Back to Journals » Clinical Ophthalmology » Volume 20
Visual Gains with Faricimab vs Aflibercept 8 mg in Naïve Retinovascular Disease: Global Real-World Cases and Literature Review
Authors Mansour HA, Eandi CM, Pichi F ![]() , Foster RE, Charbaji SA, Chakraborty D, Ellabban AA
, Foster RE, Charbaji SA, Chakraborty D, Ellabban AA ![]() , Belotto S
, Belotto S ![]() , Abu Serhan H
, Abu Serhan H ![]() , Magnin S, Lopez-Guajardo L, Pérez-Salvador García E
, Magnin S, Lopez-Guajardo L, Pérez-Salvador García E ![]() , Schwartz SG
, Schwartz SG ![]() , Stewart MW, Rey A, Jürgens I
, Stewart MW, Rey A, Jürgens I ![]() , Casella AM
, Casella AM ![]() , Upadhyay A, Sheth JU, Lima LH
, Upadhyay A, Sheth JU, Lima LH ![]() , Sinawat S
, Sinawat S ![]() , Abengoechea S, Capella MJ, Viver Oller S, Elizalde J, Kheir WJ
, Abengoechea S, Capella MJ, Viver Oller S, Elizalde J, Kheir WJ ![]() , Mammo D, Barbosa GCS, Villegas VM, Desai A, Tripathy K, Bala S, Mohan N, Elnahry AG
, Mammo D, Barbosa GCS, Villegas VM, Desai A, Tripathy K, Bala S, Mohan N, Elnahry AG ![]() , Uwaydat SH, Cherfan DG, Parodi MB, Mansour AM
, Uwaydat SH, Cherfan DG, Parodi MB, Mansour AM ![]()
Received 5 May 2026
Accepted for publication 8 July 2026
Published 15 July 2026 Volume 2026:20 622037
DOI https://doi.org/10.2147/OPTH.S622037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Hana A Mansour,1 Chiara M Eandi,2,3 Francesco Pichi,4 Robert E Foster,5 Suzanne A Charbaji,6 Debdulal Chakraborty,7,8 Abdallah A Ellabban,9 Silvana Belotto,10,11 Hashem Abu Serhan,12 Simon Magnin,2 Lorenzo Lopez-Guajardo,13,14 Eduardo Pérez-Salvador García,15 Stephen G Schwartz,16,17 Michael W Stewart,18,19 Amanda Rey,20 Ignasi Jürgens,20 Antonio MB Casella,21 Anubhav Upadhyay,22 Jay U Sheth,23 Luiz H Lima,24 Suthasinee Sinawat,25 Santiago Abengoechea,10,11 Maria Jose Capella,10,11 Sonia Viver Oller,10,11 Javier Elizalde,10,11 Wajiha J Kheir,1 Danny Mammo,26 Gabriel Castilho Sandoval Barbosa,24,26 Victor M Villegas,27 Arjun Desai,28 Koushik Tripathy,29 Suraj Bala,26,30 Nitesh Mohan,26 Ayman G Elnahry,31– 33 Sami H Uwaydat,34 Daniel G Cherfan,35 Maurizio Battaglia Parodi,36 Ahmad M Mansour1
1Department of Ophthalmology (H.A.M., W.K., A.M.M.), American University of Beirut, Beirut, Lebanon; 2Hôpital Ophtalmique Jules-Gonin (C.H.E., S.M.), Fondation Asile des Aveugles, Lausanne, Switzerland; 3Department of Surgical Science (C.H.E.), University of Torino, Torino, Italy; 4Department of Ophthalmology and Visual Sciences (F.P.), University of Toronto, Toronto, Canada; 5Cincinnati Eye Institute (R.E.F.), Cincinnati, OH, USA; 6Department of Epidemiology and Population Health (S.A.C.), American University of Beirut, Beirut, Lebanon; 7Disha Eye Hospital (D.C.), Silchar Medical College Sri Sankaradeva Nethralaya, Silchar, Assam, India; 8Sankara Nethralaya Chennai (D.C.), Kolkata, West Bengal, India; 9Hull University Teaching Hospitals NHS Trust (A.A.E.), Hull, Yorkshire, UK; 10Centro de Oftalmología Barraquer (S.B., S.A., M.J.C., S.V., J.E.), Barcelona, Spain; 11Institut Universitari Barraquer (S.B., S.A., M.J.C., S.V., J.E.), Universitat Autònoma de Barcelona, Barcelona, Spain; 12Department of Ophthalmology (H.A.S.), Hamad Medical Corporations, Doha, Qatar; 13Department of Ophthalmology (L.L.G.), Hospital Clinico San Carlos, Madrid, Spain Profesor Asociado de Oftalmología, Universidad Complutense de Madrid, Madrid, Spain; 14Department of Ophthalmology (L.L.G.), Universidad Complutense de Madrid, Madrid, Spain; 15Servicio de Oftalmología del Hospital Universitario de Burgos (E.P.-S.G.), Burgos, Spain; 16Bascom Palmer Eye Institute (S.G.S.), University of Miami Miller School of Medicine, Miami, FL, USA; 17Bascom Palmer Eye Institute at Naples (S.G.S.), Naples, FL, USA; 18Department of Ophthalmology (M.W.S.), Mayo Clinic Florida, Jacksonville, FL, USA; 19Knights Templar Eye Foundation (M.W.S.), Jacksonville, FL, USA; 20Institut Català de Retina (A.R., I.J.), Barcelona, Spain; 21Department of Ophthalmology (A.M.B.C.), Universidade Estadual de Londrina, Londrina, Paraná, Brazil; 22ASG Eye Hospitals (A.U.), Jaipur, Rajasthan, India; 23Shantilal Shanghvi Eye Institute (J.U.S.), Mumbai, India; 24Department of Ophthalmology and Visual Sciences (L.H.L., G.C.S.B.), Federal University of São Paulo, São Paulo, Brazil; 25KKU Eye Center (S.S.), Department of Ophthalmology (S.S.), Khon Kaaen University, Bangkok, Thailand; 26Cleveland Clinic Cole Eye Institute (D.A.M., G.C.S.B., N.M.), Cleveland, OH, USA; 27Department of Ophthalmology (V.M.V.), University of Puerto Rico, San Juan, PR, USA; 28ASG Saatvik Eye Hospital (A.D.), Vadodara, India; 29ASG Hospitals (K.T.), Kolkata, India; 30Hackensack Meridian School of Medicine (S.B.), Nutley, NJ, USA; 31Department of Ophthalmology and Visual Sciences (A.E.), School of Medicine and Public Health, University of Wisconsin-Madison, Madison, WI, USA; 32Department of Ophthalmology (A.E.), Faculty of Medicine, Cairo University, Cairo, Egypt; 33Retina Vitreous Center (A.E.), Edmond, OK, USA; 34Jones Eye Institute (S.H.U.), University of Arkansas, Little Rock, AR, USA; 35Beirut Eye Specialty Hospital (D.G.C.), Beirut, Lebanon; 36Department of Ophthalmology (M.B.P.), University Vita-Salute Milan, Milan, Italy
Correspondence: Ahmad M Mansour, Email [email protected] Maurizio Battaglia Parodi, Email [email protected]
Background: To compare the visual gains of faricimab and aflibercept 8 mg as first-line in real-world management of retinovascular diseases.
Methods: Retrospective multicenter interventional case series with retinovascular diseases initiated on faricimab or aflibercept 8 mg till August 30, 2025. Main outcome measure was visual gain in logMAR. Linear mixed-effects model was used to compare vision increase between the two drug groups. In addition, comparative Phase 3 trials were supplemented by a literature review of treatment-naïve eyes using major databases till September 30, 2025.
