Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Vericiguat in Heart Failure with a Reduced Ejection Fraction: Patient Selection and Special Considerations
Authors Kassis-George H, Verlinden NJ ![]() , Fu S, Kanwar M
, Fu S, Kanwar M
Received 12 January 2022
Accepted for publication 19 March 2022
Published 30 March 2022 Volume 2022:18 Pages 315—322
DOI https://doi.org/10.2147/TCRM.S357422
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Hayah Kassis-George,1 Nathan J Verlinden,1 Sheng Fu,2 Manreet Kanwar1
1Cardiovascular Institute, Allegheny General Hospital, Pittsburgh, PA, USA; 2Division of Cardiology, Department of Medicine, Medical University of South Carolina, Charleston, SC, USA
Correspondence: Nathan J Verlinden, Cardiovascular Institute, Allegheny General Hospital, 320 E. North Ave., Pittsburgh, PA, 15212, Tel +1 412-359-3240, Fax +1 412-359-4806, Email [email protected]
Abstract: With improvement in the understanding of the pathophysiological mechanisms of heart failure with reduced ejection fraction (HFrEF), several drug classes have been developed targeting the renin–angiotensin–aldosterone system, the beta adrenergic system, and to a certain extent the nitric oxide pathway. Recently, the use of sodium-glucose cotransporter-2 (SGLT-2) inhibitors has resulted in a reduction in heart failure hospitalizations and cardiovascular death. As a result, SGLT-2 inhibitors are now the fourth drug class recommended as part of guideline-directed medical therapy (GDMT) for HFrEF. Soluble guanylate cyclase (sGC) stimulators, such as vericiguat, are a novel therapy targeting the cyclic guanosine monophosphate (cGMP) pathway with downstream effects including smooth muscle cell relaxation and a reduction in hypertrophy, inflammation, and fibrosis. The recently published VICTORIA trial has demonstrated a reduction in heart failure hospitalizations or cardiovascular death with vericiguat. Patients with a baseline N-terminal pro-B-type natriuretic peptide (NT-proBNP) values < 8000 pg/mL may identify a sub-group most likely to benefit with addition of vericiguat. The cumulative benefit of quadruple therapy with the addition of sGC stimulators remains unknown. We review the mechanism of action for sGC stimulators, clinical trial data, and their real-world application to HFrEF patients with consideration of quintuple therapy.
Keywords: vericiguat, soluble guanylate cyclase stimulators, heart failure with reduced ejection fraction, guideline-directed medical therapy, VICTORIA
Introduction
Heart failure (HF) remains the number one admission diagnosis identified by the Centers for Medicare and Medicaid, with a projected incidence in the United States of 3% by 2030. The number of patients with HF is expected to further rise from 5.7 million in 2012 to 8 million in the next 8 years.1 HF with a reduced ejection fraction (HFrEF), defined as patients with a left ventricular ejection fraction (LVEF) of ≤40%, accounts for approximately 50% of overall HF cases.2 Recent advances in guideline-directed medical therapy (GDMT) for HFrEF, including the use of angiotensin receptor-neprilysin inhibitors (ARNI) and sodium-glucose cotransporter-2 (SGLT-2) inhibitors, have resulted in reduced morbidity and mortality when fully optimized.3–5
Therapies for HFrEF have not historically addressed endothelial dysfunction or targeted the nitric oxide (NO) pathway. Decompensated HF results in inhibition of the nitric oxide-soluble guanylate cyclase (NO-sGC) pathway, hence restoration of sufficient sGC signaling could help attenuate HF pathology.6,7 Vericiguat is a novel therapy targeting the cyclic guanosine monophosphate (cGMP) pathway by stimulating sGC leading to downstream effects including the relaxation of smooth muscle cells as well as reduced hypertrophy, inflammation, and fibrosis.8 A recent Phase 3 trial treating higher risk HF patients with vericiguat demonstrated a significant reduction in a composite end point of cardiovascular (CV) death or first heart failure hospitalization (HFH).9 The purpose of this review is to present the clinical trials and literature leading to the development of vericiguat with a focus on the clinical application of this drug in addition to GDMT.
