Back to Journals » Clinical Ophthalmology » Volume 19
Visual Performance and Refractive Stability of Clareon® Monofocal Intraocular Lens Implanted with an Automated Delivery System
Authors Tran E ![]() , Shah N
, Shah N ![]() , Caballero Ortiz S, Kyveris A, Berg G, Chan T
, Caballero Ortiz S, Kyveris A, Berg G, Chan T
Received 10 June 2025
Accepted for publication 8 September 2025
Published 24 October 2025 Volume 2025:19 Pages 3933—3939
DOI https://doi.org/10.2147/OPTH.S545977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Edward Tran,1,2 Nirmit Shah,2,3 Sandra Caballero Ortiz,2 Angela Kyveris,2 Graham Berg,2 Toby Chan2,4
1Schulich School of Medicine, University of Western Ontario, London, ON, Canada; 2Ocular Health Centre, Kitchener, ON, Canada; 3Melbourne Medical School, University of Melbourne, VIC, Australia; 4Michael G. DeGroote School of Medicine, McMaster University, Hamilton, ON, Canada
Correspondence: Edward Tran, Ocular Health Centre, 31 Kingsbury Dr Unit #501, Kitchener, ON, N2A 0K5, Canada, Email [email protected]
Purpose: To evaluate the visual performance, refractive stability, and glistening-free clarity of the Clareon® monofocal intraocular lens (IOL) implanted using the AutonoMe® automated delivery system in a real-world North American setting.
Patients and Methods: A prospective, single-arm study was conducted at a single Canadian site involving 46 patients, or 85 eyes, undergoing cataract surgery with Clareon® IOL implantation. Eligible participants were ≥ 22 years old with best-corrected distance visual acuity (BCDVA) of 0.3 logMAR or worse, targeted for emmetropia, and had < 1.0 D of preoperative astigmatism. Exclusion criteria included retinal disease, glaucoma, amblyopia, corneal pathology, and prior intraocular or corneal surgery. Manifest refraction, uncorrected (UDVA), best-corrected (BCDVA), and low-contrast visual acuity (LCVA) were assessed at 1, 3, and 12 months postoperatively. Glistenings were graded using the Miyata scale at 3 and 12 months.
Results: No statistically significant changes were observed in manifest refraction, UDVA, or BCDVA between 1 and 3 months (p > 0.05). At 3 months, the mean spherical equivalent was +0.09 D, with low residual astigmatism (– 0.33 D). Mean logMAR UDVA and BCDVA were 0.13 and 0.02, respectively. LCVA was 0.04 logMAR. No glistenings were observed at either 3 or 12 months in any patient. Refractive and visual outcomes remained stable over time, with no device-related complications reported.
Conclusion: The Clareon® IOL demonstrated excellent refractive accuracy, stable visual performance, and sustained optical clarity with no glistenings up to one year postoperatively. Its compatibility with the AutonoMe® delivery system supports its utility as a reliable option for cataract surgery.
Keywords: cataract surgery, Clareon, monofocal intraocular lens, automated delivery system, surgical outcomes
Introduction
Cataract surgery is the most common elective procedure in North America, with 17% of adults aged 65 and older affected by cataracts or requiring surgery.1 As demand continues to grow, selecting the most appropriate intraocular lens (IOLs) is crucial for optimizing patient outcomes and satisfaction. However, ophthalmologists must navigate an expanding array of IOL technologies, each offering distinct advantages and limitations, making this decision increasingly complex.
