Back to Journals » Clinical Ophthalmology » Volume 16
Video Game Warm-Up May Suggest Improvement in Ophthalmic Surgical Simulator Performance in Surgically Naïve Students
Authors Khimani K ![]() , Koshevarova V
, Koshevarova V ![]() , Mathew AA, Gupta AK, Schmitz-Brown M, Gupta PK
, Mathew AA, Gupta AK, Schmitz-Brown M, Gupta PK ![]()
Received 6 April 2022
Accepted for publication 28 June 2022
Published 11 August 2022 Volume 2022:16 Pages 2561—2568
DOI https://doi.org/10.2147/OPTH.S369697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Karima Khimani,1,* Victoria Koshevarova,2,* Alfred A Mathew,2 Akshaya K Gupta,1 Mary Schmitz-Brown,1 Praveena K Gupta1
1Department of Ophthalmology and Visual Sciences, University of Texas Medical Branch, Galveston, TX, USA; 2School of Medicine, University of Texas Medical Branch, Galveston, TX, USA
*These authors contributed equally to this work
Correspondence: Praveena K Gupta, Department of Ophthalmology and Visual Sciences, University of Texas Medical Branch at Galveston, 301 University Blvd, Galveston, TX, 77555-1108, USA, Tel +409 747 5823, Fax +1 409 747 5824, Email [email protected]
Purpose: Long-term video game play and its effects on the skills used in surgical simulators have been previously studied, but little information is available about short-term video game warm-ups and subsequent ophthalmic surgical simulation performance. In this study, we hypothesize that a video game warm-up will improve performance on the Eyesi Ophthalmic Surgical Simulator.
Methods: Twenty medical students with no prior surgical simulation experience were recruited for the study. Information regarding prior video game experience was gathered, and half of the participants were then randomly assigned to play a video game session prior to Eyesi performance. All subjects completed three sets of Eyesi modules, and the scores and time to completion were recorded. Bivariate analysis including Fisher’s Exact test and Wilcoxon rank-sum test were used for statistical analysis.
Results: The warm-up group scored higher in Navigation, Bimanual, and Forceps modules (33.6, 39.7, 7.2, respectively) compared to non-warm-up group (27.3, 27.3, 3.6, respectively). In addition, average times (sec) were lower (310.5, 117.4, 229.2, respectively) compared to non-warm-up group (321.9, 163.3, 235.8, respectively). It was also observed that significantly more participants in the warm-up group had reported a history of spending > 15 hours per week playing video games compared to the non-warm-up group (80% vs 20%, p=0.0402).
Conclusion: In our pilot study, there appears to be a positive trend between video game warm-up and Eyesi simulation performance; however, no statistically significant difference was observed due to lower power. This trend can be explained by a greater collective video game experience within the warm-up group, mechanical factors (increased flexibility and grip strength after playing video games) and feeling more relaxed after the video game warm-up. Larger follow-up studies are needed to further investigate the relationship between short-term video game use on ophthalmic surgical simulation performance.
Keywords: Eyesi, education, surgery, simulation, video game
Introduction
Video games are a very common form of entertainment around the world and the percentage of individuals that enjoy gaming as a hobby continues to increase every year.1 A 2020 survey by the Entertainment Software Association found that 64% of the adults in the United States over the age of 18 played video games, and 75% of the American households contained at least one video game player.1 Given their ubiquity, video games have received significant attention in the media. Consequently, video games can have a negative impact on its users, such as propensity for violence.2 Conversely, certain benefits have been seen with gaming, including increased creativity, visual-spatial skills, hand–eye coordination, depth perception, and attention.3–6 Thus, gaming seems to have potential to increase performance in other tasks that require similar skills.
Surgery is a skill-dependent practice.7–10 Surgeons may benefit from the use of video games as they rely highly on hand–eye coordination.11,12 Ophthalmology surgery is one such discipline that requires a high degree of depth perception, precise hand–eye coordination and higher order of visual-spatial skills that are essentially obtained during residency training. Cataract surgery is the most common ophthalmic surgery performed in the United States,13 and proficiency in cataract extraction is a critical part of residency training given an aging population. The use of surgical simulators is a frequent means of resident training and has been shown to improve intraoperative performance.14–17 Within ophthalmology, the Eyesi Surgical simulator has gained popularity and has been validated as an effective surgical training tool, even as effective as wet lab training.18–22 The Eyesi equips residents with basic surgical techniques while reducing surgeon anxiety, surgeon fatigue, and errors in the operating room, thereby improving patient safety.
