Back to Journals » Clinical Ophthalmology » Volume 19
Visual Outcomes Following Hyperbaric Oxygen Therapy in Acute Central Retinal Artery Occlusion Patients
Authors Thoongsuwan S, Sirichayaporn T, Rodanant N, Phasukkijwatana N, Prakhunhungsit S ![]() , Wongchaisuwat N, Montrisuksirikun C
, Wongchaisuwat N, Montrisuksirikun C ![]() , Trinavarat A, Chinaroonchai K, Jiamsawad S
, Trinavarat A, Chinaroonchai K, Jiamsawad S ![]()
Received 22 April 2025
Accepted for publication 13 August 2025
Published 18 September 2025 Volume 2025:19 Pages 3419—3429
DOI https://doi.org/10.2147/OPTH.S510772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Somanus Thoongsuwan,1 Thanut Sirichayaporn,1 Nuttawut Rodanant,1 Nopasak Phasukkijwatana,1 Supalert Prakhunhungsit,1 Nida Wongchaisuwat,1 Chinnapat Montrisuksirikun,1 Adisak Trinavarat,1 Kusuma Chinaroonchai,2 Supathida Jiamsawad1
1Department of Ophthalmology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Department of Surgery, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Supathida Jiamsawad, Department of Ophthalmology, Faculty of Medicine Siriraj Hospital, Mahidol University, 2 Wang Lang Road, Bangkok Noi, Bangkok, Thailand, 10700, Tel +66 2 419 8037, Fax +66 2 414 1232, Email [email protected]
Purpose: To evaluate the efficacy of a novel HBOT protocol, characterized by specific pressure levels and treatment duration in patients with CRAO patients presenting within 24 hours, compared to a non-HBOT cohort.
Patients and methods: This retrospective cohort study included patients diagnosed with CRAO presenting within 24 hours from October 2003 to March 2022. Patients treated with intravenous recombinant tissue plasminogen activator (rt-PA) or experiencing treatment-related visual complications were excluded. Of 49 eligible patients, 17 underwent HBOT following the novel protocol, while 32 received standard care (non-HBOT).
Results: Baseline logMAR VA was 2.3 in both groups. At discharge, 76.5% of the HBOT group exhibited a VA improvement of at least 0.3 logMAR, compared to 40.6% in the non-HBOT group (p = 0.02). Mean logMAR VA at discharge was 1.4 ± 0.8 in the HBOT group and 2.0 ± 0.8 in the non-HBOT group. After one month, the mean logMAR VA remained at 1.4 ± 0.9 in the HBOT group and was 1.9 ± 0.9 in the non-HBOT group.
Conclusion: While constrained by the small sample size and short-term outcome data, these results showed the benefits of this unique HBOT protocol in CRAO presenting within the critical 24-hour window. Nevertheless, further prospective validation is necessary before widespread clinical adoption.
Keywords: central retinal artery occlusion, hyperbaric oxygen therapy, retinal artery occlusions, ophthalmic artery, CRAO, HBOT
Introduction
Central retinal artery occlusion (CRAO) is a rare ophthalmic emergency, sharing pathophysiological similarities with acute cerebral ischemia, affecting approximately 1 in 100,000 in adult population,1 but could result in devastating visual impairments, often declining to 20/400 or worse in most cases.2,3 The primary goal of CRAO management in acute settings is the restoration of retinal blood circulation and the enhancement of retinal cell oxygenation.
Although there are a variety of standard treatments for CRAO, their efficacy and associated complications pose significant challenges.4 Conventional interventions for restoring retinal circulation, including ocular massage, anterior chamber paracentesis (AC paracentesis), and intraocular pressure-lowering medications, lack evidence supporting significant visual improvement.4,5 Intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator (rt-PA) is most effective within the 4.5-hour therapeutic window,5–7 while intra-arterial thrombolysis (IAT) within 6 hours of symptom onset achieves visual improvement in 60–70% of cases. However, the utility of IVT and IAT beyond these timeframes is controversial due to the heightened risk of severe complications such as intracerebral and systemic hemorrhage.8–11 Oxygen therapy, including high concentration oxygen inhalation, and HBOT, provide additional oxygen to hypoxic retinal cells or those contraindicated for thrombolytic therapy, with potential advantages over conventional treatments. HBOT represents a potential adjunctive option for CRAO management; however, its use is constrained by the lack of randomized controlled trial evidence, the narrow therapeutic time window, significant logistical delays in accessing treatment facilities, and the resource‑intensive nature of therapy. HBOT may be considered in specific scenarios, such as in patients presenting outside the conventional therapeutic window or in those with contraindications to thrombolytic therapy; nevertheless, its efficacy in these contexts remains uncertain and is the subject of ongoing debate in the literature.
Despite the recommendation for HBOT, there is a variety of HBOT protocols in terms of variation of cut-off time, oxygen concentration, duration and frequency of each HBOT session.12 Previous studies have shown the superiority of HBOT over non-HBOT treatment for CRAO within an 8-hour window of symptom onset window.13 Additionally, a series of comparative studies within the Korean population illustrated improved visual outcomes with HBOT compared to non-HBOT in patients presenting within 24 hours.14 In Thailand, only one retrospective study exhibited improved results of HBOT in cases of CRAO, particularly in those who received HBOT within 24 hours of symptoms, without direct visual outcome comparisons of HBOT and non-HBOT.15 Within our institution’s clinical framework, HBOT is recommended for patients diagnosed with CRAO who present within the initial 24-hour window. This recommendation follows the implementation of Siriraj Hospital’s unique HBOT protocol for CRAO patients. This research seeks to offer a distinct practical HBOT protocol, aiming to enhance patient outcomes and offering an option for CRAO patients who present within 24 hours.