Modern monofocal IOLs generally provide excellent high-contrast visual acuity; however, certain material-related phenomena, such as glistenings and surface haze, have raised concerns about long-term optical quality.2,3 Glistenings are fluid-filled microvacuoles that form within the IOL optic, typically resulting from phase separation of water in hydrophobic acrylic materials.3 These microvacuoles often appear within months after implantation.3,4 Although mild glistenings may not significantly affect high-contrast visual acuity or modulation transfer function, they can increase forward light scatter, leading to reduced contrast sensitivity and visual disturbances such as glare, halos, and hazy vision.3,5
Efforts to reduce glistenings in hydrophobic acrylic IOLs have led to the development of new materials designed to maintain optical clarity over time. The Clareon® monofocal IOL (model CNA0T0) is a single-piece, aspheric hydrophobic acrylic lens composed of an acrylate–methacrylate copolymer with 2-hydroxyethyl methacrylate (HEMA), resulting in a higher water content (~1.5%) than its predecessor, AcrySof®.6–8 This change aims to prevent microvacuole formation and minimize glistening development. While maintaining a similar optical design and refractive index to the widely used AcrySof IQ IOL, early studies suggest Clareon® has lower levels of glistenings and surface haze.7,9 The AutonoMe® system, a CO2-powered, single-use automated injector, was introduced to standardize IOL delivery.10,11 It allows surgeon-controlled implantation and may reduce variability and wound trauma.11
Although preclinical studies have shown smooth delivery and minimal impact on incision integrity, real-world clinical data on the Clareon® IOL with the AutonoMe system remain limited to Europe.12 Prior to this study, no published North American series had evaluated the visual performance and refractive stability of the Clareon® monofocal intraocular lens implanted with an automated delivery system in routine clinical practice. This study was therefore conducted to provide further insight into the lens’s optical clarity, refractive stability, and clinical utility in a real-world setting.
Methods
Study Design
This is a prospective, single-arm, single-site, single-surgeon study evaluating the visual performance and refractive stability of the Clareon® monofocal intraocular lens (IOL) CNA0T0 implanted using the AutonoMe® automated delivery system (Alcon Laboratories Inc., Fort Worth, TX, USA) after phacoemulsification and cataract extraction. The study was conducted at the Ocular Health Centre in Kitchener, Ontario, Canada, with approval from the independent ethics board Advarra (IRB #00046761). All procedures adhered to the tenets of the Declaration of Helsinki, and written informed consent was obtained from all patients prior to enrollment. Participants were allowed to withdraw at any time without affecting their standard of care.
Inclusion and Exclusion Criteria
Eligible participants met the following inclusion criteria: age ≥ 22 years at the time of study participation, best-corrected distance visual acuity (BCDVA) of 0.3 logMAR (20/40 Snellen) or worse, planned cataract removal via routine small-incision surgery, calculated IOL power between 15.0 D and 25.0 D (targeted for emmetropia, 0.00 D), and preoperative astigmatism <1.0 D, as measured by keratometry in both eyes. Exclusion criteria included any retinal disease or pathology expected to reduce potential BCDVA to worse than 0.2 logMAR, a history of glaucoma, amblyopia, or neurological conditions affecting vision, recurrent anterior or posterior segment inflammation, clinically significant corneal pathology or ocular surface disease that may adversely affect visual outcomes, and a history of prior intraocular or corneal surgery.
Clinical Endpoints
The primary endpoint of the study was the manifest refraction at 1 and 3 months post-implantation. Secondary endpoints included monocular and binocular uncorrected distance visual acuity (UDVA) and BCDVA at all study visits. Exploratory endpoints included binocular and monocular low-contrast visual acuity (LCVA) at 25% at months 3 and 12. IOL glistenings were assessed at months 3 and 12 using the Miyata protocol and grading scale. Glistening severity was assessed using the method described by Miyata et al (1997). Each patient was assessed for glistening by two independent reviewers. The same two reviewers assessed for glistening at each follow-up visit. If there was discrepancy between assessors, a third independent physician would assess the patient to make a final judgment. Pupils were pharmacologically dilated to ≥5 mm prior to slit-lamp evaluation. Glistening severity was graded on a scale of 0–3, where Grade 0 represented no glistenings, Grade 1 included up to 50 glistenings/mm³, Grade 2 included up to 100 glistenings/mm³, and Grade 3 included up to 200 glistenings/mm³. We also collected data on the clinical complications experienced by the patients while enrolled in the study. Complications assessed for included: posterior capsule pacification, intraocular pressure spikes, corneal or macular edema, uveitis, hyphema, wound leak, endopthalmitis, and retinal detachment.
