linear correlation between pupil size and logMAR visual acuity at 0 D defocus, −1.0 D defocus and −1.5 D defocus for the emmetropia group, monovision far and monovision near groups under both photopic and mesopic conditions (p > 0.05 for all).
Catquest 9-SF Questionnaire
Figure 4 shows the outcomes of the Catquest 9-SF questionnaire for both the emmetropia and monovision groups, before and after the surgery. At 1-month post-surgery, there was a clear improvement in all performance measures compared to before surgery, with 57% to 100% of patients in both groups reporting “no difficulty” in performing daily activities. Majority of the patients in both groups were very or fairly satisfied with their vision after surgery (90% and 96% for the emmetropia and monovision groups, respectively). For distance activities, both groups performed well in terms of reading subtitles on TV with 97% and 93% having no difficulty for the emmetropia and monovision groups, respectively. For near activities, specifically regarding seeing the prices of goods when shopping, 67% of patients reported having no difficulty in the emmetropia group compared to 100% in the monovision group. For reading text in the newspapers, 63% in the emmetropia group and 90% in the monovision group reported having no difficulty.
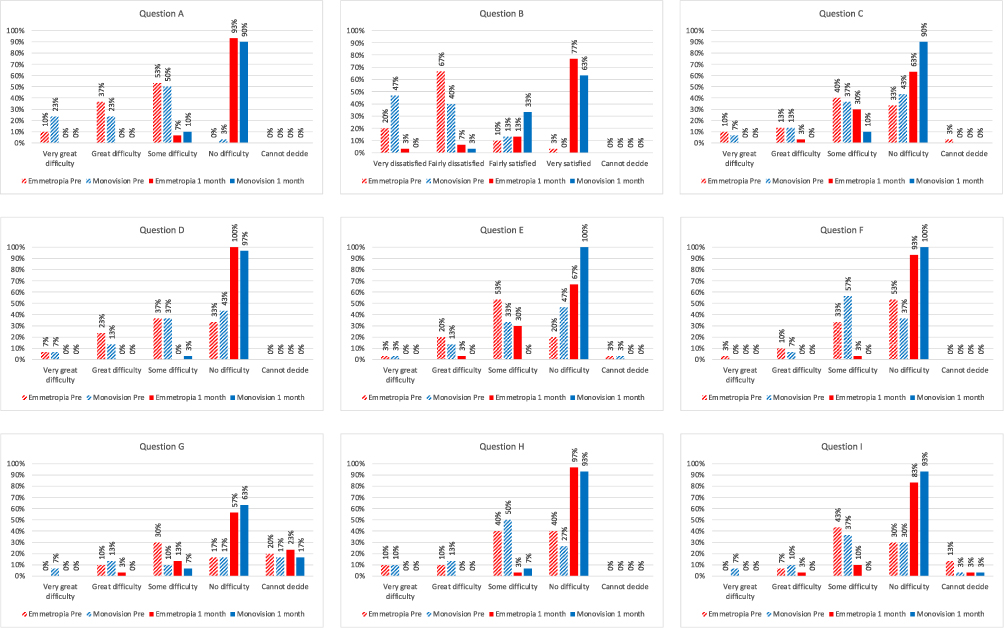 |
Figure 4 Outcomes of the Catquest 9-SF questionnaire before surgery and at the 1-month postoperative visit after the enhanced monofocal intraocular lens implantation in the emmetropia and monovision groups. (A) Do you find that your sight at present in some way causes you difficulty in your everyday life? (B) Are you satisfied or dissatisfied with your sight at present? (C) Do you have difficulty with reading text in the newspapers? (D) Do you have difficulty with recognising the faces of people you meet? (E) Do you have difficulty with seeing the prices of goods when shopping? (F) Do you have difficulty seeing to walk on uneven surfaces, eg cobblestones? (G) Do you have difficulty seeing to do handicrafts, woodwork etc.? (H) Do you have difficulty reading subtitles on TV? (I) Do you have difficulty seeing to engage in an activity/hobby that you are interested in? |
Discussion
This study aimed to elucidate the performance and patient satisfaction of the RayOne EMV IOL with either a bilateral emmetropia or modest monovision approach. The primary purpose of an enhanced monofocal IOL is to provide good quality of vision with a good level of spectacle independence for distance and intermediate vision. Our results support these objectives, demonstrating that the enhanced monofocal IOL produced good visual acuity and high percentages of patients that were able to perform near tasks, especially with modest monovision.