Role of cGMP in the Pathophysiology of HF
The NO-sGC-cGMP pathway plays an important role in the pathogenesis of HF.6,7,10 The vascular endothelium normally generates NO which stimulates sGC mediated cGMP production. The endocardial endothelium, in addition to being sensitive to NO, regulates contractility and diastolic function by raising intracellular cGMP. NO is synthesized from L-arginine by 3 different enzymes including endothelial nitric oxide synthase (eNOS), neuronal nitric oxide synthase, and inducible isoforms of nitric oxide synthase. Under typical physiological conditions, NO is produced by eNOS and diffuses rapidly to the smooth muscle cells in the vasculature, binding with the heme subunit of sGC, thus catalyzing the conversion of guanosine triphosphate (GTP) to the intracellular second messenger, cGMP.7,10
Cyclic GMP promotes the activation of the primary effector, protein kinase G (PKG). In cardiac myocytes, impaired PKG signaling has been demonstrated to promote left ventricular stiffness by hypophosphorylation of titin.11 The stimulation of PKG results in downstream effects such as smooth muscle relaxation, vasodilation, inhibition of hypertrophy, reduction in inflammation and fibrosis, and improvement in cardiac remodeling (Figure 1).10 In HF, the NO-sGC-cGMP pathway is impaired due to increased inflammation, oxidative stress, and endothelial dysfunction leading to reduced bioavailability of NO and higher conversion of sGC from its native heme-Fe2+- containing form, for which NO has a high affinity, to the oxidized, dysfunctional heme-free-Fe3+-form of sGC.7,10 This impaired cGMP pathway in HF is thought to contribute to adverse effects on the heart, kidneys, and vasculature, promoting further disease progression.
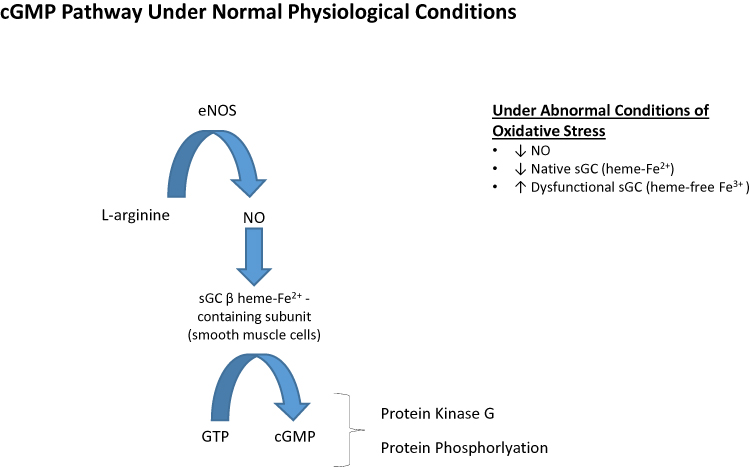 |
Figure 1 Cyclic guanosine monophosphate (cGMP) pathway. Abbreviations: eNOS, endothelial nitric oxide synthase; NO, nitric oxide; sGC, soluble guanylate cyclase; GTP, guanosine triphosphate; cGMP, cyclic guanosine monophosphate. |
Pharmacology of Vericiguat
Vericiguat acts as a stimulator of sGC, acting synergistically with available NO but also binding to the heme-containing form of sGC, leading to an increase in cGMP levels with subsequent beneficial effects on cardiac and vascular function.8 Alternatively, sGC activators, such as cinaciguat, act only on dysfunctional sGC independently of endogenous NO. Alterations in the chemical structure of vericiguat, when compared to other sGC stimulators such as riociguat, have resulted in improved pharmacokinetic stability and excellent oral bioavailability with a long half-life, allowing for once daily oral administration (Table 1).8,12 Due to these unique pharmacokinetic and pharmacodynamic properties, vericiguat has a milder effect on blood pressure, compared with other sGC inducible drugs, with approximate reductions of 2 mm Hg in systolic blood pressure on average.9,13,14 Adverse events that occurred more frequently in clinical studies with vericiguat compared to placebo include anemia (7.6% vs 5.7%) and symptomatic hypotension (9.1% vs 7.9%).9,15
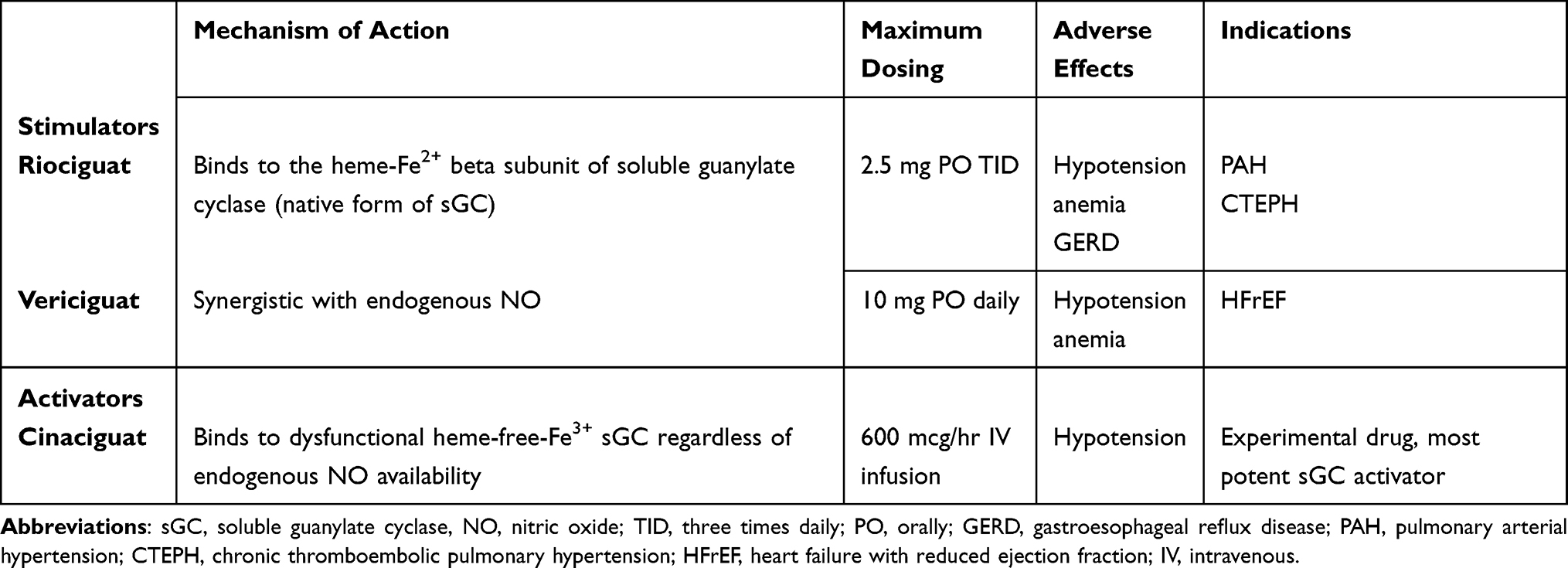 |
Table 1 sGC Stimulators and Activators |