Statistical Analysis
Descriptive statistics, including mean and standard deviation, were used to summarize primary, secondary, and exploratory outcome variables. For statistical analysis, changes in manifest refraction at months 1 and 3 were analyzed using paired t-tests. Snellen visual acuity measurements were converted to logMAR for statistical analysis. Changes in monocular UDVA and BCDVA at months 1 and 3 were also analyzed using paired t-tests. A paired T-test was used to compare LCVA between 3 and 12 months postoperatively.
Results
Patient Demographics
Patient demographics and preoperative characteristics are summarized in Table 1. The study included 46 patients, with a higher proportion of females (58.7%) than males (41.3%). The mean age was 73.0 years, with a median age of 74 years, indicating that most patients were in their early to mid-70s. The age range spanned from 47 to 86 years, reflecting a diverse patient population representative of those undergoing intraocular lens implantation. No cases of IOL glistening were observed in the cohort of 76 eyes at the 3-month and 12-month follow-ups. There were losses of 7 eyes across 4 patients by month 1–3 due to patient death, and 1 who not return for surgery of their second eye. At month 3, there were an additional 9 eyes across 5 patients which were lost to follow up. No further losses occurred between month 3 and month 12 of follow up. At 3 months following Clareon® IOL implantation, the mean spherical equivalent (SE) was +0.09 diopters (D), and the mean refractive cylinder was –0.33 D, reflecting excellent refractive accuracy and minimal residual astigmatism. UDVA measured 0.13 logMAR, while BCDVA improved to 0.02 logMAR, indicating that most patients achieved near-perfect vision with minimal correction. LCVA also demonstrated favorable outcomes, with a mean of 0.04 logMAR, suggesting that functional vision under reduced contrast conditions remained well-preserved. There were no cases of post-surgical complications by month 12.
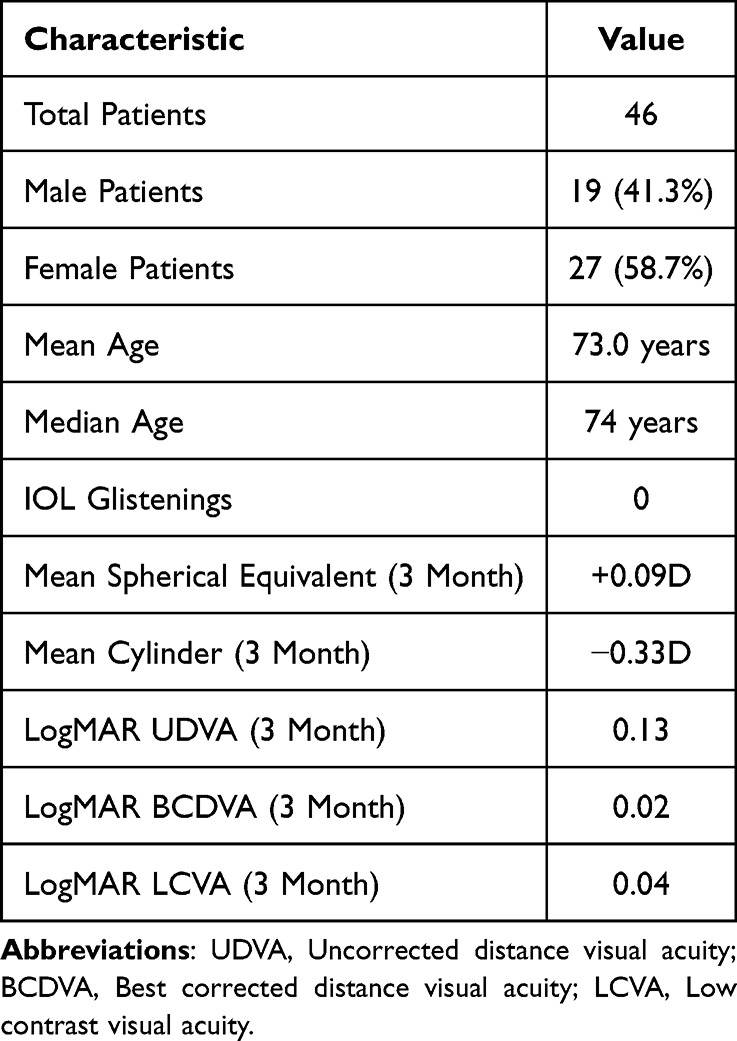 |
Table 1 Patient Demographics and Preoperative Characteristics |
Manifest Refraction
For manifest refraction, data were available for 77 eyes at 1 month and 69 eyes at 3 months. A paired t-test comparing manifest refraction outcomes between 1 and 3 months revealed no statistically significant difference in spherical equivalent (t = –1.328, p = 0.189) or cylinder (t = –0.886, p = 0.379).
