Back to Journals » Clinical Ophthalmology » Volume 19
Visual and Refractive Outcomes of a New Monofocal, Non-Constant Aberration-Correcting Aspheric Intraocular Lens
Authors Agarwal S ![]() , Thornell E
, Thornell E ![]()
Received 6 May 2025
Accepted for publication 1 September 2025
Published 18 September 2025 Volume 2025:19 Pages 3439—3447
DOI https://doi.org/10.2147/OPTH.S538686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Smita Agarwal,1,2,* Erin Thornell1,*
1Wollongong Eye Specialists, Wollongong, NSW, Australia; 2Graduate School of Medicine, University of Wollongong, Wollongong, NSW, Australia
*These authors contributed equally to this work
Correspondence: Smita Agarwal, Wollongong Eye Specialists, Level 2, 2 Victoria St, Wollongong, NSW, 2500, Australia, Tel +61242276388, Email [email protected]
Purpose: To assess early visual and refractive outcomes of the CT Lucia 621PY intraocular lens (IOL).
Methods: Retrospective analysis was performed for 47 consecutive eyes from 33 patients following routine phacoemulsification and implantation of CT Lucia 621PY monofocal IOLs for the treatment of cataract. Postoperative analysis was performed 6-weeks following surgery. Uncorrected distance visual acuity (UDVA), best-corrected distance visual acuity (BCVA) and manifest refraction were measured for all patients. Uncorrected mesopic contrast sensitivity (CS) was measured for a subset of 22 of the 47 eyes, and modulated transfer function (MTF) and angle alpha and angle kappa were measured for a separate subset of 19 eyes.
Results: Mean spherical equivalent (SE) was − 0.04± 0.38 D, with 83% of eyes achieving within ± 0.5 D of the refractive target. Mean UDVA was 0.05± 0.1 LogMAR at 6 weeks postoperative, with 98% of eyes achieving 0.2 LogMAR or better. Mean BCVA was − 0.02± 0.06 LogMAR, with 87% of eyes achieving 0.00 LogMAR or better. Mean mesopic monocular CS was 1.4± 0.26 sec arc, and 50% contrast was maintained at a spatial frequency of approximately 13 cycles per degree. There was no significant correlation between MTF and angle alpha or angle kappa.
Conclusion: The CT Lucia 621PY offers good visual and refractive outcomes. While there was no significant correlation between angle alpha or angle kappa and visual quality, further investigation is warranted.
Keywords: cataract surgery, monofocal intraocular lens, non-constant aberration IOL, alpha and kappa angles
Introduction
Worldwide, 90% of the intraocular lenses (IOLs) implanted during cataract surgery are monofocal, non-toric lenses.1 It is well accepted that positive corneal spherical aberrations (SA) are common in the general public,2 and that spherical IOLs add to this pre-existing positive SA, increasing the overall ocular SA. With the advent of aspheric IOLs, slight peripheral flattening was introduced as a means of correcting corneal SA. While spherical and aspheric IOLs provide similar visual outcomes,3 the light scattering spherical IOLs can compromise visual quality,4 with an inverse relationship between SA and contrast sensitivity (CS).5
The ability of aspheric IOLs to provide excellent visual and subjective outcomes is dependent upon the IOL being well centered, which can be compromised by other factors such as angle kappa, IOL tilt and pupil size.3,6 These same factors are less problematic in aberration-free IOLs that neither correct nor induce SA.7 However, aberration-free IOLs do not maintain visual quality to the same extent as aspheric IOLs due to the uncorrected corneal SA and reduced tolerance to decentration.8 In a real-world setting, the amount of preoperative angle alpha and angle kappa may be used as indicators about the likelihood a patient may experience decentration of an IOL, making IOLs with a high tolerance to decentration a better choice for those patients.