Evolution of GDMT in HFrEF
Pharmacologic treatment of HFrEF has come a long way in the past 50 years. While initial strategies in the 1970s focused on vasodilation, the neurohormonal aspect of heart failure soon became the dominant focus of medical therapy over the subsequent decades.16 The 1995 American College of Cardiology/American Heart Association (ACC/AHA) Guidelines for the Evaluation and Management of Heart Failure reflect this focus by giving angiotensin converting enzyme (ACE) inhibitors and hydralazine/isosorbide dinitrate a class I recommendation, while beta blockers were given a weaker recommendation.17 By the time the 2005 guideline updates were written, large-scale randomized controlled clinical trials had cemented beta blockade, renin-angiotensin system (RAS) inhibition, as well as mineralocorticoid receptor antagonism (MRA) as class I therapies in heart failure with systolic dysfunction.18–23 We are in an era of rapid growth in evidence for the use of therapies with a much wider range of pathophysiological pathways.
Reflecting the ever-changing landscape of medical therapy in this space, the next target to generate guideline changing data was neprilysin. Neprilysin is a naturally occurring peptide that is involved in the degradation of a variety of vasoactive agents including natriuretic peptides and bradykinin.24 LCZ696 was designed as a combination of sacubitril (a neprilysin inhibitor) and valsartan and was shown in the PARADIGM-HF trial to be superior to enalapril alone in reducing the risk of death or HFH.4 Of note, the patient population in this trial reflected the strong medical therapy of the time, with 93% of patients receiving beta blockers at the time of enrollment, although only a little more than half of the patients were taking an MRA.
The next evolution of heart failure therapies came with the serendipitous discovery of SGLT2 inhibitors. Found in the root bark of apple trees, phlorizin had been known since the 1930s to increase glucosuria by preventing reabsorption in the renal tubules. Synthetic versions of phlorizin were thought to be a novel therapeutic class for diabetes mellitus, until the EMPA-REG OUTCOME trial unexpectedly found empagliflozin to provide 35% relative risk reduction in heart failure hospitalizations against placebo in patients with diabetes and cardiovascular disease.25 Two additional SGLT2 inhibitors, dapagliflozin and canagliflozin, also found similar preliminary results.26,27 These findings ultimately led to the landmark EMPEROR-Reduced and DAPA-HF trials, which cemented these medications as part of the current armamentarium of guideline therapies.3,5,28
Despite the overwhelming amount of data supporting their efficacy, GDMT (currently “quadruple therapy,” encompassing a beta blocker, RAS inhibitor, MRA and SGLT2 inhibitor) usage remains infrequent in clinical practice due to a variety of factors including awareness gaps, therapeutic inertia, and side effect profiles.29 Thus, novel therapies such as vericiguat must contend with both the potency of current medical therapy as well as the ongoing struggles of individualizing patient risk and side effect profiles to increase utilization.
