Back to Journals » Clinical Ophthalmology » Volume 10
Visual acuity and patient satisfaction at varied distances and lighting conditions after implantation of an aspheric diffractive multifocal one-piece intraocular lens
Authors Chang D ![]()
Received 11 March 2016
Accepted for publication 23 June 2016
Published 3 August 2016 Volume 2016:10 Pages 1471—1477
DOI https://doi.org/10.2147/OPTH.S108298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Daniel H Chang
Empire Eye and Laser Center, Bakersfield, CA, USA
Purpose: The aim of the study is to evaluate the visual acuity and patient satisfaction at varied distances under photopic and mesopic lighting conditions in patients bilaterally implanted with aspheric diffractive multifocal one-piece intraocular lenses.
Methods: In this retrospective–prospective study, 16 patients with a mean age of 66.2±9.2 years (range: 50–81 years) who had undergone bilateral phacoemulsification surgery with implantation of a Tecnis multifocal one-piece intraocular lens (ZMB00) were evaluated. Monocular and binocular uncorrected and distance-corrected visual acuities were measured at distance (20 ft), intermediate (70–80 cm), and near (35–40 cm) under photopic (85 cd/m2) and mesopic (3 cd/m2) lighting conditions and were compared using the paired t-test. All patients also completed a subjective questionnaire.
Results: At a mean follow-up of 9.5±3.9 months, distance, near, and intermediate visual acuity improved significantly from preoperative acuity. Under photopic and mesopic conditions, 93.8% and 62.5% of patients, respectively, had binocular uncorrected intermediate visual acuity of 20/40 or better, and 62.5% and 31.3% of patients had binocular uncorrected near visual acuity of 20/20 or better. All patients were satisfied with their overall vision without using glasses and/or contact lenses when compared with before surgery. A total of 87.5% of patients reported no glare and 68.8% of patients reported no halos around lights at night.
Conclusion: Tecnis multifocal one-piece intraocular lenses provide good distance, intermediate, and near visual acuity under photopic as well as mesopic lighting conditions. High levels of spectacle independence with low levels of photic phenomenon were achieved, resulting in excellent patient satisfaction.
Keywords: Tecnis multifocal one-piece IOL, photopic visual acuity, mesopic visual acuity, intermediate visual acuity, near visual acuity
Introduction
Surgical goals and patient expectations of cataract surgery have evolved considerably over the past decade. Many patients now desire spectacle independence not only for distance but also for near and intermediate vision. Multifocal intraocular lenses (IOLs)1 provide spectacle independence by producing two or more focal points for distance, intermediate, and near vision.2–4 However, multifocality can result in reduced image contrast and unwanted photic phenomenon in the form of halos and glare.1,3
Diffractive multifocal IOLs provide better uncorrected near visual acuity, contrast sensitivity, and reading performance with less photic phenomenon than refractive multifocal IOLs,5,6 but they have still been associated with some reduction in visual quality.7 Material and design developments have contributed to improved optics. For example, the correction of spherical aberration8,9 with aspheric diffractive multifocal IOLs has been shown to improve visual quality and outcomes.2,10,11 Additionally, materials with low chromatic dispersion and a high Abbe number can reduce chromatic aberration and improve contrast sensitivity.12
The Tecnis Multifocal IOL is an aspheric diffractive multifocal IOL that comes in either silicone (three-piece [ZM900]) or a low-dispersion high Abbe number (55) hydrophobic acrylic (one-piece [ZMB00] and three-piece [ZMA00]).12 A full diffractive surface with steps of uniform height is present over the posterior surface of the optic, providing a +4.0 D near and with equal distribution of light to distance and near regardless of pupil size,13 helping to provide good functional vision under varied lighting conditions.14
The Tecnis Multifocal IOL has been demonstrated to yield high levels of spectacle independence, low residual refractive error, and good distance and near visual acuity, resulting in high levels of patient satisfaction.2,4,15 However, none of the published papers report visual acuity at intermediate with this lens. This study was designed to evaluate monocular as well as binocular visual acuity at distance, intermediate, and near under photopic and mesopic lighting conditions in patients bilaterally implanted with this aspheric diffractive multifocal one-piece IOL. Patient satisfaction for a variety of daily activities was also examined.
