Back to Journals » Clinical Ophthalmology » Volume 14
Visian® ICLV4c™ and Artiflex®: Comparative Analysis with the HD Analyser™ and Integration with Subjective Performance and Anatomical Parameters
Authors Baptista PM ![]() , Monteiro S
, Monteiro S ![]() , Abreu AC
, Abreu AC ![]() , Poças J, José D
, Poças J, José D ![]() , Lume M
, Lume M ![]() , Pinto MDC
, Pinto MDC ![]()
Received 19 November 2020
Accepted for publication 8 December 2020
Published 30 December 2020 Volume 2020:14 Pages 4541—4549
DOI https://doi.org/10.2147/OPTH.S290611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pedro Manuel Baptista,1,2 Sílvia Monteiro,1 Ana Carolina Abreu,1 João Poças,1 Diana José,1 Miguel Lume,1 Maria do Céu Pinto1
1Ophthalmology Department, Centro Hospitalar Universitário do Porto, Porto, Portugal; 2Instituto de Ciências Biomédicas Abel Salazar, Porto, Portugal
Correspondence: Pedro Manuel Baptista
Centro Hospitalar Universitário do Porto, Largo Prof. Abel Salazar, Porto 4099-001, Portugal
Tel +351 917868372
Email [email protected]
Purpose: To analyze and compare the mid-term objective and subjective performance of two phakic intraocular lenses (PIOLs) – Visian® ICL™ V4c and Artiflex® and to correlate those results with anatomical parameters.
Patients and Methods: Observational retrospective study including thirty patients (15 for each PIOL) randomly selected from those who underwent bilateral implantation of one of the PIOLs (60 eyes were analysed). Uncorrected and corrected distance visual acuities (UDVA and CDVA), anterior chamber structural parameters, and corneal endothelial cells density and morphology were evaluated. Quality of vision was assessed both subjectively with a questionnaire, and objectively using a double-pass technology optical quality analysis system.
Results: At the end of follow-up the Artiflex® group showed better UDVA (0.95± 0.11 vs 0.99± 0.05, p=0.027) and higher proportion of eyes reaching at least 20/20 (28/30 vs 18/30, p=0.005). Excellent and similar objective scatter index (1.79± 0.9 vs 2.14± 1.6, p=0.306) and modular transfer function cutoff frequency (26.91± 9.2 vs 26.51± 11.9, p=0.784) results were achieved in the HD Analyzer® and the questionnaire showed comparable high Satisfaction (55.7± 3.5 vs 54.3± 5.4, p=0.386) and low Dysphotopsia Scores (3.1± 1.8 vs 2.1± 2.2, p=0.213). The ICL group showed inferior anterior chamber volume (p< 0.001), and angle (p< 0.001) and superior pupillary diameter (p=0.007). Minimum follow-up was 24 months.
Conclusion: Both the Visian® ICLV4c™ and the Artiflex® showed excellent optical performance through the HD AnalyzerTM technology, translated in high patient satisfaction. Overall, both PIOLs showed similar safety, predictability, stability and effectiveness of for the reduction of high sphero-cylindrical refractive errors, despite better UDVA results with the Artiflex®.
Keywords: astigmatism, Artiflex®, dysphotopsia, glare, halos, HD AnalyzerTM, high myopia, phakic intraocular lens, spheric, toric, Visian® ICLV4c™
Plain Language Summary
Phakic intraocular lenses (PIOL) are options used since many years ago to decrease high sphero-cylindrical refractive errors. With the increasing prevalence of these errors and the evolving technology associated to these lenses, more patients can benefit from its implantation in the present and in the future. However, there are still some issues regarding the visual quality and long-term safety of these lenses. In fact, PIOL implantation is mostly performed on a demanding age group so the procedure should pursue perfection. However, it comprises an additional refractive surface, prone to be associated with visual quality complaints.
The analysis of the vision quantity and quality associated to PIOL implantation is classically in the dependency not only on refractive parameters but in retinal and optic nerve status and visual cortex potential, many times impaired in high myopic patients.
The present study aimed to make a comprehensive mid-term analysis of eyes implanted with perhaps the two most implanted PIOLs nowadays (Visian® ICLV4c™ and Artiflex®), including the true refractive performance with a novel light scattering measuring system (HD AnalyzerTM, Visiometrics), the anatomical status and patient-reported subjective outcomes.
Both PIOLs showed excellent optical performance, despite better UDVA results with the Artiflex®. Patient satisfaction was high with both lenses, despite some associated disphotopic complaints in relation with the pupillary diameter.
Introduction
Despite phakic intraocular lens (PIOL) implantation (iris-claw and posterior chamber) has been associated with good visual outcomes, there are still some issues regarding the visual quality and long-term safety of these lenses.1–3 Regarding most patients implanted being young and active, and the fact that many of them present retinal alterations or cortex limitations in the form of amblyopia, the evaluation and comparison of both refractive lens performance and the overall real quality of life achieved is imperative.
In recent years, contrast sensitivity (CS) testing has gained popularity, as it represents a more robust measure of visual quality; however, its assessment might be compromised even in the presence of normal visual acuity.4 The CS function is influenced by all eye structures, from the lacrimal tear film to the visual cortex, and it has been reported to increase after PIOL implantation.5,6 The double-pass imaging system (HD AnalyzerTM, Visiometrics®) is a novel technology capable of measuring the light scattering in the retina and the eye modulation transfer function, in various contrast conditions. In this way, the limitations of the subjective psychophysical measure of the CS function are overcome, making possible the assessment of true refractive performance of the eye without optic nerve and cortical compounds.7–9
Multiple studies have compared visual outcomes of the earlier Visian® ICL™ models and the anterior chamber iris-claw models of PIOL.10 There is only one study in the literature comparing visual outcomes, other than visual acuity, namely contrast sensitivity of the iris-fixed PIOL Artiflex® (Artiflex) and the new Visian® ICL™V4c model (ICL),11 and no studies addressing the light scattering in the eye or the real-life visual function have been found. Our study aims to describe and compare the mid-term objective and subjective performance of these two PIOL – ICLV4c and the Artiflex – and to correlate it with anatomical parameters.