Visual Acuity Outcomes
Figures 1 and 2 demonstrate that logMAR UDVA and BCDVA decreased from pre-operative levels and remained relatively the same from 1 month to 12 months. UDVA data were available for 85 eyes at 1 month and 74 eyes at 3 months. A paired t-test comparing UDVA between 1 and 3 months revealed no statistically significant difference (t = 1.567, p = 0.121). BCDVA measurements were recorded in 76 eyes at 1 month and 70 eyes at 3 months. A paired t-test comparing BCDVA between 1 and 3 months revealed no statistically significant difference (t = 1.629, p = 0.108).
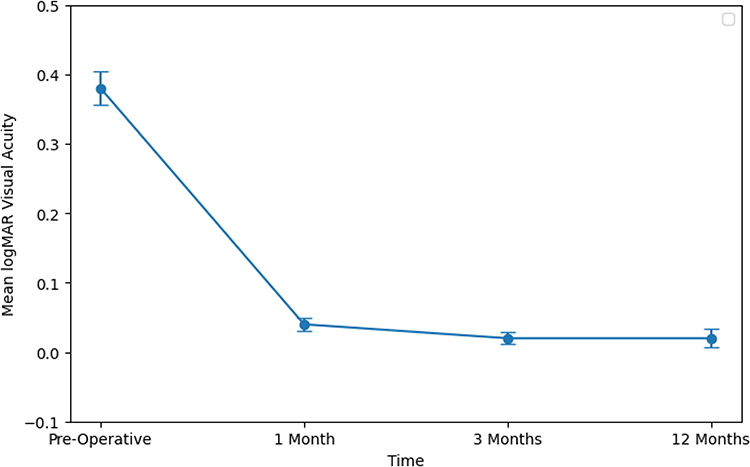 |
Figure 1 Mean logMAR uncorrected distance visual acuity over 12 months following Clareon® intraocular lens implantation. |
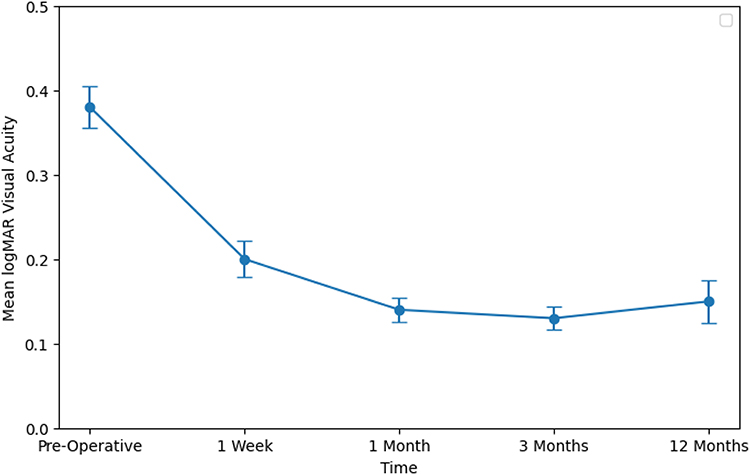 |
Figure 2 Mean logMAR best-corrected distance visual acuity over 12 months following Clareon® intraocular lens implantation. |
Figure 3 shows that logMAR low contrast visual acuity (LCVA) values at 3 and 12 months were relatively unchanged. LCVA was assessed in 47 eyes at 3 months and 19 eyes at 12 months under monocular conditions, and in 6 subjects at 3 months and 5 subjects at 12 months under binocular conditions. Paired t-tests comparing LCVA between 3 and 12 months showed no statistically significant difference with binocular measurements (t = 1.000, p = 0.500) or with monocular measurements (t = 0.402, p = 0.696).