The CT Lucia 621P and 621PY IOLs (Carl Zeiss Meditec AG, Jena, Germany) are hydrophobic acrylic heparin-coated monofocal lenses (Table 1) that feature a gradual transition of negative SA to positive SA to counteract central corneal SA while having a neutral effect in the periphery, thereby increasing tolerance to decentration.9 The 621PY differs from the 621P IOL in that it also has a blue light filtering chromophore. Previous clinical studies have reported good predictability and visual outcomes,9 and good quality of vision due to low postoperative SA.10 While the optic design of the CT Lucia IOLs hypothetically improves tolerance to decentration, reports on this are limited to benchtop studies. In one benchtop study that assessed modulation transfer function (MTF) and Strehl Ratio (SR) of the CT Lucia 621PY IOL, Borkenstein et al reported that the IOL performed well even with 1 mm decentration and 5° tilt.8 This was supported by another recent benchtop study that compared 621PY to another blue light filtering monofocal IOL (Clareon; Alcon, Ft. Worth, Texas, USA), reporting that 621PY performed better, with superior MTF with 1mm decentration and 5° tilt.11 To date, there has been little clinical evidence on the visual outcomes of the CT Lucia 621PY IOL outside the U.S, and to the authors’ knowledge, little investigation into how the eye performs with high angle kappa or angle alpha. Both angle kappa and angle alpha are recognized as factors that affect postoperative outcomes,12–22 although most of the published literature has evaluated these factors in patients undergoing cataract surgery with advanced technology IOLs rather than monofocal IOLs.12–21
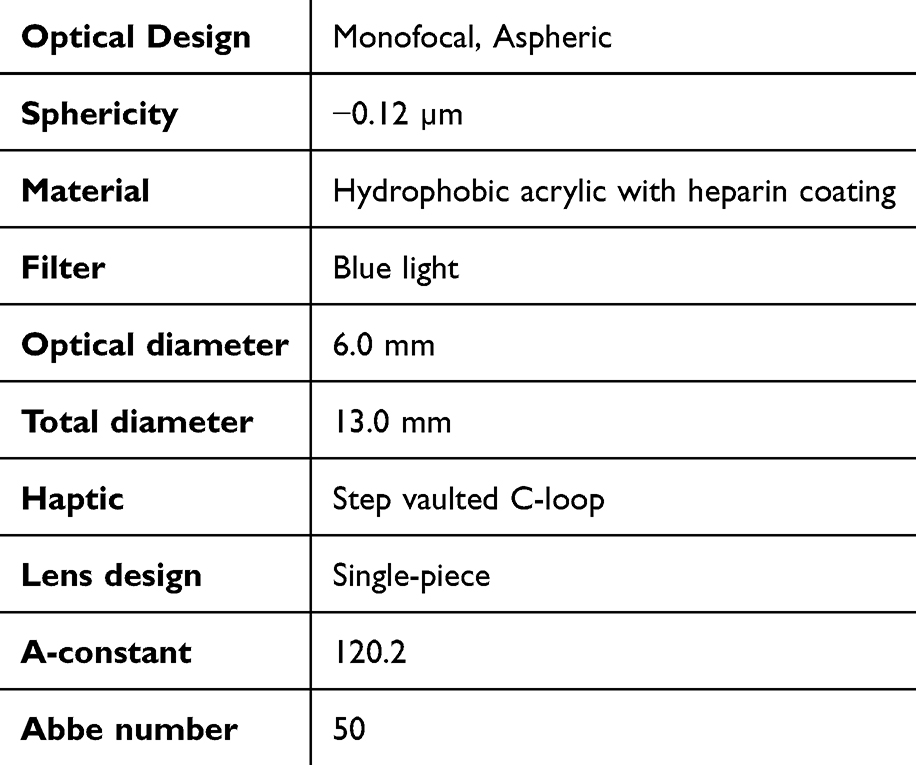 |
Table 1 Lens Specifications of the CT Lucia 621PY IOL |
Therefore, this study represents the first “real world” analysis on the clinical outcomes of the CT Lucia 621PY IOL in Australia. Visual and refractive outcomes were analyzed, with an emphasis on angle alpha and angle kappa and their impact on visual quality in patients being implanted with a monofocal IOL.
Materials and Methods
The CT Lucia 621P and CT Lucia 621PY IOLs are non-constant aberration-correcting IOLs, with a gradual transition of negative to positive SA towards the periphery. We conducted a descriptive retrospective chart review of 47 consecutive eyes from 33 patients who had undergone routine phacoemulsification and IOL implantation for the treatment of cataract. Data was included for eyes that were implanted with the CT Lucia 621PY IOL. Data was excluded for eyes that experienced intra- or postoperative complications, had preoperative astigmatism of ≥1.0 D (based on biometry), had previous history of keratorefractive procedures, had pre-existing ocular pathology that may compromise visual outcomes or were corrected for a near target.
Preoperative Evaluation
Biometry was performed preoperatively (IOLMaster 700; Carl Zeiss Meditec), and the Barrett TK Universal II formula was used to calculate lens powers, with a predicted refractive target of ±0.25 D. Retinal optical coherence tomography and dilated fundus examinations were performed to identify any pre-existing ocular conditions that may affect surgical outcomes.
Surgical Technique
All surgeries were performed by a single surgeon (SA) following standard surgical procedure (at three separate sites). Briefly, a 2.3 mm corneal incision was made along with two 1 mm side ports at 180°. A circular capsulorhexis was made followed by phacoemulsification and aspiration of lenticular material. Each eye then received a CT Lucia 621PY IOL inserted into the capsular bag. Postoperatively, patients were instructed to apply one drop each of ofloxacin 0.3% ophthalmic solution (Ocuflox; Allergan; Dublin, Ireland) and prednisolone acetate 1% ophthalmic suspension (Prednefrine forte; Allergan) eye drop, one drop every 2 hours on the day of surgery and QID thereafter for 2- and 4-weeks, respectively. Patients were also instructed to commence ketorolac trimethomine 0.5% ophthalmic solution (Acular; Allergan) eye drops 1 week after surgery, applying 1 drop QID and continuing for 1 week (until the end of the second week).