Results: We collected 500 treated eyes from 35 collaborating centers. The treatment groups included 395 eyes receiving faricimab vs 105 receiving aflibercept 8 mg distributed into neovascular macular degeneration (270 vs 58), diabetic macular edema (97 vs 39) and macular edema associated with retinal vein occlusion (28 vs 8). Adjusted visual gains were comparable between the two drugs in various retinal categories (p=0.672).
Conclusion: Visual acuity improved significantly and equally in both aflibercept 8 mg and faricimab in several treatment-naïve retinovascular diseases.
Keywords: aflibercept 8 mg, faricimab, macular degeneration, diabetic maculopathy, retinal vein occlusion
Introduction
The introduction of faricimab (VabysmoR, Genentech Inc, South San Francisco, CA, US) and aflibercept 8 mg (Eylea HDR, Regeneron Pharmaceuticals Inc, Tarrytown, New York, US) to treat chorioretinal vascular diseases has garnered significant attention in Ophthalmology. Aflibercept 2 mg (the precursor to 8 mg), a fusion protein that binds all isoforms of vascular endothelial growth factor (VEGF)-A, VEGF-B, galectin-1, and placental growth factor, has an excellent efficacy and safety profile, whereas the recently approved faricimab (2023) is a novel humanized bispecific antibody that targets isoforms of VEGF-A and angiopoietin-2 (Ang-2).
Both faricimab and aflibercept 8 mg were developed to decrease treatment burden by lengthening treatment intervals. Data from pivotal clinical trials1–6 have demonstrated the long-term efficacy and safety of both drugs in patients with diabetic macular edema (DME) and neovascular age-related macular degeneration (nAMD), with the possibility of interval extension to 16 weeks or longer in nearly 50% of eyes. Preliminary data from real-world nAMD and DME studies support the efficacy of both drugs,7–57 with excellent stabilization of vision, but no large head-to-head study has compared the visual outcomes and numbers of injections.
In this manuscript, we report the results of a large, multi-center, international comparison cohort to better define the therapeutic abilities of faricimab and aflibercept 8 mg in improving visual outcomes in treatment-naïve eyes. By including a diverse group of patients with different genetic make-ups, backgrounds, medical problems, and environmental influences, we believe that our results are generalizable to clinical practices throughout the world.
Additionally, we performed a comprehensive search of the literature to identify treatment-naïve patients receiving faricimab and aflibercept 8 mg as first line therapy. Finally, we have extracted data from the phase 3 faricimab and aflibercept 8 mg registration trials. We believe that by using data from these three distinct sources, a comprehensive data-driven understanding of the efficacy and safety of faricimab and faricimab can best be attained.
Materials and Methods
Study Approval
A multicenter case series of patients treated from January, 2025 to August 2025 was compiled from 35 retina centers throughout the world (Africa, America, Asia and Europe). The study was approved by the Ethics Committee of the Beirut Eye Specialty Hospital (BESH-EC20-251) and followed the tenets of the Declaration of Helsinki. The need for informed consent was waived because of the anonymous and retrospective nature of the research. The study was exempt from IRB oversight because of its retrospective design and deidentified patient data. Confidentiality was maintained throughout data aggregation and analysis.
Study Design
The study included a consecutive series of patients with treatment-naïve nAMD, DME, or RVO who were primarily treated with either intravitreal aflibercept 8 mg or faricimab depending on commercial availability. Inclusion criteria included the following: active subfoveal neovascular membrane due to nAMD; fovea-involving DME; or diffuse macular edema due to CRVO or BRVO. Exclusion criteria included the following: age under 20 years; previous vitrectomy; cataract surgery within the past 6 months; presence of keratitis, conjunctivitis, blepharitis or systemic infection. Most patients received a loading series of three or four monthly intravitreal injections with additional injections according to treat-and-extend or personalised protocols according to patients needs.
Each patient underwent a comprehensive ocular examination, including measurement of best corrected visual acuity (BCVA) with Snellen charts, which was converted to logMAR for analyses. Spectral domain optical coherence tomography (OCT) or OCT angiography (OCTA) were analysed at baseline and at month four. The primary outcome measures included BCVA at baseline, 1 month, and at last follow-up. Intraocular pressures (IOP) were measured at baseline, 1 minute after the injection, and at follow-up examinations. Participants were scheduled to receive at least three loading doses every four weeks and thereafter at the discretion of the ophthalmologist, based on OCT and/or functional criteria. Complications, as noted during examinations or reported by patients, were recorded.
Aflibercept 8 mg (30.1 mg/0.263 mL) was withdrawn from a vial into a 1 mL sterile syringe and 0.07 mL (8 mg) was injected into the vitreous. Faricimab (28.8 mg/0.24 mL) was withdrawn from a vial into a 1 mL sterile syringe and 0.05 mL (6 mg) was injected into the vitreous. For centers without access to aflibercept 8 mg, the same dose was achieved using multiple doses of aflibercept 2 mg58 with prior paracentesis to control the anticipated IOP rise.
Literature and Phase 3 Trial Data
Since both drugs were recently approved and only limited data sets had been published, a literature review in the aim to broaden the external validity of the current retrospective case series. We used the PICO framework (Population: treatment naïve eyes with nAMD, DME or RVO-ME, outside controlled studies. Intervention: faricimab or aflibercept 8 mg injections into the vitreous. Comparator: number of injections and period of followup, Outcome: visual gain). We searched the Medline, Scopus, Web of Science, and Cochrane Reviews (from January 1, 2023 to September 30, 2025) databases with the Medical Subject Headings “faricimab AND naïve treatment AND real world” or “8 mg aflibercept AND naïve treatment AND real world”. Inclusion criteria included: English, French and Spanish languages; no country restriction; patient age above 18 years; publications that included meeting abstracts and articles in press. Exclusion criteria included: reviews; editorials; letters; Phase 2 or 3 controlled studies; case reports; previous laser therapy; aflibercept 4 mg; and follow-up less than 2 months. The data search was performed by 2 operators (HAM, AMM).
Data were extracted from the phase 3 trials for faricimab (TENAYA and LUCERNE, YOSEMITE and RHINE, BALATON and COMINO) and aflibercept 8 mg (PULSAR, PHOTON, and QUASAR).
Statistical Analysis
Quantitative data were analyzed with mean and standard deviation (SD). For the BCVA analyses, Snellen visual acuity was converted to logMAR and, for consistency, ETDRS letters were also converted into logMAR. Linear Mixed-Effects Model was used to compare BCVA gains between the two drugs. A linear mixed-effects model (LMM) was employed as the primary analytical approach, justified by the large sample size (500 eyes), repeated BCVA measurements across three visits (initial, 1 month and final), unequal follow-up durations, and baseline imbalance between treatment groups. The model included fixed effects for time, retinal disease category, treatment type, number of injections, and follow-up duration. A random intercept for eye was specified to account for within-eye correlation across repeated measures.
Statistical analyses were performed using SPSS 29.0 (IBM SPSS Inc, Armonk, NY, US) software. A P-value equal to or less than 0.05 was considered statistically significant. To analyze the literature review data, missing results were filled using mean imputation. Comparison of two independent means was performed using the t-test.
Results
Demographics of Cohort
General demographic data on treatment-naïve patients are depicted in Table 1 and Table 2. We included a total of five hundred eyes from 467 patients (bilateral injections were performed in 14 patients with nAMD: 11 faricimab vs 3 aflibercept 8 mg; and 19 patients with DME: 12 faricimab vs 7 aflibercept 8 mg). Mean baseline BCVA was 0.61 ± 0.45 LogMAR. Mean follow-up duration was 11.67 ± 7.61 months, and eyes received a mean of 5.92 ± 4.16 intravitreal injections. The cohort consisted predominantly of age-related macular degeneration (AMD) (65.6%), followed by diabetic macular edema (DME) (27.2%) and retinal vein occlusion (RVO) (7.2%). Most eyes were treated with Faricimab (79.0%), while 21.0% received aflibercept 8 mg. No significant differences in sex (p=0.13 for nAMD and p=0.27 for DME), age and systemic diseases (diabetes mellitus p=0.86 for nAMD and p=1.0 for DME; coronary artery disease p=0.38 for nAMD and p=0.12 for DME) were noted between the cohorts. Adjusted overall mean initial BCVA (in LogMAR) improved by 0.183 (from 0.719 to 0.536) (95% confidence interval: 0.118–0.247; p<0.001) 1 month after the first injection and by 0.239 (from 0.719 to 0.480) (95% confidence interval: 0.178–0.300; p<0.001) at the end of followup. For eyes with nAMD, DME, or RVO, BCVA at one month was a strong predictor of final BCVA (p=0.001).