Clinical Trials Using sGC Stimulators or Activators in HFrEF
Prior to the development of vericiguat, both cinaciguat and riociguat were studied for their hemodynamic effects on patients with HFrEF (Table 2). In a Phase 2b trial, patients with acute decompensated HF who received cinaciguat had a significant reduction in pulmonary capillary wedge pressure (PCWP) at 8 hours compared to placebo; however, a high rate of hypotension in the cinaciguat group led to premature discontinuation of the trial.13 Riociguat was evaluated in patients with pulmonary hypertension due to LV systolic dysfunction in the phase 2 LEPHT study.30 Riociguat failed to meet the primary end point, placebo-corrected change from baseline to week 16 in mean pulmonary artery pressure (mPAP), compared to placebo (p = 0.10). Two clinical trials (SOCRATES-REDUCED and VICTORIA) have evaluated the safety and efficacy of vericiguat in patients with HFrEF.
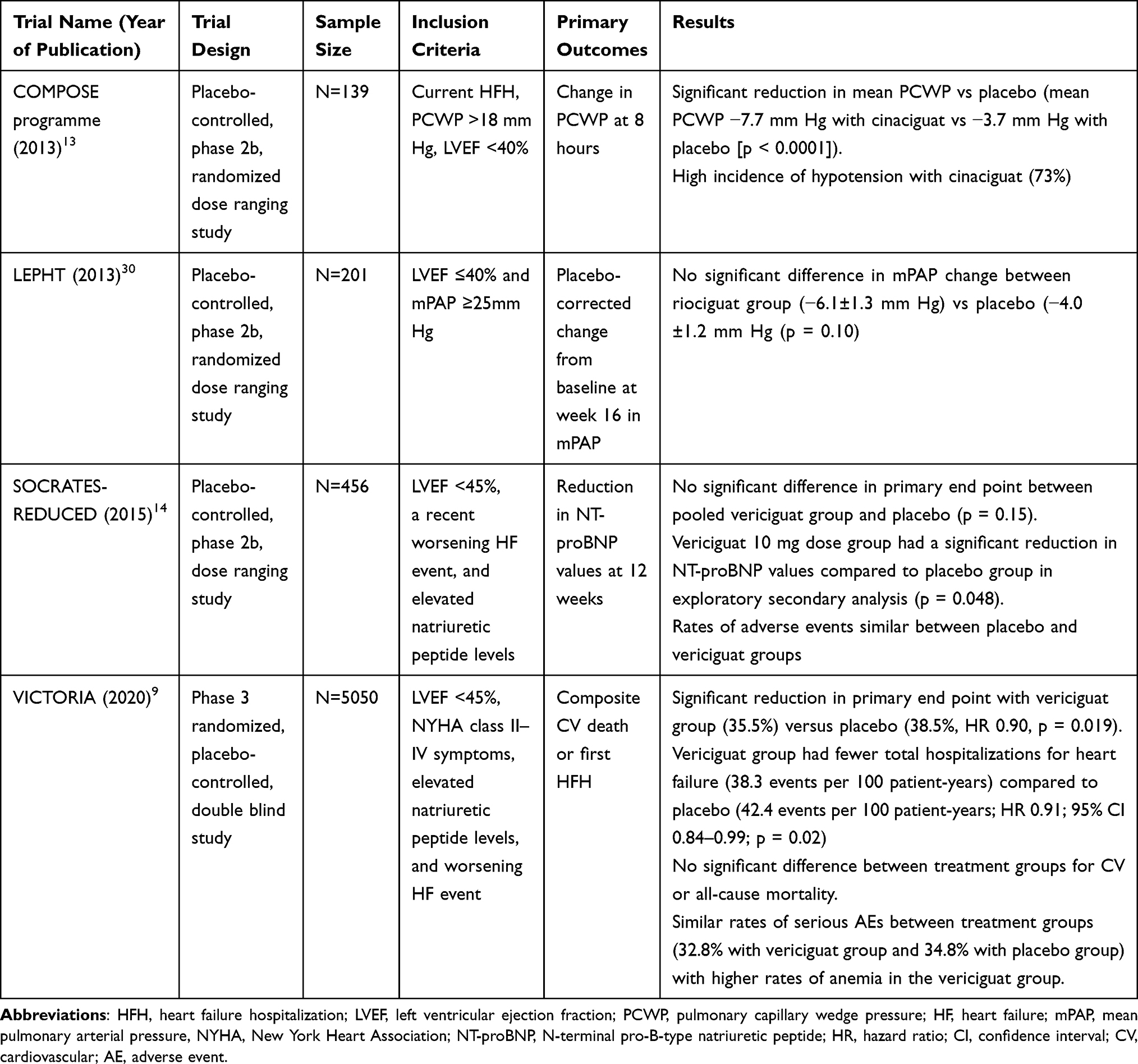 |
Table 2 Clinical Trials Evaluating Soluble Guanylate Cyclase Stimulators or Activators in Heart Failure with a Reduced Ejection Fraction |
The phase 2 SOCRATES-REDUCED trial enrolled 456 patients with an LVEF of <45%, a recent worsening HF event, and elevated natriuretic peptide levels.14 Patients were randomized to placebo or 1 of 4 target doses with vericiguat (1.25 mg, 2.5 mg, 5 mg, or 10 mg once daily). The primary end point, change in log-transformed N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels over 12 weeks, was not significantly different in the pooled vericiguat group compared to the placebo group (p = 0.15). An exploratory secondary analysis of the primary end point suggested a dose-response relationship with higher vericiguat doses associated with a larger reduction in NT-proBNP values (p < 0.02). A pairwise analysis of the vericiguat 10 mg dose demonstrated a significant reduction in log-transformed NT-proBNP values compared to placebo (p = 0.048). Vericiguat therapy was not associated with a significant change in blood pressure or heart rate and overall adverse event rates were similar between placebo and vericiguat groups.