Methods
This retrospective chart review research obtained ethical approval by the Siriraj Institutional Review Board, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand (approval no. Si132/2021 on 17 February 2021 with yearly renewal until 16 February 2024), in accordance with the principles outlined in the Declaration of Helsinki (1964). Participant consent was waived by the Siriraj Institutional Review Board due to the retrospective nature of the study. All data were anonymized and maintained with confidentiality.
A retrospective comparative cohort study was conducted by systematically reviewing the medical records of all patients diagnosed with CRAO and subsequently admitted to Siriraj Hospital from October 2003 to March 2022. Patients who are at least 18 years of age and have experienced the onset of CRAO within 24 hours were included. The diagnosis of CRAO was made primarily based on clinical manifestations: acute painless visual loss, a marked decline in VA, with physical examination corresponding to CRAO such as retinal whitening or “cherry red spot” in the macular. Patients who underwent treatment with rt-PA or encountered complications adversely affecting VA after conventional CRAO therapy were excluded from the study.
A comprehensive dataset was collected, including demographic details such as age, sex and underlying medical conditions, timing of visual loss onset and VA: initial VA at presentation, at discharge, at one week and at one month after diagnosis. Furthermore, the initial treatment modalities administered including AC paracentesis, as well as alternative non-HBOT oxygen therapies and ocular massage were recorded.
The primary outcome measure of interest focused on determining the number of patients who exhibited a minimum improvement in VA of at least 0.3 logMAR (equivalent to three lines) at the point of discharge of the HBOT group compared to the non-HBOT. Secondary outcomes included calculating the mean VA values at discharge and one month after onset or for each group. Furthermore, complications from HBOT were also thoroughly assessed.
VA assessments were standardized using both the Snellen and Early Treatment Diabetic Retinopathy Study (ETDRS) charts. For the purpose of analysis, these measurements were uniformly converted to the logarithm of the minimal angle of resolution scale (logMAR) using a conversion formula derived from the NOD values of the United Kingdom (National Ophthalmology Database) values.16,17
Structural changes were evaluated using Spectralis spectral-domain optical coherence tomography (OCT) at the initial presentation and at the 1-month follow-up. Imaging with poor quality was excluded from the study. These structural changes were represented by the inner retinal thickness, defined as the vertical distance between the internal limiting membrane and the inner border of the outer plexiform layer. The overall mean thickness of each eye was calculated as the average of measurements, which were manually obtained from four quadrants: nasal, temporal, superior, and inferior—each at 750 μm from the fovea.
HBOT Protocol
The treatment protocol includes an HBOT session every 24 hours for five days regardless of VA changes. The initial session involves administering 2.0 ATA of 100% oxygen for 180 minutes, starting with a 15-minute descent, a 5-minute air break halfway through the session, and then a 15-minute ascent. Subsequent to the first session on the first day, HBOT is administered once a day for the next four days with each session 24 hours apart. During subsequent sessions, patients receive 2.4 ATA of 100% oxygen for 90 minutes, with a 5-minute air break interspersed within each session. The rationale for this HBOT protocol is comprehensively addressed in the discussion section.
Statistical Analysis
Demographic and baseline data were summarized using mean ± standard deviation, number and percentage. Pearson’s chi-square test and Fisher’s exact test were used to compare qualitative variables eg, proportion of patients with VA improvement (logMAR improve > 0.3) between two groups. Continuous data, such as the onset of vision loss and VA, were analyzed using the Mann–Whitney U-test. Due to repeated VA measurements over time, univariable and multivariable generalized estimation equations (GEE) were employed using an exchangeable correlation structure. Variables with univariable p-value less than 0.1 were entered in the multivariable analysis by GEE with independent variables of HBOT, AC paracentesis, time point (discharge, 1 week, 1 month), initial VA and onset hours. The comparison of VA at each time point (discharge, 1 week, 1 month) between the HBOT and non-HBOT groups was adjusted using Bonferroni correction for multiple comparisons. A p-value of less than 0.05 was considered statistically significant. Statistical analysis was performed using SPSS version 29.0.0 (IBM Corp., US).
Results
Patient Characteristics
The medical records of 67 patients diagnosed with CRAO between October 2003 and March 2022 were reviewed. Of these, 49 patients’ eyes were included in the study. Among these 49 patients, 17 received HBOT, while 32 were in the non-HBOT group. Fundus fluorescein angiography (FFA) was performed initially on 20 patients (9 in HBOT and 11 in non-HBOT), all of whom demonstrated at least delayed arm-to-retinal, arteriovenous (AV) transit, or arterial filling times. Additionally, 5 patients (2 in HBOT and 3 in non-HBOT) were clinically diagnosed CRAO with cilioretinal artery sparing and were confirmed by OCT. OCT was performed on 25 patients (13 in HBOT and 12 in non-HBOT), all of whom exhibited both inner retinal hyperreflectivity and thickening consistent with the acute phase of CRAO. The majority of patients in both groups received a similar CRAO standard of care (P > 0.05), with the three most common treatments: anti-glaucoma medications, AC paracentesis, and oxygen therapy. Initial visual acuity (VA) was comparable between groups (p = 0.55), with a mean of 2.3 ± 0.4 logMAR in the HBOT group and 2.3 ± 0.6 logMAR in the non-HBOT group. Furthermore, both groups showed a similar onset time of symptoms (p = 0.83), with the mean onset time for HBOT and non-HBOT patients being 11.6 ± 6.8 and 12.0 ± 6.8 hours, respectively.
