Back to Journals » Clinical Ophthalmology » Volume 19
Visual and Refractive Outcomes of Myopic Lenticule Extraction with the Zeiss VisuMax 500 and 800 Systems
Received 10 August 2025
Accepted for publication 19 December 2025
Published 30 December 2025 Volume 2025:19 Pages 4951—4956
DOI https://doi.org/10.2147/OPTH.S559787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Jonathan Philip Chung, Robert Andrew Paul
WA Laser Eye Centre, Alfred Cove, Western Australia, 6154, Australia
Correspondence: Jonathan Philip Chung, WA Laser Eye Centre, Suite 1/533 Canning Hwy, Alfred Cove, Western Australia, 6154, Australia, Email [email protected]
Purpose: This study aimed to compare the visual outcomes, safety and efficacy of myopic keratorefractive lenticule extraction treatments using the newer Zeiss VisuMax 800 system over its precursor, the VisuMax 500 system.
Patients and Methods: A retrospective review conducted at a private clinic in Western Australia of myopic keratorefractive lenticule extraction treatments with the VisuMax 500 and the VisuMax 800 systems between July 2021 and February 2023. Pre-operative and 1-month post-operative data were compared between the two cohorts. Demographics, best corrected visual acuity, uncorrected distance visual acuity, mean refractive spherical equivalent, total suction time and complications were recorded.
Results: Fifty procedures for each system were identified. Eight eyes in the VisuMax 500 cohort (group 1) and five eyes in the VisuMax 800 cohort (group 2) were excluded due to non-attendance at the 1-month post-operative review. The average total suction time was 34 seconds vs 13 seconds respectively. A single case of suction loss occurred in group 1. The mean pre-operative mean refractive spherical equivalent of groups 1 and 2 were − 6.02D (− 3.63 to − 9.00) and − 5.56D (− 2.75 to − 8.88) (P = 0.20). The mean post-operative mean refractive spherical equivalent of the two groups were 0.08D (− 1.00 to 1.25) and − 0.03D (− 2.25 to 1.00) (P = 0.31).
Conclusion: The VisuMax 500 and 800 systems have similar visual outcomes and no significant difference in safety profiles. The main advantage of the newer VisuMax 800 femtosecond laser is its speed and potential for less cases of suction loss. Larger studies over longer terms are required.
Keywords: KLEx, myopia, laser
Introduction
Keratorefractive lenticule extraction (KLEx) is the latest term to describe lenticule extraction procedures with the aim of refractive correction.1 Carl Zeiss Meditec AG introduced small incision lenticule extraction (SMILE) in 2011, a term to describe their proprietary effort in advancing refractive lenticule extraction procedures using their femtosecond laser.2 SMILE falls within the KLEx spectrum and involves the use of a femtosecond laser that can cut an intrastromal refractive lenticule within the cornea which is then removed manually via a small 3.0 to 5.0mm corneal incision.3 This process achieves corneal reshaping with the typical goal of correcting a patient’s myopia or myopic astigmatism. The benefits of SMILE have been well described. Clinically, SMILE has advantages over the more traditional laser in situ keratomileusis (LASIK) with studies indicating less rates of post-operative dry eye, better spherical aberration control, potentially biomechanically more stable corneas and no risk of flap complications.4–6 Practically, SMILE requires only a single laser compared to the well-known bimodal solution of LASIK.7
Given the increasing popularity of SMILE and the release of a newer model of the femtosecond laser (VisuMax 800, Carl Zeiss Meditec AG, Jena, Germany), we decided to compare this newer laser with the previous model (VisuMax 500, Carl Zeiss Meditec AG, Jena, Germany).8
The VisuMax 800 incorporates several technological improvements over the earlier VisuMax 500 that may influence both surgical efficiency and safety. The newer platform operates at a significantly higher laser repetition rate (2000 kHz vs 500 kHz), allowing for faster photodisruption and theoretically shorter overall suction time.
This study presents a comparison of the Zeiss VisuMax 800 to the VisuMax 500 laser.
Materials and Methods
The study was approved by the WA Laser Eye Centre review board and adhered to the principles of the Declaration of Helsinki. Individual patient consent was also obtained and made fully aware of the purpose of the study.
Patient Selection
A retrospective review of patient files of the last 50 myopic KLEx procedures performed using the VisuMax 500 (group 1) and the first 50 procedures performed using the VisuMax 800 (group 2) by a single ophthalmologist (RP). All data was collected from one centre in Perth, Western Australia between July 2021 and February 2023. Inclusion criteria were patients who were medically suitable for and received SMILE treatment. The single exclusion criterion was patients who did not return for a 1-month post-operative review.