VICTORIA was a randomized, placebo-controlled, double-blind, phase 3 trial (n = 5050), assessing the efficacy and safety of vericiguat in patients with HFrEF.9 Patients were included if they had New York Heart Association (NYHA) functional class II–IV symptoms, elevated natriuretic peptide values, an LVEF of <45%, and were hospitalized with HF within the last 6 months or received intravenous (IV) diuretics for decompensated symptoms. For patients who received vericiguat, the starting dose was 2.5 mg daily with the dose doubled every 2 weeks if tolerated to the maximum dose of 10 mg daily. Patients were continued on dose titration if the systolic blood pressure was ≥ 100 mm Hg. The dose of vericiguat was maintained if the systolic blood pressure was < 100 mm Hg but ≥ 90 mm Hg and the dose was interrupted or decreased if the systolic blood pressure was < 90 mm Hg. The primary end point was a composite of CV death or first HFH.
Over a median follow-up of 10.8 months, patients treated with vericiguat experienced a significant reduction in the primary end point (35.5% vs 38.5% in the placebo group; hazard ratio [HR] 0.90, 95% confidence interval [CI] 0.83–0.98, p = 0.02). The number needed to treat with vericiguat for 1 year to avoid one primary end point event was 24. The reduction of primary end point was driven by a reduction in first HFH events (27.4% in the vericiguat group vs 29.6% in the placebo group, HR 0.90; 95% CI 0.81–1.00) with no significant difference between treatment groups in CV or overall mortality. On sub-group analysis, the effect of vericiguat on the primary end point appeared consistent across many sub-groups including sex, geographic region, and NYHA class; however, the benefit appeared to be attenuated in patients with an age ≥75 years, with the highest quartile of NT-proBNP (> 5314 pg/mL), or with LVEF between 40–45%, although specific p-values for interaction were not reported. Additional sub-analyses of the VICTORIA trial have demonstrated a consistent treatment effect of vericiguat regardless of baseline estimated glomerular filtration rate (eGFR), index worsening HF event, or history of atrial fibrillation.31–33 Another sub-analysis of VICTORIA further evaluated the impact of baseline NT-proBNP values on the treatment effect of vericiguat.34 Patients with baseline NT-proBNP values < 8000 pg/mL treated with vericiguat, compared to placebo, showed a significant reduction in the primary end point (HR 0.85, 95% CI 0.76–0.95) including a reduction in CV mortality (HR 0.84, 95% CI 0.71–0.99), whereas patients with baseline NT-proBNP values ≥ 8000 pg/mL experienced no significant benefit in the primary end point with vericiguat treatment (HR 1.16, 95% CI 0.94–1.41).