Patients and Methods
Design
Observational cross-sectional study set in the Ophthalmology Department of a tertiary center – Centro Hospitalar e Universitário do Porto, Porto, Portugal. The study adhered to the tenets of the Declaration of Helsinki. Approval was obtained from the “Departamento de Ensino, Formação e Investigação” (DEFI), nr: 130-DEFI/132-CE. The informed consent from the patients was waived due to total anonymization and confidentiality of the data and the absence of detailed individual data.
Population
We selected 30 consecutive patients that underwent bilateral implantation of both spherical and toric ICLV4c (n=30 eyes) or Artiflex (n=30 eyes) in our department, with similar follow-up time (minimum 24 months).
The eyes included respected the PIOL implantation criteria followed in our department:
- Age between 21 and 45 years old;
- Refractive stability for more than 1 year;
- Pupillary diameter inferior to 6 mm;
- Corrected anterior chamber depth (from endothelium) superior to 3 mm (Artiflex) and 2.8 mm (ICL);
- Central endothelial cell density superior to 2500/mm2;
- Absence of corneal ectasia, previous refractive surgery, history of glaucoma, uveitis, significant retinal pathology or detachment and chronic systemic disease.
Data Gathering
Demographic data, medical history and the event of surgical complications were recorded.
Anterior segment structural parameters analyzed with Scheimpflug technology (OCULUS Pentacam®) were anterior chamber depth (ACD, mm), volume (ACV, mm3) and angle (ACA, º) and pupillary diameter (mm). The central endothelial cell density (ECD, cells/mm2) was evaluated by specular microscopy (TOMEY EM-3000®). The end of follow-up ACD value is the distance between the endothelium and lens body (ACD1).
The uncorrected distance (UDVA) and best-corrected distance visual acuities (CDVA) were measured using Snellen visual acuity chart. For the statistical analysis, the values were converted to the Logarithm of the minimum angle of resolution (LogMAR). The final representation was made both in Snellen and decimal notation for an intuitive analysis. The ratio between postoperative UDVA and preoperative CDVA was used as a representative way to report the procedure overall efficacy (Efficacy Index). Both the sphere, cylinder, spherical equivalent (SE) and the defocus equivalent (DEQ) of the subjective refraction before and after surgery were recorded.
Objective vision quality assessment was performed using the HD AnalyzerTM. The analyzed parameters were: the objective scatter index (OSI); the modulation transfer function cutoff frequency (MTF) and the predicted visual acuities (decimal) within the 100% contrast level (PVA), the 20% contrast level (PVA20) and the 9% contrast level (PVA9). Both OSI and MTF analysis were measured under an artificial machine-made 4mm pupil and the light conditions in the PVAs measurements were automatically generated by the device.
Subjective real-life vision quality was assessed applying a modification of the validated Cataract TyPE Spec Questionnaire (Attachment 1), which was divided in two steps. The first included 6 general satisfaction questions graded from 1 to 10 and measured in a 60-pointed score (Satisfaction Score); the second reports, in a scale from 0 to 3, the presence and degree of glare sensitivity, photopic and scotopic halos, with subsequent creation of a 9-pointed score (Dysphotopsia Score).
A subgroup comparative analysis was made stratifying all sample for the toricity of the PIOL implanted and reports of glare sensitivity or scotopic halos.
Statistical Analysis
Statistical analysis was performed with the SPSS, version 24.0 (SPSS, Chicago, IL®). Normality of the data was tested with the Shapiro–Wilk test. When parametric analysis could be applied, the Student’s t-test was used to compare the variables. When nonparametric tests were needed, the Wilcoxon rank-sum test was applied. Correlations were studied with Spearman rank correlation method. Comparison of categorical variables was studied by the Fisher’s exact test. Values are show as mean ± standard deviation unless otherwise specified. All p-values (p) were 2-sided, and p-values < 0.05 were considered significant.
Results
Baseline demographic, clinical and anatomical data from both the 15 patients (30 eyes) implanted with the Visian® ICLV4c™ and the 15 patients (30 eyes) implanted with the Artiflex® are shown in Table 1. Overall mean age was 36.4±5.6 years. The mean follow-up time was 39.6±10.4 months. Anatomically, the Artiflex group had significantly higher ACV (p<0.001) (Table 1). No other statistically significant baseline differences were found. All procedures were uneventful.