Postoperative Evaluation
Postoperative analysis was performed 6 weeks after surgery. Monocular uncorrected distance visual acuity (UDVA), best corrected distance visual acuity (BCVA), and manifest refraction were measured using a Snellen chart placed at 6 meters under photopic conditions. Uncorrected CS was measured for a subset of 22 eyes (based on availability of equipment), using a Pelli Robson chart placed at 6 meters under mesopic conditions. Automated total MTF was measured for a separate subset of 19 eyes (based on availability of equipment) using an automated aberrometer (iTrace; Tracey Technologies; Texas, USA). Angle kappa and angle alpha were measured for the same subset of 19 eyes using an automated aberrometer (iTrace; Tracey Technologies; Houston, Texas, USA).
Statistical Analysis
A Pearson correlation test was performed using Microsoft Excel with the statistical add on (2019, version 16.0, Microsoft Corporation, Redmond, WA, USA) to identify any relationship between MTF measured at each contrast value (ie 5, 10, 15, 20, 25 and 30 cpd) and angle alpha and angle kappa. A P-value ≤0.05 was considered statistically significant.
This study was conducted according to the principles of the Declaration of Helsinki and has received approval from the University of Wollongong Human Research Ethics Committee (2024/281; approval date 06/11/2024). Informed patient consent was received as part of this study.
Results