Prior studies have shown preoperative surgery warm-up to improve surgical performance on laparoscopic surgeries.23–34 With the advent of electronic simulators within surgical training, the question arises of whether experience with other warm-up systems, such as video games, may offer advantages to trainees. Pike et al reviewed 13 studies, 2 of which involved video game warm-ups, and all of which overall concluded that preoperative simulation improves surgical performance.35 Numerous other studies have examined the effects of video gaming on laparoscopic and endoscopic simulator performance,36–38 and one such study indicated that those who trained on video games outperformed those who trained on the laparoscopic surgical simulator.38
While there is evidence of the benefits of long-term video game use, there is little reported evidence of short term or warm-up video game use. More importantly, to our knowledge, there is no reported study evaluating the effect of preoperative warm-up on ophthalmic surgical performance. This pilot study will primarily evaluate the effects of video game warm-up on Eyesi Ophthalmic Surgical Simulator performance. Secondary objectives will include evaluation of prior video game or musical instrument experience on surgical simulator performance.
Materials and Methods
Participants
This clinical trial was approved by the institutional review board of the University of Texas Medical Branch, Texas (UTMB, approval number 19-0110), and was conducted in accordance with Good Clinical Practice and the tenets of Helsinki Declaration. The small experimental study was set at the UTMB Ophthalmology Department and took 2 years to complete. Twenty current medical students were recruited from the UTMB School of Medicine from all years of training through email invitation and provided signed informed consent. Participants were included in the study if they were between ages 18–40 and had no prior experience on the Eyesi. Initial power calculations utilizing an alpha of 0.05 and power of 80% with expected means of 80 ± 15 and 60 ± 11.6 for intervention vs control groups determined that a sample size of at least 18 would be required (9 for each group).
Questionnaire and Training
Prior to performing Eyesi modules or being informed of their group, all participants filled out a questionnaire regarding any prior experience with video game and/or musical instruments. Information was gathered regarding the number of years and hours per week of playing video game and musical instruments, as well as the number of musical instruments played. Additionally, all participants received a brief instructional video for the Eyesi simulator software (Eyesi Surgical 2.11 SN441, Eyesi Gold Software Plan 36M MO-003-36).
Experimental Group Procedure
Participants were randomly assigned numbers associated with either the warm-up or no warm-up group prior to arrival. Half of the participants (n = 10) were assigned to the experimental video game warm-up group but were unaware of their group until they began the warm-up portion of the procedure. They played Super Smash Bros on the Nintendo 64 console for 10 minutes prior to performing Eyesi modules. Super Smash Bros is a fast-paced single or multi-player game in which the player can defeat an opponent by inputting attack combinations through the handheld controller. Participants had the option to play against the computer or with a human player.
Eyesi Procedure
Participants were instructed, under observation by, to complete three sets of Eyesi modules in the following order: Navigation, Bimanual, and Forceps. Each module was repeated three times for a total of nine tasks per participant. The scores (value between 0 and 100 for all modules) and times to completion (in seconds) were recorded. The maximum completion time was capped at 7 minutes per task.
Data Analysis Methods
Wilcoxon rank-sum test and Fisher’s Exact test were conducted with a p-value of 0.05. Bivariate analysis including Fisher’s Exact test and Wilcoxon rank-sum test was used to detect any statistically significant differences across total score averages for Navigation, Bimanual, and Forceps tasks in the two groups, as well as identify association with questionnaire responses between within each group.
