Back to Journals » Clinical Optometry » Volume 12
Visual Impairment and Blindness in Saudi Arabia’s School for the Blind: A Cross-Sectional Study
Authors Alabdulwahhab KM ![]() , Ahmad MS
, Ahmad MS ![]()
Received 30 May 2020
Accepted for publication 5 August 2020
Published 7 October 2020 Volume 2020:12 Pages 169—173
DOI https://doi.org/10.2147/OPTO.S265293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Khalid M Alabdulwahhab,1 Mohammad S Ahmad2
1Department of Opthalmology, College of Medicine, Majmaah University, Al Majmaah 11952, Saudi Arabia; 2Department of Community Medicine/ Public Health, College of Medicine, Majmaah University, Al Majmaah 11952, Saudi Arabia
Correspondence: Mohammad S Ahmad
Department of Community Medicine/ Public Health, College of Medicine, Majmaah University, Al Majmaah 11952, Saudi Arabia
Email [email protected]
Aim: Visual impairment and blindness are important global health issues as they are associated with high morbidity, mortality, and decreased quality of life, leading to substantial economic loss and productivity. There are only a few published articles on vision impairment and blindness in Saudi Arabia to compare the range of estimated global prevalence of low vision, blindness, and their causes. This study aims to find out the important causes of vision impairment and blindness in schools for the blind in Qassim province, Saudi Arabia.
Methods: The cross-sectional study was conducted at the blind schools in Buraidah city of Qassim province. A total of 278 registered cases were included in this study using a systematic random sampling of registered cases. Based on the definitions, the cases were classified as having vision impairment and/or blindness. The data were entered and analyzed using IBM SPSS 25.
Results: The mean age was 30 years (range: 6 to 83 years) and 174 (76.4%) were males and 84 (32.6%) being females. The male:female ratio was 2:1. All the respondents were of Saudi ethnicity. Mild to moderate visual impairment was found in 6%, severe visual impairment in 27%, and blindness was seen in 64% of registered cases. The causes of blindness in these registered cases from blind school were retinitis pigmentosa (26%), optic atrophy (16%), glaucoma (7%), head trauma (6%), nystagmus (6%), retinopathy of prematurity (6%), ocular albinism (4%), corneal opacities (4%), amblyopia (3%) and other causes (22%). Overall, retinal disorders (retinitis pigmentosa and retinopathy of prematurity) were the leading causes of disability followed by optic atrophy.
Conclusion: The findings of this study are useful in planning and implementing screening programs in this area for early identification and corrections, thus preventing permanent loss of sight.
Keywords: vision disability, blindness, Qassim, Saudi Arabia
Introduction
Visual impairment and blindness are important global health issues because they are associated with increased morbidity, decreased quality of life leading to substantial economic and productivity loss. Vision impairment and blindness are the 6th in the world’s major causes of loss of wellbeing. Vision impairment has a significant economic impact on the individual, family, community, and the nation of which they are part. Visual impairment increases three-fold with every decade of life after the age of 40 years.1
Although eye diseases can affect anybody most commonly it is children and elderly people who are at more risk of developing age-related vision disabilities.2 Low vision and blindness have a deep impact on demographic, socioeconomic, and cultural differences. Also, the causes of incidence and prevalence in different ages vary but most of them can be preventable if screening is done in early stages.3
At the community level, we need reliable information on incidence, prevalence, severity, and causes of visual impairment which is of great importance for planning administration at health-care management to implement and measure the outcome of programs on prevention and treatment.
We must also lend a helping hand to our government and our ophthalmological society to know the exact causes and prevalence of low vision and blindness. To best of our knowledge, there are only a few published articles on blindness in schools for blinds in Saudi Arabia. With this background, we decided to conduct this study on prevalence and to know the major causes of vision impairment and blindness in school for blinds in the Qassim region.