VA Outcomes
At discharge, 76.5% of patients in HBOT experienced an improvement in VA of at least 3 lines, compared to 40.6% observed within non-HBOT (p = 0.02). The mean VA improvement (P <0.01) from initial presentation to discharge was 2.3 ± 0.4 to 1.4 ± 0.8 in the HBOT group, while in the non-HBOT group showed a modest change (P <0.01) from 2.3 ± 0.6 to 2.0 ± 0.8 logMAR (Figure 1). The HBOT demonstrated superior mean observed VA at discharge as compared to non-HBOT (p = 0.03). Additionally, the adjusted VA at discharge (mean ± S.E. logMAR) was significantly better in the HBOT group at 1.5 ± 0.1 compared to the non-HBOT group at 2.1 ± 0.1 (p = 0.01). However, despite the significant difference in mean VA improvement between the two groups, the proportion of patients achieving a VA of at least 6/60 remained relatively low in both groups—29.41% in the HBOT group and 15.6% in the non-HBOT group (p = 0.25). This lack of statistical significance suggests that while HBOT leads to meaningful overall VA improvement, its impact on achieving a functional VA threshold of 6/60 remains inconclusive.
 |
Figure 1 Comparison of mean visual acuity (LogMAR) at initial and discharge between HBOT and non-HBOT group. |
At 1-month appointment, 13 out of 17 patients (76.5%) in the HBOT group and 27 out of 32 patients (84.4%) in the non-HBOT group attended follow-up appointments. Although there were some patients who missed 1-month post-onset, the HBOT group still consistently demonstrated better VA compared to the non-HBOT group. The mean VA of HBOT at 1-week and 1-month were 1.5 ± 0.9 and 1.4 ± 0.9, while the non-HBOT remained 2.1 ± 0.8 and 1.9 ± 0.9 logMAR respectively. Significantly better adjusted mean VA were also observed in HBOT compared to the non-HBOT at both 1 week and 1 month (p = 0.01).
Structural Outcome
The mean inner retinal thickness, measured manually from four quadrants (nasal, temporal, superior, and inferior, each at 750 μm from the fovea), was 206.8 ± 44.5 μm in the HBOT group and 192.6 ± 52.2 μm in the non-HBOT group at the time of initial presentation (p = 0.646). At the 1-month follow-up, OCT data were available for 10 of 17 patients in the HBOT group and 9 of 32 patients in the non-HBOT group. The HBOT cohort demonstrated significantly less progression of ischemic changes, with a mean inner retinal thickness of 136.3 ± 35.1 μm, compared to 104.3 ± 29.9 μm in the non-HBOT cohort (p = 0.049). These findings suggest that HBOT may contribute to structural preservation of the retina by mitigating ischemic damage in patients with CRAO.
Visual Outcome Predictor
In the univariate analysis, both onset hours and initial VA were also identified as significant predictors of visual outcome. The multivariate GEE results revealed that HBOT, AC paracentesis, and the initial VA at presentation were statistically significant predictors of the final VA (Table 1). HBOT showed a coefficient of −0.59 (95% CI [−0.94, −0.25, p < 0.01), signifying that patients receiving HBOT encountered a post-treatment reduction in VA logMAR by 0.59. Similarly, for patients who received AC paracentesis, the coefficient was −0.42 (95% CI [−0.70, −0.15], p <0.01), suggesting that the final logMAR is reduced by 0.42 for those who had AC paracentesis. Furthermore, the initial VA that presented had a coefficient of 1.05 (95% CI [0.68, 1.43], p < 0.01), indicating that for every unit increase in the initial VA logMAR, the final logMAR worsens by 1.05 (the more logMAR indicates the worsening VA).