Results
Data from 20 participants were included in the final analysis, of which 10 subjects were in the video game warm-up group. Participants in the video game warm-up group were more likely to have higher average scores than the non-warm-up group in the Navigation module (33.6 vs 27.3, p=0.2257), Bimanual module (39.7 vs 27.3, p=0.2116), and Forceps module (7.2 vs 3.6, p=0.2673), although no significant difference was observed between the two groups (Table 1 and Figure 1). Participants in the video game warm-up group also spent a shorter time (in seconds) compared to the non-warm-up group to complete the Navigation module (310.5 vs 321.9, p=0.3659), Bimanual module (117.4 vs 163.3, p=0.3256), and Forceps module (229.2 vs 235.8, p=1.000), although no significant difference was observed between the two groups (Table 1 and Figure 1). Interestingly, participants in the video game warm-up group were found to have more hours of video game experience (8697 vs 6708, p=0.4956) (Table 1). Significantly, more participants in the video game warm-up group had a history of spending >15 hours per week playing video games compared to the non-warm-up group (80% vs 20%, p=0.0402) (Table 1). There was no statistical difference observed in the number and frequency of playing musical instruments between the two groups.
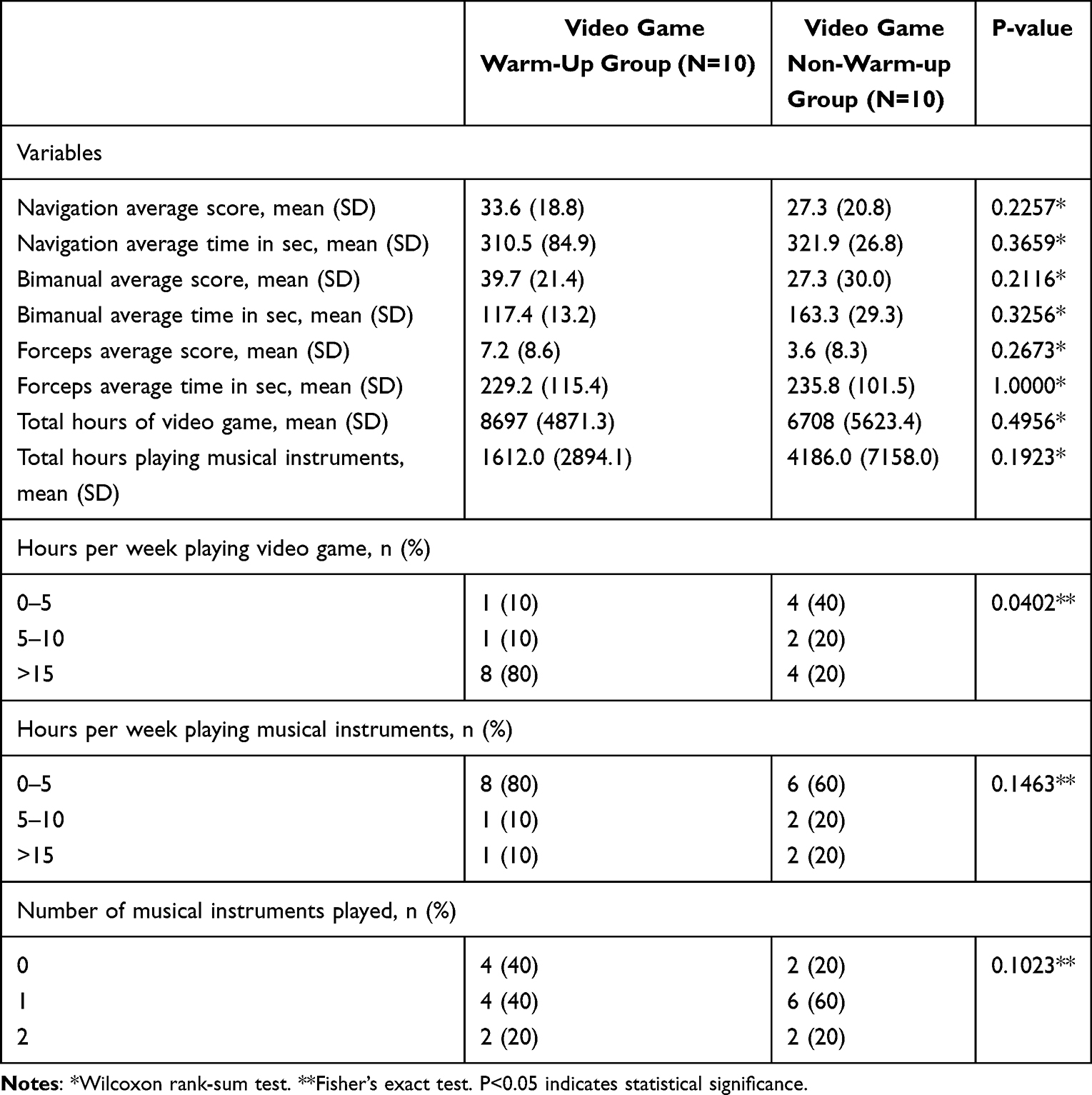 |
Table 1 Descriptive Statistics by Study Groups |
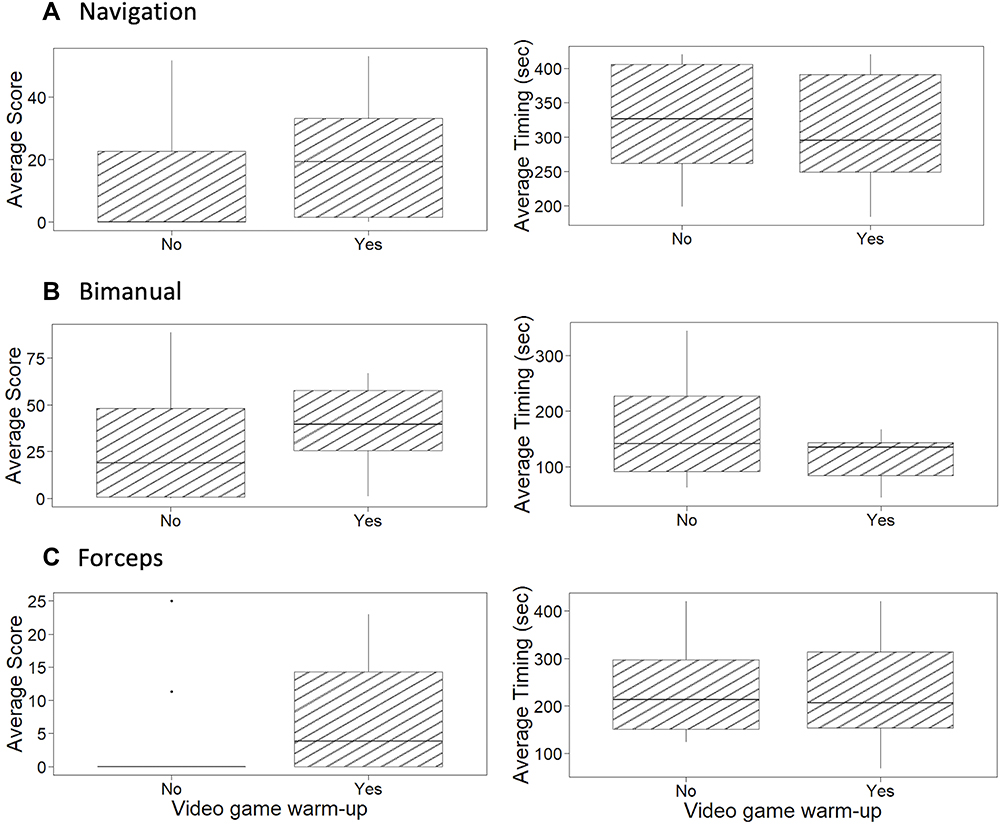 |
Figure 1 Boxplot distribution of average time and scores for (A) navigation, (B) bimanual, and (C) forceps modules in the warm-up and non-warm up study groups. |
Discussion
This pilot study evaluated the effects of preoperative video game warm-up on performance on the Eyesi Ophthalmic Surgical Simulator. The study found a trend showing participants in the video game warm-up group with higher scores and less completion time for all three modules (Navigation, Bimanual, and Forceps) on the Eyesi simulator. Since no significant difference was observed between the two groups, it cannot be reliably concluded that video game warm-up improves Eyesi simulation performance.