We found that for the emmetropia group that 76.7% of eyes were within ±0.50 D and 98.3% were within ±1.00 D, with a mean spherical equivalent of −0.30±0.39 D. These findings align with recent studies on the RayOne EMV targeted for emmetropia.10,11 García-Bella et al in a retrospective study at 3 months post-surgery, found a mean manifest spherical equivalent of −0.39±0.28 D, with 87.0% of eyes within ±0.50 D and 100% within ±1.00 D.11 For corrected vision, García-Bella et al11 found that CDVA was 0.0 logMAR or better in 92% of eyes and 0.1 logMAR or better in 100% of eyes, and in our case these values were 68.3% and 93.3%, respectively. At intermediate vision, they found that DCIVA was 0.2 logMAR or better in 39%, and 0.3 logMAR or better in 91% of eyes, and our values were 46.7% and 60.0%, respectively. In relation to the binocular defocus curve, they found a visual acuity ≤0.2 logMAR over a 2 D range from +1.00 D to –1.25 D. These results agree with the outcomes we have obtained in the binocular emmetropia group. They also reported CatQuest-9SF questionnaire outcomes indicating that 92% of patients experienced no difficulty with their vision in their daily life. Similarly, our study found that 93% of patients reported no vision-related difficulties. Regarding satisfaction, García-Bella et al11 found that 58% of patients were very satisfied with their present vision and 38% of patients were fairly satisfied, compared to our values of 77% and 13%. For everyday tasks, between 80% and 96% of their patients reported no difficulty,11 similar to our range of 57% to 100%. For reading newspapers, their cohort reported 58% with no difficulty, 37% with some difficulty, and 4% with great difficulties. Our results were 63%, 30% and 3%, respectively. Together with the binocular defocus curve outcomes, these findings indicate that the IOL when targeted for emmetropia provides solid distance and intermediate visual acuity with high levels of patient satisfaction.
Modest monovision in enhanced monofocal IOLs aims to improve intermediate and near vision without compromising distance visual acuity. For patients targeted at 0.00 D in the far eye and at –1.50 D in the near eye, the post-operative mean spherical equivalent refraction were −0.14±0.36 D and-1.60±0.42 D, respectively. The emmetropia and monovision far groups had comparable UDVA, with 78% and 83% of eyes achieving 0.2 logMAR or better, respectively. However, the monovision near group had much better UCIVA (57% of eyes 0.2 logMAR or better) and UNVA (47% of eyes 0.3 logMAR or better). In terms of binocular mean visual acuity, the emmetropia and monovision groups had similar CDVA (−0.01±0.09 logMAR and 0.02±0.07 logMAR), but the monovision group had much better UCIVA and DCNVA of 0.06±0.09 logMAR and 0.19±0.13 logMAR, respectively. The monovision results indicate that the far eye provides good distance and intermediate vision, while the near eye provides strong intermediate and near vision. In conjunction with the binocular defocus curves, there is strong evidence that blended vision is being achieved with modest monovision. In the emmetropia group, binocular depth of focus was 1.3 D under both photopic and mesopic conditions. In the modest monovision group, however, these values increased significantly to 2.6 D and 2.5 D, respectively (p < 0.05). This finding clearly supports that modest monovision modality with the RayOne EMV IOL enhances the depth of focus and extends the range of vision. For the Catquest 9-SF questionnaire, patients in both the bilateral emmetropia and modest monovision groups reported high satisfaction with their vision after surgery, with 90% and 96% respectively, expressing that they were very or fairly satisfied. Although both groups showed high percentages of patients reporting no difficulty in performing the activities, the modest monovision group reported better outcomes for near tasks. Specifically, 30% of the bilateral emmetropia patients reported some difficulty reading newspapers or seeing prices when shopping, compared to only 10% and 0% in the modest monovision group. This shows a clear advantage for modest monovision in intermediate and near tasks.