Overall, vericiguat was well tolerated in VICTORIA with similar adverse event rates compared to placebo. The target dose of 10 mg with vericiguat was achieved in 89% of patients. Rates of symptomatic hypotension were numerically higher with vericiguat (9.1%) compared to placebo (7.9%), although this did not reach statistical significance (p = 0.12). There was no significant difference between treatment groups for syncopal events. Rates of anemia occurred more frequently in patients treated with vericiguat (7.6%) compared with placebo (5.7%). At 16 weeks, the mean change in hemoglobin was mild at −0.24 g/dL with vericiguat compared to placebo (95% CI, −0.312 to −0.163; p < 0.001) and more patients experienced anemia with vericiguat (13.6%) compared to placebo (10.5%, p < 0.001).35 A time-updated analysis of hemoglobin from the VICTORIA trial showed no significant association with the treatment effect of vericiguat on the primary end point compared to placebo.35
Vericiguat in Clinical Practice
The VICTORIA trial demonstrated the efficacy and safety of vericiguat in patients with HFrEF with some unique features of this study. By design, VICTORIA included patients who were generally higher risk than those enrolled in previous clinical trials in patients with chronic HFrEF as evidenced by higher median NT-proBNP values (median 2816 pg/mL vs 1608 pg/mL in PARADIGM-HF) and more patients with NYHA class III or IV symptoms at baseline (40% vs 25% in PARADIGM-HF).4 This is further demonstrated by a considerably higher event rate in VICTORIA (38.5% with placebo) compared to PARADIGM-HF (26.5% with enalapril) over a shorter follow-up period (11 months in VICTORIA vs 27 months in PARADIGM-HF). The study also required enrollment within 6 months of HFH or within 3 months of IV diuretic therapy with most patients (67%) being enrolled within 3 months of HFH. Patients with a baseline systolic blood pressure < 100 mm Hg or on long-acting nitrates were excluded, and few Black patients (4.9%) and NYHA class IV patients (1.3%) were enrolled, limiting generalizability of results in these patient populations. Notably, 60% of patients were on background triple GDMT therapy, including beta-blockers, RAS inhibitor, and MRA, with low rate of ARNI utilization (15%) and unreported rates of SGLT-2 inhibitor use. Therefore, vericiguat was primarily studied in addition to triple GDMT therapy and further studies are warranted to ascertain additional benefit in combination with SGLT-2 inhibitors and an ARNI. Indeed, neprilysin inhibition enhances guanylate cyclase signaling via particulate guanylate cyclase, but it remains to be seen if this leads to synergistic clinical benefit or enhances the risk of adverse events.6
Currently, vericiguat is not addressed in the most recent 2021 update to the ACC Decision Pathway for HF as the medication was not approved by Food and Drug Administration (FDA) at the time of publication.28 The 2021 European Society of Cardiology (ESC) HF guidelines provide one recommendation on the use of vericiguat, based upon the findings of the VICTORIA trial.36 Vericiguat may be considered in symptomatic patients with HFrEF who have had worsening HF despite treatment with GDMT to reduce the risk of CV mortality or HFH (Class IIb; Level of Evidence: B).
With the recent advances in GDMT for HFrEF, it remains an ongoing challenge to position newer treatments, such as vericiguat, while understanding that traditional GDMT remains underutilized in clinical practice. Vericiguat joins an increasingly growing list of oral HFrEF medications that have been demonstrated to reduce HFH events without a significant impact on CV mortality, including digoxin, ivabradine, and, most recently, omecamtiv mecarbil.37–39 Compared to other HF treatments, vericiguat requires only once daily administration, is well-tolerated with minimal hemodynamic impact, and does not require routine laboratory testing or therapeutic drug monitoring for use. Escalating a patient’s underlying GDMT to include quadruple therapy, with a focus on ARNI and SGLT-2 inhibitor use, seems most rational in a majority of patients with HFrEF while reserving vericiguat in high risk patients who are already on optimal quadruple GDMT. Patients unable to tolerate traditional quadruple GDMT therapy (i.e chronic kidney disease or hyperkalemia) with a recent HFH may also be candidates for an additional HF medication, including vericiguat (Figure 2). Furthermore, patients with a recent worsening HF event and baseline NT-proBNP value < 8000 pg/mL appear to derive the greatest benefit with vericiguat. Ultimately, taking a personalized approach accounting for baseline risk, patient preference, cost, and pill burden is fundamental to amplifying the potential benefit with vericiguat.