Interestingly, even though the participants were randomly assigned to the two groups, participants in the video game warm-up group were more likely to have played >15 hours of video games per week (p = 0.0402) compared to the other group. This finding may have acted as a confounding factor on the Eyesi scores, and although it is still in favor of the hypothesis suggesting that playing video games may improve surgical simulator performance, the distinction between short-term warm-up and long-term play is now difficult to make. Other suggested explanations for the higher performance in the warm-up group include mechanical factors. Increased flexibility and grip strength after the warm-up could have led to better scores, especially on the earlier tasks. Another factor to be considered for both groups is how being observed may have impacted students’ performances, as stress or adrenaline may have affected hand-steadiness.39,40 Conversely, some students may have felt more relaxed from the warm-up itself which could have helped with performance. These possibilities leave room for further investigations on the effects of warm-ups on Eyesi performance.
Furthermore, it can be implied that the effects of prior video game experience on ophthalmic surgery will be similar to its effects on Eyesi simulation performance shown by the pilot study. All Eyesi modules used in this study correlate to basic skills required for performing cataract surgery. The Navigation module develops stereopsis and instrument stability in the anterior chamber of the eye. The Bimanual module develops manual dexterity in the non-dominant hand, allowing users to perform various cataract surgery steps requiring simultaneous use of both hands. The Forceps module develops skills for performing the capsulorhexis step of the cataract surgery, which requires precision in instrument control, and this seemed to be the most technically challenging of the three modules based off the low scores. However, since the participants were all medical students and not surgeons, it can be said that each module appeared relatively independent in terms of difficulty (essentially, all students received below a passing score of 60), though a more experienced Eyesi user may consider certain modules easier/harder. However, almost all participants in both groups improved performance between the first and third tasks of each module. This is consistent with the idea that deliberate practice improves performance.10,41 The study was unable to directly assess the effects of the video game warm-up on ophthalmic surgical performance. However, follow-up studies can be performed on eye surgeons or surgeons-in-training to confirm this relationship.
Prior studies have supported correlation between video game experiences and laparoscopic surgical skills. Both Sammut et al and Datta et al found the video game experience to be advantageous to laparoscopic performance.42,43 Rosser et al analyzed laparoscopic surgical performance of 33 surgical residents with video game exercises and past video game experiences.44 Video game experience of >3 hours per week correlated with 37% fewer errors and 27% faster completion.44 Past video game experiences and video game skills were found to be significant predictors of laparoscopic skills.44 In another study, Richey et al analyzed the effects of past athletic experiences on medical students’ performance on an arthroscopic simulator.45 Students with prior athletic experiences were more likely to achieve competence on the arthroscopic surgical simulator.45 No such studies have been conducted for ophthalmic surgical training, and our pilot study serves as the first known study evaluating the relationship between both, prior video game experiences and video game warm-up, and performance on an ophthalmic surgical simulator.
Limitations
One of the major limitations of the study is the small sample size (N = 20). However, the trend between prior video game exposure and higher performance on the surgical simulator suggests that future studies with a larger study group may show statistically significant associations, supporting our results. Additional factors that may have affected Eyesi performance include improvement on the later tasks with repetition, and conversely, increasing hand fatigue towards the later modules. Secondly, the Eyesi tasks were limited to 7 minutes each, which may have limited the information gathered. For example, even though spending more time on an Eyesi module results in a lower score, some subjects may still have scored higher if provided with more time. Thirdly, some video game participants experienced an increased amount of time between watching the simulator tutorial and performing on the simulator. This time gap may have impacted their performance on the Eyesi simulator. Lastly, although all participants had no prior simulator or ophthalmic surgery experience, the study did not control for exposure to ophthalmology. Participants with greater knowledge of the eye anatomy and cataract surgery may have performed better.
Conclusion
Although the results of the study were not statistically significant due to low power, a positive trend was found which can be considered consistent with prior studies reporting enhanced simulator performance in the context of prior video game experience. The positive trend can also be explained by a greater collective video game experience within the warm-up group, which introduced an important confounding. Other explanations include mechanical factors (increased flexibility and grip strength after playing video games) and feeling more relaxed after the video game warm-up. However, the technical skills of laparoscopic simulation differ from microsurgical ophthalmic simulation and may not be completely comparable. No prior studies have evaluated the effects of video game experience on ophthalmic surgical training specifically. Future studies with more participants as well as longer trial periods could be beneficial in providing more significant results.