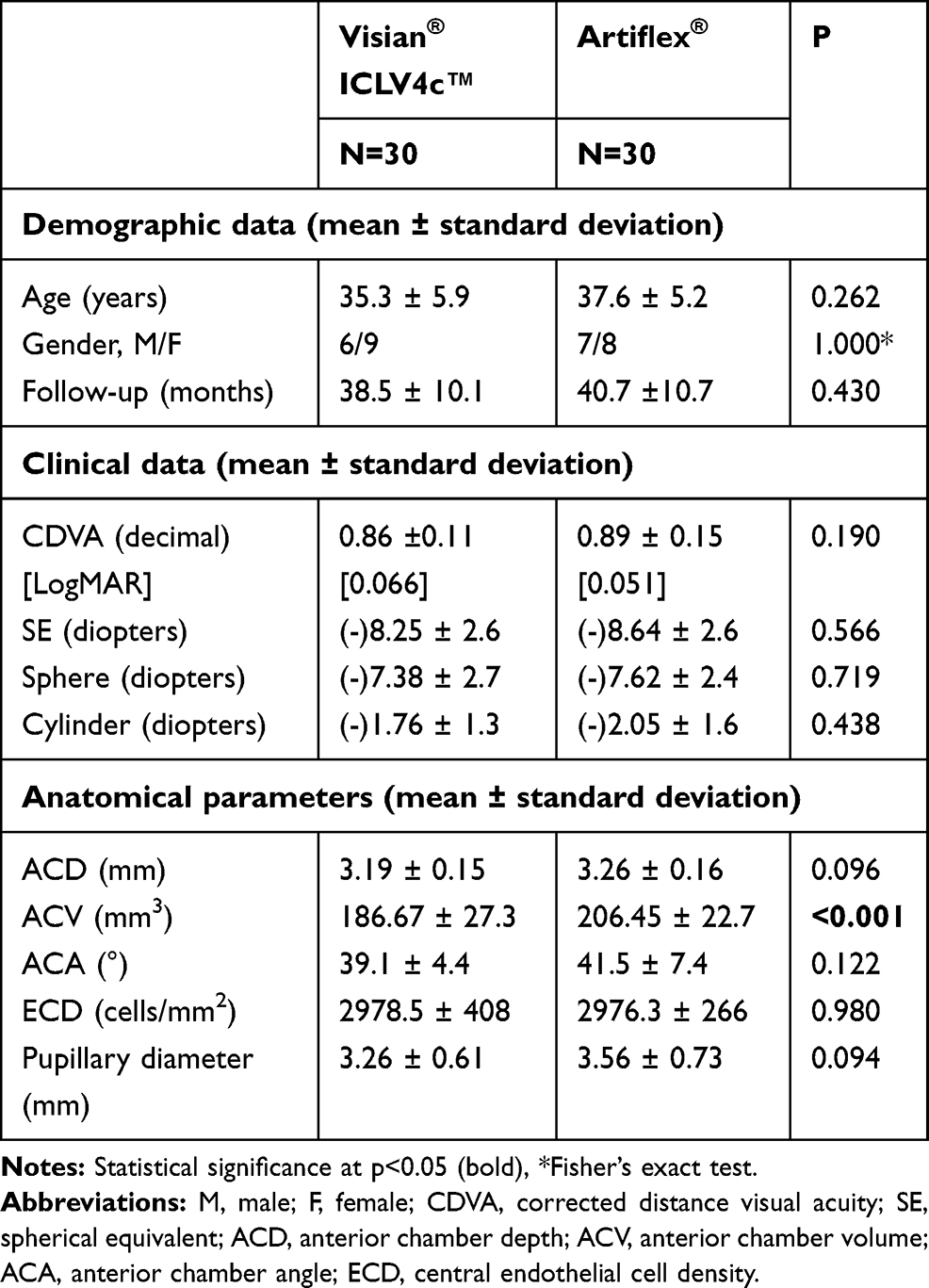 |
Table 1 Baseline Characteristics per PIOL |
Visual Acuity and Spherical Equivalent
Overall, the procedure provided a minimum of one Snellen line gain in 23/60 eyes (38%) and 1 eye (ICL group) lost 1 line between baseline CDVA and final UDVA, from 20/25 to 20/32 (Figure 1). Forty-six out of sixty eyes (77%) presented at least a 20/20 UDVA with 55 eyes (92%) within the SE plano target interval (−0.50 to +0.50) of subjective refraction (Figures 2 and 3). Mild improvement in visual acuity with optical correction was additionally observed in 7 eyes of the ICL group (mean SE −0.53D; mean DEQ 0.78) and in 4 eyes of the Artiflex group (mean SE −0.65D; mean DEQ 0.9), but less than one line in all.
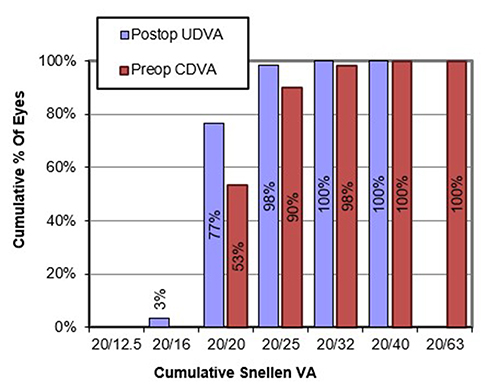 |
Figure 1 Visual acuities at baseline and at the end of follow-up (all eyes). |
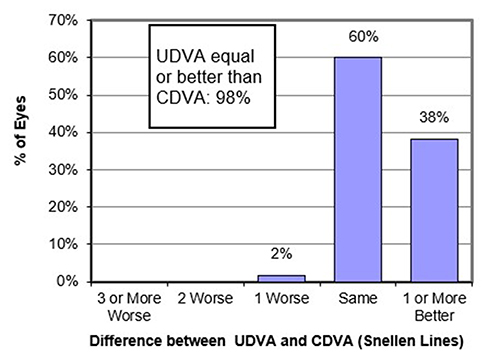 |
Figure 2 Visual acuity differences between baseline and the end of follow-up (all eyes). |
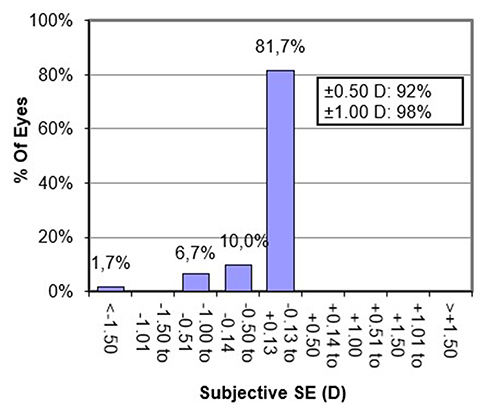 |
Figure 3 Subjective spherical equivalent at the end of follow-up (all eyes). |
Despite similar number of eyes reaching the plano target SE interval (≤0.5D SE) (28/30 vs 27/30, p=1.000) and a minimum of one Snellen line gain (12/30 vs 11/30, p=1.000), the Artiflex group showed better UDVA (0.95±0.11 vs 0.99±0.05, p=0.027) and higher proportion of eyes reaching at least 20/20 (28/30 vs 18/30, p=0.005) (Table 2).