Subjects/Materials and Methods
Qassim province is one of the thirteenth administrative provinces of Saudi Arabia. Qassim is the seventh-highest populated province of Saudi Arabia (population: 1,215,858). More than 400 towns, cities, villages, and Bedouin settlements serve this province. Buraidah is the capital of Qassim province. A cross-sectional prevalence study was conducted in blind schools in Buraidah. A total of 278 registered cases of vision impairment and blindness from the blind schools were included in this study. The duration of the study was about 5 months. The data on age, gender, causes of eye diseases were collected using a predesigned proforma.
We used WHO criteria (ICD-9-CM, 1996) to assess and classify Vision impairment and blindness.4 Visual impairment is defined as per 10th version of the international classification of diseases (ICD-10, 2010) and vision-related problems according to visual acuity at the time of study.5
- “Blindness” Is defined as visual acuity of less than 3/60.
- “Severe visual impairment” is defined as visual acuity between 6/60 and 3/60.
- “Moderate visual impairment” Is defined as visual acuity of less than 6/18 to 6/60.
- Vision impairment include both moderate and severe vision impairment.
Statistical Analysis
The data were entered and analyzed using IBM SPSS 25. Mean ± SD is given for quantitative variables, whereas, qualitative variables are expressed as frequencies, percentages, and graphs.
Ethical Approval
A prior written approval was obtained from the school of blindness for sharing of the data on the condition that anonymity would be maintained. This study was conducted in accordance with the Declaration of Helsinki Ethical Principles and Good Clinical Practices and was approved at each site by an independent local ethics committee of Majmaah University, KSA vides reference no: MUREC April 02/COM-2016.
Results
The mean age of included subjects of this study was 30 years (range: 6 to 83 years) and 174 (76.4%) were males and 84 (33.6%) were females as shown in Table 1. The ratio of male to female was 2:1. All the respondents were of Saudi ethnicity. The percentage of the registered cases in Qassim province following the severity of vision impairment is shown in Table 2. Hence the prevalence of blindness was found be to higher in the Saudi population among the registered cases. The causes of blindness are shown in Figure 1. The blindness due to retinitis pigmentosa and optic atrophy were high in our study population. The prevalence of vision impairment which includes both low vision and blindness and the education/employment status among our study population is shown in Figure 2. The prevalence rate was comparatively higher in the student population.