Of note, the RayOne EMV IOL performed well with similar defocus ranges in both photopic and mesopic conditions, for both the bilateral emmetropia and modest monovision groups. This was supported by results which showed that visual acuities at 0.0 D, −1.0 D and −1.5D defocus had no linear correlation with pupil size. This suggests that the enhanced monofocal IOL performs well in various lighting conditions with different pupil sizes, maintaining its depth of focus. This is in contrast to EDOF IOLs where mesopic contrast sensitivity has been reported to be poorer than photopic contrast sensitivity, with pupil dependency on the depth of focus.20 Vega et al also reported that for the ICB00 (Johnson & Johnson Vision, USA) IOL, when the pupil size was 2mm, it induced a myopic shift to improve intermediate vision, while when the pupil size was bigger than 3.5mm, there is no apparent difference between the ICB00 and a standard monofocal IOL of the same platform.21
This study is the first to analyze the effect of modest monovision (−1.5 D target for the near eye) with the RayOne EMV IOL. The target of −1.5 D is a commonly used target locally and in several Asian countries. This may be because patients in the region have a habitual nearer reading distance compared to their Western counterparts. Hayashi et al reported that −1.5 D improves near vision without a significant drop in stereopsis, while −1 D maintains stereopsis but has poorer near vision, and −2 D causes a significant drop in stereopsis.15 A recent study on the RayOne EMV IOL with micro-monovision reported improved intermediate and near visual acuity with 72% achieving binocular UIVA of 0.2 logMAR or better and 60% achieving binocular UNVA of 0.3 logMAR or better, without compromising distance acuity or contrast sensitivity.22 Previous studies on the Tecnis Eyhance IOL using modest monovision targets (−0.50 to −1.25 D) have shown statistically significant improvements in uncorrected binocular visual acuity at intermediate and near distances compared to monofocal lenses. Beltraminelli et al reported superior uncorrected binocular visual acuity for the enhanced monofocal group at these distances,12 while Sandoval et al found a one-line improvement in UIVA (p = 0.02) and UNVA (p = 0.01) with a −0.75 D monovision target.13 Dell et al, using targets between −0.50 D and −1.50 D, reported mean binocular logMAR UDVA, UIVA, and UNVA of −0.03±0.08, 0.09±0.12, and 0.32±0.15, respectively.14
The limitations of the study include a relatively short follow-up time of 1 month. However, it is understood that for most patients, refractive stability would have likely been achieved within this period. At the initiation of this study, the RayOne EMV IOL lacked a toric version and with the inclusion criteria allowing up to −1.5 D of corneal astigmatism, this may have impacted uncorrected visual acuity outcomes. Nevertheless, the defocus curves which were measured with distance correction illustrate the performance of the IOL when astigmatism is fully corrected. As this was a new IOL, the manufacturer’s lens constant of 118.6 was used at the beginning of the study. This resulted in early myopic outcomes that may have negatively impacted the uncorrected visual acuities of the early patients. After the first ten eyes, the lens constant was optimized to 118.1. The optimized lens constant for the IOL based on a large series is also now available on the IOLCON.org website. The allocation of each patient to each specific study groups was based on the patient visual needs. Although this may have resulted in allocation bias, the study methodology reflects actual clinical practice where the surgeon selects the refractive targets based on the patient’s requirements. The study also did not assess stereoacuity in patients with modest monovision, although none of the patients expressed any difficulties in their everyday life. Future studies could be performed to consider visual phenomena, stereoacuity, contrast sensitivity and longer-term outcome evaluations to confirm the results of our study.
Conclusion
In conclusion, the results indicate that the RayOne EMV IOL provides solid distance and intermediate vision regardless of whether it is targeted for bilateral emmetropia or modest monovision, with additional near vision benefits with modest monovision. The IOL performed well under both photopic and mesopic conditions, with no significant dependency on pupil size. Both groups reported high satisfaction, with the modest monovision group showing greater capability for near tasks compared to the bilateral emmetropia group.
Funding
This study received research funding from Rayner Intraocular Lens Limited, Worthing, United Kingdom.
Disclosure
Dr Yeo received research funding and speaker honoraria from Alcon, Bausch and Lomb, CSO, Topcon, Rayner, Intalight and Zeiss, and licenses his intraocular lens formula to Bausch and Lomb, and Towardpi. The other authors report no financial interests or conflicts of interest with respect to this work.