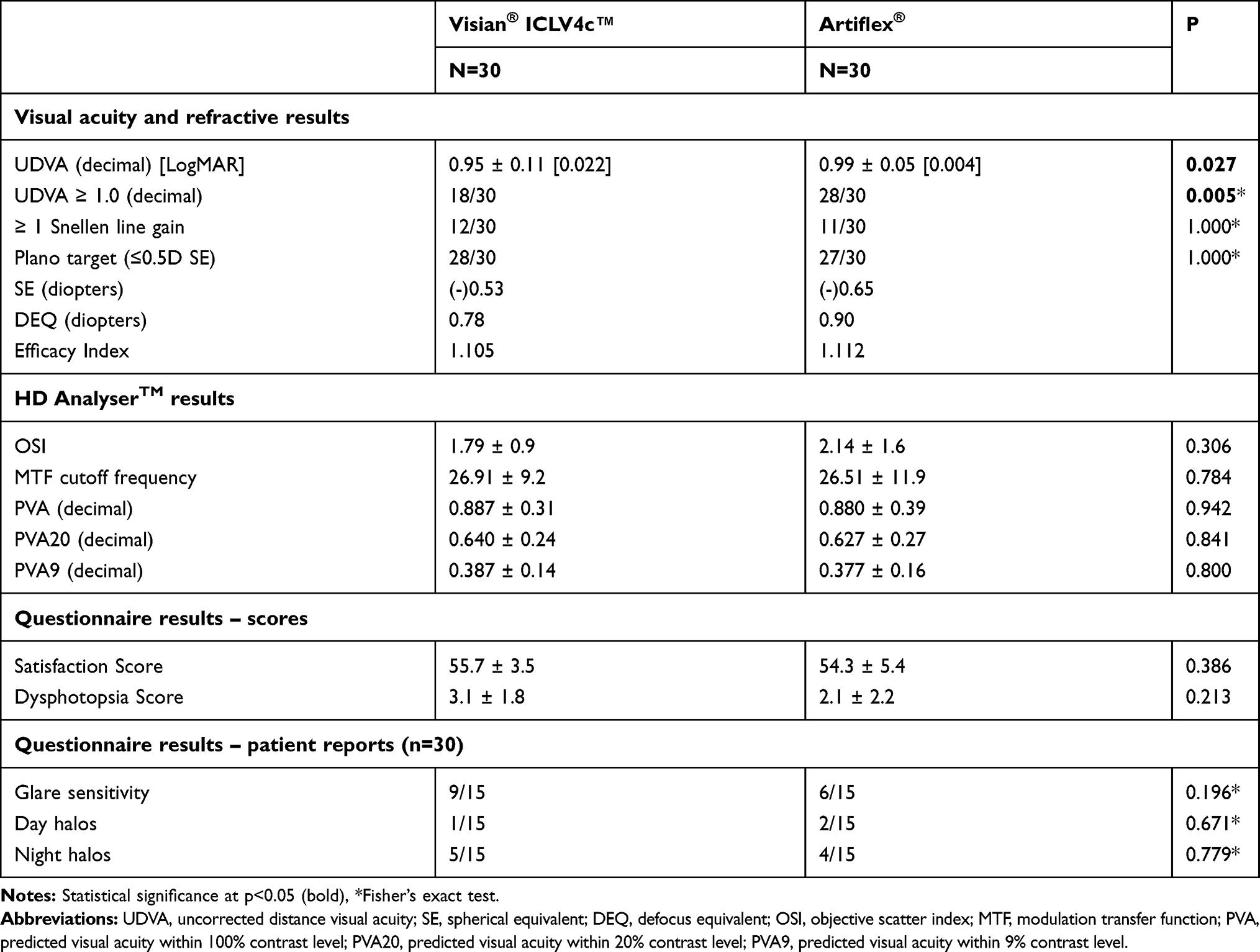 |
Table 2 End of Follow-Up Visual Acuity and Quality of Vision per PIOL |
Objective and Subjective Quality of Vision
The objective quality of vision assessment presented excellent results in both groups, without significant differences between groups (p>0.05) (Table 2). Concerning the contrast-associated variation in the PVAs, and starting from 100% level, an overall loss of 2.5 lines to 20% level and 5 lines to 9% level were found, with no differences between groups (p>0.05 in all) (Table 2).
Analyzing the real-life vision quality questionnaire, the average Satisfaction Score was high and similar in both groups (p=0.386) and the average Dysphotopsia Score was low and similar in both groups. There were no significant differences between both groups regarding each type of dysphotopsia report (p>0.05 in all) (Table 2).
Glasses independency was achieved in all patients from the ICL group and one patient in the Artiflex group needed glasses for distance vision.
Anterior Chamber Anatomical Parameters
Regarding anatomical results, normal range values at the end of follow-up in both groups were found (Table 3). The ICL group showed an inferior ACV (p<0.001), inferior ACA (p<0.001) and superior pupillary diameter (p=0.007) compared with the Artiflex group. The decrease from baseline in the ACD (p=0.008), ACA (p<0.001) and pupillary diameter (p<0.001) were more pronounced in the Artiflex group. The decrease in the ECD was similar in both groups (p=0.615).