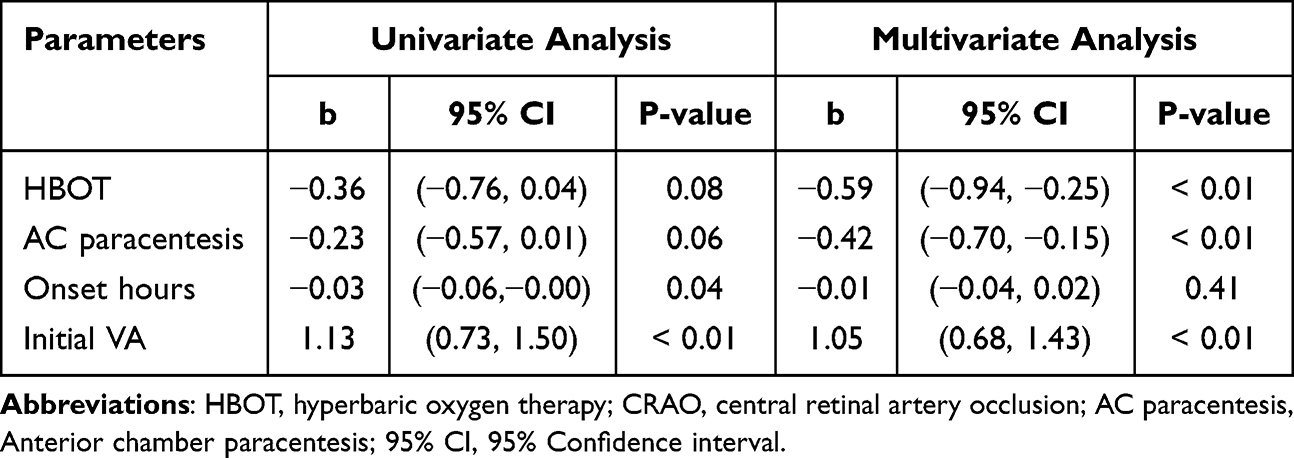 |
Table 1 Results From GEE of Visual Acuity at 3 Time Points |
Adverse Events
Although all patients underwent thorough safety evaluations prior to their initial HBOT session, adverse events were observed in 2 out of 17 patients (11.8%). One patient had headache, nausea, and vomiting before continuing to complete HBOT series, while the other experienced a generalized tonic-clonic seizure lasting one minute, which spontaneously resolved. A comprehensive evaluation was conducted to identify the cause of the seizure, revealing hypocalcemia as the only notable risk factor. Oxygen toxicity was considered the most likely etiology of the seizure. After a detailed discussion with the patient about the risks and benefits of continuing HBOT, the patient who experienced the seizure decided to terminate HBOT. During hospitalization, the patient received a short course of antiepileptic medication, which was carefully tapered prior to discharge. Importantly, both patients made a full recovery without the need for further intervention or long-term complications. No recurrence of headaches, seizures, or other adverse symptoms was reported during the follow-up period.
Discussion
Our study demonstrated a better outcome with HBOT compared to the non-HBOT group in CRAO patients who presented within 24 hours. Notably, no patients in our cohort had giant cell arteritis or other inflammatory etiologies, indicating that the study population predominantly consisted of non-arteritic CRAO cases. The number of patients with visual improvement of at least 3 lines was significantly higher in the HBOT group compared to the non-HBOT group (P < 0.02). Although both groups had comparable initial mean VA, the HBOT group demonstrated significantly better observed and adjusted mean VA compared to the non-HBOT group at discharge, as well as at the 1-week and 1-month follow-up assessments. However, despite this minimal superiority in the HBOT group, the mean VA at discharge remained at 1.4 ± 0.8 logMAR (approximately 6/150 Snellen equivalent), compared to 2.0 ± 0.8 logMAR (approximately counting fingers) in the non-HBOT group. The proportion of patients achieving a VA of at least 6/60 remained relatively low in both groups (p = 0.25). This lack of statistical significance suggests that while HBOT leads to meaningful overall VA improvement, its impact on achieving a functional VA threshold of 6/60 remains inconclusive. Nonetheless, while both values still fall below the 6/60 threshold defining legal blindness in many countries, even modest improvements in VA could contribute to a better quality of life for patients, allowing ability to perform daily tasks, and potentially increased independence.
Comparing the outcomes of HBOT for CRAO across studies by Hadanny et al (Israel),18 Menzel-Severing et al (Germany),19 and our own results reveals both similarities and differences. While there is some variation in baseline VA—with Hadanny et al reporting 2.1 ± 0.5 logMAR and Menzel-Severing et al reporting 1.8 ± 0.3 logMAR, compared to our baseline VA of 2.3 ± 0.4 logMAR—all studies show a similar improvement in VA at discharge: 1.6 ± 0.8 logMAR, 1.5 ± 0.5 logMAR, and 1.4 ± 0.8 logMAR, respectively.18,19 These consistent findings highlight the potential benefit of HBOT for CRAO patients, despite variations in baseline VA and racial differences between study populations.
However, it is important to note the differences in the mean time from symptom onset to treatment initiation. Hadanny et al reported a mean of 7.8 ± 3.8 hours, and Menzel-Severing et al reported 5.3 ± 2.9 hours,18,19 while our cohort had a significantly longer delay of 11.6 ± 6.8 hours. Despite this delay, the similar VA improvements suggest that HBOT may still be effective even in patients who present later, reinforcing its potential as a treatment option for CRAO.
According to the results obtained by GEE, HBOT is a statistically significant predictor of visual outcome (P < 0.01). Kim et al demonstrated significantly greater visual improvement in patients who received HBOT compared to those who did not more than 1 month after treatment.14 Further GEE analysis revealed that the onset time surprisingly was not a significant predictor of the VA outcome (p = 0.41) of patients with CRAO who onset within 24 hours, which was similar to Rozenberg’s study.20 Rozenberg’s study also suggested a lack of correlation between the timing of the first HBOT session and the final VA outcome between the HBOT and non-HBOT group with presentation less than 24 hours.20 Therefore, this offers an opportunity for patients with CRAO who present within this time frame. However, this discrepancy contrasts with the findings of Hayreh et al’s monkey central artery clamping experiment, which demonstrated that occlusion for 4 hours or more led to total or near-total optic nerve damage.21 The variation in VA observed in our study may be explained by differences in the pathophysiology of CRAO, which often results in incomplete artery occlusion, rather than the direct clamping used in the experimental model. CRAO typically presents either partially or as completely developed but temporary, with varying degrees of reperfusion that may be intermittent or sustained. This variability is often due to transient arterial spasms or the resolution of emboli or thrombi, which allows for periods of retinal blood perfusion beyond the time frame observed in the monkey experiment.22,23 Additionally, anatomical differences in the blood supply of the human eye may not be accurately reflected by primate models, further contributing to the observed discrepancies.22,23 Further analysis of anatomical changes, as suggested by the experiment by Hayreh et al, may provide a more objective evaluation. Despite several studies that recommended the initiation of HBOT within 12 hours24 of CRAO diagnosis or even as early as 6 to 8 hours.13,25 Our findings suggest that HBOT could remain a viable treatment option for patients presenting within 24 hours, even with delayed initiation of therapy.