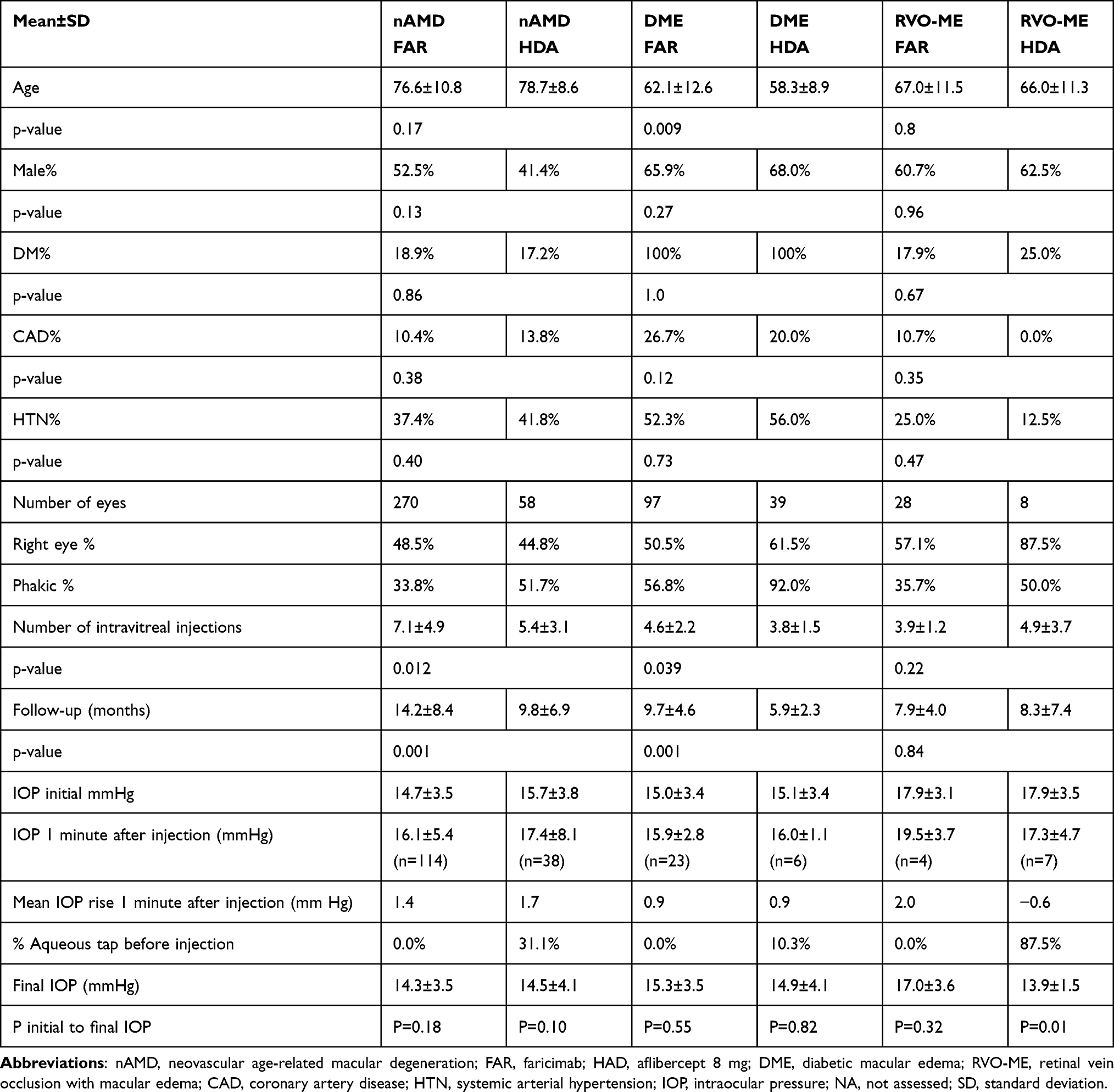 |
Table 1 Real World Comparison Between 500 Consecutive Treatment-Naive Eyes Treated with Either Faricimab or Aflibercept 8 mg |
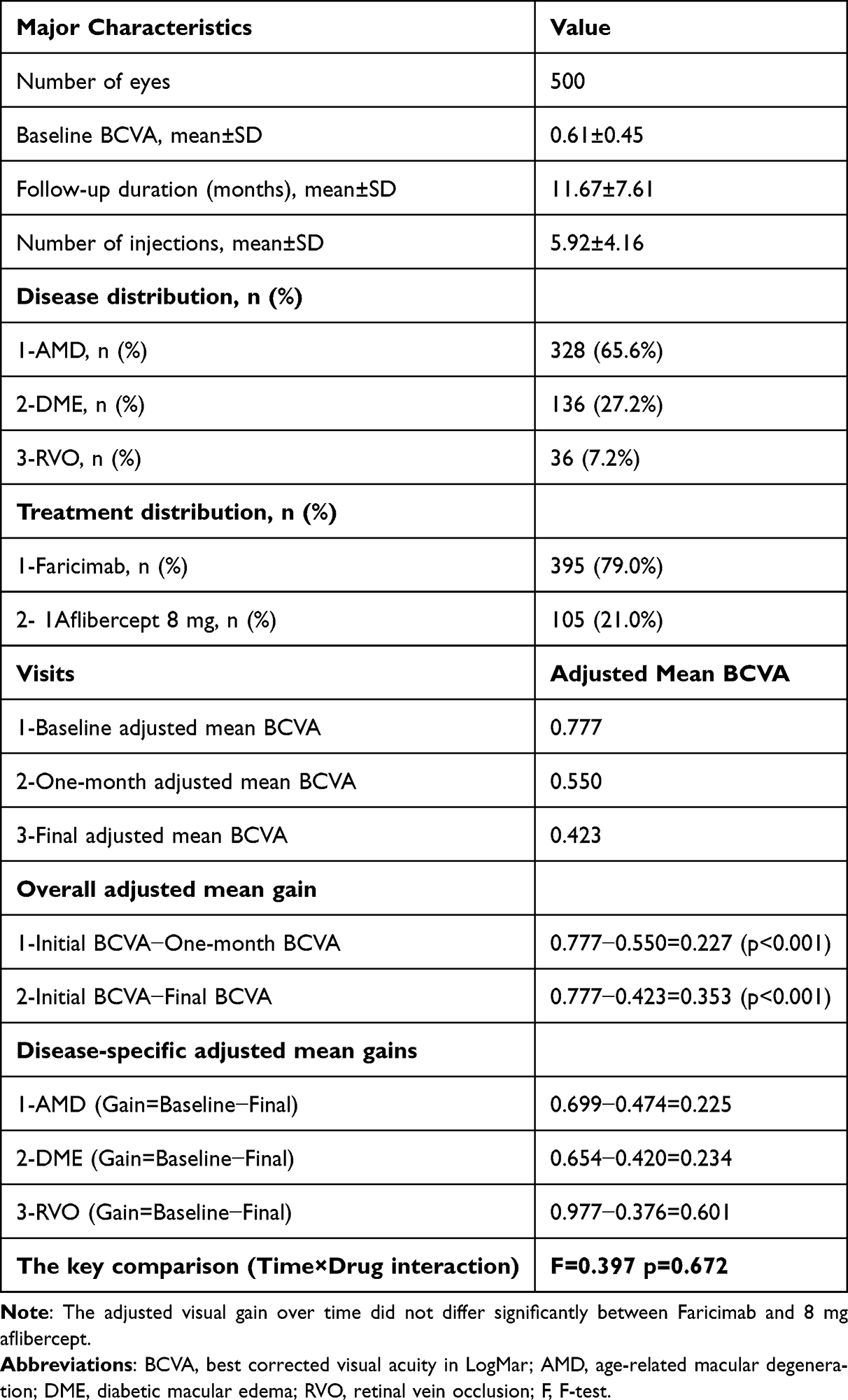 |
Table 2 Distribution of 500 Eyes Treated with Faricimab of Aflibercept 8 mg. Comparison of Vision is Based on Estimated Marginal Means |
Final Results
The final LMM demonstrated a significant effect of time on visual acuity (F=42.12, p<0.001). After adjustment for repeated measurements, retinal disease, follow-up duration, and injection number, the (Treatment × Time interaction) was not significant (F=0.397; p=0.672), indicating that the longitudinal pattern of visual gain over time was comparable between treatment groups. Thus both treatments demonstrated similar visual improvement over the course of follow-up.