Methods
Sixteen patients (13 females and three males) with a mean age of 66.2±9.2 years (range: 50–81 years) who had previously undergone bilateral phacoemulsification surgery with implantation of the Tecnis Multifocal one-piece IOL (ZMB00; Abbott Medical Optics, Inc., Santa Ana, CA, USA) at Empire Eye and Laser Center, Bakersfield, CA, USA, between June 2010 and June 2011 were examined prospectively for visual acuity assessment under different lighting conditions and were asked to report satisfaction based on a subjective questionnaire. IOL power calculations were targeted for emmetropia. Careful centration was done in all surgeries and manual limbal relaxing incisions were performed in eyes with astigmatism ≥0.75 D. Eyes with significant ocular pathology, previous refractive surgery, or intraoperative adverse events were excluded. The study was approved by the Western Institutional Review Board, Olympia, WA, and written informed consent was obtained from all patients prior to participation.
All patients were evaluated prospectively at least 3 months following surgery on the second eye. At the single study visit, subjective manifest refraction was conducted and visual acuities were recorded. Monocular and binocular uncorrected and distance-corrected visual acuities were measured using the Good-Lite ESV1500 self-calibrated illuminated cabinet for distance (20 ft/6 m), intermediate (28–32 in/70–80 cm), and near (14–16 in/35–40 cm) under photopic (85 cd/m2) and mesopic (3 cd/m2) lighting conditions. All patients also completed a subjective questionnaire.
Statistical analysis of data
Statistical analysis of the data was carried out using SPSS software (V 17.0; SPSS Inc., Chicago, IL, USA). Visual acuity data were converted into the logMAR scale for statistical analysis. Variables were presented as mean ± standard deviation and cumulative percentages of eyes with different levels of visual acuity. Visual acuity measurements performed under photopic and mesopic light conditions were assessed for normality using quantile–quantile plot and then compared using the paired t-test. Statistical significance was defined as a P-value of <0.05.
Results
Visual outcomes
Patients were examined at a mean follow-up of 9.4±3.8 months (range: 4.7–16.2 months). The mean residual manifest refraction spherical equivalent was 0.004±0.289 D. Mean values and cumulative percentages of photopic uncorrected distance visual acuity and corrected distance visual acuity, measured binocularly and monocularly, are presented in Figure 1A and B and reveal better visual outcomes under photopic conditions. Likewise, the binocular and monocular intermediate (Figure 2A and B) and near (Figure 3A and B) visual acuities were observed to be significantly better under photopic conditions than mesopic.
 | Figure 1 Mean and cumulative percentages for distance visual acuity. |
 | Figure 2 Mean and cumulative percentages for intermediate visual acuity. |
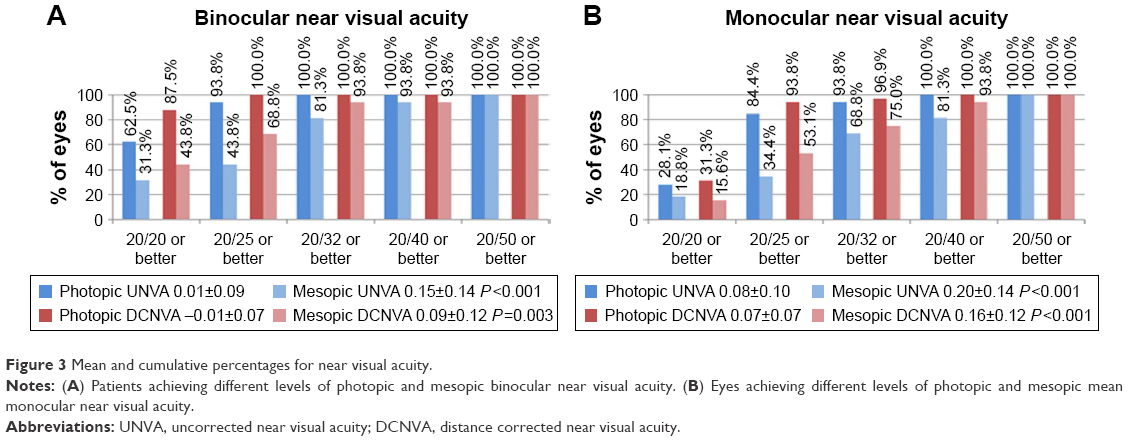 | Figure 3 Mean and cumulative percentages for near visual acuity. |
Patient-reported outcomes
All patients were overall “satisfied” (12.5%) or “very satisfied” (87.5%) with their postoperative vision without using glasses or contact lenses (Figure 4). Nearly all patients (93.8%) reported that they “never” or “hardly ever” wore glasses (Figure 5). Additionally, all patients reported that it was “much more” or “more” convenient to see without glasses while performing normal daily activities when compared with before surgery. While all patients reported that it was “very easy” or “easy” to see far away without glasses (Figure 6), 6.3% reported “difficulty” in reading small print in dim light without glasses, 6.3% reported “difficulty” in seeing at arm’s length without glasses, and 12.5% reported “difficulty” in driving at night without glasses. Overall, 75% of patients reported that the distance at which it was comfortable to read was “perfect,” whereas 25% of patients reported that the distance was “a little too close” (Figure 7). Furthermore, 87.5% of patients did not notice any fluctuations in their vision; the other 12.5% of patients said that they noticed fluctuations in vision only occasionally when reading small print in dim light or driving at night.