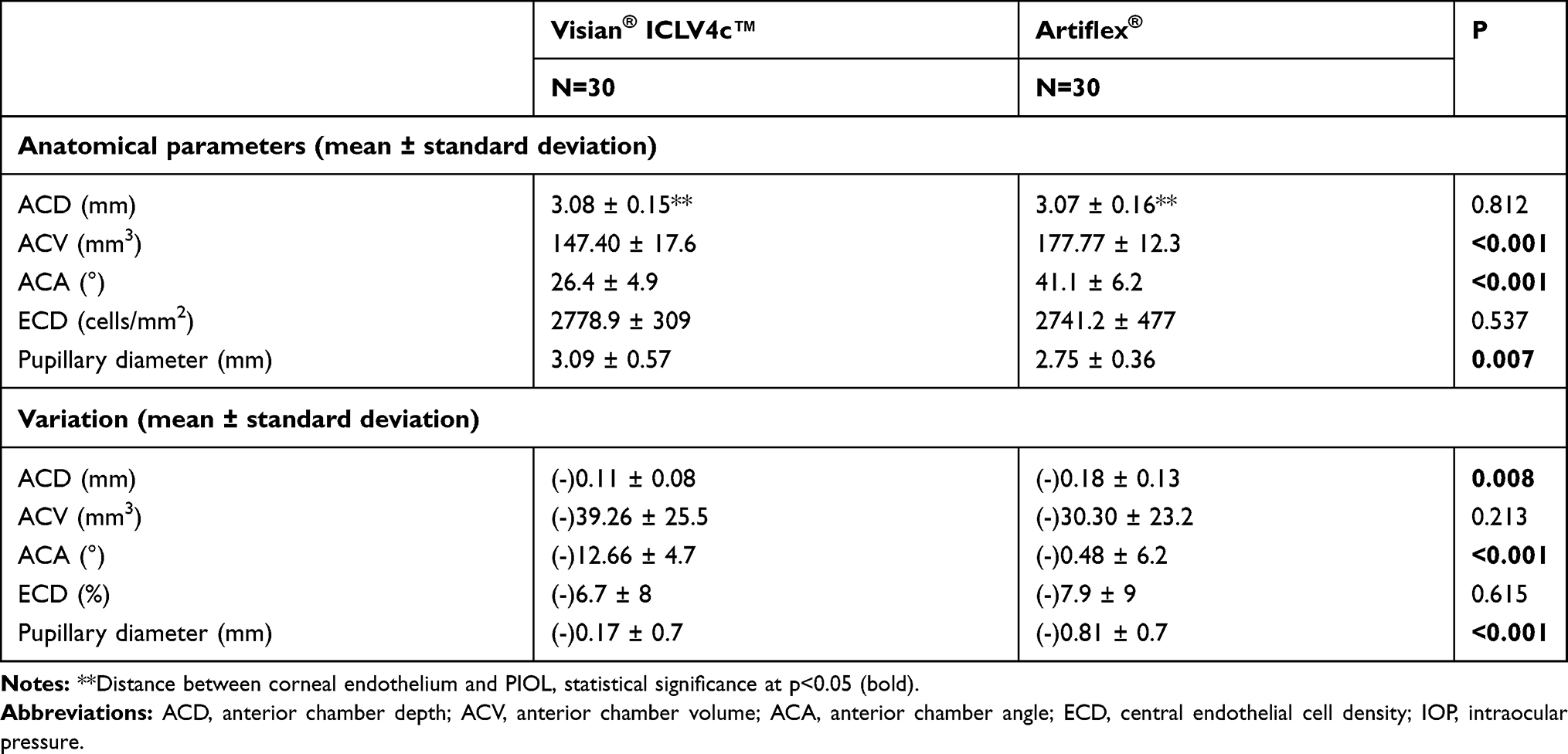 |
Table 3 End of Follow-Up Anatomical Parameters and Its Variation from Baseline per PIOL |
Subgroup Analysis
Toric PIOLs were implanted in 72.1% (n=44) of the eyes (25/30 in the ICL group and 19/30 in the Artiflex group), with overall mean baseline cylinder of 2.25±1.3D. No differences were found between subgroups in both UDVA and objective vision quality measurements (p>0.05) (Table 4).