References
1. Cho JY, Won YK, Park J, et al. Visual outcomes and optical quality of accommodative, multifocal, extended depth-of-focus, and monofocal intraocular lenses in presbyopia-correcting cataract surgery: a systematic review and Bayesian network meta-analysis. JAMA Ophthalmol. 2022;140(11):1045–1053. doi:10.1001/jamaophthalmol.2022.3667
2. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12(12):CD003169. doi:10.1002/14651858.CD003169.pub4
3. Rodov L, Reitblat O, Levy A, Assia EI, Kleinmann G. Visual outcomes and patient satisfaction for trifocal, extended depth of focus and monofocal intraocular lenses. J Refract Surg. 2019;35(7):434–440. doi:10.3928/1081597X-20190618-01
4. Wan KH, Au ACK, Kua WN, et al. Enhanced monofocal versus conventional monofocal intraocular lens in cataract surgery: a meta-analysis. J Refract Surg. 2022;38(8):538–546. doi:10.3928/1081597X-20220707-01
5. Łabuz G, Son HS, Naujokaitis T, Yildirim TM, Khoramnia R, Auffarth GU. Laboratory investigation of preclinical visual-quality metrics and halo-size in enhanced monofocal intraocular lenses. Ophthalmol Ther. 2021;10(4):1093–1104. doi:10.1007/s40123-021-00411-9
6. Schmid R, Borkenstein AF. Analysis of higher order aberrations in recently developed wavefront-shaped IOLs. Graefes Arch Clin Exp Ophthalmol. 2022;260(2):609–620. doi:10.1007/s00417-021-05362-2
7. Schmid R, Fuchs C, Luedtke H, Borkenstein AF. Depth of focus of four novel extended range of vision intraocular lenses. Eur J Ophthalmol. 2023;33(1):257–261. doi:10.1177/11206721221125081
8. Schmid R, Luedtke H, Borkenstein AF. Effect of decentration and tilt on four novel extended range of vision intraocular lenses regarding far distance. Eur J Ophthalmol. 2023;33(2):933–942. doi:10.1177/11206721221128864
9. Alarcon A, Canovas C, Koopman B, Pande MV, Koch DD, Piers P. Optical bench evaluation of the effect of pupil size in new generation monofocal intraocular lenses. BMC Ophthalmol. 2023;23(1):112. doi:10.1186/s12886-023-02839-y
10. Madhivanan N, Nivean PD, Madanagopalan VG, Priya S, Madhivanan N, Arthi M. Clinical results after binocular implantation of a unique nondiffractive enhanced monofocal intraocular lens designed for enhanced monovision to increase the depth of focus. Indian J Ophthalmol. 2024;72(1):63–65. doi:10.4103/IJO.IJO_447_23
11. García-Bella J, Burgos-Blasco B, Vidal-Villegas B, Garzón N, Villanueva C, García-Feijoo J. Visual and refractive outcomes after bilateral implantation of an enhanced monofocal intraocular lens: prospective study. J Cataract Refract Surg. 2024;50(6):585–590. doi:10.1097/j.jcrs.0000000000001422
12. Beltraminelli T, Rizzato A, Toniolo K, Galli A, Menghini M. Comparison of visual performances of enhanced monofocal versus standard monofocal IOLs in a mini-monovision approach. BMC Ophthalmol. 2023;23(1):170. doi:10.1186/s12886-023-02920-6
13. Sandoval HP, Potvin R, Solomon KD. Comparing visual performance and subjective outcomes with an enhanced monofocal intraocular lens when targeted for emmetropia or monovision. Clin Ophthalmol. 2023;17:3693–3702. doi:10.2147/OPTH.S442752
14. Dell SJ, Hannan SJ, Venter JA, et al. Comparative analysis of clinical and patient-reported outcomes of a new enhanced monofocal IOL and a conventional monofocal IOL. Clin Ophthalmol. 2024;18:1157–1169. doi:10.2147/OPTH.S456332
15. Hayashi K, Yoshida M, Manabe S, Hayashi H. Optimal amount of anisometropia for pseudophakic monovision. J Refract Surg. 2011;27(5):332–338. doi:10.3928/1081597X-20100817-01
16. McAlinden C, Gothwal VK, Khadka J, Wright TA, Lamoureux EL, Pesudovs K. A head-to-head comparison of 16 cataract surgery outcome questionnaires. Ophthalmology. 2011;118(12):2374–2381. doi:10.1016/j.ophtha.2011.06.008
17. Kabanovski A, Hatch W, Chaudhary V, et al. Validation and application of Catquest-9SF in various populations: a systematic review. Surv Ophthalmol. 2020;65(3):348–360. doi:10.1016/j.survophthal.2019.12.002
18. Reinstein DZ, Archer TJ, Srinivasan S, et al. Standard for reporting refractive outcomes of intraocular lens-based refractive surgery. J Cataract Refract Surg. 2017;43(4):435–439. doi:10.1016/j.jcrs.2017.04.005
19. Zeilinger J, Kronschläger M, Schlatter A, et al. Comparing an advanced monofocal with a non-diffractive extended depth of focus intraocular lens using a mini-monovision approach. Am J Ophthalmol. 2025;271:86–95. doi:10.1016/j.ajo.2024.10.014
20. Baur ID, Yan W, Auffarth GU, Khoramnia R, Łabuz G. Optical quality and higher order aberrations of refractive extended depth of focus intraocular lenses. J Refract Surg. 2023;39(10):668–674. doi:10.3928/1081597X-20230831-01
21. Vega F, Millán MS, Gil MA, Garzón N. Optical performance of a monofocal intraocular lens designed to extend depth of focus. J Refract Surg. 2020;36(9):625–632. doi:10.3928/1081597X-20200710-01
22. Law EM, Aggarwal RK, Buckhurst PJ. Visual outcomes, contrast sensitivity and defocus profile with an aspheric monofocal intraocular lens utilizing positive spherical aberration. J Cataract Refract Surg. 2025;51:394–398. doi:10.1097/j.jcrs.0000000000001612
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.