A total of 47 eyes from 33 patients (67% female; mean age 71.1±7.4 years) were included for analysis. Bilateral surgery was performed on 14 patients (42%); 76% of all surgeries were performed on the right eye. Mean cataract grade as measured using the LOCS III scale was 3.1±0.69 (range 2–4) and mean preoperative CDVA was 0.31±0.21 LogMAR. Mean preoperative SE was 0.89±2.0 D, with 72% of eyes having preoperative cylinder ≤0.5 D and 89% ≤0.75D (mean preoperative cylinder 0.51±0.34).
Mean SE improved to −0.04±0.38 D at 6 week postoperative (range −1.125 to 0.75 D; Table 2), with 83% and 98% of eyes achieving within ±0.5 D and ±1.0 D of the refractive target, respectively (Figures 1 and 2).
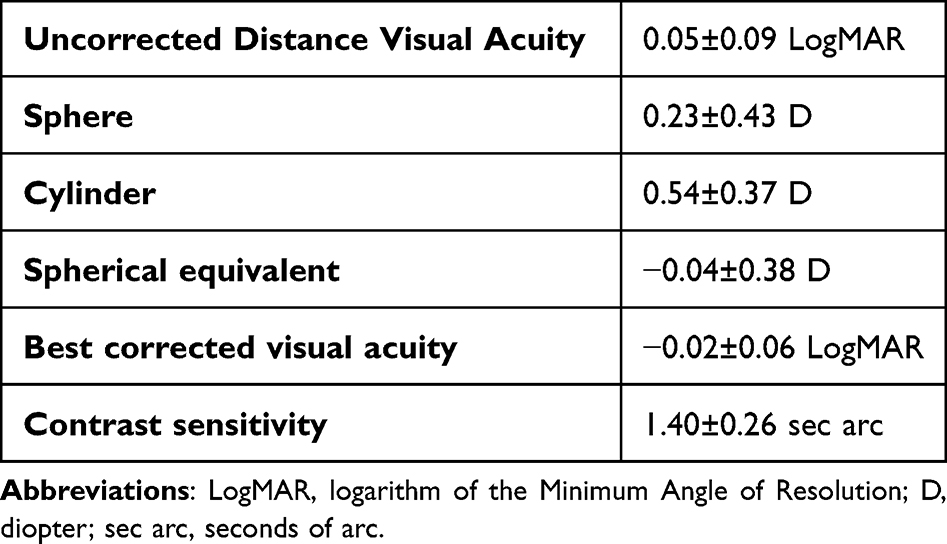 |
Table 2 Postoperative Outcomes at 6 weeks Following Surgery (N=47) |
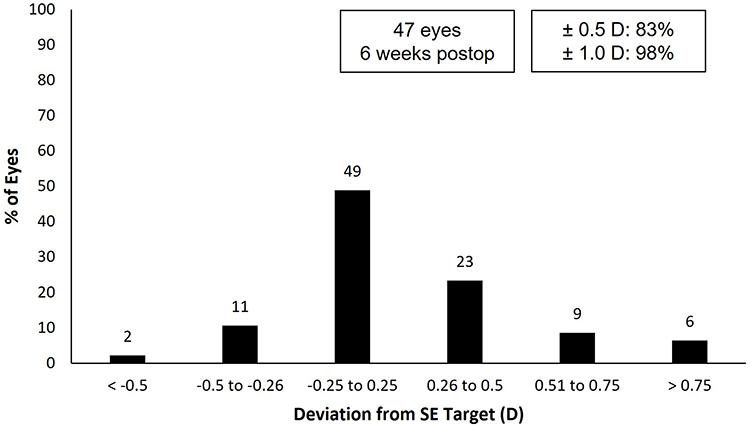 |
Figure 1 Deviation of postoperative spherical equivalent from target. |
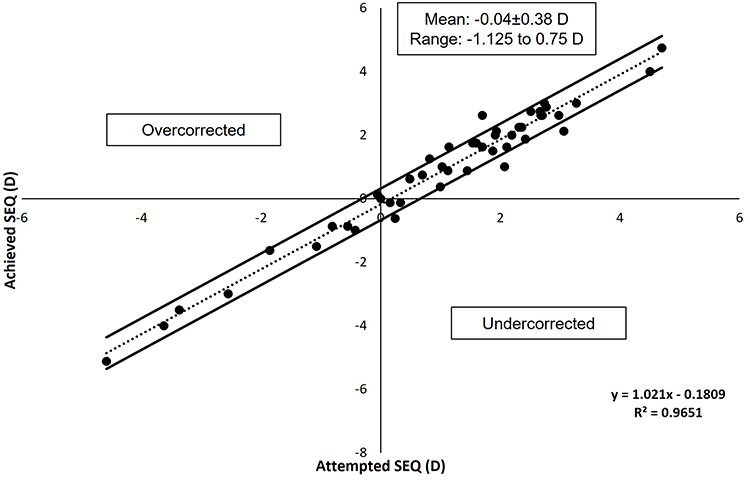 |
Figure 2 Attempted versus achieved spherical equivalent correction. |
Mean UDVA was 0.05±0.09 LogMAR at 6 weeks postoperative (Table 2), with 62% and 98% of eyes achieving 0.0 LogMAR and 0.2 LogMAR or better, respectively (Figure 3). Mean BCVA was −0.02±0.06 LogMAR (Table 2), with 94% of eyes achieving 0.00 LogMAR or better (Figure 3). Postoperative UDVA was the same or better than postoperative BCVA in 47% of eyes (13 eyes) and within 1 line of BCVA in 83% of eyes (25 eyes; Figure 4).
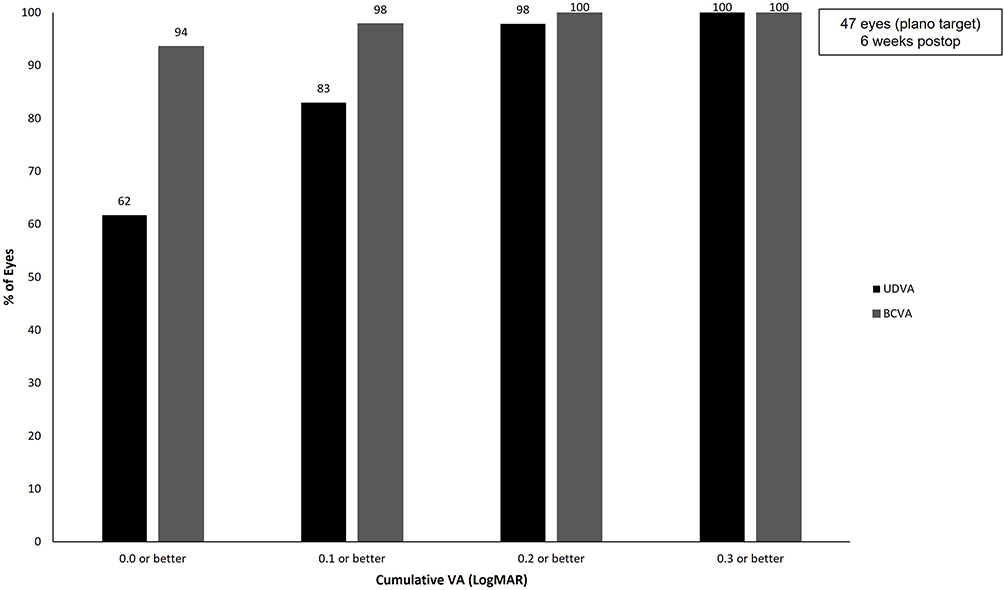 |
Figure 3 Cumulative postoperative monocular visual acuity. Abbreviations: BCVA, best corrected distance visual acuity; UDVA, uncorrected distance visual acuity; VA, visual acuity; LogMAR, logarithm of the Minimum Angle of Resolution. |
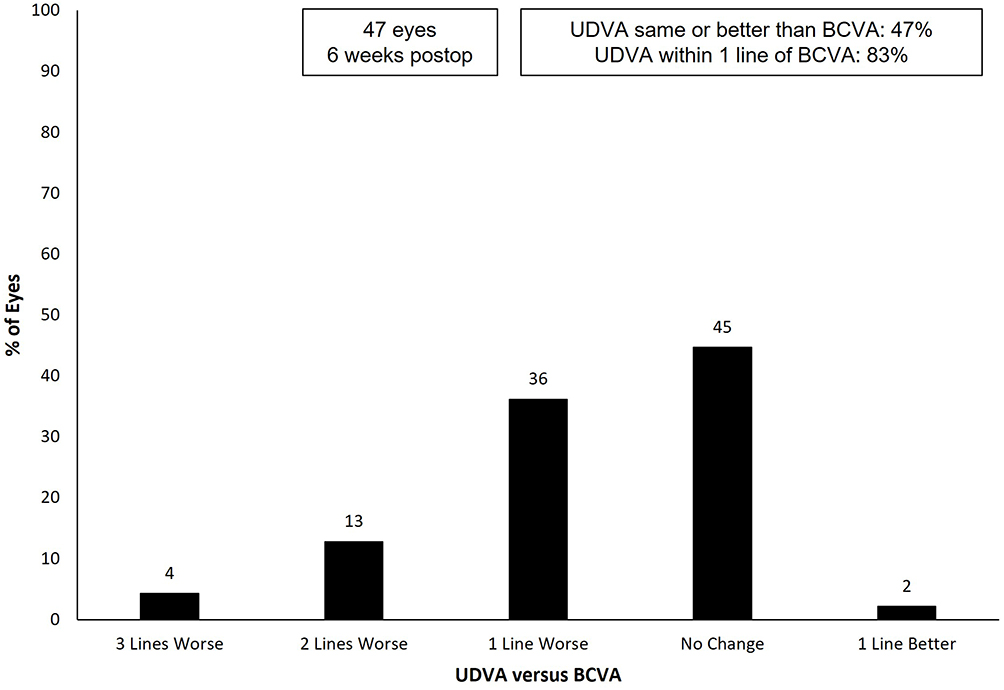 |