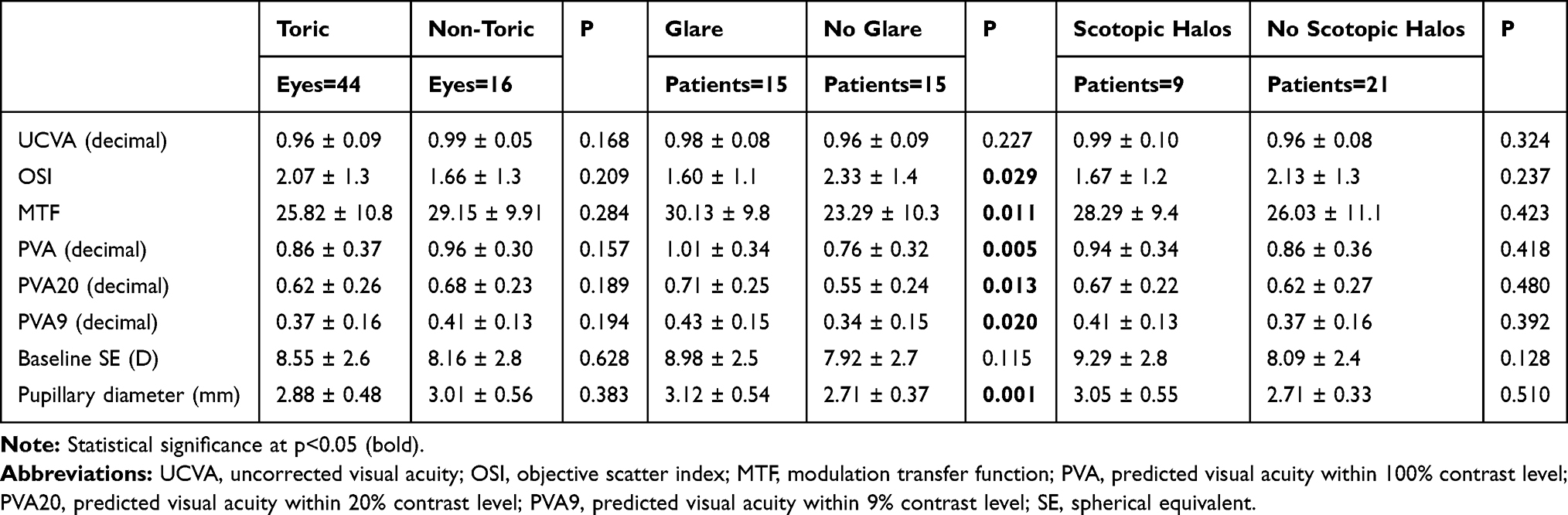 |
Table 4 Subgroup Analysis, End of Follow-Up |
Moderate to severe glare sensitivity was reported by 15 patients and moderate to severe difficult in adaptation to scotopic halos was reported by 9 patients. In the glare complaining patients were found better results in OSI (p=0.029), MTF (p=0.011), PVA (p=0.005) PVA 20 (p=0.013) and PVA 9 (p=0.020). Despite a tendency towards better results in the scotopic halos complaining patients, there were no significant differences between groups regarding postoperative visual function (p>0.05 in all). We found a higher pupillary diameter in the glare complaining patients (p=0.001) but not in the scotopic halos complaining patients (p=0.510) (Table 4).
Associations
A higher UDVA was associated with better results in objective quality of vision assessment: OSI (r=−0.377; p=0.003), MTF (r=0.350; p=0.006), PVA (r=0.365; p=0.004), PVA20 (r=0.338; p=0.008) and PVA9 (r=0.373; p=0.003). On the other hand, was not associated with the subjective quality of vision assessment (p>0.05).
Worse objective vision quality results were associated with higher baseline refractive measurements. The OSI correlations were: r=0.435 (p=0.001) with sphere and r=0.277 (p=0.032) with cylinder; the MTF correlations were r=−0.335 (p=0.009) with sphere and r=−0.305 (p=0.018) with cylinder; the PVA correlations were r=−0.330 (p=0.010) with sphere and r=−0.294 (p=0.022) with cylinder; the PVA20 correlations were r=−0.323 (p=0.012) with sphere and r=−0.289 (p=0.025) with cylinder; the PVA9 correlations were r=−0.309 (p=0.016) with sphere and r=−0.292 (p=0.024) with cylinder.
A worse Dysphotopsia Score was associated with better results in the objective quality of vision assessment: for OSI, r=−0.291 (p=0.024); for MTF, r=0.336 (p=0.009); for PVA, r=0.335 (p=0.009); for PVA20 r=0.336 (p=0.005); for PVA9, r=0.357 (p=0.005). On the other hand, the results on the Satisfaction Score were not associated with any functional parameter (p>0.05 in all).
Discussion
Eyes with similar preoperative refractive errors implanted with either ICL and Artiflex presented very good visual acuities in the present study. Besides similar refractive results, the Artiflex group achieved better UDVA outcomes, not in line with those described by Awadein et al12 which compared Artiflex with ICL V4b in each eye of the same patient, and by Risk et al11 who presented a comparison between the Artiflex with this new ICL V4c. More than a third of eyes improved in, at least, one line after the procedure, with an overall Efficacy Index of 1.11, similar between the two PIOLs. In fact, this improvement in visual acuity has been reported in other studies, and it might be attributed to the neutralization of the concave spectacle lenses effect in high myopic subjects.13,14
In our sample, only 11 out of 60 eyes showed mild additional improvements with sphero-cylindrical correction. These results are similar to those reported in the study of Karimian et al15 which compared results with ICL V4, Artiflex and Artisan®, where a refractive error of nearly half a diopter, in average, was reported with Artiflex and ICL. On the other hand, when comparing only ICL V4c and Artiflex lenses, very good and similar postoperative UDVA and CDVA have been reported; however, with slightly higher SE with both lenses, at 12 months post-procedure, comparing with the present study.11 It is important to refer that despite the high proportion (44/60) of toric PIOLs implanted, in the present study, the refractive and visual acuities were no worse than the reported in the aforementioned studies.
PIOL implantation is mostly performed on a demanding age group and it comprises an additional refractive surface, prone to be associated with visual quality complaints. The assessment of visual quality, achieved through CS testing, was compared between Artiflex and the previous ICL model,16 or the new ICLV4c,11 and both reported only slightly higher sensitivity in the Artiflex group, mainly at low spatial frequencies. Regarding ocular aberrometry, Karimian et al15 reported that both ICL and Artiflex implantation resulted in lower amount of aberrations when compared to Artisan PIOL, and the ICL group has the lowest amount of both total and higher-order aberrations. There is controversy concerning the impact of the central hole presented in the new V4c on patient´s quality of vision when compared with the former V4. Early reports17 showed no difference regarding ocular aberrations and CS, but a recent study18 highlighted an increase in higher-order aberrations, mainly spherical, with still no repercussion in patients complaints, which is justified by the small hole size, according to the authors.