 | Figure 4 Histogram demonstrating percentage of patients satisfied with their vision without using glasses and/or contact lenses (over the last month) when compared with before surgery (in response to a directed questionnaire). |
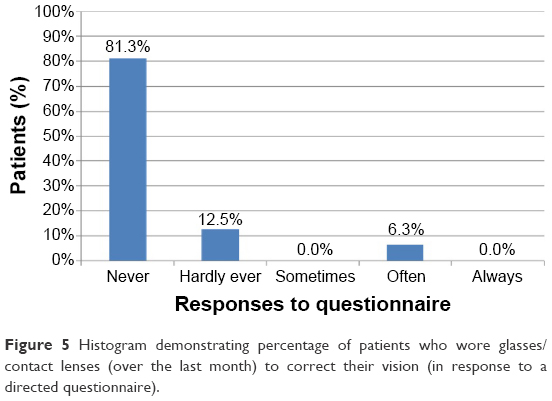 | Figure 5 Histogram demonstrating percentage of patients who wore glasses/contact lenses (over the last month) to correct their vision (in response to a directed questionnaire). |
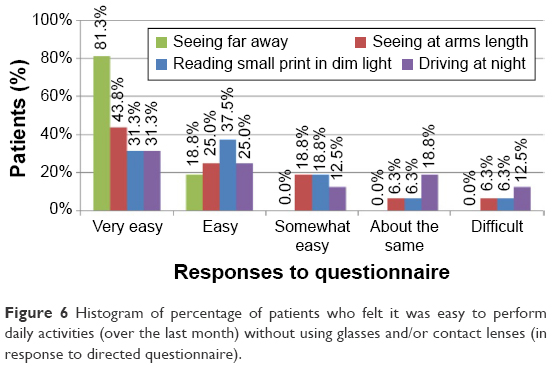 | Figure 6 Histogram of percentage of patients who felt it was easy to perform daily activities (over the last month) without using glasses and/or contact lenses (in response to directed questionnaire). |
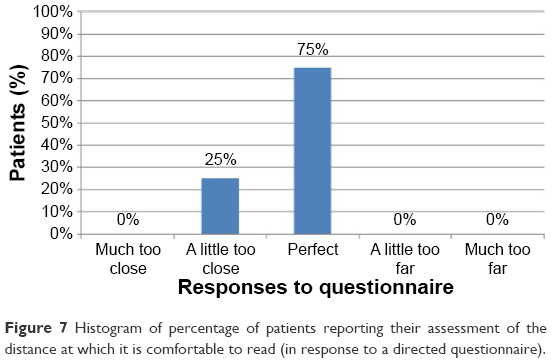 | Figure 7 Histogram of percentage of patients reporting their assessment of the distance at which it is comfortable to read (in response to a directed questionnaire). |
With respect to photic symptoms, 87.5% of patients reported no glare at night; 6.3% reported “mildly bothersome” glare, and only 6.3% reported “very bothersome” glare (Figure 8). In addition, 68.8% of patients reported no halos around lights at night, 18.8% of patients reported halos to be “present but not bothersome” or “mildly bothersome,” and 12.5% had “moderately bothersome” or “very bothersome” halos (Figure 8). Only 6.3% of patients experienced double images/ghosting, which was reported to be “present but not bothersome.” A total of 93.8% patients stated that they would “definitely” or “most likely” choose to have the same lens implanted again (Figure 9).