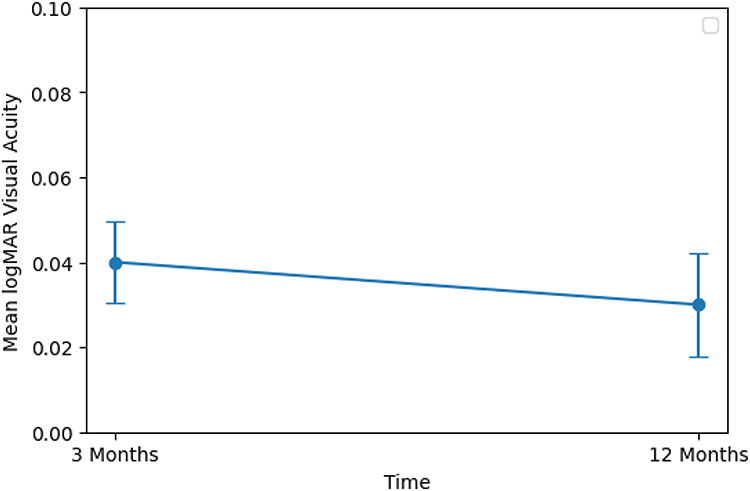 |
Figure 3 Mean logMAR low contrast visual acuity at 3 months and 12 months following Clareon® intraocular lens implantation. |
Discussion
This study included 46 patients who underwent Clareon® IOL implantation, with an emphasis on evaluating refractive outcomes, visual performance and IOL glistenings. Manifest refraction at 3 months showed minimal residual error (+0.09 D) and low residual astigmatism (–0.33 D). At 3 months, the cohort demonstrated excellent refractive precision and minimal residual astigmatism, indicating refractive stability.
At 3 months, the mean UDVA was 0.13 logMAR, indicating good uncorrected vision. BCDVA was 0.02 logMAR, consistent with near 20/20 acuity, and LCVA remained strong at 0.04 logMAR, suggesting preserved contrast sensitivity. Both UDVA and BCDVA remained stable from 1 to 3 months, and LCVA was preserved from 3 months to 12 months, indicating excellent functional vision under reduced contrast conditions. These results underscore the long-term reliability and visual performance of the Clareon® IOL, offering patients consistent visual outcomes with significant clinical implications for refractive stability over time. Additionally, the use of the AutonoMe® automated delivery system allows for a minimized incision size, reducing the risk of post surgical complications.13 The injector design also helps to maintain wound integrity by limiting damage to the corneal tissue and Descemet’s membrane, further reducing the likelihood of surgical complications.10
No glistenings were observed on slit-lamp examination at either 3 or 12 months postoperatively, with all Clareon® IOLs graded as Miyata grade 0. The absence of glistenings observed in our cohort is consistent with prior multicenter studies, which reported no glistenings in Clareon® IOLs up to 1 year postoperatively.6,12,14 This outcome highlights a key advantage of the Clareon® lens over earlier hydrophobic acrylic lenses. Its predecessor, the AcrySof®, has been shown in both laboratory and clinical studies to develop glistenings within months or years of implantation.15,16 The Clareon® IOL appears to effectively resist this phenomenon, likely due to its modified acrylic composition incorporating a small proportion of 2-hydroxyethyl methacrylate (HEMA) and a slightly higher water content.9,17 These material changes help prevent microvacuole formation, contributing to the sustained optical clarity observed in our study.17 The glistening-free performance of the Clareon® IOL supports its role as a viable lens option for cataract surgery, given its potential benefits for maintaining visual quality and reducing patient-reported visual disturbances.