Clinical Application
Given cataract surgery is the most commonly performed ophthalmic surgery in the United States, it is imperative that ophthalmology trainees are proficient in performing them. This study seeks to identify potential tools that may be beneficial in developing skills necessary to become competent cataract surgeons and avoid potentially vision-threatening outcomes.
Data Sharing Statement
The patient data used to support the findings of this study are restricted by the University of Texas Medical Branch Institutional Review Board (approval number 19-0110) in order to protect patient privacy. Data are available from Praveena Gupta, PhD, OD, FAAO ([email protected]) for researchers who meet the criteria for access to confidential data.
Acknowledgments
The authors would like to acknowledge Humair Khan, MD, and Andrew Wallmann, MD, for their contributions to the design of the study. The authors would also like to thank Ms Efstathia Polychronopoulou and Ms Biai Dominique Elmir Digbeu for helping with the biostatistics for data analysis.
Funding
This study was conducted using internal grants to the department of Ophthalmology at the University of Texas at Medical Branch.
Disclosure
The authors have not published, posted, or submitted any related papers from this study. The authors report no conflicts of interest.
References
1. Entertainment Software Association. Essential facts - theesa.com. 2020 Essential facts about the video game industry; (n.d.). Available from: http://www.theesa.com/wp-content/uploads/2021/03/Final-Edited-2020-ESA_Essential_facts.pdf.
2. Gentile DA, Lynch PJ, Linder JR, Walsh DA. The effects of violent video game habits on adolescent hostility, aggressive behaviors, and school performance. J Adolesc. 2004;27(1):5–22. doi:10.1016/j.adolescence.2003.10.002
3. Griffith JL, Voloschin P, Gibb GD, Bailey JR. Differences in eye-hand motor coordination of video-game users and non-users. Percept Mot Skills. 1983;57(1):155–158. doi:10.2466/pms.1983.57.1.155
4. Burgos PI, Mariman JJ, Makeig S, Rivera-Lillo G, Maldonado PE. Visuomotor coordination and cortical connectivity of modular motor learning. Hum Brain Mapp. 2018;39(10):3836–3853. doi:10.1002/hbm.24215
5. Green CS, Bavelier D. Effect of action video games on the spatial distribution of visuospatial attention. J Exp Psychol Hum Percept Perform. 2006;32(6):1465–1478. doi:10.1037/0096-1523.32.6.1465
6. Green CS, Bavelier D. Action video game modifies visual selective attention. Nature. 2003;423(6939):534–537. doi:10.1038/nature01647
7. Bech B, Lönn L, Schroeder TV, Ringsted C. Fine-motor skills testing and prediction of endovascular performance. Acta Radiol. 2013;54(10):1165–1174. doi:10.1177/0284185113491088
8. Figueiredo S, Machado L, Lousada ADP, Castelo LS, Fardilha ML, Sa A. Physicians versus surgeons. A pilot study on hand dexterity within a controlled population. Acta Orthop Belg. 2016;82(3):456–461.
9. Squire D, Giachino AA, Profitt AW, Heaney C. Objective comparison of manual dexterity in physicians and surgeons. Can J Surg. 1989;32(6):467–470.