Pre-Operative Assessment
Baseline data for each eye was collected including patient age, sex, uncorrected distance visual acuity (UDVA), best corrected visual acuity (BCVA), manifest refraction and intended visual outcome (eg mini-monovision).
To minimise potential confounding, all procedures were performed by the same highly experienced refractive surgeon using a standardized protocol. Baseline refractive error was measured pre-operatively to ensure comparability between groups. To reduce loss to follow-up bias, only patients who attended their 1-month post-operative review were included in the analysis.
Surgical Protocol
Group 1 eyes had KLEx treatment with the VisuMax 500 femtosecond laser and group 2 eyes were treated with the VisuMax 800 femtosecond laser. Single 4mm cap incisions were created in all eyes. The standard femtosecond laser protocol was followed to determine spot and track distances and energy settings to achieve a bubble pattern and separation (lenticule 3.5µm, lenticule cut 1.2µm, cap 3.2µm, cap cut 1.5µm, and energy 26 for both VisuMax500/800 systems).9 The cap thickness was 140µm and target refraction was set at +0.50D in all cases as per the surgeon’s nomogram. The minimum peripheral thickness of the lenticule was set at 15µm. Intraoperatively, the surgeon positioned the patient under the laser delivery arm, checked the laser data on the screen, and positioned the eye speculum to the eye. Once centration was achieved, suction was initiated to immobilize the eye. The femtosecond laser cutting was initiated via the foot pedal and once treatment was completed, suction was released. The lenticule was extracted using the Reinstein lenticule separator tool and grasping forceps. The tissue removed was inspected to check it was complete. Antibiotic (ciprofloxacin 0.3%) and steroid (dexamethasone 0.1%) eye drops were used four times per day for two weeks as standard prophylaxis once the procedure was complete. Intraoperative data collected for each patient included suction time and any complications including suction loss.
Post-Operative Assessment
Patients were followed up at day 1 and month 1 post-operatively. The 1-month post-operative data collected for each eye included UDVA, BCVA, and manifest refraction. Patients were subjectively refracted by the same experienced clinical optometrist, ensuring consistency and reducing inter-observer variability. Contrast sensitivity was tested through visual acuity contrast reduction testing at 12.5% with an electronic phoropter (Topcon Corporation, Tokyo, Japan).
Calculations and Statistical Analysis
The baseline and post-operative mean refractive spherical equivalent (MRSE) were calculated from manifest refractions. MRSE was chosen as it is the standard and most widely reported refractive outcome metric in refractive surgery studies. Visual acuity results were converted to LogMAR. Microsoft Excel 365 (Microsoft Corporation, Washington, USA) was used to record data, perform statistical tests and create graphs. Statistical analysis was verified using SPSS (IBM, New York, USA). Student’s t test was used to compare means, and Chi-Square test or Fisher’s exact test to compare groups. Hartley’s F-test was used to check whether the variances of the two groups were equal and normality was assumed under the Central Limit Theorem due to sample sizes greater than 30. A P value of less than 0.05 was considered as statistically significant.
Results
Fifty procedures were identified from each group. Eight eyes from group 1 and five eyes from group 2 met the exclusion criteria. Group 1 consisted of 42 procedures from 21 different patients compared to 45 procedures from 23 patients in group 2. Seven patients in group 1 and two patients in group 2 elected for mini-monovision, with a +1.25D add to the non-dominant eye. Patients in group 1 were significantly older compared to group 2 (P = 0.001, Student’s t test, unpaired, equal variance, two tailed). The average patient age was 36 years (20–49) and 32 years (21–48), respectively. The majority of patients were female, 87.5% in group 1 and 88% in group 2.
There was no significant difference in mean pre-operative MRSE between groups 1 and 2, −6.02D (−3.63 to −9.00) and −5.56D (−2.75 to −8.88) respectively (P = 0.20). There was also no significant difference in mean post-operative MRSE between the two groups 0.08D (−1.00 to 1.25) and −0.03D (−2.25 to 1.00) for groups 1 and 2 respectively (P = 0.31). Post-operatively, 81% (95% CI 69% to 93%) of cases fell within ±0.5D of targeted MRSE in group 1 compared to 94% (95% CI 87% to 100%) in group 2 however, there was no statistical difference between the two groups (P = 0.07, Chi-Square statistic 3.28). At the ±1.0D threshold, 98% of cases from group 1 and 96% of cases from group 2 fell within the targeted MRSE (P = 1.00, Fisher’s exact test).