The absence of glistenings in the Clareon® IOL is clinically meaningful, as glistenings can increase intraocular light scatter and reduce contrast sensitivity, particularly under mesopic or high-demand conditions.9,18 Although mild cases may not impact high-contrast visual acuity, more pronounced glistenings have been linked to measurable declines in visual quality.19 In our study, no glistenings were observed at any time point, and IOL optics remained consistently clear. This aligns with the preserved low-contrast visual acuity (LCVA) seen in our cohort and supports the lens’s ability to maintain long-term optical clarity. Compared to earlier hydrophobic acrylic lenses, the Clareon® lens material composition appears to minimize light scatter, potentially improving patient satisfaction and sustaining visual performance over time.
The AutonoMe® automated injector was well tolerated in our series, with smooth lens delivery and no device-related complications. Surgeon feedback was favorable, aligning with previous studies that reported high usability and consistent performance compared to manual injectors.20
This study has a couple of limitations. First, it was conducted at a single site with a single surgeon, which may limit the generalizability of the findings to other surgical settings or surgeons with different levels of experience. Second, the study lacked a control or comparison group (eg, a cohort receiving AcrySof® or another IOL), which restricts direct conclusions about the relative advantages of the Clareon® IOL. Finally, there was inconsistent data collection of visual acuity outcomes such as the low contrast distance visual acuity, limiting the data analysis that could occur despite relatively low losses to follow up during the study.
In summary, Clareon® IOL’s refractive stability, glistening-free clarity, and compatibility with the AutonoMe delivery system make it a strong option for cataract surgery, offering clinical reliability and surgical efficiency.
Abbreviations
BCDVA, Best-Corrected Distance Visual Acuity; D, Diopter; HEMA, 2-Hydroxyethyl Methacrylate; IOL, Intraocular Lens; LCVA, Low-Contrast Visual Acuity; logMAR, Logarithm of the Minimum Angle of Resolution; SE, Spherical Equivalent; UDVA, Uncorrected Distance Visual Acuity.
Funding
This study received financial support from Alcon, approximately $5000 CAD, which will be used to cover publication costs and conference presentation fees related to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shahbazi S, Studnicki J, Warner-Hillard CW. A cross-sectional retrospective analysis of the racial and geographic variations in cataract surgery. PLoS One. 2015;10(11):e0142459. doi:10.1371/journal.pone.0142459
2. Mönestam E, Behndig A. Change in light scattering caused by glistenings in hydrophobic acrylic intraocular lenses from 10 to 15 years after surgery. J Cataract Refract Surg. 2016;42(6):864–869. doi:10.1016/j.jcrs.2016.02.047
3. Grzybowski A, Markeviciute A, Zemaitiene R. A narrative review of intraocular lens opacifications: update 2020. Ann Transl Med. 2020;8(22):1547. doi:10.21037/atm-20-4207
4. Miyata A, Suzuki K, Boku C, et al. Glistening particles in the implanted acrylic intraocular lens. Rinsho Ganka. 1997;51:729–732.