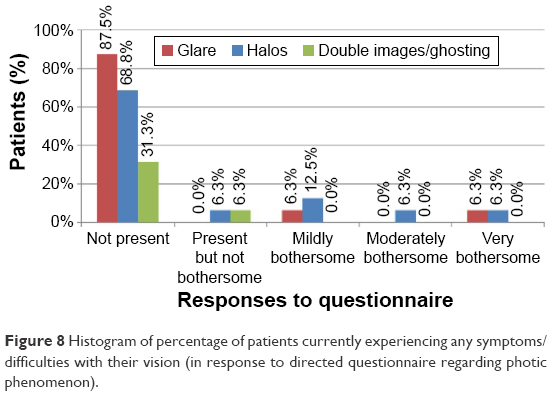 | Figure 8 Histogram of percentage of patients currently experiencing any symptoms/difficulties with their vision (in response to directed questionnaire regarding photic phenomenon). |
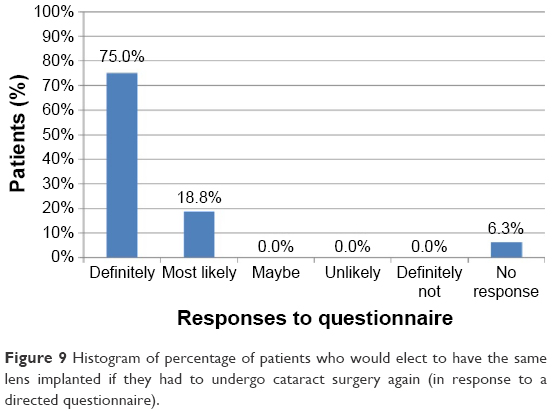 | Figure 9 Histogram of percentage of patients who would elect to have the same lens implanted if they had to undergo cataract surgery again (in response to a directed questionnaire). |
Discussion
Patients seeking multifocal IOL implantation have high expectations for their vision at all distances and under all lighting conditions. It is, therefore, important to assess the quality of vision at distant, intermediate, and near under different illumination settings monocularly as well as binocularly. This study evaluated visual outcomes of patients bilaterally implanted with the Tecnis Multifocal one-piece IOL (model ZMB00) and found excellent distance, intermediate, and near visual acuity outcomes yielding a high degree of spectacle independence and a low level of photic phenomena, resulting in high patient satisfaction. In general, all patients were satisfied with their vision without using glasses for seeing far away and most of the patients felt comfortable in performing activities such as reading small print in dim light, seeing at arm’s length, and driving at night.
The visual acuity results of this study are comparable to or better than those reported in previous publications with Tecnis Multifocal IOLs (ZMB00, ZMA00, and ZM900) and other presbyopia-correcting IOLs.1,2,15–23 Since most studies do not state whether visual acuity was measured under photopic or mesopic light conditions, visual acuities are assumed to be photopic unless otherwise specified. Mean binocular distance visual acuities (Figure 1A) are either comparable to or better than those reported in previous studies with three-piece silicone (ZM900), one-piece acrylic (ZMB00), and three-piece acrylic (ZMA00) versions of the Tecnis Multifocal IOL.2,4,16,19,22 Likewise, mean monocular distance visual acuities (Figure 1B) are comparable to or better than those reported by previous authors.1,15,17–23 A comparison of cumulative percentages of patients achieving visual acuity of 20/20 revealed that 87.5% of patients had uncorrected distance visual acuity of 20/20 or better in this study (Figure 1A), compared with the corresponding values of 30% and 57.9% reported by Ngo et al24 and Packer et al,3 respectively, in patients with the three-piece silicone (ZM900) lens. The corresponding value for corrected distance visual acuity (20/20 or better) was 100% in this study, compared with the studies by Ngo et al24 (43.3%) and Packer et al3 (~70%) reported previously. Furthermore, comparison with other models of refractive and diffractive multifocal IOLs also revealed that the binocular distance visual acuity found in the current study is either equivalent or better.25–28 The development of posterior capsular opacification may degrade optical quality with a diffractive IOL and might be expected to disproportionately affect visual acuity with the study IOL compared with other lenses. However, posterior capsular opacification was not found to be significant in any eye in the current study.