10. Khunger N, Kathuria S. Mastering surgical skills through simulation-based learning: practice makes one perfect. J Cutan Aesthet Surg. 2016;9(1):27–31. doi:10.4103/0974-2077.178540
11. Dye MW, Green CS, Bavelier D. Increasing speed of processing with action video games. Curr Dir Psychol Sci. 2009;18(6):321–326. doi:10.1111/j.1467-8721.2009.01660.x
12. Latham AJ, Patston LL, Tippett LJ. The virtual brain: 30 years of video-game play and cognitive abilities. Front Psychol. 2013;4:629. doi:10.3389/fpsyg.2013.00629
13. Usmani B, Iftikhar M, Latif A, Shah SMA. Epidemiology of primary ophthalmic procedures performed in the United States. Can J Ophthalmol. 2019;54(6):727–734. doi:10.1016/j.jcjo.2019.03.006
14. Crochet P, Aggarwal R, Dubb SS, et al. Deliberate practice on a virtual reality laparoscopic simulator enhances the quality of surgical technical skills. Ann Surg. 2011;253(6):1216–1222. doi:10.1097/SLA.0b013e3182197016
15. McCannel CA, Reed DC, Goldman DR. Ophthalmic surgery simulator training improves resident performance of capsulorhexis in the operating room. Ophthalmology. 2013;120(12):2456–2461. doi:10.1016/j.ophtha.2013.05.003
16. Pokroy R, Du E, Alzaga A, et al. Impact of simulator training on resident cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2013;251(3):777–781. doi:10.1007/s00417-012-2160-z
17. Seymour NE, Gallagher AG, Roman SA, et al. Virtual reality training improves operating room performance: results of a randomized, double-blinded study. Ann Surg. 2002;236(4):
18. Thomsen AS, Kiilgaard JF, Kjaerbo H, la Cour M, Konge L. Simulation-based certification for cataract surgery. Acta Ophthalmol. 2015;93(5):416–421. doi:10.1111/aos.12691
19. Bergqvist J, Person A, Vestergaard A, Grauslund J. Establishment of a validated training programme on the Eyesi cataract simulator. A prospective randomized study. Acta Ophthalmol. 2014;92(7):629–634. doi:10.1111/aos.12383
20. Solverson DJ, Mazzoli RA, Raymond WR, et al. Virtual reality simulation in acquiring and differentiating basic ophthalmic microsurgical skills. Simul Healthc. 2009;4(2):98–103. doi:10.1097/SIH.0b013e318195419e
21. Thomsen AS, Bach-Holm D, Kjaerbo H, et al. Operating room performance improves after proficiency-based virtual reality cataract surgery training. Ophthalmology. 2017;124(4):524–531. doi:10.1016/j.ophtha.2016.11.015
22. Daly MK, Gonzalez E, Siracuse-Lee D, Legutko PA. Efficacy of surgical simulator training versus traditional wet-lab training on operating room performance of ophthalmology residents during the capsulorhexis in cataract surgery. J Cataract Refract Surg. 2013;39(11):1734–1741. doi:10.1016/j.jcrs.2013.05.044
23. Weston MK, Stephens JH, Schafer A, Hewett PJ. Warm-up before laparoscopic surgery is not essential. ANZ J Surg. 2014;84(3):143–147. doi:10.1111/j.1445-2197.2012.06321.x
24. Chen CC, Green IC, Colbert-Getz JM, et al. Warm-up on a simulator improves residents’ performance in laparoscopic surgery: a randomized trial. Int Urogynecol J. 2013;24(10):1615–1622. doi:10.1007/s00192-013-2066-2
25. Calatayud D, Arora S, Aggarwal R, et al. Warm-up in a virtual reality environment improves performance in the operating room. Ann Surg. 2010;251(6):1181–1185. doi:10.1097/SLA.0b013e3181deb630
26. Do AT, Cabbad MF, Kerr A, Serur E, Robertazzi RR, Stankovic MR. A warm-up laparoscopic exercise improves the subsequent laparoscopic performance of Ob-Gyn residents: a low-cost laparoscopic trainer. JSLS. 2006;10(3):297–301.