In the GEE analysis, both HBOT and AC paracentesis were the significant predictors of VA outcomes, with coefficients of -0.59 and -0.42, respectively. AC paracentesis may be worth considering as a complementary intervention for patients undergoing HBOT. However, as the majority of patients in our cohort received AC paracentesis, the subgroup analysis of patients treated exclusively with HBOT is limited by the small sample size. With our result alone, it remains inconclusive whether the observed VA improvement can be attributed solely to HBOT. However, when compared to a study evaluating the efficacy of AC paracentesis in CRAO,26 where patients who underwent paracentesis within 7–24 hours (mean onset: 15.3 ± 6.3 hours) demonstrated a minimal improvement in baseline VA from 1.99 ± 0.25 logMAR to 1.92 ± 0.3 logMAR at 3 days post-intervention, the results in our cohort are notably different. In our study, 76.5% of patients in the HBOT group also received AC paracentesis, and patients exhibited more improvement in VA, from 2.3 ± 0.4 logMAR to 1.4 ± 0.8 logMAR at discharge. This raises the possibility that the observed VA improvement could be primarily attributed to HBOT rather than AC paracentesis alone. Nonetheless, further investigations, including direct comparisons between standard CRAO treatments and HBOT, are required to elucidate the specific contributions of each intervention.
Retinal structural analysis using OCT demonstrated significantly less progression of ischemic changes, as evidenced by less reduced inner retinal thinning at 1 month, in CRAO patients who received HBOT compared to non-HBOT group. In CRAO, the inner retina, which relies predominantly on the central retinal artery for oxygen, becomes ischemic due to the arterial occlusion.27 HBOT mitigates this ischemia by increasing the amount of dissolved oxygen in plasma,28 enabling oxygen to diffuse from the choroidal circulation and peripheral retina into the ischemic central retina. This oxygen diffusion supports critical retinal layers, including ganglion cells, the inner plexiform layer, and the inner nuclear layer. Although HBOT does not restore blood flow through the occluded artery, the elevated plasma oxygen levels allow oxygen to bypass the blockage and reach ischemic tissues via diffusion from adjacent capillaries and non-occluded vessels.29 This process temporarily preserves retinal function during the acute phase of CRAO, providing crucial support while awaiting natural recanalization.
While the observed preservation of inner retinal thickness at 1 month is statistically significant, larger sample sizes are needed to confirm the structural benefits of HBOT with greater reliability. Additionally, combining structural imaging with functional assessments, such as electroretinography or visual field, could provide a more comprehensive evaluation of retinal recovery, capturing functional improvements that may not be evident through structural analysis alone.
Although the outer retina, primarily supplied by the choroidal circulation, is less affected by CRAO, it still benefits from the increased oxygenation provided by HBOT. The photoreceptors, which have high metabolic demands, are supported by the enhanced oxygen delivery from the choroid.27 Furthermore, by maintaining the function of the retinal pigment epithelium and outer retinal layers, HBOT helps preserve overall retinal integrity, preventing secondary degeneration that could result from inner retinal ischemia.
Adverse Events
The primary complications associated with HBOT are barotrauma and oxygen toxicity. Middle ear barotrauma is frequently documented in various studies, with an incidence ranging from approximately 9% to 27%.15,30,31 However, in our study, none of our patients experienced barotrauma complications. Of all the patients in our study, only two encountered HBOT-related problems. One patient developed headache, nausea, and vomiting after the third session of HBOT, while another experienced a generalized tonic-clonic seizure during the first session. While central nervous system oxygen toxicity was considered a potential etiology, but the patient’s underlying hypocalcemia might be a possible contributing factor for the seizure. Importantly, both patients made a full recovery without requiring additional treatment or experiencing further complications. Notably, among patients who underwent HBOT under standardized conditions, no serious adverse events were observed.
HBOT Protocol discussion
Our inclusion criterion was set at 24 hours from the onset of symptoms, based on the physiology of retinal circulation. Studies on central retinal artery clamping in monkeys suggest that irreversible damage occurs after 4 hours.21 However, multiple studies12,18,32–34 have shown improvements in VA following HBOT, even when initiated days after the event. This could be attributed to the incomplete occlusion nature of CRAO, which differs from the total retinal artery clamping in the monkey model. Importantly, the majority of cases with favorable visual outcomes began treatment within the first day.12 Given the time required for hyperbaric chamber preparation, team mobilization, patient evaluation for HBOT, and standard interventions such as ocular massage and AC paracentesis, the 24-hour window from symptom onset to the initiation of HBOT was adopted as the cut-off point.