Adverse Events
IOP rise immediately after injections was similar between the two drugs. No drug reflux was noted when aflibercept 8 mg was preceded by paracenteses.
Reported adverse events included death (three months after follow-up and receipt of two faricimab injections), endophthalmitis (two eyes after second injections of aflibercept 8 mg in two patients with severe flu-like diseases), iritis (one faricimab and one aflibercept 8 mg), glaucoma (two faribimab and one aflibercept 8 mg), retinal pigment epithelial tear (one faricimab), subretinal hemorrhage (two faricimab), retinal detachment (two faricimab). Loss to follow-up was due to the following conditions: uremic encephalopathy (one aflibercept 8 mg); macular scars (two faricimab); two aflibercept 8 mg switched to faricimab after third injection; two faricimab switched to aftlibercept 2 mg after 22 months and 24 months on faricimab; one faricimab switched to aflibercept 8 mg after 22 months on faricimab.
Literature Review of Treatment-Naïve Eyes
The database searches yielded 43 papers after deduplication; of these 43 were subjected to full text screen and 32 were judged to be appropriate for inclusion. Additional 21 papers were identified through hand searching and were also deemed suitable for inclusion. In total, the review analyzed 6179 treatment-naïve eyes in 52 studies7–57 (Table 3): a total of treated with faricimab nAMD (4089), DME (1903), RVO-ME (47) and a total of treated with aflibercept 8 mg for nAMD (140). There was a robust significant visual increase of 1.3 ETDRS line after an average of 4.1 faricimab injections. A marginally significant increase of one ETDRS line was noted in the aflibercept 8 mg group after an average of 3.3 injections. The short follow-up precluded commenting on the difference in the number of injections. Moreover, the faricimab group included worse baseline vision than the aflibercept 8 mg group introducing a bias limiting direct comparison of final outcome.
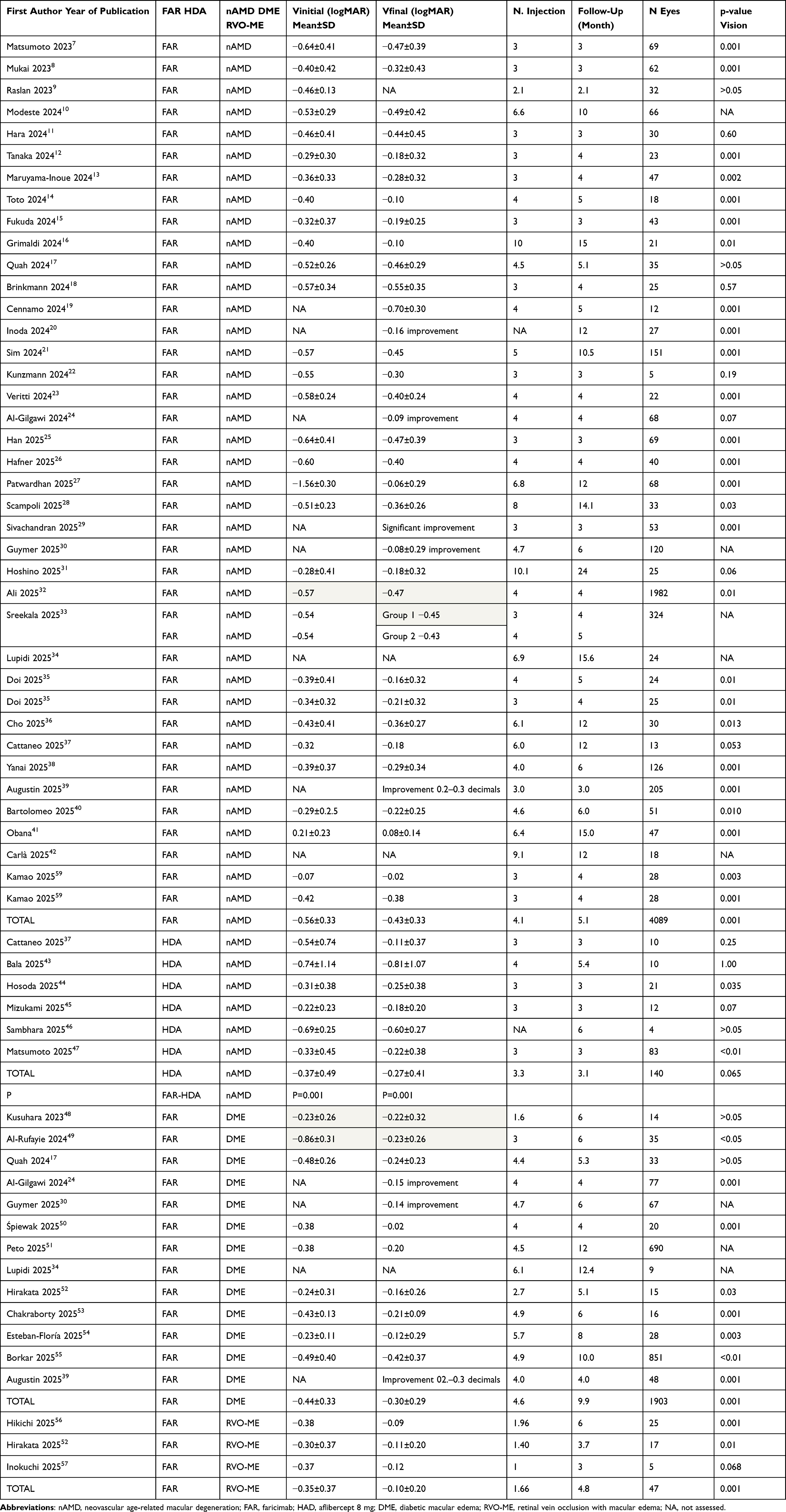 |
Table 3 Systematic Review of 6179 Eyes Through August 30, 2025 for Real-World Treatment Naïve Eyes.7–57,59 Visual Outcomes with Aflibercept 8 mg or Faricimab are Shown |
Phase 3 Trial Data
Phase 3 nAMD trials demonstrated similar one-year improvements in mean BCVA (logMAR) and numbers of injections between faricimab (−0.12, 6.6) and aflibercept 8 mg (−0.13, 5.7) (Table 4). For eyes with DME, one year improvements in mean BCVA and numbers of injections were −0.23, 9.0 for faricimab and −0.17, 5.5 for aflibercept 8 mg. For eyes with RVO-ME, improvements in mean BCVA and numbers of injections were −0.34, 6.0 for faricimab (mean follow-up of 6 months) and −0.36, 6.5 for aflibercept 8 mg (mean follow-up of 8 months).