To the best of our knowledge, the present study is the first making a comprehensive quality of vision assessment between these two lenses, both objectively and subjectively, but one limitation is the fact that these parameters were not evaluated preoperatively. Considering the groups included in this study were comparable regarding age, visual acuity and SE, postoperative comparison and assessment seems appropriate. The light scattering in the retina as a marker of global refractive performance of the eye, including the implanted PIOL, showed excellent results with both lenses. The MTF gives information about the CS function, while evaluating only the ocular optical quality. It thus overcomes the possible effect of retinal, optic nerve or even amblyopic changes, which is common in these patients. Our study showed outstanding results in this setting, for both lenses. Despite being the first study using this technology to compare between PIOL, these results are consistent with the reported literature aberrometry outcomes.15,19 Furthermore, the excellent light scattering results achieved with the V4c model, in this study, emphasize the idea of only mild optic aberrations resulting from residual effect of the central hole.18
Considering PVA assessment – which can be understood as the monocular visual acuity the patient would have, should that magnitude depend only on optical factors – similar results were found at the 3 contrast levels, when comparing both lenses, with a total decrease of approximately 2.5 lines of Snellen, between 100% and 20% levels, and 5 lines between 20% and 9% levels, which can be considered a very good optical performance. The association found between worse objective quality of vision results and higher preoperative spherical equivalent highlights the subjective refractive state as a main predictor of surgical outcomes.
Regarding subjective quality of vision assessment – modified Cataract TyPE Spec Questionnaire20 – all patients were found to be very satisfied with the procedure, with the Artiflex group presenting slightly better results on the Satisfaction Score. Complaints of glare were found in half of patients, more than those reported by Karimian et al15 and, in contrast, more in the ICL group; however, the impairment on the adaptation to halos was low and similar in both lenses.
In the subgroup analysis, the unexpected better results achieved in the objective visual function assessment by the glare complaining patients deserve a cautious analysis. It is important to remember that, unlike artificial pupil-based (4 mm) OSI and MTF measurements, real-life vision complaints are related to personality factors and are influenced by the patient pupillary status. Therefore, the significantly higher pupillary diameter found at the end of follow-up in the ICL group is, in our knowledge, the main ocular factor explaining more glare reports, despite the slightly lower light scattering found in the objective analysis. Moreover, only those reporting glare had significantly higher pupillary diameters, which validates our previous discussion. Glare complaints were found both in patients with and without residual SE, no differences found in the preoperative SE between groups, therefore, the authors do not consider the refractive error as an explanatory factor. Nevertheless, the authors consider the sample size of each subgroup a limiting factor in this analysis.
PIOL implantation is still subject to debate in many countries, especially due to the risk of corneal endothelial cell loss above the mean annual rate of 0.6%21 and the risk of cataract development.13 The present study found a 6.7% and 7.9% proportion of ECD decrease in the ICL and Artiflex groups, respectively. Regarding ICL, the ECD losses are slightly inferior to those found in a large meta-analysis,22 including 4196 eyes in which a maximum of 9% was reported. Regarding the Artiflex group, the losses are also slightly inferior than the 9.5% and 10.2% reported at 5 year by Jonker et al, either in spheric and in toric lenses, respectively.23 Our results are in line with those reported in literature, where the procedure is considered the main cause for ECD loss during the first years after the surgery.24 Despite the well-known greater trauma associated to Artiflex implantation, this study showed no differences in the variation of ECD between both groups. In a meta-analysis including 6338 eyes25 undergoing PIOL implantation, the overall risk of developing cataract was 1.1% in the iris-fixated PIOL group (mean follow-up of 32.7 months) and 9.6% in the posterior chamber PIOL group (mean follow-up of 19.2 months). None of the patients in our sample had cataract in both groups, resulting in better outcomes than the previously reported studies. These results might be explained by the low mean age of our sample, below that at which the cataract usually appears and the use of V4c ICL model, associated with less contact between the ICL and the crystalline lens and, therefore, a more physiologic aqueous humor flow.22
Concerning anatomic parameters, significantly lower ACA and ACV were found in the ICL group. The ACA is considered the parameter that better reflects the AC anatomy and a significantly greater variation was observed in the ICL group, similar to previous results.26 Despite the variation in the ACD in the Artiflex group, there was not a variation in the ACA, which guarantees safety, since the ACD after implantation is the critical distance between the corneal endothelium and the PIOL (ACD*) and, therefore, an erroneous measurement of the AC anatomy.
The advantages of the present study are predominantly: the similar baseline characteristics; the same number of eyes in each group; the high proportion of toric lenses in both groups; the analysis of the new ICL V4c model; the comprehensive assessment of quality of vision, both with a new objective measuring technology and with complementary subjective data; the follow-up period since the procedure. The disadvantages and limitations considered in this study are the retrospective nature, the small sample size, and the lack of baseline data on quality of vision parameters.
Conclusion
Both the Visian® ICLV4c™ and the Artiflex® showed excellent optical performance through the HD AnalyzerTM technology, translated in high patient satisfaction in the subjective questionnaire, despite some associated disphotopic complaints in relation with the pupillary diameter. Overall, both PIOLs showed similar safety, predictability, stability and effectiveness of for the reduction of high sphero-cylindrical refractive errors, despite better UDVA results with the Artiflex®.
Acknowledgments
The authors want to acknowledge all the support granted by the head of the Ophthalmology Department of Centro Hospitalar e Universitário do Porto, Prof. Dr. Pedro Menéres. The abstract of this paper was presented at the 37th Congress of the ESCRS as a conference talk with interim findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tinwala SI, Titiyal JS, Titiyal JS. Phakic intraocular lenses an overview. Delhi J Ophthalmol. 2013;24(1):7–15. doi:10.7869/djo.2013.2
2. Galvis V, Villamil JF, Acuña MF, et al. Long-term endothelial cell loss with the iris-claw intraocular phakic lenses (Artisan®). Graefes Arch Clin Exp Ophthalmol. 2019;257(12):2775–2787. doi:10.1007/s00417-019-04506-9
3. Kohnen T. Phakic intraocular lenses: where are we now? J Cataract Refract Surg. 2018;44(2):121–123. doi:10.1016/j.jcrs.2018.03.005
4. Milling A, O’Connor A, Newsham D. The importance of contrast sensitivity testing in children. Br Ir Orthopt J. 2014;11.