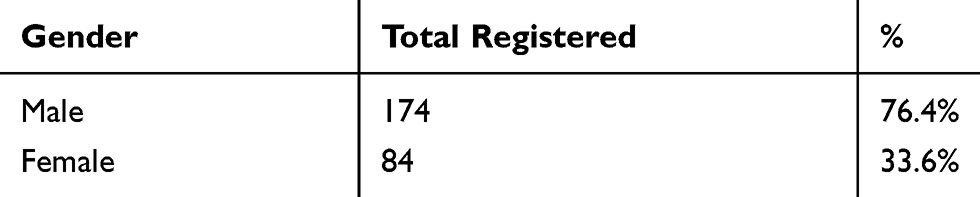 |
Table 1 Gender Wise Distribution Among the Study Population |
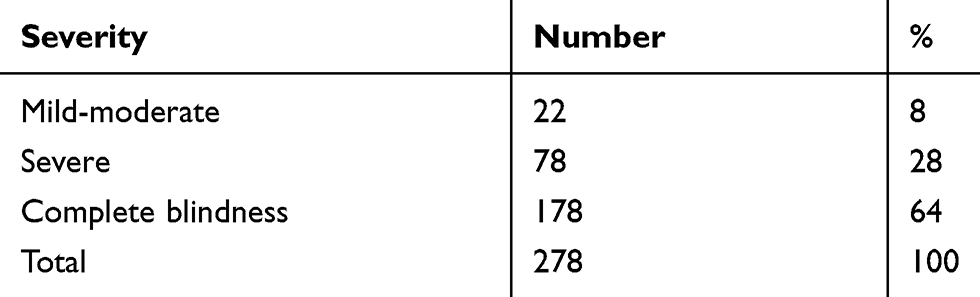 |
Table 2 Percentage of Registered Cases Following Visual Impairment Severity |
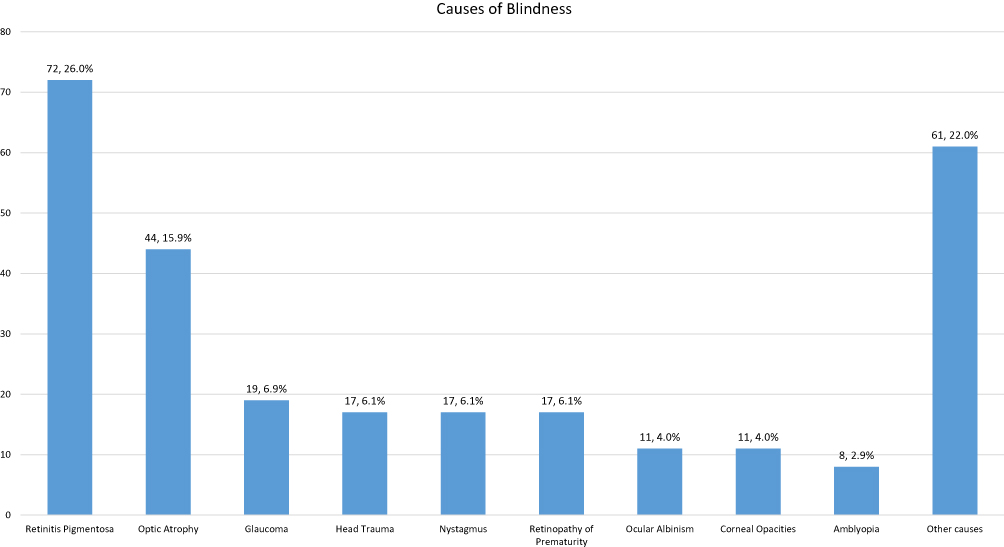 |
Figure 1 Causes of Blindness among the study population. |
 |
Figure 2 Prevalence percentages of visual impairment by the occupation. |
The present study included a sample size of 278 subjects with the mean age of 30.1 ± 16.1 years range (6 to 83 years). All the respondents were of Saudi ethnicity. Among 278 persons, 174 (76.4%) males and 84 (33.4%) females, were registered as blind in the blind school which is located in Buraidah. The age, gender, and severity of disability were also studied. The prevalence of low vision and blindness was more in males than females in all age groups. The most important causes for blindness among patients aged more than 30 years of age in our study were retinitis pigmentosa and optic atrophy.
Discussion
The present study was conducted to estimate the prevalence of blindness and their major causes among the Saudi population of the Qassim region. Blind school studies although easy to conduct are biased, as they do not represent blinds in the concerned population. In developing countries, only about 10% of blind children are in blind schools.6 Despite that, these studies provide valuable information on the causes of blindness.
A study carried out in visually impaired children aged between 5 and 16 years from four blind schools from a city in North India, noted major causes of severe visual impairment and blindness were microphthalmos (34.44%), corneal scar (22.23%), anophthalmos (14.45%) and pseudophakia (6.67%).7 On the contrary, the major causes of blindness in our study were retinitis pigmentosa (25.8%), optic atrophy (15.8%), and glaucoma (17%).
Retinitis pigmentosa, a hereditary progressive retinal dystrophy was the most important cause of blindness in our study this has been addressed by Tabbara and Badr when they found that genetic diseases account for 84% in people born after 1962.8,9 Later studies from Kuwait, Lebanon, and Jordan support the same fact.3,10,11
This might be explained the effort made by the government to treat infectious and other treatable eye diseases while consanguinity is still prevalent in the Saudi culture.