Post-operatively, there was no loss of BCVA in any cases in either group. One hundred percent of cases from group 1 and 95.5% from group 2 achieved UDVA better than or equal to 20/30. At the 20/25 threshold, the results were 83.3% and 90.1% and at the 20/20 threshold the results were 72.2% and 79.5% for groups 1 and 2, respectively (Figure 1). There was no difference in contrast sensitivity at the 12.5% contrast threshold (P > 0.05).
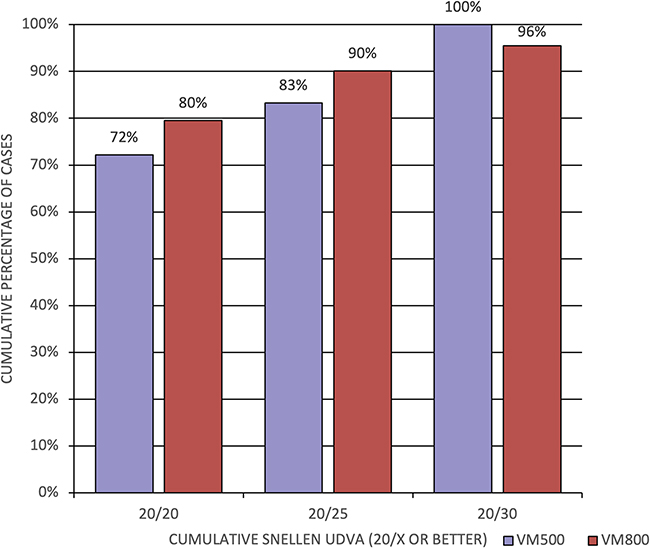 |
Figure 1 Percentage of cases after SMILE surgery achieving uncorrected distance visual acuity (UDVA) equal to or better than threshold values (20/20, 20/25, 20/30) compared between the VisuMax 500 (purple) and VisuMax 800 (red). There were no statistical differences between groups at any threshold. |
The average total suction time for group 1 was 34 seconds and for group 2 was 13 seconds. There was a single case where loss of suction occurred in group 1 and none in group 2. One patient from group 2 received further treatment in both eyes due to undercorrection. Their post-operative MRSE was −2.00D in the right eye and −2.25D in the left eye. In a scatter graph comparing attempted spherical equivalence correction to achieved correction, this patient appears as an outlier (Figure 2).
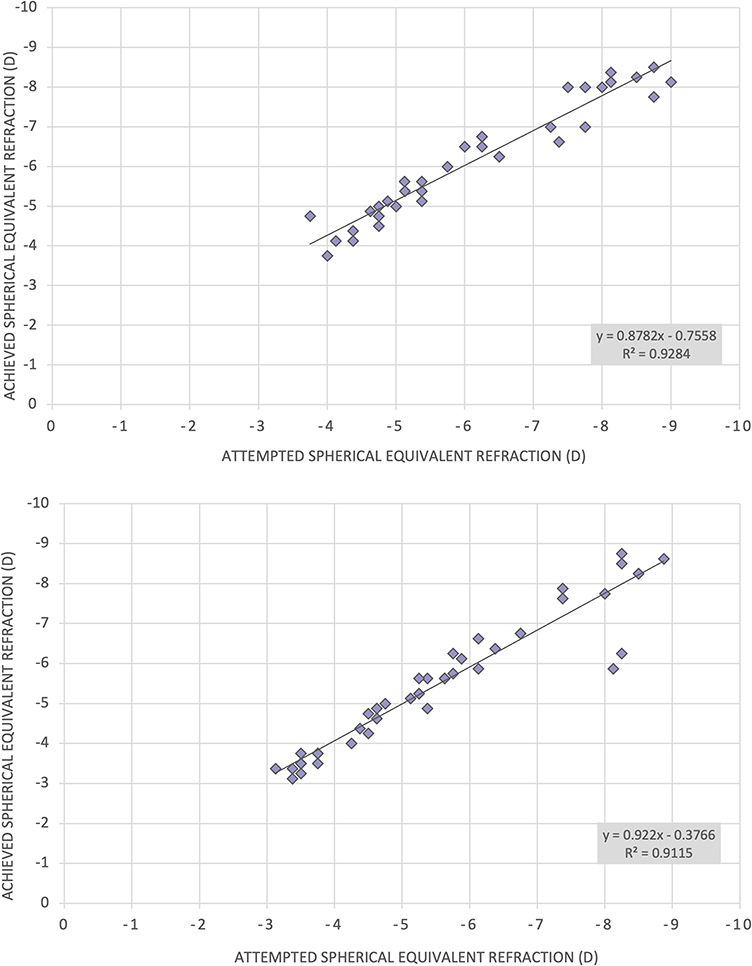 |
Figure 2 Attempted spherical equivalent refraction correction compared to achieved correction after SMILE surgery with the VisuMax 500 (top) and VisuMax 800 (bottom). The two outlying data points in the bottom panel represent a patient who required further treatment. |
Discussion
This single centre study compared myopic KLEx treatments using the VisuMax 500 versus the VisuMax 800 lasers. This approach is commonly known as SMILE surgery and was first introduced to the scientific literature in 2008 by Sekundo and Blum who used a femtosecond laser (VisuMax prototype, Carl Zeiss Meditec AG) to perform a flapless minimally invasive refractive procedure to correct myopia.10 The outcomes of their SMILE technique were published in 2011 and since then, there has been a significant increase in the interest and use of femtosecond lasers in the field of corneal lenticule refractive surgery.2
Over the past 12 years, SMILE has been adopted internationally for the treatment of myopia and myopic astigmatism. Long-term outcomes and safety profile data are available through published cohort studies.11–13 Comparisons with other corneal refractive procedures such as LASIK have also been performed and results from meta-analysis demonstrate comparative safety, efficacy and predictability outcomes.14 Studies have demonstrated that the SMILE procedure results in less post-operative dry eye disease compared with LASIK which can be a quality of life consideration for patients who have the choice between these two procedures.15