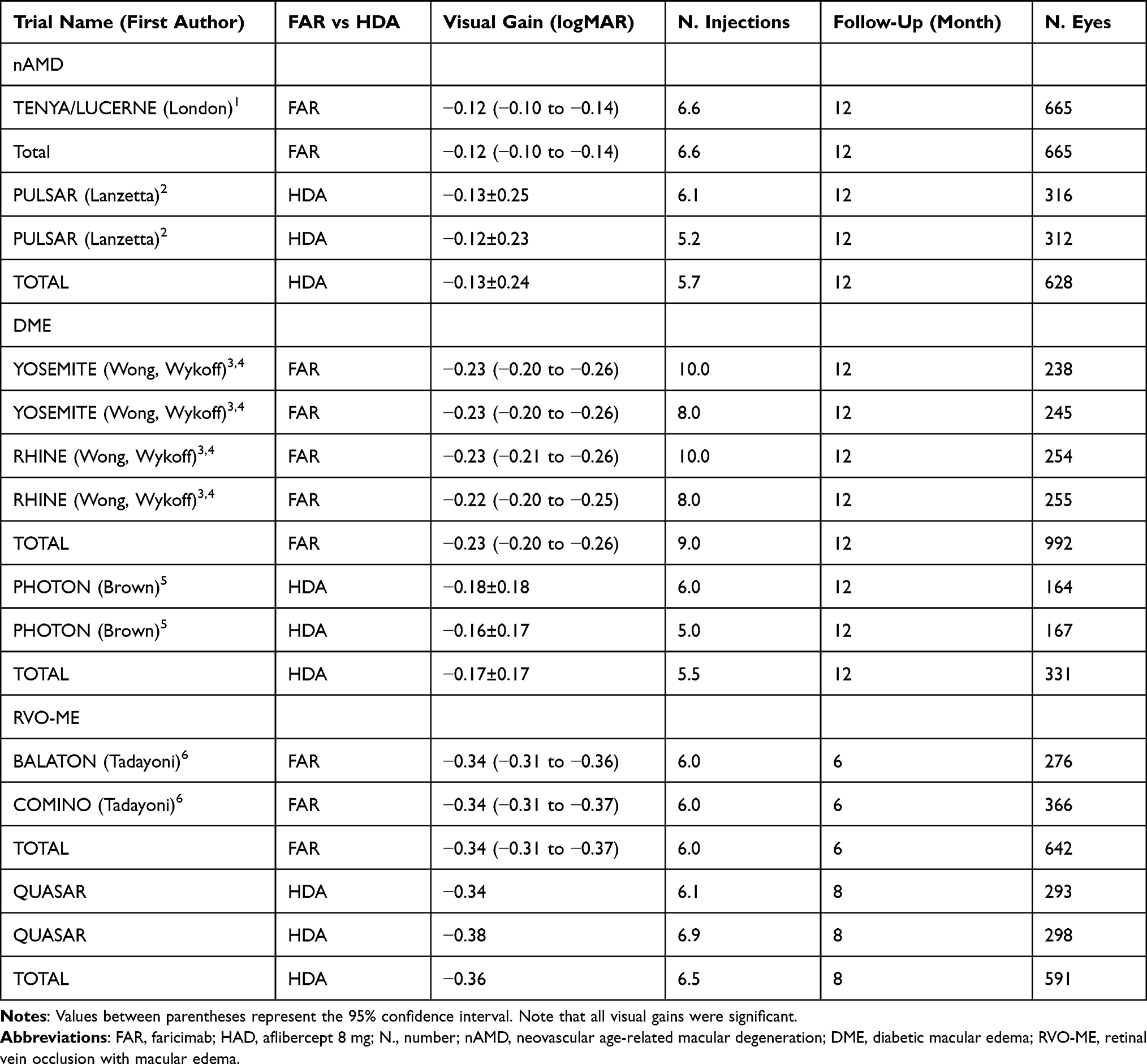 |
Table 4 The Table Includes 3849 Treatment-Naïve Eyes in Phase 3 Faricimab and Aflibercept 8 mg Registration Trials with Data Captured at Approximate One Year (Depending on the Primary Endpoints) Except for Retinal Vein Occlusion Trials Which Terminated Earlier |
When combining results of the three analytic models (Tables 1–4) into one (Table 5), complete unadjusted comparative data can be found for nAMD only. Mean unadjusted BCVA improvements were comparable between faricimab and aflibercept 8 mg −0.12 vs −0.13 in phase 3 trials (6.6 vs 5.7 injections over a follow-up of 12 months), −0.13 vs −0.10 in the real-world literature (4.1 vs 3.3 injections over a follow-up of 5.1 vs 3.1 months), and −0.23 vs −0.23 in the current study (7.1 vs 5.4 injections over a follow-up of 14.2 vs 9.8 months).
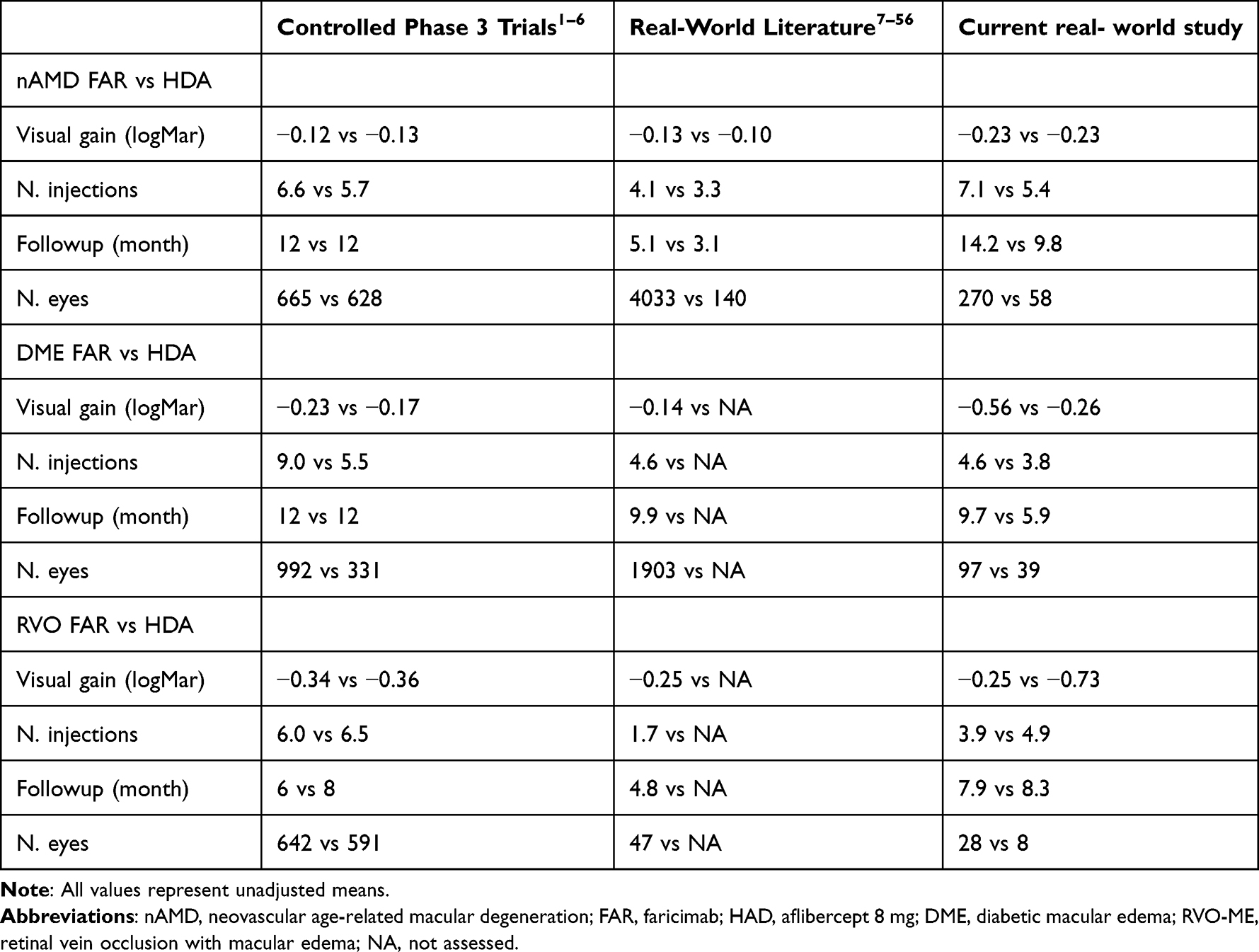 |
Table 5 Summary of Head to Head Comparison Between First Line Therapy with Faricimab or Aflibercept 8 mg in the Phase 3 Clinical Controlled Trials, Real World Published Studies, and Current Real World Retrospective Study |
Discussion
This comparative study of real world treatment-naïve eyes with nAMD, DME, and RVO (Table 1), backed by even larger numbers of real world treatment-naïve eyes from the published world literature (Table 2) and supported by a comparative analysis of phase 3 controlled trials (Table 3), emphasizes the clinical efficacy of faricimab and aflibercept 8 mg with comparable visual gains. The drugs produce similar BCVA gains, comparable final BCVA when initial BCVA is used as a covariate and after matching for follow-up, excellent safety profiles (including minimal IOP rise), and rapid improvments in vision as early as one month post-injection. The unique multifaceted comparison used in this analysis between the two benchmark drugs for three chorioretinal vascular diseases highlights the similarities in safety and efficacy. Because these drugs appear to produce longer dosing intervals with reduced treatment burden compared to previously introduced anti-VEGF drugs, they should become convenient options for real-world practice.60
Several lines of evidence point to vision benefits between faricimab and aflibercept 8 mg despite their different mechanisms of action. Faricimab’s dual VEGF-A/Ang-2 inhibition and aflibercept’s broader VEGF-A/B/PlGF blockade both achieve similar visual outcomes in head-to-head trials, with comparable durability and safety profiles. The similar intravitreal half-lives (faricimab: 7.5 days; aflicercept 8 mg: 7.2 days)61,62 further support similar clinical efficacies, since both drugs maintain therapeutic intraocular concentrations over extended periods of time.