Our data showed the prevalence rates for the major causes of disability in all age groups and both genders. The prevalence rate for males was two to three times more than female patients. In optic atrophy, a similar finding was noted by a study done in Kuwait.3 In our current study, optic atrophy (16%) was the second common cause followed by retinal disorders. Our findings are well supported by an Iran study that reported optic nerve diseases as the second most common etiology of visual impairment among patients referred to visual rehabilitation clinics.12
Our findings differ from a study conducted among 4700 patients attending rehabilitation centers in Tubingen of Germany. In that study age-related macular degeneration (ARMD) was the most important cause of low vision (40%), followed by optic nerve atrophy and Diabetic retinopathy as other important causes. This might be since our study sample is young.13
Tsai et.al, in their study, analyzed the registry of patients identified by the Department of Social Welfare among patients having vision impairment and blindness, 55.8% had vision impairment and 44.2% were blind.14 The important causes of vision impairment and blindness were glaucoma, optic neuropathy, diabetes retinopathy, retinitis pigmentosa, ARMD, and myopic macular degeneration. The authors also noted that vision impairment and blindness were low below the age of 50 years. Those in the 50- and 64-years age group, diabetic retinopathy was the leading cause of blindness followed by glaucoma.10
In our study, retinal diseases were the most common causes (32%) low vision (retinitis pigmentosa 26% and Retinopathy of prematurity 6%). This can be explained as retinal diseases are less amenable to treatment and are irreversible compared to other eye disorders. The findings of this study compare well with other studies conducted in India, Tehran, Brazil, Thailand, Germany and in the Netherlands which identified retinal disorders as the most common cause of blindness.13,15–18 Anterior segment disorders were a more common cause of vision loss in studies performed in Uganda and Ethiopia which might reflect a high prevalence of infectious diseases and vitamin A deficiencies in these states.19,20
As our study was conducted among the students in the school of blind, the two common diseases which are the important cause of low vision (cataract and refractive error) was not seen as a major cause of vision loss in our study population. This finding is explained by the fact that these are treatable causes.
Our sample size (278) is comparable to other similar studies with a sample size (217, 360, 362) conducted in schools for blindness in Riyadh, Ethiopia and Iran respectively and might provide valuable guidelines for setting up of research and eye care services for the community.21–23
Conclusion and Limitation
This study identified the most common irreversible and untreatable causes of vision impairment in our province and helps plan to frame screening programs for the establishment.
The findings of this study can be used for the effected groups to create and framing guidelines on the establishment of rehabilitation clinics for affected peoples. As this study was conducted in the only school of the entire region the beneficiary number is on the lesser side and more robust studies covering the rest of the regions of the country could help in giving us a larger picture.
Acknowledgments
Authors acknowledge the Majmah University for given the permission to conduct this research.
Funding
The authors extend their appericiation to the Deanship of Scientific Research at Majmaah University for funding this research work under project number (R- 1441-151).
Disclosure
The authors have no conflicts of interest for this work.
References
1. Focus on Low Vision 2007 - Centre For Eye Research Australia. Available from: http://www.cera.org.au/uploads/CERA_FocusLowVision.pdf.
2. World Health Organization. Visual impairment and blindness. Fact sheet N°282; 2013. Available from: http://www.who.int/mediacentre/factsheets/fs282/en/.
3. Al-Merjan JI, Pandova MG, Al-Ghanim M, Al-Wayel A, Al-Mutairi S. Registered blindness, and low vision in Kuwait. Ophthalmic Epidemiol. 2005;12(4):251–257. doi:10.1080/09286580591005813
4. United States Department of Health and Human Services. The International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM).
5. World Health Organization. International statistical classification of diseases and related health problems 10th revision (ICD-10) version for 2010 chapter (VII H54) visual impairment including blindness (binocular or monocular). Available from: http://apps.who.int/classifications/icd10/browse/2010/en#/H54.