The latest femtosecond laser VisuMax 800 was released in 2021 and claims some advantages over the previous model, the VisuMax 500. One of the main advantages advertised has been improved speed with the VisuMax 800 operating at 2000 kHz compared to the 500 kHz of the previous model. Results from our study showed that the average total suction time when using the VisuMax 800 was less than half compared to the VisuMax 500, 13s and 34s, respectively.
There was no significant difference between the VisuMax 500 and the VisuMax 800 when comparing pre- or post-operative MRSE. There were more cases that fell within 0.5D of the targeted MRSE in the VisuMax 800 cohort (94%) compared to the VisuMax 500 cohort (81%); however, this was not a statistically significant result (P = 0.07) and at the 1.0D threshold there was very little difference between the two groups, 98% and 96% respectively. These results suggest that post-operative visual outcomes are not a differentiating factor in choosing between the two devices.
There was one case of suction loss in the VisuMax 500 cohort and no cases in the VisuMax 800 cohort. The rates of suction loss during SMILE procedures have reduced over time with surgeon experience and improved device software. An incidence rates of between 0.5% and 0.93% have been reported in recent studies.11,16 Over 60% of suction loss occurs after 10s so theoretically there should be less cases of suction loss with the VisuMax 800.17 No other intraoperative complications were noted in this study. One patient (both eyes) was unhappy with their post-operative UDVA from the VisuMax 800 cohort and was retreated with a successful visual outcome of 20/20 (uncorrected) in both eyes.
Some limitations of the study are that the results of this study should be interpreted in the context of a single centre, with all cases operated on by a single experienced refractive ophthalmologist. As such the results were less likely to be affected by surgeon variability factors. However, the results are also more susceptible to selection bias given the size of the centre with only one surgeon. The fact that most cases were female in both cohorts and that the VisuMax 500 cohort was significantly older than the VisuMax 800 can theoretically affect the results and may be areas that future studies can address. Likely explanations for the patients who did not return for a 1-month follow-up may be due to their occupation as fly-in-fly-out workers or because they live in rural country towns especially if they were asymptomatic and happy with their vision.
Conclusion
In this study, both the VisuMax 500 and VisuMax 800 femtosecond laser systems demonstrated comparable safety and visual outcomes for myopic keratorefractive lenticule extraction, with no statistically significant differences in refractive predictability or post-operative visual acuity. The VisuMax 800, however, required shorter suction times, reflecting a procedural efficiency advantage. While clinical outcomes were comparable, the increased speed and potential for reduced suction-related complications may offer practical benefits in surgical workflow and patient comfort. Further multicentre studies with larger sample sizes and longer follow-up are warranted to confirm these findings.