Commenting on the HBOT protocol, there exist a variety of HBOT protocols and recommendations concerning the number of sessions required. Some HBOT protocols suggest continuing HBOT sessions until VA improvement reaches a plateau.12 However, we have adopted a fixed protocol consisting of a HBOT session with a 5-minute air break in the middle, conducted every 24 hours for a total of 5 days regardless of change in VA as natural recanalization typically occurs within 72 hours.35 CRAO patients particularly benefit from HBOT in the acute phase, as early intervention is crucial to mitigate cellular necrosis during the critical period of ischemia while awaiting spontaneous recanalization. Thus, the HBOT protocol is limited to the initial 5-day period, postulating that extending therapy beyond this window may yield diminishing returns, as irreversible retinal damage may have already occurred. This approach helps in conserving human resources by reducing the need for repeated VA evaluations, particularly during non-office hours when medical staff are limited. The fixed protocol also enhances HBOT schedule management, particularly when sharing HBOT with other departments. Additionally, this standardized number of sessions has a consistent 5 days endpoint which ensures the predictability of treatment costs.
There are variations of HBOT protocol ranging from 1.5 ATA to 3 ATA,12,34 which mostly yield VA improvements. Given that most patients with CRAO are elderly, they may struggle to tolerate increased atmospheric pressure, potentially leading to barotrauma or seizures due to oxygen toxicity. Our protocol then starts with the lower initial session at 2 ATA to mitigate the risk of oxygen toxicity, while compensating for oxygen supply by the longer duration at 180 minutes, followed by subsequent days with sessions lasting 90 minutes at 2.4 ATA.
Although several studies have addressed retinal artery vasoconstriction as a consequence of hyperoxia,36 in general, the positive effects of HBOT outweigh the vasoconstriction effects. Vasoconstriction typically occurs only if the cell is adequately perfused, making it less likely to manifest in the acute phase of CRAO. Oxygen is delivered in two ways in the blood: a bound fraction of hemoglobin and a dissolved free fraction in plasma.28 In a normal environment, 99% of hemoglobin is loaded with oxygen, whereas the free fraction of oxygen in plasma is relatively small. In HBOT, the dissolved free fraction is significantly elevated, which supplies the ischemic area as an additional oxygen supply independently of saturated hemoglobin.29 In addition to the vascular supply, aquaporin-1 (AQP-1), water channels can serve as another alternative oxygen transporter between cells.37
Furthermore, the 24-hour interval between each session is intended to stimulate the hyperoxic-hypoxic paradox, where intermittent hypoxia triggers a cascade of tissue survival regulations under limited oxygen without the hazardous effects of hypoxemia. During the 24-hour rest period, the lower oxygen stimulates the hypoxic inducible factor transcription factor (HIF), which regulates more than 100 genes necessary for cellular survival under oxygen-deprived conditions.38 This improves the cell’s ability to synthesize adenosine triphosphate irrespective of oxygen dependence, while inducing vascular endothelial growth factor (VEGF) to improve angiogenesis for long-term cell survival.19,39
In general, our HBOT protocol represents a potential framework for a structured approach designed to improve outcomes for CRAO patients. It focuses on minimizing adverse events related to oxygen toxicity and maximizing the hypoxic response, aligning with cellular adaptation physiology in low-oxygen environments. Additionally, it maintains practicality within healthcare settings. Although further research is required to improve our understanding, our HBOT protocol presents an intriguing option, especially for patients with CRAO who present within 24 hours.
Limitations
While our results suggested a trend toward improved outcomes in the HBOT group compared to the non-HBOT group, there were several limitations to consider. These include a small sample size, lack of long-term outcomes, and unregulated administration of adjunctive treatments between the two groups due to the retrospective nature of our study design. As our hospital serves as a tertiary facility, some patients were referred back to their initial hospital for long-term follow-up after acute-phase treatment, resulting in missing information, particularly regarding VA at 1 month. The difference in our 1-month VA outcomes might have been more pronounced with a larger sample size. Additionally, our diagnosis of CRAO was based on typical clinical manifestations, supplemented by OCT and/or FFA in some cases, but without fully standardized, objective imaging-based diagnostic criteria as used in certain clinical trials. The exclusion of poor-quality OCT images was determined subjectively without predefined quantitative thresholds, and manual measurement of inner retinal thickness, even when divided into quadrants, may introduce inter-observer variability and potential measurement bias. Furthermore, the reduced follow-up adherence at 1 month, particularly in OCT data acquisition could limit the robustness of our structural outcome analysis. Although our study groups demonstrated a balanced standard of care with a P-value greater than 0.05 (Table 2), indicating uniformity in treatments including ocular massage, AC paracentesis, and the administration of antiglaucoma medications, these management practices could potentially affect the final visual acuity results. Due to the limited number of patients in each group who did not receive standard CRAO treatments, conducting a subgroup analysis for isolated HBOT treatment was not feasible. Therefore, a study design with more standardized diagnostic protocols, objective image quality criteria, and better control of standard of care—while addressing the challenges posed by the emergency nature of CRAO—represents an important avenue for future research.
 |
Table 2 Baseline Characteristics of CRAO Patients with HBOT and Non-HBOT, n (%) |
Summary
This retrospective study showed the efficacy and safety of HBOT in patients with CRAO who presented within 24 hours of symptom onset. Patients who received HBOT demonstrated better outcomes, including visual improvement and structural change, than non-HBOT. Our fixed HBOT protocol is practical and feasible to implement in clinical practice. While limited by a small sample size and short-term follow-up, this study provides preliminary evidence that HBOT could be considered as a potential treatment option for CRAO patients presenting within 24 hours of onset.