The mean binocular photopic and mesopic near visual acuities in the current study are better than those reported in previous paper evaluating the one-piece acrylic Tecnis Multifocal IOL (ZMB00).4 Similarly, in comparison to the three-piece acrylic (ZMA00; Abbe number 55) and the three-piece silicone (ZM900) versions (Abbe number 42), the near visual acuities reported here are either comparable or better.3,16,19,22,23 The near visual outcomes in this study are also similar to or better than those reported for other diffractive and refractive multifocal IOLs.26–30
The improvement in distance and near visual outcomes found in the current study may be due to a number of factors. A change in lens material from silicone (ZM900) to a particular hydrophobic acrylic (ZMA00 and ZMB00) with significantly less intrinsic chromatic aberration and chromatic dispersion (higher Abbe number) may be a contributor.12 Additionally, the rings on the one-piece acrylic version (ZMB00) provide an enhanced diffractive profile that is designed to improve night vision symptoms. Differences in surgical technique, which included the correction of astigmatism in this study, as well as careful centration,31 may also have contributed. Finally, variability of testing conditions, particularly when comparing a multicenter study with a single center study, could account for some differences as well.
Along with distance and near visual acuity, this study examined intermediate visual acuity under both photopic and mesopic light conditions and found comparable or better results than in previous studies with the Tecnis Multifocal IOLs and other diffractive and refractive multifocal IOLs.16,22,27,30
Comparison of mean visual acuity data revealed that distance visual acuity outcomes were the best, followed by near and intermediate. While the distance visual acuities were ~0.5–1 line better than the near visual acuities, the near visual acuities were 1–1.5 lines better than the intermediate visual acuities. Furthermore, photopic visual acuities were 1–2 lines better than mesopic acuities at any distance. This may be attributed in part to changes in pupil size. Finally, due to expected gains from binocular summation, binocular visual acuities were 0.5–1 line better than the monocular visual acuity.32
For evaluation of visual performance and patient satisfaction following presbyopic IOL implantation, visual acuity data alone are not sufficient. Patient satisfaction, spectacle independence, ease of performing vision-dependent tasks, and problems with photic phenomena can all be further evaluated with patient-reported outcome (PRO) questionnaires. As more specific functional visual outcome analyses are needed, PRO devices are becoming an increasingly important tool in these assessments.
With respect to spectacle independence, the present study reports 81.3% of patients “never” wore glasses after surgery on a 5-point scale. In the US Food and Drug Administration (FDA) premarket approval study with the three-piece silicone IOL (ZM900), 86.2% of patients “never” wore glasses (one year) after surgery on a 3-point scale.25 Interestingly, if the data from the present study were pooled into a 3-point scale, 93.8% of patients would fall into a “never” or “hardly ever” wear glasses category. Either way, this study compares favorably to other studies with diffractive or refractive multifocal IOLs, which have reported spectacle independence for distance in the 80%–100% range1,3,4,17,19,21,25 and for near in the 12%–98% range.1,3,17,19,21,25
With respect to photic phenomenon, in the present study, one patient (6.3%) reported “very bothersome” glare and two patients (12.5%) had “moderately bothersome” or “very bothersome” halos around lights at night (Figure 8). Corresponding values for “mildly bothersome” glare and halos were 6.25% and 12.5%, respectively. In two other studies with the one-piece acrylic ZMB00, Bautista et al15 reported combined photic effects as moderate in 1.4% and mild in 10% of subjects, and Schmickler et al4 reported glare to be present in 8% of patients at night and in 4% during day. Schmickler et al4 did not report corresponding information on halos. When compared with the FDA premarket approval study data with the three-piece silicone (ZM900) IOL, severe night glare and halos were reported to be as low as 2.4% and 5.4%, respectively, in nondirected responses and as high as 16.6% and 18.3%, respectively, in a prompted-choice questionnaire.25 As such, it seems that the current study demonstrates photic phenomenon comparable to previous reports.4,15,25
Differences in patient-reported outcomes for photic phenomena may in part be due to differences in the method of questioning as well as the scoring strategy. For example, Bautista et al15 used a 4-point scale to assess glare or halos (none, mild, moderate, and severe), this study used a 5-point scale (not present, present but not bothersome, mildly bothersome, moderately bothersome, and very bothersome) and the FDA study used as high as a 7-point scale. Other variables in PRO construction, such as differences in wording and directed versus nondirected questioning, can affect the results. Thus, it would be beneficial to have validated PRO questionnaires for future studies of presbyopia-correcting IOLs.