The current study found small, similar IOP rises one minute post-injection, consistent with published observations.63 Ocular and systemic complications were infrequent and mild, which closely matched the phase 3 trials safety profiles.64
Limitations of our real-world case study included its retrospective design, short follow-up, heterogeneous subcategories, inclusion of advanced maculopathy, variable retreatment strategies, missing anatomic markers, and selection bias for most difficult scenarios that collectively limit clinical interpretability between the faricimab and the aflibercept cohorts. Additionally, one must be cautious when comparing data from different studies (multicenter real-world study, compendium of world literature, and phase 3 trials) because of the differences in study designs and populations. Also, we did not compare the behavior of the two drugs in refractory cases.65,66 However, the major strength of this study is the comprehensive accumulation of a large volume of data from several sources, all of which point to quite similar results. It is still unknown if the two drugs keep their therapeutic efficacy and safety profile in the long-range.
Conclusions
In conclusion, comparable, robust, rapid, and durable BCVA gains were achieved across different disease processes (nAMD, DME and possibly RVO-ME) with very low rates of ophthalmic or systemic adverse effects in clinical trials (long-term), real world literature (midterm), and our large-cohort multicenter real world study (short term) when using faricimab or aflibercept 8 mg as first-line therapies.
Abbreviations
Ang-2, angiopoietin-2; BCVA, best corrected visual acuity; BRVO, branch retinal vein occlusion; CRVO, central retinal vein occlusion; DME, diabetic macular edema; nAMD, neovascular age-related macular degeneration; VEGF, vascular endothelial growth factor.
Data Sharing Statement
Data are available on reasonable request to corresponding author AMM. The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding authors.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of the Beirut Eye Specialty Hospital (BESH-EC20-251) and followed the tenets of the Declaration of Helsinki. The need for informed consent was waived because of the anonymous and retrospective nature of the research. The study was exempt from IRB oversight because of its retrospective design and deidentified patient data. Confidentiality was maintained throughout data aggregation and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was not supported.
Disclosure
Professor Stephen Schwartz reports grants from Research to Prevent Blindness; Stock or stock options from GE Healthcare Technologies, Inc, outside the submitted work. Professor Michael Stewart reports grants from Alexion; Consulting fees from Biogen, Revana, Regeneron, Bayer; Expert testimony from Regeneron, outside the submitted work. Professor Antonio Casella reports honoraria from Alcon, Zeiss, Roche, outside the submitted work. Dr Wajiha Kheir is part of the data safety/advisory board for Roche, outside the submitted work. The authors declare no other competing interests in relation to the work described.
References
1. London NJS, Cheung CMG, Michels S, et al. Outcomes by faricimab treatment interval at week 48 of TENAYA-LUCERNE Phase III Trials in neovascular age-related macular degeneration. Ophthalmol Retina. 2025;9:1081–14. doi:10.1016/j.oret.2025.05.004
2. Lanzetta P, Korobelnik JF, Heier JS, et al. Intravitreal aflibercept 8 mg in neovascular age-related macular degeneration (PULSAR): 48-week results from a randomised, double-masked, non-inferiority, phase 3 trial. Lancet. 2024;403:1141–1152. doi:10.1016/S0140-6736(24)00063-1
3. Wong TY, Haskova Z, Asik K, et al. Faricimab treat-and-extend for diabetic macular edema: two-year results from the randomized phase 3 YOSEMITE and RHINE Trials. Ophthalmology. 2024;131:708–723. doi:10.1016/j.ophtha.2023.12.026
4. Wykoff CC, Brown DM, Reed K, et al. Effect of high-dose intravitreal aflibercept, 8 mg, in patients with neovascular age-related macular degeneration: the phase 2 CANDELA randomized clinical trial. JAMA Ophthalmol. 2023;141:834–842. doi:10.1001/jamaophthalmol.2023.2421
5. Brown DM, Boyer DS, Do DV, et al. Intravitreal aflibercept 8 mg in diabetic macular oedema (PHOTON): 48-week results from a randomised, double-masked, non-inferiority, phase 2/3 trial. Lancet. 2024;403:1153–1163. doi:10.1016/S0140-6736(23)02577-1
6. Tadayoni R, Paris LP, Danzig CJ, et al. Efficacy and safety of faricimab for macular edema due to retinal vein occlusion: 24-week results from the BALATON and COMINO Trials. Ophthalmology. 2024;131:950–960. doi:10.1016/j.ophtha.2024.01.029
7. Matsumoto H, Hoshino J, Nakamura K, Nagashima T, Akiyama H. Short-term outcomes of intravitreal faricimab for treatment-naïve neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2023;261:2945–2952. doi:10.1007/s00417-023-06116-y
8. Mukai R, Kataoka K, Tanaka K, et al. Three-month outcomes of faricimab loading therapy for wet age-related macular degeneration in Japan. Sci Rep. 2023;13:8747. doi:10.1038/s41598-023-35759-4
9. Raslan W, Younis S, Fabozzi L, Hassan I, Palmieri F. Early real-world outcomes in patients with neovascular Age-related Macular Degeneration (nAMD) treated with Faricimab. Invest Ophthalmol Vis Sci. 2023;64:OD79.