6. Gogate P, Kalua K, Courtright P. Blindness in childhood in developing countries: time for a reassessment? PLoS Med. 2009;6(12):e1000177. doi:10.1371/journal.pmed.1000177
7. Bhalerao SA, Tandon M, Singh S, Dwivedi S, Kumar S, Rana J. Visual impairment and blindness among the students of blind schools in Allahabad and its vicinity: a causal assessment. Indian J Ophthalmol. 2015;63:254–258. doi:10.4103/0301-4738.156930
8. Tabbara KF, Badr I. Changing pattern of childhood blindness in Saudi Arabia. Br J Ophthalmol. 1985;69:312–315. doi:10.1136/bjo.69.4.312
9. Al Salem M, Rawac HN. Pattern of childhood blindness and partial sight among Jordanians in two generations. J Pediatr Ophthalmol Strabismus. 1992;29:361–365.
10. Mansour AM, Kassak K, Chaya M, et al. National survey of blindness and low vision in Lebanon. Br J Ophthalmol. 1997;81:905–906. doi:10.1136/bjo.81.10.905
11. Baarah BT, Shatnawi RA, Khatatbeh AE. Causes of permanent severe visual impairment and blindness among the Jordanian population. Middle East Afr J Ophthalmol. 2018;25:25–29. doi:10.4103/meajo.MEAJO_202_16
12. Rens GH, Chmielowski RJ, Lemmens WA. Results obtained with low vision aids a retrospective study. Doc Ophthalmol. 1991;78:205–210. doi:10.1007/BF00165682
13. Nguyen NX, Weismann M, Trauzettel-Klosinski S. Spectrum of ophthalmologic and social rehabilitation at the Tubinger Low-Vision Clinic: a retrospective analysis for 1999–2005. Der Ophthalmologe. 2008;105(6):563–569. doi:10.1007/s00347-007-1651-5
14. Tsai IL, Woung LC, Tsai CY, et al. Trends in blind and low vision registrations in Taipei City. Eur J Ophthalmol. 2008;18(1):118–124. doi:10.1177/112067210801800120
15. Tabbara KF, Baghdassarian SA. Childhood blindness in Lebanon. Am J Ophthalmol. 1975;79:827–830. doi:10.1016/0002-9394(75)90744-8
16. Mirdehghan SA, Dehghan MH, Mohammadpour M, et al. Causes of severe visual impairment and blindness in schools for visually handicapped children in Iran. Br J Ophthalmol. 2005;89:612–614. doi:10.1136/bjo.2004.050799
17. Sarabandi A, Mobaraki H, Kamali M, Chabok A, Soltani S. The effect of rehabilitation services on quality of life for the blind. Mod Rehabil. 2014;7(4):48–56.
18. Haddad MA, Sei M, Sampaio MW, Kara-Jose N. Causes of visual impairment in children: a study of 3210 cases. J Pediatr Ophthalmol Strabismus. 2007;44:232–240. doi:10.3928/01913913-20070701-04
19. Herse P, Gothwal VK. Survey of visual impairment in an Indian tertiary eye hospital. Indian J Ophthalmol. 1997;45:189–193.
20. Pathanapitoon K, Ausayakhun S, Kunavisarut P, et al. Blindness and low vision in a tertiary ophthalmologic center in Thailand: the importance of cytomegalovirus retinitis. Retina. 2007;27:635–640. doi:10.1097/01.iae.0000249575.38830.45
21. Waddell KM. Childhood blindness and low vision in Uganda. Eye (Lond). 1998;12(Pt 2):184–192. doi:10.1038/eye.1998.45
22. Ramezani A, Pardis M, Rafati N, Kazemi-Moghaddam M, Katibeh M, Rostami P. Causes of visual impairment among patients referred to a visual rehabilitation clinic in Iran. Korean J Ophthalmol. 2012;26(2):80–83. doi:10.3341/kjo.2012.26.2.80
23. Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82:844–851. doi:/S0042-96862004001100009
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.