In spite of the variation in the scope and content of different questions for the same variable in the PRO surveys, the current study compares favorably with the outcomes reported in previous studies. However, the sex difference and small sample size may have affected the PRO. Future studies with larger sample size and equivalent distribution of males and females may validate the current study results. Nevertheless, the current study results are indicative of good patient satisfaction after Tecnis Multifocal IOL implantation.
Conclusion
Bilateral implantation of Tecnis Multifocal one-piece IOLs provided good distance, intermediate, and near visual acuity under photopic as well as mesopic lighting conditions. High levels of spectacle independence with low levels of photic phenomenon were achieved, resulting in excellent patient satisfaction.
Acknowledgments
Jan Beiting (Wordsmith Consulting, Cary, North Carolina, USA) and Raman Bedi (IrisARC – Analytics, Research & Consulting, Chandigarh, India) provided research, statistics, and editorial assistance in the preparation of this manuscript. Abbott Medical Optics Inc., Santa Ana, CA, USA, provided an unrestricted research grant.
Disclosure
The author is a paid consultant to AMO. The author reports no other conflicts of interest in this work.
References
Akaishi L, Vaz R, Vilella G, Garcez RC, Tzelikis PF. Visual performance of Tecnis ZM900 diffractive multifocal IOL after 2500 implants: a 3-year followup. J Ophthalmol. 2010;2010:ii:717591. | ||
Friedrich R. Intraocular lens multifocality combined with the compensation for corneal spherical aberration: a new concept of presbyopia-correcting intraocular lens. Case Rep Ophthalmol. 2012;3(3):375–383. | ||
Packer M, Chu YR, Waltz KL, et al. Evaluation of the aspheric tecnis multifocal intraocular lens: one-year results from the first cohort of the Food and Drug Administration clinical trial. Am J Ophthalmol. 2010;149(4):577–584.e571. | ||
Schmickler S, Bautista CP, Goes F, Shah S, Wolffsohn JS. Clinical evaluation of a multifocal aspheric diffractive intraocular lens. Br J Ophthalmol. 2013;97(12):1560–1564. | ||
Cillino S, Casuccio A, Di Pace F, et al. One-year outcomes with new-generation multifocal intraocular lenses. Ophthalmology. 2008;115(9):1508–1516. | ||
Hayashi K, Manabe S, Hayashi H. Visual acuity from far to near and contrast sensitivity in eyes with a diffractive multifocal intraocular lens with a low addition power. J Cataract Refract Surg. 2009;35(12):2070–2076. | ||
Vingolo EM, Grenga P, Iacobelli L, Grenga R. Visual acuity and contrast sensitivity: AcrySof ReSTOR apodized diffractive versus AcrySof SA60AT monofocal intraocular lenses. J Cataract Refract Surg. 2007;33(7):1244–1247. | ||
Denoyer A, Le Lez ML, Majzoub S, Pisella PJ. Quality of vision after cataract surgery after Tecnis Z9000 intraocular lens implantation: effect of contrast sensitivity and wavefront aberration improvements on the quality of daily vision. J Cataract Refract Surg. 2007;33(2):210–216. | ||
Packer M, Fine IH, Hoffman RS, Piers PA. Improved functional vision with a modified prolate intraocular lens. J Cataract Refract Surg. 2004;30(5):986–992. | ||
Bellucci R, Morselli S. Optimizing higher-order aberrations with intraocular lens technology. Curr Opin Ophthalmol. 2007;18(1):67–73. | ||
Montes-Mico R, Ferrer-Blasco T, Cervino A. Analysis of the possible benefits of aspheric intraocular lenses: review of the literature. J Cataract Refract Surg. 2009;35(1):172–181. | ||
Zhao H, Mainster MA. The effect of chromatic dispersion on pseudophakic optical performance. Br J Ophthalmol. 2007;91(9):1225–1229. | ||
Lichtinger A, Rootman DS. Intraocular lenses for presbyopia correction: past, present, and future. Curr Opin Ophthalmol. 2012;23(1):40–46. | ||