5. Jiménez-Alfaro I, Gómez-Tellería G, Bueno JL, Puy P. Contrast sensitivity after posterior chamber phakic intraocular lens implantation for high myopia. J Refract Surg. 2001;17:641–645.
6. Yu A, Wang Q, Xue A, et al. Comparison of contrast sensitivity after angle-supported, iris-fixated and posterior chamber phakic intraocular lens implantation for high myopia. Ophthalmologica. 2008;222(1):53–57. doi:10.1159/000109280
7. Artal P. Understanding aberrations by using double-pass techniques. J Refract Surg. 2000;16:S560–2.
8. Lim DH, Chung ES, Kim MJ, Chung TY. Visual quality assessment after presbyopic laser in-situ keratomileusis. Int J Ophthalmol. 2018;11(3):462–469. doi:10.18240/ijo.2018.03.17
9. Kamiya K, Fusako F, Takushi K, et al. Quantitative analysis of objective forward scattering and its relevant factors in eyes with cataract. Sci Rep. 2019;9(1):3167. doi:10.1038/s41598-019-39680-7
10. Liang GL, Wu J, Shi JT, Liu J, He FY, Xu W. Implantable collamer lens versus iris-fixed phakic intraocular lens implantation to correct myopia: a meta-analysis. PLoS One. 2014;9(8):e104649. doi:10.1371/journal.pone.0104649
11. Rizk IM, Al-Hessy AA, El-Khouly SE, Sewelam AM. Visual performance after implantation of two types of phakic foldable intraocular lenses for correction of high myopia. Int J Ophthalmol. 2019;12(2):284–290. doi:10.18240/ijo.2019.02.16
12. Awadein A, Habib AE. ICL versus veriflex phakic IOL for treatment of moderately high myopia: randomized paired-eye comparison. J Refract Surg. 2013;29(7):445–452. doi:10.3928/1081597X-20130617-02
13. Menezo JL, Peris-Martínez C, Cisneros A, Martínez-Costa R. Posterior chamber phakic intraocular lenses to correct high myopia: a comparative study between staar and adatomed models. J Refract Surg. 2001;17:32–42.
14. Mertens EL. Toric phakic implantable collamer lens for correction of astigmatism: 1-year outcomes. Clin Ophthalmol. 2011;5:369–375. doi:10.2147/OPTH.S7259
15. Karimian F, Baradaran-Rafii A, Hashemian SJ, et al. Comparison of three phakic intraocular lenses for correction of myopia. J Ophthalmic Vis Res. 2014;9(4):427–433. doi:10.4103/2008-322X.150805
16. Ghoreishi M, Masjedi A, Nasrollahi K, Rahgozar A, Jenab K, Fesharaki H. Artiflex versus STAAR implantable contact lenses for correction of high myopia. Oman J Ophthalmol. 2011;4(3):116–119. doi:10.4103/0974-620X.91266
17. Shimizu K, Kamiya K, Igarashi A, Shiratani T. Intraindividual comparison of visual performance after posterior chamber phakic intraocular lens with and without a central hole implantation for moderate to high myopia. Am J Ophthalmol. 2012;154(3):486–94.e1. doi:10.1016/j.ajo.2012.04.001
18. Tian Y, Jiang HB, Jiang J, Wen D, Xia XB, Song WT. Comparison of Implantable Collamer Lens Visian ICL V4 and ICL V4c for high myopia: a cohort study. Medicine. 2017;96(25):e7294. doi:10.1097/MD.0000000000007294
19. Tahzib NG, MacRae SM, Yoon G, et al. Higher-order aberrations after implantation of iris-fixated rigid or foldable phakic intraocular lenses. J Cataract Refract Surg. 2008;34(11):1913–1920. doi:10.1016/j.jcrs.2008.07.014
20. Javitt JC, Jacobson G, Schiffman RM. Validity and reliability of the cataract type spec: an instrument for measuring outcomes of cataract extraction. Am J Ophthalmol. 2003;136(2):285–290. doi:10.1016/S0002-9394(03)00204-6
21. Bourne WM, Nelson LR, Hodge DO. Central corneal endothelial cell changes over a ten-year period. Invest Ophthalmol Vis Sci. 1997;38:779–782.
22. Packer M. The Implantable Collamer Lens with a central port: review of the literature. Clin Ophthalmol. 2018;12:2427–2438. doi:10.2147/OPTH.S188785
23. Jonker SMR, Berendschot T, Ronden AE, Saelens IEY, Bauer NJC, Nuijts R. Five-year endothelial cell loss after implantation with artiflex myopia and artiflex toric phakic intraocular lenses. Am J Ophthalmol. 2018;194:110–119. doi:10.1016/j.ajo.2018.07.015
24. Edelhauser HF, Sanders DR, Azar R, Lamielle H. Corneal endothelial assessment after ICL implantation. J Cataract Refract Surg. 2004;30(3):576–583. doi:10.1016/j.jcrs.2003.09.047
25. Chen LJ, Chang YJ, Kuo JC, Rajagopal R, Azar DT. Metaanalysis of cataract development after phakic intraocular lens surgery. J Cataract Refract Surg. 2008;34(7):1181–1200. doi:10.1016/j.jcrs.2008.03.029
26. Eissa SA, Sadek SH, El-Deeb MWA. Anterior chamber angle evaluation following phakic posterior chamber collamer lens with centraFLOW and its correlation with ICL vault and intraocular pressure. J Ophthalmol. 2016;2016:1383289. doi:10.1155/2016/1383289
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.