Figure 4 Difference between postoperative monocular uncorrected and best corrected distance visual acuity in LogMAR. Abbreviations: LogMAR, logarithm of the Minimum Angle of Resolution; BCVA, best corrected distance visual acuity; UDVA, uncorrected distance visual acuity. |
Mean mesopic monocular CS for a subset of 22 eyes was 1.40±0.26 sec arc (Table 2). Figure 5 shows the MTF as a function of spatial frequency for a subset of 19 eyes; 50% contrast is achieved at a spatial frequency of approximately 10 cycles/degree (cpd). Mean angle alpha was 0.47±0.20 mm and mean angle kappa was 0.95±1.37 mm (skewed by 3 eyes with alpha kappa >3.5 mm). There was no significant correlation between angle alpha and MTF at any spatial frequency (5 cpd [r = 0.162, P = 0.51]; 10 cpd [0.170, P = 0.49]; 15 cpd [r = 0.224, P = 0.35]; 20 cpd [r = 0.267, P = 0.27]; 25 cpd [r = 0.267, P = 0.28]; 30 cpd [r = 0.236, P = 0.33]) or angle kappa (5 cpd [r = −0.180, P = 0.52]; 10 cpd [−0.200, P = 0.47]; 15 cpd [r = −0.159, P = 0.35]; 20 cpd [r = −0.307, P = 0.26]; 25 cpd [r = −0.291, P = 0.29]; 30 cpd [r = −0.291, P = 0.29]).
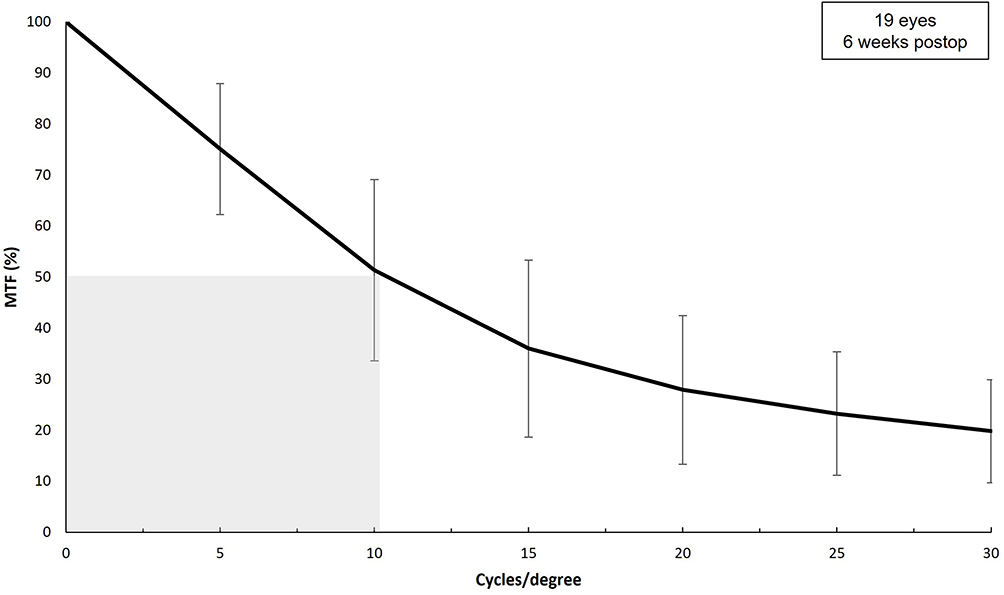 |
Figure 5 Postoperative uncorrected monocular modulation transfer function as a spatial frequency. Abbreviation: MTF, modulation transfer function. |
Discussion
This study evaluated the CT Lucia 621PY monofocal IOL in a real-world clinic setting. The authors found the lens provided good visual and refractive outcomes, with 83% of eyes having UCDA within 1 line of BCVA, and 62% of eyes achieved 0.0 logMAR or better. Furthermore, good objective quality of vision as measured using MTF was maintained even in eyes with larger angles kappa.