Gooi P, Ahmed IK. Review of presbyopic IOLs: multifocal and accommodating IOLs. Int Ophthalmol Clin. 2012;52(2):41–50. | ||
Bautista CP, Gonzalez DC, Gomez AC. Evolution of visual performance in 70 eyes implanted with the Tecnis((R)) ZMB00 multifocal intraocular lens. Clin Ophthalmol. 2012;6:403–407. | ||
Cillino G, Casuccio A, Pasti M, Bono V, Mencucci R, Cillino S. Working-age cataract patients: visual results, reading performance, and quality of life with three diffractive multifocal intraocular lenses. Ophthalmology. 2014;121(1):34–44. | ||
Guo X, Sun Y, Zhang B, Zheng D. Medium-term visual outcomes of apodized diffractive multifocal intraocular lens with +3.00 d addition power. J Ophthalmol. 2014;2014:247829. | ||
Hutz WW, Jackel R, Hoffman PC. Comparison of visual performance of silicone and acrylic multifocal IOLs utilizing the same diffractive design. Acta Ophthalmol. 2012;90(6):530–533. | ||
Mesci C, Erbil HH, Olgun A, Yaylali SA. Visual performances with monofocal, accommodating, and multifocal intraocular lenses in patients with unilateral cataract. Am J Ophthalmol. 2010;150(5):609–618. | ||
Rasp M, Bachernegg A, Seyeddain O, et al. Bilateral reading performance of 4 multifocal intraocular lens models and a monofocal intraocular lens under bright lighting conditions. J Cataract Refract Surg. 2012;38(11):1950–1961. | ||
Yamauchi T, Tabuchi H, Takase K, Ohsugi H, Ohara Z, Kiuchi Y. Comparison of visual performance of multifocal intraocular lenses with same material monofocal intraocular lenses. PLoS One. 2013;8(6):e68236. | ||
Ye PP, Li X, Yao K. Visual outcome and optical quality after bilateral implantation of aspheric diffractive multifocal, aspheric monofocal and spherical monofocal intraocular lenses: a prospective comparison. Int J Ophthalmol. 2013;6(3):300–306. | ||
Yoshino M, Bissen-Miyajima H, Oki S, Minami K, Nakamura K. Two-year follow-up after implantation of diffractive aspheric silicone multifocal intraocular lenses. Acta Ophthalmol. 2011;89(7):617–621. | ||
Ngo C, Singh M, Sng C, Loon SC, Chan YH, Thean L. Visual acuity outcomes with SA60D3, SN60D3, and ZM900 multifocal IOL implantation after phacoemulsification. J Refract Surg. 2010;26(3):177–182. | ||
TECNIS® ZMB00 multifocal IOL [package insert]. Santa Ana, CA: Abbott Medical Optics Inc.; 2012. | ||
Lane SS, Javitt JC, Nethery DA, Waycaster C. Improvements in patient-reported outcomes and visual acuity after bilateral implantation of multifocal intraocular lenses with +3.0 diopter addition: multicenter clinical trial. J Cataract Refract Surg. 2010;36(11):1887–1896. | ||
Munoz G, Albarran-Diego C, Ferrer-Blasco T, Sakla HF, Garcia-Lazaro S. Visual function after bilateral implantation of a new zonal refractive aspheric multifocal intraocular lens. J Cataract Refract Surg. 2011;37(11):2043–2052. | ||
Tsaousis KT, Plainis S, Dimitrakos SA, Tsinopoulos IT. Binocularity enhances visual acuity of eyes implanted with multifocal intraocular lenses. J Refract Surg. 2013;29(4):246–250. | ||
Alfonso JF, Fernandez-Vega L, Puchades C, Montes-Mico R. Intermediate visual function with different multifocal intraocular lens models. J Cataract Refract Surg. 2010;36(5):733–739. | ||
de Vries NE, Webers CA, Montes-Mico R, Ferrer-Blasco T, Nuijts RM. Visual outcomes after cataract surgery with implantation of a +3.00 D or +4.00 D aspheric diffractive multifocal intraocular lens: comparative study. J Cataract Refract Surg. 2010;36(8):1316–1322. | ||
Chang DH, Waring GO. The subject-fixated coaxially sighted corneal light reflex: a clinical marker for centration of refractive treatments and devices. Am J Ophthalmol. 2014;158(5):863–874. | ||
Rabin J. Two eyes are better than one: binocular enhancement in the contrast domain. Ophthalmic Physiol Opt. 1995;15(1):45–48. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.