10. Modeste D, Stewart C, Premanandhan H, Awad MH, Williams GS. Evaluating faricimab in treatment-naive neovascular age related macular degeneration: a retrospective analysis of real-world data. Clin Ophthalmol. 2024;18:2821–2829. doi:10.2147/OPTH.S468458
11. Hara C, Suzue M, Fujimoto S, et al. Comparison of loading dose between aflibercept and faricimab for neovascular age-related macular degeneration. J Clin Med. 2024;13:385. doi:10.3390/jcm13020385
12. Tanaka A, Hata M, Tsuchikawa M, et al. Short-term outcomes of 3 monthly intravitreal faricimab on different subtypes of neovascular age-related macular degeneration. Clin Ophthalmol. 2024;18:507–516. doi:10.2147/OPTH.S448507
13. Maruyama-Inoue M, Yanagi Y, Inoue T, Kadonosono K. Comparison of functional and morphologic changes between brolucizumab and faricimab in neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2024;262:589–599. doi:10.1007/s00417-023-06241-8
14. Toto L, Formenti F, Ruggeri ML, et al. Efficacy and durability of Faricimab in naïve eyes with neovascular age-related macular degeneration. Ophthalmic Res. 2024;67:528–536. doi:10.1159/000540194
15. Fukuda Y, Notomi S, Shiose S, et al. Three-month outcomes of treatment with faricimab or aflibercept for neovascular age-related macular degeneration: a propensity score matching study in a Japanese population. Graefes Arch Clin Exp Ophthalmol. 2024;262:3971–3978. doi:10.1007/s00417-024-06582-y
16. Grimaldi G, Cancian G, Paris A, et al. Intravitreal faricimab for treatment naïve patients with neovascular age-related macular degeneration: a real-world prospective study. Int J Retin Vitr. 2024;10:70. doi:10.1186/s40942-024-00586-w
17. Quah NQ, Javed KM, Arbi L, Hanumunthadu D. Real-world outcomes of faricimab treatment for neovascular age-related macular degeneration and diabetic macular edema. Clin Ophthalmol. 2024;18:1479–1490. doi:10.2147/OPTH.S463624
18. Brinkmann M, Viggiano P, Boscia G, et al. Analysis of Choriocapillaris reperfusion topography following Faricimab treatment for Neovascular age-related macular degeneration in therapy-naive patients. Ophthalmol Ther. 2024;13:1981–1992. doi:10.1007/s40123-024-00967-2
19. Cennamo G, Rinaldi M, Chiosi F, Costagliola C. Changes in macular pigment optical density after intravitreal faricimab in neovascular age-related macular degeneration: a pilot study. J Clin Med. 2024;13:4893. doi:10.3390/jcm13164893
20. Inoda S, Takahashi H, Sato A, et al. One year visual and anatomical outcomes of Intravitreal faricimab Injection for treatment-naïve neovascular age-related macular degeneration: a single-center retrospective study. Invest Ophthalmol Vis Sci. 2024;65:OD69.
21. Sim SY, Nicholson L, Patel PJ, et al. Real-world outcomes of faricimab injections in treatment-naïve neovascular age-related macular degeneration (nAMD) patients: the Moorfields Experience. Invest Ophthalmol Vis Sci. 2024;65:246.
22. Kunzmann BC, Schweig AS, Bartz-Schmidt KU, Sobolewska B. Real-world-data of treatment-naïve and previously treated patients receiving up to 3 injections of faricimab in neovascular age-related macular degeneration. Clin Ophthalmol. 2024;18:4029–4039. doi:10.2147/OPTH.S482948
23. Veritti D, Sarao V, Di Bin F, Lanzetta P. Pharmacokinetic and pharmacodynamic rationale for extending VEGF inhibition increasing intravitreal aflibercept dose. Pharmaceutics. 2023;15:1416. doi:10.3390/pharmaceutics15051416
24. Al-Gilgawi A, Patel A, Green A, et al. Real world data of the use of Faricimab in the treatment of neovascular age-related macular degeneration (nAMD) and diabetic macular oedema (DMO) in a multi-ethnic population: experience of first 1000 injections. Invest Ophthalmol Vis Sci. 2024;65:5076.
25. Han HY, Park SM, Lee JH, et al. Outcomes and predictive factors for fluid resolution following three loading injections of faricimab for treatment-naïve neovascular age-related macular degeneration. Sci Rep. 2025;15:938. doi:10.1038/s41598-024-82746-4
26. Hafner M, Asani B, Eckardt F, et al. Deep-learning-assisted analysis of early biomarker changes in treatment-naive patients with neovascular AMD under intravitreal faricimab. Ophthalmol Ther. 2025;14:1025–1037. doi:10.1007/s40123-025-01125-y
27. Patwardhan A, Ali N, Law S. Intravitreal Faricimab in treatment-naïve neovascular age-related macular degeneration: real-world outcome of 12-week extension after the loading dose from a UK centre. Eye. 2025;39:766–770. doi:10.1038/s41433-024-03487-2
28. Scampoli A, Carlà MM, Grieco G, et al. One-year functional and structural results of faricimab for treatment-naïve neovascular age related macular degeneration: an OCT angiography study. Graefe’s Archiv Clin Exp Ophthalmol. 2025;263:2219–2226. doi:10.1007/s00417-025-06849-y
29. Sivachandran N, Pickel L, Khan H, et al. Visual and anatomic outcomes of dual inhibition in naive nAMD patients with associated subretinal hemorrhage. Invest Ophthalmol Vis Sci. 2025;66:4101.
30. Guymer RH, Schmitz-Valckenberg S, Bailey C, et al. Global real-world clinical and anatomical outcomes with faricimab in treatment-naïve patients with nAMD or DME from a prospective non-interventional study: the VOYAGER study. Invest Ophthalmol Vis Sci. 2025;66:3111.
31. Hoshino J, Matsumoto H, Numaga S, Nakamura K, Akiyama H. Two-year outcomes of treat-and-extend regimen with intravitreal faricimab for treatment-naïve neovascular age-related macular degeneration. Jpn J Ophthalmol. 2025;69:521–528. doi:10.1007/s10384-025-01204-4
32. Ali FS, Tabano DC, Borkar DS, et al. Early outcomes after initiation of faricimab for neovascular age-related macular degeneration. Ophthalmic Surg Lasers Imaging Retina. 2025;56:468–477. doi:10.3928/23258160-20250304-02
33. Sreekala S, Adusumilli HB, North L, et al. Comparison of three versus four loading doses of Faricimab in management of treatment naive and switch neovascular Age related Macular Degeneration (nAMD) patients. Invest Ophthalmol Vis Sci. 2025;66:3119.
34. Lupidi M, Iaculli C, Marco L, et al. Faricimab in the treatment of exudative neovascular age-related macular degeneration and diabetic macular edema in Italy: The FARIT Real World Study. Ophthalmol Ther. 2025;14:2197–2214. doi:10.1007/s40123-025-01204-0
35. Doi Y, Hata M, Kawashima Y, et al. One-year outcomes of three-monthly and four-monthly loading regimens of faricimab for treatment-naïve neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2025;263:3073–3079. doi:10.1007/s00417-025-06930-6
36. Cho J, Han HY, Park S, Kim JH, Cho HJ. One-year outcomes of faricimab versus aflibercept treatment for polypoidal choroidal vasculopathy: a comparative study. Eye. 2025;39:2893–2898. doi:10.1038/s41433-025-03980-2
37. Cattaneo J, De Oliveira Figueiredo EC, Montesel A, Vermeirsch S, Eandi CM. Early real-world outcomes of intravitreal aflibercept 8 mg in treatment-Naïve neovascular AMD: AI-assisted fluid volume analysis. Int J Retin Vitr. 2025;11:42. doi:10.1186/s40942-025-00665-6
38. Yanai R, Murao F, Miki A, et al. 6-month outcomes of intravitreal faricimab injection for neovascular age-related macular degeneration and their relationships with clinical findings: a multicentre cohort study from the J-CREST. BMJ Open Ophthalmol. 2025;10:e002415. doi:10.1136/bmjophth-2025-002415
39. Augustin AJ, Theine FF, Kaymak H, et al. Clinical care and therapeutic practice of patients with neovascular age-related macular degeneration (nAMD) and diabetic macular edema (DME) and effectiveness of faricimab in treatment-naive patients in Germany. ZEUS research project medRxiv preprint. 2025. doi:10.1101/2025.03.26.25324686.