Disclosure
Professor Robert Paul reports travel reimbursement from Zeiss, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Dupps WJ, Randleman JB, Kohnen T, Srinivasan S, Werner L. Scientific nomenclature for keratorefractive lenticule extraction (KLEx) procedures: a joint editorial statement. J Cataract Refract Surg. 2023;49(11):1085. doi:10.1097/j.jcrs.0000000000001328
2. Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95(3):335–339. doi:10.1136/bjo.2009.174284
3. Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: all-in-one femtosecond laser refractive surgery. J Cataract Refract Surg. 2011;37(1):127–137. doi:10.1016/j.jcrs.2010.07.033
4. Sekundo W, Gertnere J, Bertelmann T, Solomatin I. One-year refractive results, contrast sensitivity, high-order aberrations and complications after myopic small-incision lenticule extraction (ReLEx SMILE). Graefes Arch Clin Exp Ophthalmol. 2014;252(5):837–843. doi:10.1007/s00417-014-2608-4
5. Shetty R, Francis M, Shroff R, et al. Corneal biomechanical changes and tissue remodeling after SMILE and LASIK. Invest Ophthalmol Vis Sci. 2017;58(13):5703–5712. doi:10.1167/iovs.17-22864
6. Kobashi H, Kamiya K, Shimizu K. Dry eye after small incision lenticule extraction and femtosecond laser-assisted LASIK: meta-analysis. Cornea. 2017;36(1):85–91. doi:10.1097/ICO.0000000000000999
7. Ang M, Tan D, Mehta JS. Small incision lenticule extraction (SMILE) versus laser in-situ keratomileusis (LASIK): study protocol for a randomized, non-inferiority trial. Trials. 2012;13:75. doi:10.1186/1745-6215-13-75
8. Ang M, Gatinel D, Reinstein DZ, Mertens E, Alió Del Barrio JL, Alió JL. Refractive surgery beyond 2020. Eye. 2021;35(2):362–382. doi:10.1038/s41433-020-1096-5
9. Reinstein DZ. The Surgeon’s Guide to SMILE: Small Incision Lenticule Extraction. Slack Incorporated; 2018.
10. Sekundo W, Kunert K, Russmann C, et al. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: six-month results. J Cataract Refract Surg. 2008;34(9):1513–1520. doi:10.1016/j.jcrs.2008.05.033
11. Wang Y, Ma J, Zhang J, et al. Incidence and management of intraoperative complications during small-incision lenticule extraction in 3004 cases. J Cataract Refract Surg. 2017;43(6):796–802. doi:10.1016/j.jcrs.2017.03.039
12. Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology. 2014;121(4):822–828. doi:10.1016/j.ophtha.2013.11.006
13. Blum M, Lauer AS, Kunert KS, Sekundo W. 10-year results of small incision lenticule extraction. J Refract Surg. 2019;35(10):618–623. doi:10.3928/1081597X-20190826-02
14. Fu Y, Yin Y, Wu X, et al. Clinical outcomes after small-incision lenticule extraction versus femtosecond laser-assisted LASIK for high myopia: a meta-analysis. PLoS One. 2021;16(2):e0242059. doi:10.1371/journal.pone.0242059
15. Denoyer A, Landman E, Trinh L, Faure JF, Auclin F, Baudouin C. Dry eye disease after refractive surgery: comparative outcomes of small incision lenticule extraction versus LASIK. Ophthalmology. 2015;122(4):669–676. doi:10.1016/j.ophtha.2014.10.004
16. Reinstein DZ, Archer TJ, Vida RS, Carp GI. Suction stability management in small incision lenticule extraction: incidence and outcomes of suction loss in 4000 consecutive procedures. Acta Ophthalmol. 2020;98(1):e72–e80. doi:10.1111/aos.14215
17. Reinstein DZ, Archer TJ, Potter JG, Gupta R, Wiltfang R. Refractive and visual outcomes of SMILE for compound myopic astigmatism with the VISUMAX 800. J Refract Surg. 2023;39(5):294–301. doi:10.3928/1081597X-20230301-02
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Three-Month Outcomes of SMILE Pro with the VISUMAX 800 for Myopic Astigmatism in a Large Population
Cung HS, Tran LHT, Tran TN
Clinical Ophthalmology 2025, 19:417-425
Published Date: 7 February 2025