27. Plerhoples TA, Zak Y, Hernandez-Boussard T, Lau J. Another use of the mobile device: warm-up for laparoscopic surgery. J Surg Res. 2011;170(2):185–188. doi:10.1016/j.jss.2011.03.015
28. Lendvay TS, Brand TC, White L, et al. Virtual reality robotic surgery warm-up improves task performance in a dry laboratory environment: a prospective randomized controlled study. J Am Coll Surg. 2013;216(6):1181–1192. doi:10.1016/j.jamcollsurg.2013.02.012
29. Kroft J, Ordon M, Arthur R, Pittini R. Does surgical “warming up” improve laparoscopic simulator performance? Simul Healthc. 2012;7(6):339–342. doi:10.1097/SIH.0b013e31826230d4
30. Willaert WI, Aggarwal R, Daruwalla F, et al.; European Virtual Reality Endovascular Research Team EVEResT. Simulated procedure rehearsal is more effective than a preoperative generic warm-up for endovascular procedures. Ann Surg. 2012;255(6):1184–1189. doi:10.1097/SLA.0b013e31824f9dbf
31. Lee JY, Mucksavage P, Kerbl DC, et al. Laparoscopic warm-up exercises improve performance of senior-level trainees during laparoscopic renal surgery. J Endourol. 2012;26(5):545–550. doi:10.1089/end.2011.0418
32. Moldovanu R, Târcoveanu E, Dimofte G, Lupaşcu C, Bradea C. Preoperative warm-up using a virtual reality simulator. JSLS. 2011;15(4):533–538. doi:10.4293/108680811X13176785204409
33. Rosser JC, Gentile DA, Hanigan K, Danner OK. The effect of video game “warm-up” on performance of laparoscopic surgery tasks. JSLS. 2012;16(1):3–9. doi:10.4293/108680812X13291597715664
34. Kahol K, Satava RM, Ferrara J, Smith ML. Effect of short-term pretrial practice on surgical proficiency in simulated environments: a randomized trial of the “preoperative warm-up” effect. J Am Coll Surg. 2009;208(2):255–268. doi:10.1016/j.jamcollsurg.2008.09.029
35. Pike TW, Pathak S, Mushtaq F, Wilkie RM, Mon-Williams M, Lodge JPA. A systematic examination of preoperative surgery warm-up routines. Surg Endosc. 2017;31(5):2202–2214. doi:10.1007/s00464-016-5218-x
36. Adams BJ, Margaron F, Kaplan BJ. Comparing video games and laparoscopic simulators in the development of laparoscopic skills in surgical residents. J Surg Educ. 2012;69(6):714–717. doi:10.1016/j.jsurg.2012.06.006
37. Middleton KK, Hamilton T, Tsai PC, Middleton DB, Falcone JL, Hamad G. Improved nondominant hand performance on a laparoscopic virtual reality simulator after playing the Nintendo Wii. Surg Endosc. 2013;27(11):4224–4231. doi:10.1007/s00464-013-3027-z
38. Schlickum MK, Hedman L, Enochsson L, Kjellin A, Fellander-Tsai L. Systematic video game training in surgical novices improves performance in virtual reality endoscopic surgical simulators: a prospective randomized study. World J Surg. 2009;33(11):2360–2367. doi:10.1007/s00268-009-0151-y
39. Arnold RW, Springer DT, Engel WK, Helveston EM. The effect of wrist rest, caffeine, and oral timolol on the hand steadiness of ophthalmologists. Ann Ophthalmol. 1993;25(7):250–253.
40. Dhaif F, Paparoidamis G, Sideris M, et al. The role of anxiety in simulation-based dexterity and overall performance: does it really matter? J Invest Surg. 2019;32(2):164–169. doi:10.1080/08941939.2017.1387624
41. Bosse HM, Mohr J, Buss B, et al. The benefit of repetitive skills training and frequency of expert feedback in the early acquisition of procedural skills. BMC Med Educ. 2015;15:22. doi:10.1186/s12909-015-0286-5
42. Sammut M, Sammut M, Andrejevic P. The benefits of being a video gamer in laparoscopic surgery. Int J Surg. 2017;45:42–46. doi:10.1016/j.ijsu.2017.07.072
43. Datta R, Chon SH, Dratsch T, et al. Are gamers better laparoscopic surgeons? Impact of gaming skills on laparoscopic performance in “Generation Y” students. PLoS One. 2020;15(8):e0232341. doi:10.1371/journal.pone.0232341
44. Rosser JC, Lynch PJ, Cuddihy L, Gentile DA, Klonsky J, Merrell R. The impact of video games on training surgeons in the 21st century. Arch Surg. 2007;142:181–186. doi:10.1001/archsurg.142.2.181
45. Richey BP, Deal MJ, Baker A, et al. Predictors of performance on the arthrobox arthroscopy simulator for medical students. Arthrosc Sports Med Rehabil. 2020;2(6):e829–e837. doi:10.1016/j.asmr.2020.07.022
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.