40. Bartolomeo N, Schuetz YP, Nascimbeni AC, et al. Early outcome analysis of intravitreal aflibercept 8 mg treatment in naïve patients with neovascular age-related macular degeneration using artificial intelligence. Ophthalmol Ther. 2025;14:2819–2829. doi:10.1007/s40123-025-01239-3
41. Obana A, Asaoka R, Ishii K, et al. Propensity score analysis of treat-and-extend therapy with aflibercept versus faricimab in age-related macular degeneration. AJO Int. 2025;2:100178. doi:10.1016/j.ajoint.2025.100178
42. Carlà MM, Scampoli A, Grieco G, et al. Morphometric changes in macular neovascularization architecture after faricimab treatment in neovascular age-related macular degeneration: comparison between naive and switched eyes. Retina. 2026;46:125–135. doi:10.1097/IAE.0000000000004635
43. Bala S, Barbosa GCS, Mohan N, et al. Initial functional and anatomical outcomes of high-dose aflibercept 8 mg in exudative neovascular age-related macular degeneration. Ophthalmol Retina. 2025;9(8):756–766. doi:10.1016/j.oret.2025.02.002
44. Hosoda S, Sakurada Y, Fukuda Y, Kotoda Y, Kikushima W, Kashiwagi K. Short-term outcomes of three consecutive monthly loading administrations of aflibercept 8 mg for treatment-naïve exudative age-related macular degeneration. Pharmaceuticals. 2025;18:438. doi:10.3390/ph18030438
45. Mizukami T, Ueno S, Mishima S, Shimomura Y. One-month real-world comparison of aflibercept 8 mg versus 2 mg in treatment-naïve and previously treated eyes with neovascular age-related macular degeneration. Biologics. 2025;5:25. doi:10.3390/biologics5030025
46. Sambhara D, Vakharia P, Eichenbaum DA. Real-world efficacy and safety of 8 mg aflibercept in neovascular AMD: a case series. BMJ Open Ophthalmol. 2025;10:e002091. doi:10.1136/bmjophth-2024-002091
47. Matsumoto H, Hoshino J, Numaga S, Asatori Y, Akiyama H. Loading phase outcomes of intravitreal aflibercept 8 mg for treatment-naïve neovascular age-related macular degeneration. Jpn J Ophthalmol. 2025;69:911–917. doi:10.1007/s10384-025-01229-9
48. Kusuhara S, Kishimoto-Kishi M, Matsumiya W, Miki A, Imai H, Nakamura M. Short-term outcomes of intravitreal faricimab injection for diabetic macular edema. Medicina. 2023;59:665. doi:10.3390/medicina59040665
49. Al-Rufayie M, Palmieri F, Hamoud Bedan A, et al. Real-world results in treating diabetic macular edema with faricimab at a London-based tertiary eye hospital. Cureus. 2024;16:e75002. doi:10.7759/cureus.75002
50. Śpiewak D, Drzyzga Ł, Dorecka M, Witek K, Wyględowska-Promieńska D. Efficacy of faricimab in the treatment of diabetic macular edema and faricimab-related changes in OCT and OCT Angiography. Pharmaceutics. 2025;17:858. doi:10.3390/pharmaceutics17070858
51. Peto T, Sivaprasad S, Rhianon Reynolds R, et al. Effectiveness and safety of faricimab in eyes with DME in the United Kingdom: 1-year results from the FARWIDE-DME study. Invest Ophthalmol Vis Sci. 2025;66:2388.
52. Hirakata T, Hara F, Nochi Y, et al. Short-term real-world outcomes of diabetic macular edema treated with intravitreal faricimab. PLoS One. 2025;20:e0323088. doi:10.1371/journal.pone.0323088
53. Chakraborty D, Das S, Maiti A, et al. Clinical evaluation of faricimab in real-world diabetic macular edema in India- a multicenter observational study. Clin Ophthalmol. 2025;19:269–277. doi:10.2147/OPTH.S502033
54. Esteban-Floría O, Mateo J, Lara J, et al. Efficacy and safety of faricimab in diabetic macular edema: real-world outcomes in treatment-naïve and previously treated eyes. J Clin Med. 2025;14:6173. doi:10.3390/jcm14176173
55. Borkar DS, Tabano DC, Ali FS, et al. Early outcomes after initiation of faricimab in patients with diabetic macular edema. Ophthalmic Surg Lasers Imaging Retina. 2025;56:478–486. doi:10.3928/23258160-20250304-01
56. Hikichi T, Kurabe H, Notoya A, Oguro Y, Hirano M, Doi Y. Six-month comparative outcomes of aflibercept and faricimab in treatment-naïve macular edema secondary to branch retinal vein occlusion. Jpn J Ophthalmol. 2025;69:918–925. doi:10.1007/s10384-025-01254-8
57. Inokuchi S, Mizuki Y, Akihiro Kamata A, Onishi J, Hayashi T, Mizuki N. Real-world efficacy of intravitreal faricimab for macular edema secondary to retinal vein occlusion: short-term outcomes and optical coherence tomography biomarker analysis. Clin Ophthalmol. 2025;19:3669–3679. doi:10.2147/OPTH.S549896
58. Mansour AM, Lima LH, Battaglia Parodi M, Casella AMB, Cherfan DG, Arevalo JF. Outcomes of and surgical technique for treatment with high-dose aflibercept. J Vitreoretin Dis. 2025;9(5):628–631. doi:10.1177/24741264251352890
59. Kamao H, Goto K, Mizukawa K, Hiraki R, Miki A, Kimura S. Impact of punctate hyperfluorescence status on treatment outcomes of faricimab versus aflibercept in neovascular age-related macular degeneration. J Clin Med. 2025;14:6637. doi:10.3390/jcm14186637
60. Kuznik A, Coughlan A, Pinsent A, Toro-Diaz H, Sherman S, Patel N. Economic benefit of aflibercept 8 mg versus faricimab for neovascular age-related macular degeneration or diabetic macular edema in the US. Ophthalmol Ther. 2025;14:2863–2875. doi:10.1007/s40123-025-01236-6
61. Diack C, Gibiansky L, Jaminion F, et al. Ocular pharmacokinetics of faricimab following intravitreal administration in patients with retinal disease. Transl Vis Sci Technol. 2024;13:14. doi:10.1167/tvst.13.11.14
62. Do DV, Rhoades W, Nguyen QD. Pharmacokinetic study of intravitreal aflibercept in humans with neovascular age-related macular degeneration. Retina. 2020;40:643–647. doi:10.1097/IAE.0000000000002566
63. Paris A, Volpe G, Perruchoud-Ader K, Casanova A, Menghini M, Grimaldi G. Short-term intraocular pressure changes after intravitreal aflibercept 2 mg, aflibercept 8 mg and faricimab: a prospective, comparative study. Br J Ophthalmol. 2025;109:600–605. doi:10.1136/bjo-2024-326053
64. Lakhani M, Popovic MM, Al-Ani A, et al. Comparative analysis of ocular adverse events between aflibercept 8 mg and faricimab. a global population-based study across 65 countries. Ophthalmol Retina. 2026;10:373–384. doi:10.1016/j.oret.2025.10.019
65. Pandit SA, Momenaei B, Wakabayashi T, et al. Clinical outcomes of faricimab in patients with previously treated neovascular age-related macular degeneration. Ophthalmol Retina. 2024;8:360–366. doi:10.1016/j.oret.2023.10.018
66. Szigiato A, Mohan N, Talcott KE, et al. Short-term outcomes of faricimab in patients with neovascular age-related macular degeneration on prior anti-VEGF therapy. Ophthalmol Retina. 2024;8:10–17. doi:10.1016/j.oret.2023.08.018
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.