 |
Figure 2 Place in therapy for vericiguat according to progression through the ACC/AHA stages B and C of heart failure. Abbreviations: BB, beta blocker; ACE-I, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; GDMT, guideline-directed medical therapy; ARNI, angiotensin receptor-neprilysin inhibitor; SGLT-2, sodium-glucose cotransporter-2; MRA, mineralocorticoid receptor antagonist. |
Conclusion
Vericiguat is the newest addition to the armamentarium of therapies in the treatment of HFrEF. Clinical studies support the efficacy and safety of vericiguat as an add-on therapy for patients with HFrEF and a recent worsening HF event to reduce the incidence of CV death or HFH. Patients with baseline NT-proBNP values < 8000 pg/mL may derive the greatest benefit from the addition of vericiguat. Recent updates to the ESC HF guidelines endorse the use of vericiguat in patients with HFrEF who have worsening HF despite treatment with GDMT. Vericiguat may be considered in patients with a worsening HF event, despite being on optimal GMDT or in patients who cannot tolerate traditional GDMT.
Funding
There is no funding to report.
Disclosure
Dr. Kassis-George’s disclosure includes speaking for Merck. Dr. Kanwar’s disclosures include consulting for Bayer, Abiomed, and CareDx. The other authors (Drs. Verlinden and Fu) report no conflicts of interest related to this work.
References
1. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143:e254–e743. doi:10.1161/CIR.0000000000000950
2. Shah KS, Xu H, Matsouaka RA, et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J Am Coll Cardiol. 2017;70:2476–2486. doi:10.1016/j.jacc.2017.08.074
3. Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383:1413–1424. doi:10.1056/NEJMoa2022190
4. McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371:993–1004. doi:10.1056/NEJMoa1409077
5. McMurray JJ, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381:1995–2008. doi:10.1056/NEJMoa1911303
6. Emdin M, Aimo A, Castiglione V, et al. Targeting cyclic guanosine monophosphate to treat heart failure: JACC review topic of the week. J Am Coll Cardiol. 2020;76:1795–1807. doi:10.1016/j.jacc.2020.08.031
7. Gheorghiade M, Marti CN, Sabbah HN, et al. Soluble guanylate cyclase: a potential therapeutic target for heart failure. Heart Fail Rev. 2013;18:123–134. doi:10.1007/s10741-012-9323-1
8. Follmann M, Ackerstaff J, Redlich G, et al. Discovery of the soluble guanylate cyclase stimulator vericiguat (BAY 1021189) for the treatment of chronic heart failure. J Med Chem. 2017;60:5146–5161. doi:10.1021/acs.jmedchem.7b00449
9. Armstrong PW, Pieske B, Anstrom KJ, et al. Vericiguat in patients with heart failure and reduced ejection fraction. N Engl J Med. 2020;382:1883–1893. doi:10.1056/NEJMoa1915928
10. Tsai EJ, Kass DA. Cyclic GMP signaling in cardiovascular pathophysiology and therapeutics. Pharmacol Ther. 2009;122:216–238. doi:10.1016/j.pharmthera.2009.02.009
11. Borbely A, Falcao-Pires I, van Heerebeek L, et al. Hypophosphorylation of the Stiff N2B titin isoform raises cardiomyocyte resting tension in failing human myocardium. Circ Res. 2009;104:780–786. doi:10.1161/CIRCRESAHA.108.193326
12. Boettcher M, Thomas D, Mueck W, et al. Safety, pharmacodynamic, and pharmacokinetic characterization of vericiguat: results from six phase I studies in healthy subjects. Eur J Clin Pharmacol. 2021;77:527–537. doi:10.1007/s00228-020-03023-7
13. Erdmann E, Semigran MJ, Nieminen MS, et al. Cinaciguat, a soluble guanylate cyclase activator, unloads the heart but also causes hypotension in acute decompensated heart failure. Eur Heart J. 2013;34:57–67. doi:10.1093/eurheartj/ehs196
14. Gheorghiade M, Greene SJ, Butler J, et al. Effect of vericiguat, a soluble guanylate cyclase stimulator, on natriuretic peptide levels in patients with worsening chronic heart failure and reduced ejection fraction: the SOCRATES-REDUCED randomized trial. JAMA. 2015;314:2251–2262. doi:10.1001/jama.2015.15734