Institutional Review Board Statement
This research was approved by Siriraj Institutional Review Board, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand (approval no. Si132/2021 on 17 February 2021 with yearly renewal until 16 February 2024), in accordance with the principles outlined in the Declaration of Helsinki (1964).
Data Sharing Statement
All datasets generated or analyzed during this study are included in this published article. The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Informed Consent Statement
This retrospective chart review research obtained ethical approval, which the requirement for informed consent was waived by the Institutional Review Board.
Acknowledgment
We would like to thank Asst. Prof. Dr. Chulaluk Komoltri for her invaluable support and expertise in statistical consultation throughout this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
All authors hereby declare that no funding was received for this research.
Disclosure
The authors declare no competing interests in this work.
References
1. Leavitt JA, Larson TA, Hodge DO, Gullerud RE. The incidence of central retinal artery occlusion in Olmsted County, Minnesota. Am J Ophthalmol. 2011;152(5):820–3e2. doi:10.1016/j.ajo.2011.05.005
2. Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005;140(3):376–391. doi:10.1016/j.ajo.2005.03.038
3. Shah R, Zheng X, Patel AP, Bhatti MT, Gilbert A, Vora RA. Central retinal artery occlusion: visual outcomes from a Large Northern California cohort. Ophthalmol Retina. 2024;8(6):566–570. doi:10.1016/j.oret.2023.12.007
4. Roskal-Walek J, Ruzik A, Kubis N, et al. Therapeutic strategies for retinal artery occlusion-a literature review. J Clin Med. 2024;13(22). doi:10.3390/jcm13226813.
5. Mac Grory B, Nackenoff A, Poli S, et al. Intravenous fibrinolysis for central retinal artery occlusion: a cohort study and updated patient-level meta-analysis. Stroke. 2020;51(7):2018–2025. doi:10.1161/STROKEAHA.119.028743
6. Mac Grory B, Schrag M, Biousse V, et al. Management of central retinal artery occlusion: a scientific statement from the American heart association. Stroke. 2021;52(6):e282–e94. doi:10.1161/STR.0000000000000366
7. Schrag M, Youn T, Schindler J, Kirshner H, Greer D. Intravenous fibrinolytic therapy in central retinal artery occlusion: a patient-level meta-analysis. JAMA Neurol. 2015;72(10):1148–1154. doi:10.1001/jamaneurol.2015.1578
8. Chen CS, Lee AW, Campbell B, et al. Efficacy of intravenous tissue-type plasminogen activator in central retinal artery occlusion: report from a randomized, controlled trial. Stroke. 2011;42(8):2229–2234. doi:10.1161/STROKEAHA.111.613653
9. Hayreh SS, Zimmerman MB, Kimura A, Sanon A. Central retinal artery occlusion. Retinal survival time. Exp Eye Res. 2004;78:723–736. doi:10.1016/S0014-4835(03)00214-8
10. Mac Grory B, Lavin P, Kirshner H, Schrag M. Thrombolytic therapy for acute central retinal artery occlusion. Stroke. 2020;51(2):687–695. doi:10.1161/STROKEAHA.119.027478
11. Schumacher M, Schmidt D, Jurklies B, et al. Central retinal artery occlusion: local intra-arterial fibrinolysis versus conservative treatment, a multicenter randomized trial. Ophthalmology. 2010;117(7):1367–75e1. doi:10.1016/j.ophtha.2010.03.061
12. Murphy-Lavoie H, Butler FK, Hagan C. Arterial insufficiencies: central retinal artery occlusion. Undersea Hyperb Med. 2022;49(4):533–547. doi:10.22462/07.08.2022.12
13. Beiran I, Goldenberg I, Adir Y, Tamir A, Shupak A, Miller B. Early hyperbaric oxygen therapy for retinal artery occlusion. Eur J Ophthalmol. 2001;11(4):345–350. doi:10.1177/112067210101100405
14. Kim YS, Nam MS, Park EJ, et al. The effect of adjunctive hyperbaric oxygen therapy in patients with central retinal artery occlusion. Undersea Hyperb Med. 2020;47(1):57–64. doi:10.22462/01.03.2020.7
15. Kraisornpornsan CVT, Kedkovid N. Outcomes of hyperbaric oxygen therapy for central retinal artery occlusion in Somdech Phra Pinklao Hospital. Chula Med J. 2023;64:307–14.