To date, published data on the lens is currently limited to two benchtop studies,8,11 with few recently published clinical studies reporting on outcomes from the 621P IOL.9,10,23,24 This is the first real world clinical study outside of Europe to report visual and refractive outcomes of the CT Lucia 621PY IOL; and the first to investigate the relationship between visual quality and angle kappa within the CT Lucia 621 family.
Our results add to the published literature on the CT Lucia 621 family of lenses; the primary difference between the 621 P and 621PY IOLs is that the latter incorporates a blue light filtering chromophore. Both lenses are hydrophobic acrylic and feature a C-loop platform haptics with an optimized Zeiss optic non-constant aberration aspheric design. Garcia-Tomas et al23 recently published outcomes of 55 eyes (45 patients) implanted with the CT Lucia 621P IOL. At postop month 3, the authors reported the mean Snellen decimal UDVA and DCVA were 1.07±0.15 and 1.13±0.11, respectively, with 94.55% of eyes achieving Snellen VA of 20/20 or better.23 Additionally, CS functions were good and similar at all spatial frequencies. Hernandez-Martinez et al24 reported visual outcomes of 90 eyes (86 patients) implanted with CT Lucia 621P. At postop month 1, patients had a mean Snellen decimal UDVA of 0.64±0.22 and CDVA of 0.89±0.13, but only 8.9% of eyes achieved Snellen VA of 20/20 or better. While the authors did not specifically address these outcomes, uncorrected refractive error is a likely explanation. Schallhorn et al9 evaluated 191 eyes (133 patients) with a mean follow-up of 1.7 months. Mean postop UDVA was 0.09±0.16 logMAR, with 77.5% of eyes achieving 20/20 or better UDVA. Our study reported 62% of patients achieved 0.0 LogMAR.
All of these studies reported a similar or higher percentage of eyes within ±0.5 D than was reported here: Garcia-Tomas et al, 92.3%; Hernandez-Martinez et al, 73.3%; Schallhorn et al, 84.8%; whereas we reported 83% of eyes within ±0.5 D. Differences in these outcomes may be a result of biometry used (SRK/T and Hoffer-Q in the Hernandez-Martinez et al study, Barrett in the Garcia-Tomas et al study, and Haigis in the Schallhorn et al study),9,23,24 whereas we used the Barrett TK Universal II formula. We also evaluated patients at postop week 6, whereas the other studies evaluated patients at postop month 1 (Hernandez-Martinez et al) or postop month 3 (Garcia-Tomas et al).23 Schallhorn et al reported a mean follow-up of 1.7±1.3 months (range, 1–8 months).9
Aberration-free IOLs are tolerant to decentration;25 Kim et al26 reported much higher reduction in contrast with 1 mm decentration in monofocal aspheric IOLs (12.2% to 15.8%) compared to monofocal aberration-free IOLs (3.1% to 5.1%). Other studies have compared monofocal aspheric IOLs to multifocal or trifocal IOLs and consistently find aspheric monofocal lenses to be most tolerant of decentration, although that benefit can diminish if decentration is >0.5 mm.27–29 Borkenstein et al8 compared the performance of the CT Lucia 621PY IOL with standard aspheric and spheric IOL models and found the IOL maintained good visual quality (as measured in vitro using MTF and Strehl ratio) even with 1 mm decentration and 5° tilt. Much of the previous research that has investigated the relationship between angle alpha and angle kappa with visual quality has focused on multifocal IOLs,16,20,21,30,31 as misalignment between the visual axis and the distance optic can cause visual disturbances. However, despite decentration also being associated with loss of visual quality with monofocal IOLs,29 reports of tolerance of the CT Lucia 621PY IOL are currently restricted to benchtop studies, and there are no studies currently reporting on how ocular anatomy may affect visual quality with this lens.
Although our results do not reach statistical significance, there was a negative correlation between angle kappa and MTF which became more notable (ie more negative r value and a lower P value) with higher contrast levels. Of the 19 eyes that were measured, 3 eyes had angle kappa over 3.5 mm. Notably, while the number of eyes were too few to perform stratified statistical analyses (ie compare groups with high versus low angle kappa), these eyes did not seem to differ in MTF compared to eyes with much lower angle kappa values (data not shown). While future studies with larger data sets stratified according to angle kappa values may elucidate this further, these early findings suggest that the ZO optic design may in fact help negate the risk of reduced visual quality in eyes with large angle kappa.