15. Verquvo (Vericiguat) [Package Insert]. Whitehouse Station, NJ: Merck Sharp and Dohme Corp; 2021.
16. Cohn JN, Franciosa JA. Vasodilator therapy of cardiac failure: (first of two parts). N Engl J Med. 1977;297:27–31. doi:10.1056/NEJM197707072970105
17. ACC/AHA Task Force on Practice Guidelines. Guidelines for the evaluation and management of heart failure. Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Evaluation and Management of Heart Failure). Circulation. 1995;92:2764–2784. doi:10.1161/01.CIR.92.9.2764
18. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American college of cardiology/American heart association task force on practice guidelines (writing committee to update the 2001 guidelines for the evaluation and management of heart failure): developed in collaboration with the American college of chest physicians and the international society for heart and lung transplantation: endorsed by the heart rhythm society. Circulation. 2005;112:e154–e235. doi:10.1161/CIRCULATIONAHA.105.167586
19. CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. 1987;316:1429–1435. doi:10.1056/NEJM198706043162301
20. Pfeffer MA, Swedberg K, Granger CB, et al. Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-overall programme. Lancet. 2003;362:759–766. doi:10.1016/S0140-6736(03)14282-1
21. Packer M, Bristow MR, Cohn JN, et al. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. N Engl J Med. 1996;334:1349–1355. doi:10.1056/NEJM199605233342101
22. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet. 1999;353:2001–2007. doi:10.1016/S0140-6736(99)04440-2
23. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med. 1999;341:709–717. doi:10.1056/NEJM199909023411001
24. Mangiafico S, Costello-Boerrigter LC, Andersen IA, Cataliotti A, Burnett JC. Neutral endopeptidase inhibition and the natriuretic peptide system: an evolving strategy in cardiovascular therapeutics. Eur Heart J. 2013;34:886–893c. doi:10.1093/eurheartj/ehs262
25. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–2128. doi:10.1056/NEJMoa1504720
26. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380:347–357. doi:10.1056/NEJMoa1812389
27. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377:644–657. doi:10.1056/NEJMoa1611925
28. Maddox TM, Januzzi JL, Allen LA, et al. 2021 update to the 2017 ACC expert consensus decision pathway for optimization of heart failure treatment: answers to 10 pivotal issues about heart failure with reduced ejection fraction: a report of the American college of cardiology solution set oversight committee. J Am Coll Cardiol. 2021;77:772–810. doi:10.1016/j.jacc.2020.11.022
29. Brownell NK, Ziaeian B, Fonarow GC. The gap to fill: rationale for rapid initiation and optimal titration of comprehensive disease-modifying medical therapy for heart failure with reduced ejection fraction. Card Fail Rev. 2021;7:e18. doi:10.15420/cfr.2021.18
30. Bonderman D, Ghio S, Felix SB, et al. Riociguat for patients with pulmonary hypertension caused by systolic left ventricular dysfunction: a phase IIb double-blind, randomized, placebo-controlled, dose-ranging hemodynamic study. Circulation. 2013;128:502–511. doi:10.1161/CIRCULATIONAHA.113.001458
31. Lam CSP, Giczewska A, Sliwa K, et al. Clinical outcomes and response to vericiguat according to index heart failure event: insights from the VICTORIA trial. JAMA Cardiol. 2021;6:706–712. doi:10.1001/jamacardio.2020.6455
32. Ponikowski P, Alemayehu W, Oto A, et al. Vericiguat in patients with atrial fibrillation and heart failure with reduced ejection fraction: insights from the VICTORIA trial. Eur J Heart Fail. 2021;23:1300–1312. doi:10.1002/ejhf.2285
33. Voors AA, Mulder H, Reyes E, et al. Renal function and the effects of vericiguat in patients with worsening heart failure with reduced ejection fraction: insights from the VICTORIA (Vericiguat Global Study in Subjects with HFrEF) trial. Eur J Heart Fail. 2021;23:1313–1321. doi:10.1002/ejhf.2221
34. Ezekowitz JA, O’Connor CM, Troughton RW, et al. N-terminal pro-B-type natriuretic peptide and clinical outcomes: vericiguat heart failure with reduced ejection fraction study. JACC Heart Fail. 2020;8:931–939. doi:10.1016/j.jchf.2020.08.008
35. Ezekowitz JA, Zheng Y, Cohen-Solal A, et al. Hemoglobin and clinical outcomes in the vericiguat global study in patients with heart failure and reduced ejection fraction (VICTORIA). Circulation. 2021;144:1489–1499. doi:10.1161/CIRCULATIONAHA.121.056797
36. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42:3599–3726. doi:10.1093/eurheartj/ehab368
37. Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336:525–533. doi:10.1056/NEJM199702203360801
38. Swedberg K, Komajda M, Bohm M, et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet. 2010;376:875–885. doi:10.1016/S0140-6736(10)61198-1
39. Teerlink JR, Diaz R, Felker GM, et al. Cardiac myosin activation with omecamtiv mecarbil in systolic heart failure. N Engl J Med. 2021;384:105–116. doi:10.1056/NEJMoa2025797
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.