16. Day AC, Donachie PH, Sparrow JM, Johnston RL. The Royal College of Ophthalmologists’ National Ophthalmology Database study of cataract surgery: report 1, visual outcomes and complications. Eye. 2015;29(4):552–560. doi:10.1038/eye.2015.3
17. Moussa G, Bassilious K, Mathews N. A novel excel sheet conversion tool from Snellen fraction to LogMAR including ‘counting fingers’, ‘hand movement’, ‘light perception’ and ‘no light perception’ and focused review of literature of low visual acuity reference values. Acta Ophthalmol. 2021;99(6):e963–e5. doi:10.1111/aos.14659
18. Hadanny A, Maliar A, Fishlev G, et al. Reversibility of retinal ischemia due to central retinal artery occlusion by hyperbaric oxygen. Clin Ophthalmol. 2017;11:115–125. doi:10.2147/OPTH.S121307
19. Menzel-Severing J, Siekmann U, Weinberger A, Roessler G, Walter P, Mazinani B. Early hyperbaric oxygen treatment for nonarteritic central retinal artery obstruction. Am J Ophthalmol. 2012;153(3):454–9e2. doi:10.1016/j.ajo.2011.08.009
20. Rozenberg A, Peled A, Hadad A, et al. Hyperbaric oxygen treatment for non-arteritic central retinal artery occlusion retrospective comparative analysis from two tertiary medical centres. Eye. 2022;36(6):1261–1265. doi:10.1038/s41433-021-01617-8
21. Hayreh SS, Jonas JB. Optic disk and retinal nerve fiber layer damage after transient central retinal artery occlusion: an experimental study in rhesus monkeys. Am J Ophthalmol. 2000;129(6):786–795. doi:10.1016/S0002-9394(00)00384-6
22. Tobalem S, Schutz JS, Chronopoulos A. Central retinal artery occlusion - rethinking retinal survival time. BMC Ophthalmol. 2018;18(1):101. doi:10.1186/s12886-018-0768-4
23. Singh S, Dass R. The central artery of the retina. I. Origin and course. Br J Ophthalmol. 1960;44(4):193–212. doi:10.1136/bjo.44.4.193
24. Butler FK Jr, Hagan C, Murphy-Lavoie H. Hyperbaric oxygen therapy and the eye. Undersea Hyperb Med. 2008;35(5):333–387.
25. Wu X, Chen S, Li S, et al. Oxygen therapy in patients with retinal artery occlusion: a meta-analysis. PLoS One. 2018;13(8):e0202154. doi:10.1371/journal.pone.0202154
26. Fieb A, Cal Ö, Kehrein S, Halstenberg S, Frisch I, Steinhorst UH. Anterior chamber paracentesis after central retinal artery occlusion: a tenable therapy? BMC Ophthalmol. 2014;14:28. doi:10.1186/1471-2415-14-28
27. Forrester JV, Dick AD, McMenamin PG, Roberts F, Pearlman E. Chapter 1 - Anatomy of the eye and orbit. In: Forrester JV, Dick AD, McMenamin PG, Roberts F, Pearlman E, editors. The Eye.
28. Trayhurn P. Oxygen-A Critical, but overlooked, nutrient. Front Nutr. 2019;6:10. doi:10.3389/fnut.2019.00010
29. Hadanny A, Efrati S. The hyperoxic-hypoxic paradox. Biomolecules. 2020;10(6):958. doi:10.3390/biom10060958
30. hadanny A, Meir O, Bechor Y, Fishlev G, Bergan J, Efrati S. The safety of hyperbaric oxygen treatment--retrospective analysis in 2334 patients. Undersea Hyperb Med. 2016;43(2):113–122.
31. Grory M. Correction to: management of central retinal artery occlusion: a scientific statement from the American Heart Association. Stroke. 2021;52(6):e309. doi:10.1161/STR.0000000000000374
32. Tang PH, Engel K, Parke DW. Early Onset of Ocular neovascularization after hyperbaric oxygen therapy in a patient with central retinal artery occlusion. Ophthalmol Ther. 2016;5(2):263–269. doi:10.1007/s40123-016-0064-4
33. Cope A, Eggert JV, O’Brien E. Retinal artery occlusion: visual outcome after treatment with hyperbaric oxygen. Diving Hyperb Med. 2011;41(3):135–138.
34. Maldonado F, Reis da Silva A, Ar R, et al. Effects of hyperbaric oxygen therapy in the treatment of patients with central retinal artery occlusion: a retrospective study. Cureus. 2024;16(8):e66196. doi:10.7759/cureus.66196
35. Murphy-Lavoie H, Butler F, Hagan C. Central retinal artery occlusion treated with oxygen: a literature review and treatment algorithm. Undersea Hyperb Med. 2012;39(5):943–953.
36. Saltzman HA, Hart L, Sieker HO, Duffy EJ. Retinal vascular response to hyperbaric oxygenation. JAMA. 1965;191(4):290–292. doi:10.1001/jama.1965.03080040032007
37. Echevarria M, Munoz-Cabello AM, Sanchez-Silva R, Toledo-Aral JJ, Lopez-Barneo J. Development of cytosolic hypoxia and hypoxia-inducible factor stabilization are facilitated by aquaporin-1 expression. J Biol Chem. 2007;282(41):30207–30215. doi:10.1074/jbc.M702639200
38. Minet E, Ernest I, Michel G, et al. HIF1A gene transcription is dependent on a core promoter sequence encompassing activating and inhibiting sequences located upstream from the transcription initiation site and cis elements located within the 5’UTR. Biochem Biophys Res Commun. 1999;261(2):534–540. doi:10.1006/bbrc.1999.0995
39. Haase VH. Regulation of erythropoiesis by hypoxia-inducible factors. Blood Rev. 2013;27(1):41–53. doi:10.1016/j.blre.2012.12.003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.