As part of an in vitro study using CT Lucia 621 P IOLs implanted in cadaver eyes, Zhang et al32 reported a longer arc in contact with the capsule and the absence of capsule striae when compared to other lens models. This may suggest that the CT Lucia 621PY IOL would have good stability in the bag and may have lower rates of posterior capsular opacification due to its sharp edge haptic and its large surface area in contact with the capsular bag and optic haptic junction. This offers another area of future study, along with rotational stability in the bag (for a toric version, if one is commercially available).
Limitations of this study include a small sample size and use of both eyes from some patients, lack of a comparison group, incomplete data due to equipment availability and the retrospective nature of the study, the lack of direct measurement of postoperative IOL decentration and tilt, and the absence of a control or comparison group. Future studies involving a comprehensive analysis of IOL positioning in situ, large sample sizes with stratification of angle kappa values, and comparison with other monofocal IOL models will help elucidate the findings of this study.
Conclusion
The data presented here suggests that good visual outcomes can be achieved with the CT Lucia 621PY IOL. Notably, preliminary findings also provide evidence for high tolerance in eyes with ocular anatomy predisposed to IOL decentration (ie high angle kappa). Further investigation into how the ZO optic of the CT Lucia 621PY IOL may help maintain quality of vision in eyes at risk of decentration (ie large angle kappa), pseudoexfoliation and zonular insufficiency is justified. However, these limitations are secondary to the study findings, the first “real world” clinical outcomes in Australia.
Acknowledgments
Michelle Dalton, ELS, provided medical writing and editing; this was funded by Carl Zeiss Meditec. Clinical staff of Wollongong Eye Specialists assisted in data acquisition.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Market Scope. IOL report: a global market analysis for 2019 to 2025. Market scope. 2023.
2. Lai YJ, Yeh SI, Cheng HC. Distribution of corneal and ocular spherical aberrations in eyes with cataract in the Taiwanese population. Taiwan J Ophthalmol. 2015;5(2):72–75. doi:10.1016/j.tjo.2015.03.003
3. Martinez-Plaza E, Lopez-de la Rosa A, Papadatou E, et al. Influence of decentration and tilt of tecnis ZCB00 on visual acuity and higher order aberrations. Eye. 2023;37(8):1640–1645. doi:10.1038/s41433-022-02211-2
4. Chen Y, Wang X, Zhou CD, Wu Q. Evaluation of visual quality of spherical and aspherical intraocular lenses by optical quality analysis system. Int J Ophthalmol. 2017;10(6):914–918. doi:10.18240/ijo.2017.06.13
5. van Gaalen KW, Jansonius N, Koopmans S, Terwee T, Kooijman AC. Relationship between contrast sensitivity and spherical aberration. J Cataract Refract Surg. 2009;35(1):47–56. doi:10.1016/j.jcrs.2008.09.016
6. Xu J, Lin P, Zhang S, Lu Y, Zheng T. Risk factors associated with intraocular lens decentration after cataract surgery. Am J Ophthalmol. 2022;242:88–95. doi:10.1016/j.ajo.2022.05.005
7. McKelvie J, McArdle B, McGhee C. The influence of tilt, decentration, and pupil size on the higher-order aberration profile of aspheric intraocular lenses. Ophthalmology. 2011;118(9):1724–1731. doi:10.1016/j.ophtha.2011.02.025
8. Borkenstein AF, Borkenstein EM, Luedtke H, Schmid R. Impact of decentration and tilt on spherical, aberration correcting, and specific aspherical intraocular lenses: an optical bench analysis. Ophthalmic Res. 2022;65(4):425–436. doi:10.1159/000522510
9. Schallhorn SC, Teenan D, Venter JA, Schallhorn JM, Hannan SJ. Early clinical experience with a new hydrophobic acrylic single-piece monofocal intraocular lens. Clin Ophthalmol. 2023;17:3419–3427. doi:10.2147/OPTH.S433530
10. Han J, Lee YE, Park N, et al. Comparison of short-term clinical outcomes after implantation of two monofocal, aspheric intraocular lenses. Diagnostics. 2024;14(24). doi:10.3390/diagnostics14242862
11. Yan W, Auffarth GU, Khoramnia R, Labuz G. Blue-light filtering monofocal intraocular lenses: a study on optical function and tolerance to misalignment. J Refract Surg. 2024;40(2):e79–e88. doi:10.3928/1081597X-20240112-02
12. Ang RET, Doroy ZAM, Yao JAA, Cruz EM. Correlation of angle kappa and angle alpha on visual outcomes in eyes implanted with three types of multifocal intraocular lenses. Sci Rep. 2024;14(1):26732. doi:10.1038/s41598-024-77699-7