5. Das K, Stover J, Schwiegerling J, Karakelle M. Technique for measuring forward light scatter in intraocular lenses. J Cataract Refract Surg. 2013;39(5):770–778. doi:10.1016/j.jcrs.2012.10.049
6. Oshika T, Sasaki N, Clinical Study Group on New Intraocular Lens and Delivery System. One-year multicenter evaluation of a new hydrophobic acrylic intraocular lens with hydroxyethyl methacrylate in an automated preloaded delivery system. J Cataract Refract Surg. 2022;48(3):275–279. doi:10.1097/j.jcrs.0000000000000746
7. Oshika T, Fujita Y, Inamura M, Miyata K. Mid-term and long-term clinical assessments of a new 1-piece hydrophobic acrylic IOL with hydroxyethyl methacrylate. J Cataract Refract Surg. 2020;46(5):682–687. doi:10.1097/j.jcrs.0000000000000142
8. Lane S, Collins S, Das KK, et al. Evaluation of intraocular lens mechanical stability. J Cataract Refract Surg. 2019;45(4):501–506. doi:10.1016/j.jcrs.2018.12.031
9. Werner L, Thatthamla I, Ong M, et al. Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. J Cataract Refract Surg. 2019;45(10):1490–1497. doi:10.1016/j.jcrs.2019.06.035
10. Negishi K, Masui S, Torii H, Nishi Y, Tsubota K. Refractive stability of a new single-piece hydrophobic acrylic intraocular lens and corneal wound repair after implantation using a new automated intraocular lens delivery system. PLoS One. 2020;15(9):e0238366. doi:10.1371/journal.pone.0238366
11. Mastropasqua L, Toto L, D’Ugo E, et al. In vivo and in vitro results of an automated preloaded delivery system for IOL implantation in cataract surgery. Int Ophthalmol. 2020;40(1):125–134. doi:10.1007/s10792-019-01154-0
12. Bouvarel E, He Z, Robert PY, et al. Early clinical outcomes and visual quality of a novel glistening-free intraocular lens: a European multicenter evaluation. J Cataract Refract Surg. 2024;50(1):45–53. doi:10.1097/j.jcrs.0000000000001089
13. Liu J, Wolfe P, Hernandez V, Kohnen T. Comparative assessment of the corneal incision enlargement of 4 preloaded IOL delivery systems. J Cataract Refract Surg. 2020;46(7):1041–1046. doi:10.1097/j.jcrs.0000000000000214
14. Titiyal JS, Basak SK, Shetty N, et al. Twelve-months follow-up postmarket study of a hydrophobic intraocular lens using a preloaded automated injector in an Indian population. Clin Ophthalmol. 2022;16:4215–4225. doi:10.2147/OPTH.S379054
15. Dhaliwal DK, Mamalis N, Olson RJ, et al. Visual significance of glistenings seen in the AcrySof intraocular lens. J Cataract Refract Surg. 1996;22(4):452–457. doi:10.1016/s0886-3350(96)80041-1
16. Christiansen G, Durcan FJ, Olson RJ, Christiansen K. Glistenings in the AcrySof intraocular lens: pilot study. J Cataract Refract Surg. 2001;27(5):728–733. doi:10.1016/s0886-3350(00)00700-8
17. Maxwell A, Suryakumar R. Long-term effectiveness and safety of a three-piece acrylic hydrophobic intraocular lens modified with hydroxyethyl-methacrylate: an open-label, 3-year follow-up study. Clin Ophthalmol. 2018;12:2031–2037. doi:10.2147/OPTH.S175060
18. Łabuz G, Knebel D, Auffarth GU, et al. Glistening formation and light scattering in six hydrophobic-acrylic intraocular lenses. Am J Ophthalmol. 2018;196:112–120. doi:10.1016/j.ajo.2018.08.032
19. Xi L, Liu Y, Zhao F, et al. Analysis of glistenings in hydrophobic acrylic intraocular lenses on visual performance. Int J Ophthalmol. 2014;7(3):446–451. doi:10.3980/j.issn.2222-3959.2014.03.11
20. Lee MW, Cheong FM, Yeo KC. Clinical evaluation of a new hydrophobic acrylic intraocular lens with a novel delivery system. Malays J Ophthalmol. 2022;4(1):63–74. doi:10.35119/myjo.v4i1.255
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.