13. Wang Q, Stoakes IM, Moshirfar M, Harvey DH, Hoopes PC. Assessment of pupil size and angle kappa in refractive surgery: a population-based epidemiological study in predominantly American caucasians. Cureus. 2023;15(8):e43998. doi:10.7759/cureus.43998
14. Prakash G, Prakash DR, Agarwal A, Kumar DA, Agarwal A, Jacob S. Predictive factor and kappa angle analysis for visual satisfactions in patients with multifocal IOL implantation. Eye. 2011;25(9):1187–1193. doi:10.1038/eye.2011.150
15. Garzon N, Garcia-Montero M, Lopez-Artero E, et al. Influence of angle kappa on visual and refractive outcomes after implantation of a diffractive trifocal intraocular lens. J Cataract Refract Surg. 2020;46(5):721–727. doi:10.1097/j.jcrs.0000000000000156
16. Fu Y, Kou J, Chen D, et al. Influence of angle kappa and angle alpha on visual quality after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2019;45(9):1258–1264. doi:10.1016/j.jcrs.2019.04.003
17. Mahr MA, Simpson MJ, Erie JC. Angle alpha orientation and magnitude distribution in a cataract surgery population. J Cataract Refract Surg. 2020;46(3):372–377. doi:10.1097/j.jcrs.0000000000000066
18. Grzybowski A, Eppig T. Angle alpha as predictor for improving patient satisfaction with multifocal intraocular lenses? Graefes Arch Clin Exp Ophthalmol. 2021;259(3):563–565. doi:10.1007/s00417-020-05053-4
19. Wang R, Long T, Gu X, Ma T. Changes in angle kappa and angle alpha before and after cataract surgery. J Cataract Refract Surg. 2020;46(3):365–371. doi:10.1097/j.jcrs.0000000000000063
20. Qin M, Ji M, Zhou T, et al. Influence of angle alpha on visual quality after implantation of extended depth of focus intraocular lenses. BMC Ophthalmol. 2022;22(1):82. doi:10.1186/s12886-022-02302-4
21. Cervantes-Coste G, Tapia A, Corredor-Ortega C, et al. The influence of angle alpha, angle kappa, and optical aberrations on visual outcomes after the implantation of a high-addition trifocal IOL. J Clin Med. 2022;11(3):896. doi:10.3390/jcm11030896
22. Moshirfar M, Hoggan RN, Muthappan V. Angle Kappa and its importance in refractive surgery. Oman J Ophthalmol. 2013;6(3):151–158. doi:10.4103/0974-620X.122268
23. Garcia-Tomas B, Marin-Sanchez JM, Garcia-Elskamp C, Alcon-Ruiz E, Montesinos-Lopez L, Martinez-Lozano B. Clinical outcomes of a monofocal, optimised, aspheric, hydrophobic acrylic intraocular lens implant. Clin Ophthalmol. 2023;17:3215–3224. doi:10.2147/OPTH.S434378
24. Hernandez-Martinez A, Diaz-Del-Rio MA, Ruiz-Santos M, Ruiz-Mesa R, Tana-Rivero P. Refractive and visual outcomes of a monofocal non-constant aberration aspheric intraocular lens. Clin Ophthalmol. 2022;16:2521–2530. doi:10.2147/OPTH.S373587
25. Altmann GE, Nichamin LD, Lane SS, Pepose JS. Optical performance of 3 intraocular lens designs in the presence of decentration. J Cataract Refract Surg. 2005;31(3):574–585. doi:10.1016/j.jcrs.2004.09.024
26. Kim MJ, Yoo YS, Joo CK, Yoon G. Evaluation of optical performance of 4 aspheric toric intraocular lenses using an optical bench system: influence of pupil size, decentration, and rotation. J Cataract Refract Surg. 2015;41(10):2274–2282. doi:10.1016/j.jcrs.2015.10.059
27. Ashena Z, Maqsood S, Ahmed SN, Nanavaty MA. Effect of intraocular lens tilt and decentration on visual acuity, dysphotopsia and wavefront aberrations. Vision. 2020;4(3). doi:10.3390/vision4030041
28. Tandogan T, Son HS, Choi CY, Knorz MC, Auffarth GU, Khoramnia R. Laboratory evaluation of the influence of decentration and pupil size on the optical performance of a monofocal, bifocal, and trifocal intraocular lens. J Refract Surg. 2017;33(12):808–812. doi:10.3928/1081597X-20171004-02
29. Pan RL, Tan QQ, Liao X, et al. Effect of decentration and tilt on the in vitro optical quality of monofocal and trifocal intraocular lenses. Graefes Arch Clin Exp Ophthalmol. 2024;262(10):3229–3242. doi:10.1007/s00417-024-06490-1
30. Holladay JT, Simpson MJ. Negative dysphotopsia: causes and rationale for prevention and treatment. J Cataract Refract Surg. 2017;43(2):263–275. doi:10.1016/j.jcrs.2016.11.049
31. Qi Y, Lin J, Zhao G, Wang Q, Li C, Hu L. Role of angla kappa in visual quality in patients with a trifocal diffractive intraocular lens. J Cataract Refract Surg. 2018;44(8):949–954. doi:10.1016/j.jcrs.2018.05.026
32. Zhang L, Schickardt S, Auffarth GU. An experimental laboratory study using the Miyake-apple posterior view technique to investigate the dynamics between capsular bags and different IOL models. J Refract Surg. 2022;38(10):654–660. doi:10.3928/1081597X-20220825-01
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.